

RSS-Feed abonnieren
DOI: 10.1055/s-0044-1779282
Predictive Value of Corrected 18F-FDG PET/CT Baseline Parameters for Primary DLBCL Prognosis: A Single-center Study
Autor*innen


Abstract
Objective The purpose of this study was to evaluate the prognostic significance of corrected baseline metabolic parameters in fluorodeoxyglucose positron emission tomography imaging (18F-FDG PET/CT) for 3-year progression-free survival (PFS) in patients with primary diffuse large B cell lymphoma (DLBCL).
Patients and Methods Retrospective clinical and pathological data were collected for 199 patients of DLBCL diagnosed between January 2018 and January 2021. All patients underwent 18F-FDG PET/CT scans without any form of treatment. The corrected maximum standardized uptake value (corSUVmax), corrected mean standardized uptake value (corSUVmean), corrected whole-body tumor metabolic volume sum (corMTVsum), and corrected total lesion glycolysis of whole body (corTLGtotal) were corrected using the SUVmean in a 1-cm diameter mediastinal blood pool (MBP) from the descending thoracic aorta of patients. Kaplan–Meier survival curves and Cox regression were used to examine the predictive significance of corrected baseline metabolic parameters on 3-year PFS of patients. The incremental values of corrected baseline metabolic parameters were evaluated by using Harrell's C-indices, receiver operating characteristic, and Decision Curve Analysis.
Results The multivariate analysis revealed that only the National Comprehensive Cancer Network (NCCN)-International Prognostic Index (IPI) and corMTVsum had an effect on 3-year PFS of patients (p < 0.05, respectively). The Kaplan–Meier survival analysis demonstrated significant differences in PFS between the risk groups classified by corSUVsum, corMTVsum, and corTLGtotal (log-rank test, p < 0.05). The predictive model composed of corMTVsum and corTLGtotal surpasses the predictive performance of the model incorporating MTVsum and TLGtotal. The optimal performance was observed when corMTVsum was combined with NCCN-IPI, resulting in a Harrell's C index of 0.785 and area under the curve values of 0.863, 0.891, and 0.947 for the 1-, 2-, and 3-year PFS rates, respectively.
Conclusion The corMTVsum offers significant prognostic value for patients with DLBCL. Furthermore, the combination of corMTVsum with the NCCN-IPI can provide an accurate prediction of the prognosis.
Introduction
Diffuse large B cell lymphoma (DLBCL) is the most prevalent form of non-Hodgkin lymphoma, constituting approximately 30 to 35% of cases.[1] [2] It is a complex and heterogeneous malignancy characterized by a diffuse pattern of growth and aggressive behavior. While standard treatment with rituximab, cyclosphosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) induces complete response in approximately 75 to 80% of patients diagnosed with DLBCL, a subset of approximately 10 to 15% of patients will present with primary refractory disease, and an additional 20 to 25% will experience relapse after initial response.[3]
The International Prognostic Index (IPI)[4] and its modifications, age-adjusted IPI (aa-IPI),[5] and the National Comprehensive Cancer Network-IPI (NCCN-IPI),[6] have served as established prognostic models for DLBCL, helping clinicians make informed decisions and guiding treatment strategies for patients. While other prognostic factors, activated B cell-like subtype historically carries a less favorable prognosis[7] and protein expression patterns of MYC, BCL2 and BCL6, and MYC rearrangements were predictive of outcome and provided prognostic information independent of the IPI for overall survival (OS) and event-free survival.[8] However, most of the above indices were based on serum or fluorescence in situ hybridization, required a combination of several factors.
Fluorodeoxyglucose positron emission tomography imaging is a widely utilized technique for staging, restaging, and evaluating treatment response in DLBCL patients.[9] [10] [11] Various parameters that were measured during this process, such as maximum standard uptake value (SUVmax), metabolic tumor volume (MTV), and total lesion glycolysis (TLG), have demonstrated significant prognostic value in DLBCL. However, standardization of segmentation thresholds and measurement methods remains a crucial issue in the field of nuclear medicine literature, leading to inconclusive and contentious research outcomes with noticeable inconsistencies.[12] [13] [14] [15]
Accurate prognostic markers are essential for prognostic stratification, guiding timely interventions with novel treatments to improve their prognosis. Standardizing segmentation thresholds and measurement methods may also have significant impacts on clinical decision-making and ultimately improve patient outcomes with DLBCL. The principal objectives of our study were to evaluate the prognostic performance of corrected baseline tumor metabolic parameters and to determine the additional value in DLBCL patients, compared with the uncorrected baseline tumor metabolic parameters and NCCN-IPI.
Materials and Methods
Patients
Between January 2018 and January 2021, we retrospectively examined 199 patients diagnosed with DLBCL through lymph node or target lesion biopsy with postoperative pathological confirmation. All patients had complete clinical and follow-up data with a first-line R-CHOP chemotherapy regimen administered after the definitive diagnosis. Exclusion criteria included (1) a previous association with other malignancies, (2) progression or transformation from inert lymphoma, (3) prior malignancy-related treatment (including surgery, radiotherapy, and targeted drug therapy), (4) DLBCL of the central nervous system, (5) and comorbidities of acute and chronic active infectious diseases.
Follow-up information was obtained based on routine follow-up clinical examination, CT, and/or FDG-PET/CT scans. Progression-free survival (PFS) was defined as the duration from the initial diagnosis of the disease to the time of disease progression, recurrence, or death.
Clinical/Histological Parameters
In this retrospective study, we evaluated the gender, age, erythrocyte sedimentation rate (ESR), hemoglobin level, number of extranodal invasion sites, lactate dehydrogenase (LDH), and ferritin levels of 199 patients diagnosed with DLBCL. Disease stages were classified according to the Ann Arbor staging criteria as I to IV, while patients were classified as having either A or B symptoms based on the presence or absence of unexplained fever of 38°C or higher, nocturnal sweating, and weight loss of 10% or more within 6 months. Physical status was evaluated using the Zubrod- Eastern Clinical Oncology Group (ECOG)-WHO (ZPS, 5-point scale) criterion, with scores ranging from 0 to 5. The IPI, aa-IPI, and the NCCN-IPI were calculated based on different criteria.
Positron Emission Tomography Imaging Image Acquisition
Prior to undergoing an Ingenuity TF 128 PET/CT examination, patients were required to fast for 6 to 8 hours and maintain fasting blood glucose levels below 11.1 mmol/L. The imaging agent 18F-FDG was injected via a superficial vein on the back of the hand at a dose of 3.7 MBq/kg, following which patients were instructed to rest calmly in the PET/CT lounge for approximately 50 to 60 minutes before the whole-body examination. Patients were advised to drink 500 mL of water and urinate prior to the exam. A whole-body PET/CT scan was conducted in the supine position, scanning from the cranial vault to the middle femur. This was followed by a 15- to 20-minutes PET scan while still in the same posture, followed by a CT scan with 128 rows at 120 kV, 100 to 150 mA, 0.75-mm pitch, and 3.75-mm layer thickness. PET data were corrected for attenuation and iteratively reconstructed using the self-contained software once the scan had been completed. Finally, all PET and CT images were transferred to a MEDEX computer workstation (Phillips Medical Systems), which constructs fused PET/CT images for further analysis.
Positron Emission Tomography Imaging Image Analysis
To ensure accuracy, two diagnostic PET/CT physicians with more than 10 years of experience at the associate senior level or above collaborated to measure the SUVmean of systemic lesions as well as the SUVmean in the MBP of the descending thoracic aorta, which is 1 cm in diameter on PET/CT images. In the event of a disagreement, a consensus was achieved through consultation. The SUVmean of the lesion was corrected by the PET/CT diagnostician using the SUVmean of the patients' MBP of the descending thoracic aorta. The corSUVmean was calculated using the following formula: corSUVmean = patient whole-body lesion SUVmean × average MBP SUVmean/patients MBP SUVmean. The ratio of corSUVmean to SUVmean was used to determine corSUVmax. The region of interest (ROI) was determined using the threshold of 41% of corSUVmax proposed by the European Society of Nuclear Medicine. Corrected whole-body tumor metabolic volume sum (corMTVsum) was measured, and corrected total lesion glycolysis of whole body (corTLGtotal) = Σ (corSUVmean × corMTVsum). Lastly, based on the median, baseline metabolic parameters were separated into low- and high-risk groups.
Statistical Analysis
This study conducted a statistical evaluation using R (version. 4.2.1). Continuous variables were presented as mean ± standard deviation or median with interquartile range (IQR), and categorical variables were reported as frequency and proportions. The R packages “survival” were used for Kaplan–Meier survival analyses and “rms” for Cox proportional hazards regression. Univariate regression analysis was conducted to obtain variables significantly related to PFS. In the uncorrected or corrected baseline parameters, significant variables identified through univariate regression analysis were used to construct the uncorrected and corrected model. All significant variables through univariate regression analysis were integrated into a multivariate regression analysis, then selected the significant variables to construct the combined models. Harrell's C-indices, ROC curve and Decision Curve Analysis (DCA) were used to compare the performance of the prediction. All tests were two-sided, with a significance level set at p-value less than 0.05.
Results
Patient Characteristics
The main characteristics of the patients are summarized in [Table 1]. This study included a total of 199 patients with confirmed diagnosis of DLBCL, with a mean age of 62.91 ± 11.73 years and a range of 15 to 87 years. Complete follow-up information was obtained for all patients in the trial as of January 2021. Of the all patients, 91 patients experienced progression, relapse, or death, with a median time of 6.0 (IQR 4.0–9.0) months. In total of 108 patients did not experience such an event by the follow-up time, which had a median duration of 19.5 (IQR 13.0–27.0) months. A total of 25 patients died, with 3-year PFS and OS rates of 45.7 and 12.6%, respectively. Extranodal involvement was observed in 147 cases, with the gastrointestinal region being the most commonly affected (52 cases), followed by the bone (34 cases) the spleen (22 cases). A patient with multiple extranodal involvement is detailed in [Fig. 1].

Abbreviations: aa-IPI, age-adjusted International Prognostic Index; ECOG PS, Eastern Clinical Oncology Group Performance Status; ESR, erythrocyte sedimentation rate; IPI, International Prognostic Index; LDH, lactate dehydrogenase; NCCN-IPI, National Comprehensive Cancer Network-International Prognostic Index.
Cox Regression Analysis
According to univariate regression analysis, sex, age, ESR, B symptoms, number of extralymph node invasions, SUVmax and SUVmean and corSUVmean were not the factors influencing patients 3-year PFS (p > 0.05). Conversely, lactate dehydrogenase, hemoglobin, ferritin, Eastern Clinical Oncology Group Performance Status, Ann Arbor staging, IPI, aa-IPI, NCCN-IPI, MTVsum, and TLGtotal, corSUVmax, corMTVsum, and corTLGtotal were identified as significant factors that impacted PFS (p < 0.05). Following the univariate regression analysis, only significant variables were subjected to further multivariate regression analysis. Based on the results, it was noted that NCCN-IPI (hazard ratio [HR] 3.077, 95% confidence interval [CI] 1.147–8.250) and corMTVsum (HR 7.099, 95% CI 2.642–19.078) were identified as the significant factors that influenced the 3-year PFS of patients, as shown in [Table 2].
Abbreviations: aa-IPI, age-adjusted International Prognostic Index; corMTVsum, corrected whole-body tumor metabolic volume sum; corSUVmax, corrected maximum standardized uptake value; corSUVmean, corrected mean standardised uptake value; corTLGtotal, corrected total lesion glycolysis of total body; ECOG PS, Eastern Clinical Oncology Group Performance Status; ESR, erythrocyte sedimentation rate; IPI, International Prognostic Index; LDH, lactate dehydrogenase; NCCN-IPI, National Comprehensive Cancer Network-International Prognostic Index.
Survival Analysis
Kaplan–Meier estimates showed that patients could be stratified into low- or high-risk according to median of corrected baseline tumor parameters. The median SUVmax, SUVmean, MTVsum, and TLGtotal was 22.610 (IQR 16.150, 28.830), 12.802 (IQR 9.100, 17.011), 60.282 (IQR 15.832, 180.543), and 642.247 (IQR 215.270, 2807.637), respectively. The median corSUVmax, corSUVmean, corMTVsum, and corTLGtotal was 19.550 (IQR 13.878, 27.718), 10.924 (IQR 7.669, 15.348), 49.783 (IQR 13.410, 173.735), and 678.474 (IQR 161.732, 2667.590), respectively. A statistically significant difference (log-rank test, p < 0.05) in PFS between the risk groups categorized by corSUVmax, corMTVsum, and corTLGtotal. However, no significant differences were observed between the risk groups categorized by corSUVmean (log-rank test, p > 0.05). These results are depicted in [Fig. 2A–D].

Performance of the Prediction
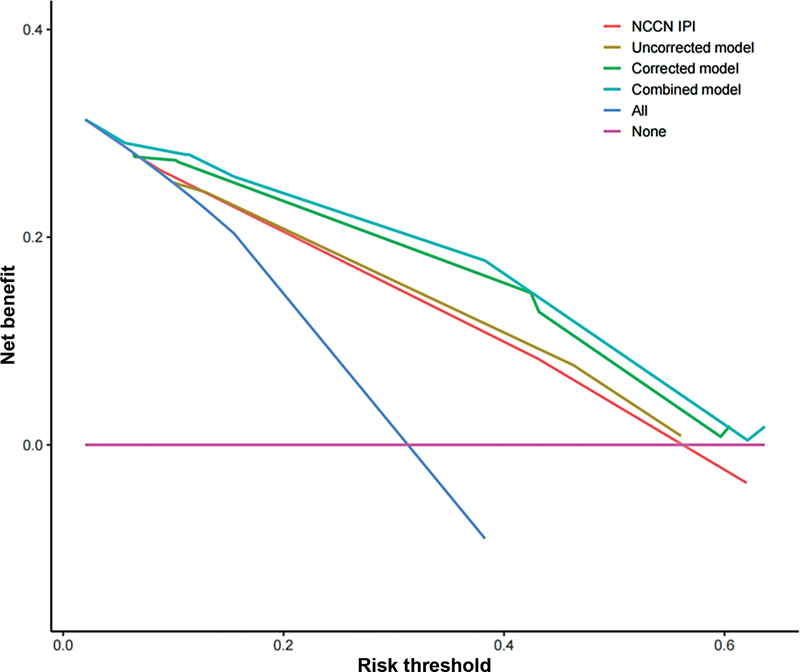
The NCCN-IPI, MTVsum and TLGtotal, corMTVsum and corTLGtotal all showed predictive ability for PFS, with C-indices of 0.730 (95% CI 0.684, 0.776), 0.731 (95% CI 0.685, 0.778), and 0.769 (95% CI 0.728, 0.811), respectively. Notably, the combined model, incorporating NCCN-IPI and corMTVsum, outperformed above predictive model, achieving a C-index of 0.785 (95% CI 0.746, 0.824) for predicting PFS. The predictive model composed of corMTVsum and corTLGtotal (area under the curve [AUC] 0.857, 0.859, and 0.936 for 1-, 2-, and 3-year PFS) surpasses the predictive performance of the model incorporating MTVsum and TLGtotal (AUC 0.803, 0.833, and 0.914 for 1-, 2-, and 3-year PFS). The combined model derived from a multivariate regression analysis, incorporating NCCN-IPI and corMTVsum, attains the highest AUC (AUC 0.863, 0.891, and 0.947 for 1-, 2-, and 3-year PFS). Notably, all these models above superior performance compared with NCCN-IPI (AUC 0.768, 0.818, and 0.898 for 1-, 2-, and 3-year PFS). Detailed results are provided in [Fig. 3] and [Table 3]. DCA demonstrated a notably higher net benefit for both the combined and corrected models compared with the uncorrected model and NCCN-IPI across diverse threshold probabilities in predicting PFS ([Fig. 4]).

Abbreviations: AUC, area under the curve; CI, confidence interval; corMTVsum, corrected whole-body tumor metabolic volume sum; corTLGtotal, corrected total lesion glycolysis of total body; NCCN-IPI, National Comprehensive Cancer Network-International Prognostic Index; PFS, progression-free survival.
Discussion
The MTV and TLG volumetric parameters have been recognized as reliable indicators for survival prediction in DLBCL patients. However, the lack of a standardized methodology for calculating these values hinders their broader clinical application. To improve accuracy and provide more meaningful results in practice, it is crucial to develop a normalized methodology for calculating these parameters. In this study, we have corrected baseline metabolic parameters to take into account the radiochemical purity and dose of each patient. Our study showed that baseline corSUVsum, corMTVsum, and corTLGtotal were significantly correlated with DLBCL. Improved prediction accuracy (Harrell's C rose from 0.731 to 0.769) for PFS was achieved by incorporating corMTVsum and corTLGtotal over MTVsum and TLGtotal. It also revealed that the combined model incorporating corMTVsum and NCCN-IPI provided superior predictive performance (AUC: 0.863, 0.891, and 0.947 for 1-, 2-, and 3-year PFS). These results outperformed the NCCN-IPI model and highlight the potential of our methodology to predict prognostic accuracy in clinical practice for patients diagnosed with DLBCL.
MTV has been regarded as a potential biomarker for the development of initial PET-adapted approaches in follicular lymphoma.[16] However, debates have arisen regarding the predictive value of baseline metabolic parameters in patients with DLBCL and the existing studies have presented conflicting results. Shagera et al[17] discovered that prechemotherapy MTV was an independent prognostic factor in addition to NCCN-IPI. The combination of baseline TMTV and NCCN-IPI may have the potential to improve the prognosis of DLBCL patients with high-risk NCCN-IPI group. On the other hand, Sasanelli et al[18] found that MTV was the only independent factor in the prognosis of DLBCL patients, while TLG was not significant. Zhou et al[15] reported that baseline TLG was an independent predictor of survival in DLBCL patients before R-CHOP treatment. Nevertheless, diverging from these results, Gallicchio et al[19] revealed that only SUVmax was a predictor of PFS in DLBCL patients, and lower SUVmax values were associated with worse outcomes.
To ensure the reliability and comparability of PET imaging parameters across centers, we propose a collaborative effort similar to the Image Biomarker Standardization Initiative. This study utilizes a hybrid measurement method that combines the fixed threshold of corSUVmax method with the threshold of 41% corSUVmax method to calculate baseline parameters. The determination of the fixed threshold for corSUVmax is based on the average SUVmean in the MBP form the Deauville criteria. It is a 5-point scale model, implemented to standardize the visual assessment of treatment response in DLBCL through interim and post-treatment FDG-PET/CT.[20] In this scale model, the FDG uptake in the MBP and liver is referenced.[21] Barrington et al[22] delineated the methodology and location for measuring SUV in reference regions, but there remains a lack of uniformity in the measurement details. Variations include the choice between SUVmean and SUVmax, as well as the use of ROI versus volume of interest. To enhance reproducibility, we adopted a 1-cm diameter ROI within the MBP from the descending thoracic aorta to correct the SUVmean. In contrast, the SUVmean of the liver was not used to normalize the SUVmean of the whole-body lesions since many patients had liver involvement, and the SUVmean of the affected liver was substantially higher than the normal liver. Additional correction methods, such as partial volume correction (PVC), have demonstrated enhanced accuracy in quantifying PET images in cancer studies.[23] [24] A previous investigation, the application of PVC improved the accuracy of TLG for predicting survival in patients with relapsing/refractory lymphoma before and after radioimmunotherapy.[25] Our study utilized the SUVmean of the MBP to eliminate the heterogeneity caused due to unequal radioactivity during the FDG injection or varying doses of patients owing to their body weight or other factors. After correction, the corSUVmax emerged as a predictive variable for PFS in univariate regression analysis than SUVmax without correction. With a 100% follow-up rate, cor SUVmax, corMTVsum, and corTLGtotal were all significantly correlated with PFS in DLBCL before R-CHOP treatment.
To evaluate 3-year PFS in patients with primary DLBCL, we combined all available clinical variables that could impact prognosis with PET/CT baseline metabolic parameters. B symptoms,[26] anemia,[27] elevated levels of ESR[28] and ferritin[29] have been proved to be poor prognostic factors in DLBCL patients. However, conflicting results have been reported regarding their impact on prognosis. Our study confirms that anemia and elevated levels of ferritin are associated with a poor prognosis, but we did not observe B symptoms and ESR levels as significant predictors of outcomes.
Our study has several limitations that should be noted. This study was a single-center retrospective study, a small sample size and heterogeneous population may have introduced potential bias and confounding variables that could have influenced the identified clinical prognostic factors. Additionally, we did not perform molecular pathology analysis, including assessments of MYC, BCL-2, and BCL-6 protein expression and gene rearrangements, known as prognostic factors. This limitation arose from the unavailability of data for all patients. To further explore the potential of combining baseline tumor metabolic characteristics and radiomics for personalized prognosis in DLBCL patients and to assess whether it could eventually replace the NCCN-IPI, future prospective research is warranted.
Conclusion
Corrected PET-CT baseline metabolic parameters can serve as critical prognostic factors for primary DLBCL patients. A combined model incorporating corMTVsum with the NCCN-IPI can provide additional prognostic value to PFS in primary DLBCL patients. Ultimately, this approach may lead to the development of more precise and individualized treatment plans, thereby enhancing the accuracy of prognostication and improving patient outcomes in primary DLBCL patients.
Conflict of Interest
None declared.
* These authors contributed equally to this work and retain the first authorship.
-
References
- 1 Flowers CR, Sinha R, Vose JM. Improving outcomes for patients with diffuse large B-cell lymphoma. CA Cancer J Clin 2010; 60 (06) 393-408
- 2 Friedberg JW. Relapsed/refractory diffuse large B-cell lymphoma. Hematology (Am Soc Hematol Educ Program) 2011; 498-505
- 3 Sehn LH, Gascoyne RD. Diffuse large B-cell lymphoma: optimizing outcome in the context of clinical and biologic heterogeneity. Blood 2015; 125 (01) 22-32
- 4 International Non-Hodgkin's Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin's lymphoma. N Engl J Med 1993; 329 (14) 987-994
- 5 Ziepert M, Hasenclever D, Kuhnt E. et al. Standard International prognostic index remains a valid predictor of outcome for patients with aggressive CD20+ B-cell lymphoma in the rituximab era. [published correction appears in J Clin Oncol 2011 Feb 20;29(6):779] J Clin Oncol 2010; 28 (14) 2373-2380
- 6 Zhou Z, Sehn LH, Rademaker AW. et al. An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood 2014; 123 (06) 837-842
- 7 Read JA, Koff JL, Nastoupil LJ, Williams JN, Cohen JB, Flowers CR. Evaluating cell-of-origin subtype methods for predicting diffuse large B-cell lymphoma survival: a meta-analysis of gene expression profiling and immunohistochemistry algorithms. Clin Lymphoma Myeloma Leuk 2014; 14 (06) 460-467.e2
- 8 Horn H, Ziepert M, Becher C. et al; German High-Grade Non-Hodgkin Lymphoma Study Group. MYC status in concert with BCL2 and BCL6 expression predicts outcome in diffuse large B-cell lymphoma. Blood 2013; 121 (12) 2253-2263
- 9 Cheson BD, Pfistner B, Juweid ME. et al; International Harmonization Project on Lymphoma. Revised response criteria for malignant lymphoma. J Clin Oncol 2007; 25 (05) 579-586
- 10 Juweid ME, Stroobants S, Hoekstra OS. et al; Imaging Subcommittee of International Harmonization Project in Lymphoma. Use of positron emission tomography for response assessment of lymphoma: consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma. J Clin Oncol 2007; 25 (05) 571-578
- 11 Cheson BD, Fisher RI, Barrington SF. et al; Alliance, Australasian Leukaemia and Lymphoma Group, ; Eastern Cooperative Oncology Group, ; European Mantle Cell Lymphoma Consortium, ; Italian Lymphoma Foundation, ; European Organisation for Research, ; Treatment of Cancer/Dutch Hemato-Oncology Group, ; Grupo Español de Médula Ósea, ; German High-Grade Lymphoma Study Group, ; German Hodgkin's Study Group, ; Japanese Lymphorra Study Group, ; Lymphoma Study Association, ; NCIC Clinical Trials Group, ; Nordic Lymphoma Study Group, ; Southwest Oncology Group, ; United Kingdom National Cancer Research Institute. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol 2014; 32 (27) 3059-3068
- 12 Gupta N, Singh N. To determine the prognostic significance of 18-fluorodeoxyglucose positron emission tomography/computed tomography scan-derived parameters (total lesion glycolysis and metabolic tumor volume) in patients of diffuse large B-cell lymphoma with only nodal involvement. Indian J Nucl Med 2020; 35 (02) 100-104
- 13 Guzmán Ortiz S, Mucientes Rasilla J, Vargas Núñez JA, Royuela A, Navarro Matilla B, Mitjavila Casanovas M. Evaluation of the prognostic value of different methods of calculating the tumour metabolic volume with 18F-FDG PET/CT, in patients with diffuse large cell B-cell lymphoma. Rev Esp Med Nucl Imagen Mol (Engl Ed) 2020; 39 (06) 340-346
- 14 Ceriani L, Martelli M, Zinzani PL. et al. Utility of baseline 18FDG-PET/CT functional parameters in defining prognosis of primary mediastinal (thymic) large B-cell lymphoma. Blood 2015; 126 (08) 950-956
- 15 Zhou M, Chen Y, Huang H, Zhou X, Liu J, Huang G. Prognostic value of total lesion glycolysis of baseline 18F-fluorodeoxyglucose positron emission tomography/computed tomography in diffuse large B-cell lymphoma. Oncotarget 2016; 7 (50) 83544-83553
- 16 Meignan M, Cottereau AS, Versari A. et al. Baseline metabolic tumor volume predicts outcome in high-tumor-burden follicular lymphoma: a pooled analysis of three multicenter studies. J Clin Oncol 2016; 34 (30) 3618-3626
- 17 Shagera QA, Cheon GJ, Koh Y. et al. Prognostic value of metabolic tumour volume on baseline 18F-FDG PET/CT in addition to NCCN-IPI in patients with diffuse large B-cell lymphoma: further stratification of the group with a high-risk NCCN-IPI. Eur J Nucl Med Mol Imaging 2019; 46 (07) 1417-1427
- 18 Sasanelli M, Meignan M, Haioun C. et al. Pretherapy metabolic tumour volume is an independent predictor of outcome in patients with diffuse large B-cell lymphoma. Eur J Nucl Med Mol Imaging 2014; 41 (11) 2017-2022
- 19 Gallicchio R, Mansueto G, Simeon V. et al. F-18 FDG PET/CT quantization parameters as predictors of outcome in patients with diffuse large B-cell lymphoma. Eur J Haematol 2014; 92 (05) 382-389
- 20 Meignan M, Itti E, Bardet S. et al. Development and application of a real-time on-line blinded independent central review of interim PET scans to determine treatment allocation in lymphoma trials. J Clin Oncol 2009; 27 (16) 2739-2741
- 21 Chiaravalloti A, Danieli R, Abbatiello P. et al. Factors affecting intrapatient liver and mediastinal blood pool 18F-FDG standardized uptake value changes during ABVD chemotherapy in Hodgkin's lymphoma. Eur J Nucl Med Mol Imaging 2014; 41 (06) 1123-1132
- 22 Barrington SF, Kluge R. FDG PET for therapy monitoring in Hodgkin and non-Hodgkin lymphomas. Eur J Nucl Med Mol Imaging 2017; 44 (suppl 1): 97-110
- 23 Cysouw MCF, Kramer GM, Hoekstra OS. et al. Accuracy and precision of partial-volume correction in oncological PET/CT studies. J Nucl Med 2016; 57 (10) 1642-1649
- 24 Hoetjes NJ, van Velden FH, Hoekstra OS. et al. Partial volume correction strategies for quantitative FDG PET in oncology. Eur J Nucl Med Mol Imaging 2010; 37 (09) 1679-1687
- 25 Taghvaei R, Zadeh MZ, Sirous R. et al. Pre-treatment partial-volume-corrected TLG is the best predictor of overall survival in patients with relapsing/refractory non-hodgkin lymphoma following radioimmunotherapy. Am J Nucl Med Mol Imaging 2018; 8 (06) 407-414
- 26 Škor O, Bicanová L, Wolfesberger B. et al. Are B-symptoms more reliable prognostic indicators than substage in canine nodal diffuse large B-cell lymphoma. Vet Comp Oncol 2021; 19 (01) 201-208
- 27 Adams HJ, de Klerk JM, Fijnheer R. et al. Prognostic value of anemia and C-reactive protein levels in diffuse large B-cell lymphoma. Clin Lymphoma Myeloma Leuk 2015; 15 (11) 671-679
- 28 Wu S, Zhou Y, Hua HY. et al. Inflammation marker ESR is effective in predicting outcome of diffuse large B-cell lymphoma. BMC Cancer 2018; 18 (01) 997
- 29 Kim DJ, Kim T, Jeong JY. et al. Poor prognostic impact of high serum ferritin levels in patients with a lower risk of diffuse large B cell lymphoma. Int J Hematol 2020; 111 (04) 559-566
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
13. Februar 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Flowers CR, Sinha R, Vose JM. Improving outcomes for patients with diffuse large B-cell lymphoma. CA Cancer J Clin 2010; 60 (06) 393-408
- 2 Friedberg JW. Relapsed/refractory diffuse large B-cell lymphoma. Hematology (Am Soc Hematol Educ Program) 2011; 498-505
- 3 Sehn LH, Gascoyne RD. Diffuse large B-cell lymphoma: optimizing outcome in the context of clinical and biologic heterogeneity. Blood 2015; 125 (01) 22-32
- 4 International Non-Hodgkin's Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin's lymphoma. N Engl J Med 1993; 329 (14) 987-994
- 5 Ziepert M, Hasenclever D, Kuhnt E. et al. Standard International prognostic index remains a valid predictor of outcome for patients with aggressive CD20+ B-cell lymphoma in the rituximab era. [published correction appears in J Clin Oncol 2011 Feb 20;29(6):779] J Clin Oncol 2010; 28 (14) 2373-2380
- 6 Zhou Z, Sehn LH, Rademaker AW. et al. An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood 2014; 123 (06) 837-842
- 7 Read JA, Koff JL, Nastoupil LJ, Williams JN, Cohen JB, Flowers CR. Evaluating cell-of-origin subtype methods for predicting diffuse large B-cell lymphoma survival: a meta-analysis of gene expression profiling and immunohistochemistry algorithms. Clin Lymphoma Myeloma Leuk 2014; 14 (06) 460-467.e2
- 8 Horn H, Ziepert M, Becher C. et al; German High-Grade Non-Hodgkin Lymphoma Study Group. MYC status in concert with BCL2 and BCL6 expression predicts outcome in diffuse large B-cell lymphoma. Blood 2013; 121 (12) 2253-2263
- 9 Cheson BD, Pfistner B, Juweid ME. et al; International Harmonization Project on Lymphoma. Revised response criteria for malignant lymphoma. J Clin Oncol 2007; 25 (05) 579-586
- 10 Juweid ME, Stroobants S, Hoekstra OS. et al; Imaging Subcommittee of International Harmonization Project in Lymphoma. Use of positron emission tomography for response assessment of lymphoma: consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma. J Clin Oncol 2007; 25 (05) 571-578
- 11 Cheson BD, Fisher RI, Barrington SF. et al; Alliance, Australasian Leukaemia and Lymphoma Group, ; Eastern Cooperative Oncology Group, ; European Mantle Cell Lymphoma Consortium, ; Italian Lymphoma Foundation, ; European Organisation for Research, ; Treatment of Cancer/Dutch Hemato-Oncology Group, ; Grupo Español de Médula Ósea, ; German High-Grade Lymphoma Study Group, ; German Hodgkin's Study Group, ; Japanese Lymphorra Study Group, ; Lymphoma Study Association, ; NCIC Clinical Trials Group, ; Nordic Lymphoma Study Group, ; Southwest Oncology Group, ; United Kingdom National Cancer Research Institute. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol 2014; 32 (27) 3059-3068
- 12 Gupta N, Singh N. To determine the prognostic significance of 18-fluorodeoxyglucose positron emission tomography/computed tomography scan-derived parameters (total lesion glycolysis and metabolic tumor volume) in patients of diffuse large B-cell lymphoma with only nodal involvement. Indian J Nucl Med 2020; 35 (02) 100-104
- 13 Guzmán Ortiz S, Mucientes Rasilla J, Vargas Núñez JA, Royuela A, Navarro Matilla B, Mitjavila Casanovas M. Evaluation of the prognostic value of different methods of calculating the tumour metabolic volume with 18F-FDG PET/CT, in patients with diffuse large cell B-cell lymphoma. Rev Esp Med Nucl Imagen Mol (Engl Ed) 2020; 39 (06) 340-346
- 14 Ceriani L, Martelli M, Zinzani PL. et al. Utility of baseline 18FDG-PET/CT functional parameters in defining prognosis of primary mediastinal (thymic) large B-cell lymphoma. Blood 2015; 126 (08) 950-956
- 15 Zhou M, Chen Y, Huang H, Zhou X, Liu J, Huang G. Prognostic value of total lesion glycolysis of baseline 18F-fluorodeoxyglucose positron emission tomography/computed tomography in diffuse large B-cell lymphoma. Oncotarget 2016; 7 (50) 83544-83553
- 16 Meignan M, Cottereau AS, Versari A. et al. Baseline metabolic tumor volume predicts outcome in high-tumor-burden follicular lymphoma: a pooled analysis of three multicenter studies. J Clin Oncol 2016; 34 (30) 3618-3626
- 17 Shagera QA, Cheon GJ, Koh Y. et al. Prognostic value of metabolic tumour volume on baseline 18F-FDG PET/CT in addition to NCCN-IPI in patients with diffuse large B-cell lymphoma: further stratification of the group with a high-risk NCCN-IPI. Eur J Nucl Med Mol Imaging 2019; 46 (07) 1417-1427
- 18 Sasanelli M, Meignan M, Haioun C. et al. Pretherapy metabolic tumour volume is an independent predictor of outcome in patients with diffuse large B-cell lymphoma. Eur J Nucl Med Mol Imaging 2014; 41 (11) 2017-2022
- 19 Gallicchio R, Mansueto G, Simeon V. et al. F-18 FDG PET/CT quantization parameters as predictors of outcome in patients with diffuse large B-cell lymphoma. Eur J Haematol 2014; 92 (05) 382-389
- 20 Meignan M, Itti E, Bardet S. et al. Development and application of a real-time on-line blinded independent central review of interim PET scans to determine treatment allocation in lymphoma trials. J Clin Oncol 2009; 27 (16) 2739-2741
- 21 Chiaravalloti A, Danieli R, Abbatiello P. et al. Factors affecting intrapatient liver and mediastinal blood pool 18F-FDG standardized uptake value changes during ABVD chemotherapy in Hodgkin's lymphoma. Eur J Nucl Med Mol Imaging 2014; 41 (06) 1123-1132
- 22 Barrington SF, Kluge R. FDG PET for therapy monitoring in Hodgkin and non-Hodgkin lymphomas. Eur J Nucl Med Mol Imaging 2017; 44 (suppl 1): 97-110
- 23 Cysouw MCF, Kramer GM, Hoekstra OS. et al. Accuracy and precision of partial-volume correction in oncological PET/CT studies. J Nucl Med 2016; 57 (10) 1642-1649
- 24 Hoetjes NJ, van Velden FH, Hoekstra OS. et al. Partial volume correction strategies for quantitative FDG PET in oncology. Eur J Nucl Med Mol Imaging 2010; 37 (09) 1679-1687
- 25 Taghvaei R, Zadeh MZ, Sirous R. et al. Pre-treatment partial-volume-corrected TLG is the best predictor of overall survival in patients with relapsing/refractory non-hodgkin lymphoma following radioimmunotherapy. Am J Nucl Med Mol Imaging 2018; 8 (06) 407-414
- 26 Škor O, Bicanová L, Wolfesberger B. et al. Are B-symptoms more reliable prognostic indicators than substage in canine nodal diffuse large B-cell lymphoma. Vet Comp Oncol 2021; 19 (01) 201-208
- 27 Adams HJ, de Klerk JM, Fijnheer R. et al. Prognostic value of anemia and C-reactive protein levels in diffuse large B-cell lymphoma. Clin Lymphoma Myeloma Leuk 2015; 15 (11) 671-679
- 28 Wu S, Zhou Y, Hua HY. et al. Inflammation marker ESR is effective in predicting outcome of diffuse large B-cell lymphoma. BMC Cancer 2018; 18 (01) 997
- 29 Kim DJ, Kim T, Jeong JY. et al. Poor prognostic impact of high serum ferritin levels in patients with a lower risk of diffuse large B cell lymphoma. Int J Hematol 2020; 111 (04) 559-566