

Subscribe to RSS
DOI: 10.1055/s-0044-1779317
Convolutional Neural Networks in the Diagnosis of Cervical Myelopathy
Article in several languages: português | EnglishAuthors
Financial Support The authors declare that the present research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.

Abstract
Objective Artificial intelligence technologies have been used increasingly in spine surgery as a diagnostic tool. The aim of the present study was to evaluate the effectiveness of the convolutional neural networks in the diagnosis of cervical myelopathy (CM) compared with conventional cervical magnetic resonance imaging (MRI).
Materials and Methods This was a cross-sectional descriptive analytical study. A total of 125 participants with clinical and radiological diagnosis of CM were included in the study. Sagittal and axial MRI images in the T2 sequence of the cervical spine were used. All image parts were obtained as 8 bytes/pixel in 2 different categories, CM and normal, both in axial and sagittal views.
Results Triple cross validation was performed to prevent overfitting during the training process. A total of 242 sample images were used for training and testing the model created for axial views. In the axial view, the calculated values are 97.44% for sensitivity and 97.56% for specificity. A total of 249 sample images were used for training and testing the model created for sagittal views. The calculated values are 97.50% for sensitivity and 97.67% for specificity. After the training, the average accuracy value was 96.7% (±1.53) for the axial view and 97.19% (±1.2) for the sagittal view.
Conclusion Deep learning (DL) has shown a great improvement especially in spine surgery. We found that DL technology works with a higher accuracy than other studies in the literature for the diagnosis of CM.
Keywords
artificial neural networks - cervical vertebrae - deep learning - magnetic resonance imaging - myelopathyIntroduction
Cervical myelopathy (CM) is a common degenerative disease of the cervical spine caused by spinal cord compression.[1] The decrease in the volume of the spinal canal is usually due to disc degeneration, osteophytes or ossified posterior longitudinal ligament results with ischemic changes. The clinical findings of the CM vary with the severity and location of the spinal cord compression.[2] Patients generally present with numbness and pain in the extremities and neurological symptoms such as loss of coordination and balance. The clinical and radiological modalities of the patient should be evaluated together in the evaluation of this disease and in determining the treatment options.[3]
The imaging procedures for CM are plain radiography, magnetic resonance imaging (MRI) and computed tomography (CT). Magnetic resonance imaging in CM is more valuable in evaluating the spinal cord, disc and other soft tissues compared with other imaging methods.[4] [5] As a result of advances in MRI technology such as MR spectroscopy and diffusion tensor imaging, resolution and image quality have greatly improved. In parallel with these developments, new imaging methods are being developed with many studies in the diagnosis of CM.[6]
Convolutional neural networks (CNNs), a machine learning (ML) technique, are increasingly used in various industrial and research fields.[7] Deep learning (DL) is a multi-layered neural network in which feature extraction is done automatically. It extends traditional neural networks by adding more hidden layers to the network architecture between the input and output layers to model more complex and nonlinear relationships.
Machine learning technologies are also used in many health applications such as medical image analysis, biological signal analysis, prediction of medical events, computer-aided detection and diagnosis, aiding in treatment selection, and analysis of health records for recent years.[8]
Machine learning technology has been used increasingly in spine surgery as well as in many medical fields. However, it is noticed that most of the studies about this subject in the literature have been conducted except of the cervical spine.[9] In the present study, we aimed to demonstrate the effectiveness of the CNN in the diagnosis of CM compared with conventional cervical MRI.
Materials and Methods
Participants and MRI Samples
Participants aged between 18 and 75 years old diagnosed as CM were included in the study. All images were obtained with a 3.0 Tesla Siemens MR scanner (Siemens, Erlangen, Germany) with a standard cervical collar. Radiological images of the cervical spine were evaluated by three investigators experienced with a minimum experience of 5 years in spinal surgery. Axial and sagittal MRI images of the cervical spine were used. Magnetic resonance imaging scans in Digital Imaging and Communications in Medicine (DICOM) format (8 bits/pixel) have been converted to one of the raster formats (png). Thereafter, the 'region of interest' selection was made, and the regions were labeled as CM and normal, both in axial and sagittal views ([Fig. 1]).

The inclusion criteria for the study were the participants with classical CM symptoms such as weakness and clumsiness at the upper extremities, hyperreflexia, and/or gait difficulties; radiological findings of spinal compression; scores on the modified Japanese Orthopedic Association scale (mJOA) < 18. Participants with a previous history of cervical spinal surgery and those with a systematic disease (rheumatologic or neural disease) were excluded from the study. The present study was approved by the local ethical committee (KAEK/2020.07.129) and registered at Clinicaltrials.gov (NCT04796987).
Calculation Environment
A computer with 8 GB memory and Intel i7 processor was used to perform the calculations and train the DL model. Deep learning models were developed using the Python programming language. To assess the model performance, mean and median cross-validated accuracies, sensitivity, specificity, positive, and negative predictive value were used.
Neural Network Design
Significant developments in ML and image processing techniques enable medical images to be evaluated more accurately using DL methods.[7] The term “deep learning” has been used for many years in the classification of medical images. Convolutional neural network, one of the popular DL methods, was used to classify images in the present study. A simple CNN architecture consists of convolutional layer (Conv), pooling layer (for example, Max-pooling), nonlinear layer (for example, ReLU, TanH) and a loss function (for example, Sigmoid, Softmax) on the last fully connected (FC). Output can be of a single class; however, it can also have multiple outputs.[10] The CNN architecture used in the study is presented in [Fig. 2].

Results
A total of 125 participants (58 female and 67 male) with a mean age of 56.32 ± 6.77 years old who were diagnosed as CM were included in the study. The mean mJOA scores of the participants was 12.01 ± 2.46. Demographic characteristics of the participants are shown in [Table 1]. Normal and myelomalasic MRI layers of the participants were analyzed.
|
Variable |
Participants (n = 125) |
|---|---|
|
Age (in years) (mean ± SD) |
56.32 ± 6.77 |
|
Gender (female/male) n (%) |
58 (46.4%)/67 (53.6%) |
|
Height (cm) (mean ± SD) |
164.5 ± 8.52 |
|
Weight (kg) (mean ± SD) |
74.96 ± 8.48 |
|
mJOA score |
12.01 ± 2.46 |
Training Information
In the created network design, sample images taken in both axial and sagittal view were subjected to training. Thus, two different DL trainings were performed for both views; 67% of the images were used for training, and 33% for validation and testing. Triple cross validation was used to test the consistency of the results.
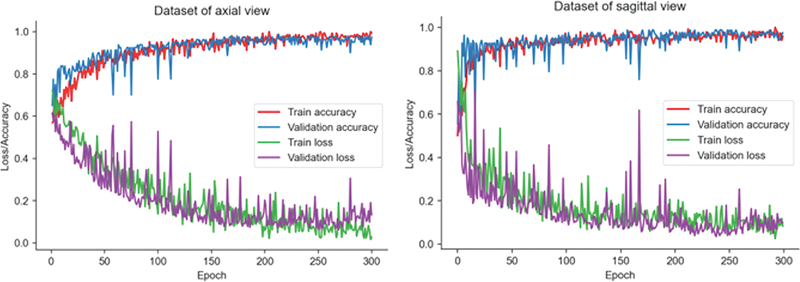
The models obtained for both views consist of 300 epochs. Triple cross validation was performed to prevent overfitting during the training process. After training, the average accuracy value was 96.7% (±1.53) for the axial view and 97.19% (±1.2) for the sagittal view. The graphs of the DL training process are shown in [Fig. 3].
Evaluation Metrics of Training
Axial View
A total of 242 sample images were used for training and testing the model created for axial views. Of these images, 120 were labeled as CM, and 122 were labeled as normal. A total of 162 of these images were used for the training of the DL model, and 80 for the evaluation of the training. The true positive, true negative, false positive, and false negative values obtained from the evaluation of the training are shown in [Table 2]. The confusion matrix accuracy values formed by these values are shown in [Fig. 4]. After the evaluation, the overall accuracy value of the model was calculated as 97.50%.
|
Total population |
Human (true condition) |
||
|---|---|---|---|
|
Condition positive |
Condition negative |
||
|
Developed model (predicted condition) for sagittal images |
Predicted condition positive |
True positive = 39 |
False positive = 1 (type-I error) |
|
Predicted condition negative |
False negative = 1 (type-II error) |
True negative = 42 |
|
|
Developed model (predicted condition) for axial images |
Predicted condition positive |
True positive = 38 |
False positive = 1 (type-I error) |
|
Predicted condition negative |
False negative = 1 (type-II error) |
True negative = 40 |
|

The calculated values are 97.44% for true-positive rate (TPR, recall, sensitivity), 97.56% for true-negative rate (TNR, specificity), 2.56% for false-negative rate (FNR, miss rate), and 97.44% for positive predictive value (PPV, precision). Also, the F1 score is calculated as 0.97, Matthew correlation coefficient (MCC) as 0.95, and Cohen kappa coherent as 0.95.
After the evaluation, the receiver operating characteristic (ROC) curve was drawn, the area under the ROC curve[11] was calculated, and shown in [Fig. 5].

Sagittal view
A total of 249 sample images from the MRI of the participants were selected for training and testing the model created for sagittal views. Of these images, 124 were labeled as CM, and 125 were labeled as normal. A total of 166 of these images were used for the training of the DL model, and 83 for the evaluation of the training. The true positive, true negative, false positive, and false negative values that occur after the evaluation of the training are shown in [Table 2]. The confusion matrix accuracy values formed by these values are given in [Fig. 4]. After the evaluation, the overall accuracy value of the model was calculated as 97.59%.
The calculated values are 97.50% for TPR (recall, sensitivity), 97.67% for TNR (specificity), 2.50% for FNR (miss rate), and 97.50% for PPV (precision). Also, the F1 score is calculated as 0.98, MCC as 0.95, and Cohen kappa coherent as 0.95.
After the evaluation, the ROC curve was drawn, the AUC was calculated, and shown in [Fig. 5].
Discussion
Machine learning technologies have started to be used in many areas with the development it has shown in recent years.[12] Deep learning, a sub-branch of ML, has shown a great improvement especially in the medical field. In parallel with this development, the use of DL in spine surgery has increased significantly in recent years and has brought a new breath to the determination of spine problems and the evaluation of treatment options.[9] Machine learning is currently used more frequently in the evaluation of diagnostic imaging, such as the location of vertebra and discs and the shape of the spine, with the information obtained from radiological imaging methods such as CT and MRI.[13] However, with the progress in ML studies, its use is gradually increasing in treatment protocols and predicting possible results.[14]
The diagnosis of CM is based on findings obtained in clinical examination and radiological imaging. Magnetic resonance imaging is the most effective diagnostic method in the radiological evaluation of patients with clinical myelopathic symptoms.[15] Spinal cord anatomy and medullary canal structures are better evaluated in sagittal and axial views.[16] [17] Cervical myelopathy characteristically manifests itself as hypointense focal cord atrophy in the T1 sequence and hyperintense in the T2 sequence. However, it has been reported that the T2 sequence detects intramedullary changes better and is more valuable in terms of prognosis.[15] It has also been reported that between 58 and 85% of patients with clinical symptoms of CM have a hyperintense signal in the T2 sequence.[18] Evaluation of CM is primarily based on subjective judgements of the MRI findings of the spinal cord and is therefore limited by the training and expertise of the evaluator.[19] Therefore, in the present study, we tried to reveal the effectiveness of DL in the diagnosis of myelopathy to eliminate the subjection on the person at diagnosis.
In this respect, we evaluated the T2 sequence of the cervical MRI of participants with myelomalacia in the present study. In this sequence, sagittal and axial MR sections of the participants were obtained, normal and areas of myelomalacia in the intramedullary region were marked and the machine was trained. Cervical MRI of the participants were taken in a single center and with the same MRI device. However, because MRI scans may differ from patient to patient, normal images and those of the field of myelomalacia were obtained in the same section to standardize the scans.
In a pilot study, the effectiveness of ML in the diagnosis of CM was evaluated on 28 patients. In this study in which the cervical MRIs of participants with myelopathy symptoms were evaluated, the median accuracy was determined as 90%. The mean sensitivity was 90% and specificity was 85%.[20] Similarly, in another study investigating the effectiveness of ML in CM, diffusion tensor imaging was used. In this study, mean accuracy was 89.7%, sensitivity was 85%, and specificity was 92.4%.[21] In another study, the highest mean accuracy found at the end of the study was 77%, the mean sensitivity was 78%, and mean specificity was 80%.[22] In the present study, we used conventional cervical MRIs, which are used as a standard in diagnosis in a daily routine. Because the anatomy of the spinal cord is best evaluated in the axial and sagittal planes, we evaluated these two planes separately. At the end of the study, the median accuracy in the axial plane was found to be 97.50%. Average sensitivity was 97.44% and specificity was 97.56%. In the sagittal plane, mean accuracy was 97.59%, sensitivity was 97.50%, and specificity was 97.67%. In this respect, a statistically significant diagnosis of myelopathy was made in both axial and sagittal planes. However, it is seen that the rates of myelopathy detection in our study are higher than those of other studies in the literature.
The present study has some limitations. The retrospective nature of the study and small sample size can be considered as limitations. More participants could be included in the study and more accurate information could be obtained in determining the accuracy rate. On the other hand, there are also strengths of the study. The cervical MRIs of the participants with myelopathy symptoms taken in a single center and with the same MRI device were evaluated by two physicians experienced in spinal diseases. In this way, standardization of the images was tried to be kept at the maximum level. In addition, since there could be a difference between MRI sequences taken even in the same participant, normal and the area of myelomalacia images were compared on the same sections.
In the last half century, ML and artificial neural networks (ANN) are frequently preferred in solving nonlinear problems. The DL method, which is a multi-layered ANN, is widely used in the field of health, with the increasing computational power of computers and the easier digital acquisition of medical images. Human-induced errors can be reduced with high accuracy and fast prediagnosis systems to be revealed. In subsequent studies based on the present study, a pre-diagnosis system can be established by automatic detection of the region with anomaly, staging and monitoring of the myelopathy status can be achieved.
Conclusion
Machine learning technologies are used in many health applications, especially in medical image analysis. Deep learning, a sub-branch of ML, has shown a great improvement especially in spine surgery. In the present study, we aimed to reveal the effectiveness of DL in the diagnosis of CM. As a result of our study, we observed that DL technology works with a higher accuracy than other studies in the literature for the diagnosis of CM. However, in subsequent studies, a prediagnosis system can be established by automatic detection of the region with anomaly, staging, and monitoring of the myelopathy status can be provided.
Conflito de Interesses
Os autores não têm conflitos de interesses a declarar.
Work carried out at the Department of Physical Medicine and Rehabilitation, University of Health Sciences, Istanbul Kanuni Sultan Suleyman Training and Research Hospital, Istanbul, Turkey.
-
Referências
- 1 Klineberg E. Cervical spondylotic myelopathy: a review of the evidence. Orthop Clin North Am 2010; 41 (02) 193-202
- 2 Cook C, Brown C, Isaacs R, Roman M, Davis S, Richardson W. Clustered clinical findings for diagnosis of cervical spine myelopathy. J Manual Manip Ther 2010; 18 (04) 175-180
- 3 Kadanka Z, Bednarík J, Vohánka S, Vlach O, Stejskal L, Chaloupka R. et al. Conservative treatment versus surgery in spondylotic cervical myelopathy: a prospective randomised study. Eur Spine J 2000; 9 (06) 538-544
- 4 Nagata K, Kiyonaga K, Ohashi T, Sagara M, Miyazaki S, Inoue A. Clinical value of magnetic resonance imaging for cervical myelopathy. Spine 1990; 15 (11) 1088-1096
- 5 Kanna RM, Kamal Y, Mahesh A, Venugopal P, Shetty AP, Rajasekaran S. The impact of routine whole spine MRI screening in the evaluation of spinal degenerative diseases. Eur Spine J 2017; 26 (08) 1993-1998
- 6 Maki S, Koda M, Kitamura M, Inada T, Kamiya K, Ota M. et al. Diffusion tensor imaging can predict surgical outcomes of patients with cervical compression myelopathy. Eur Spine J 2017; 26 (09) 2459-2466
- 7 Lee JG, Jun S, Cho YW, Lee H, Kim GB, Seo JB, Kim N. Deep Learning in Medical Imaging: General Overview. Korean J Radiol 2017; 18 (04) 570-584
- 8 Lundervold AS, Lundervold A. An overview of deep learning in medical imaging focusing on MRI. Z Med Phys 2019; 29 (02) 102-127
- 9 Galbusera F, Casaroli G, Bassani T. Artificial intelligence and machine learning in spine research. JOR Spine 2019; 2 (01) e1044
- 10 Abdelhafiz D, Yang C, Ammar R, Nabavi S. Deep convolutional neural networks for mammography: advances, challenges and applications. BMC Bioinformatics 2019; 20 (Suppl. 11) 281
- 11 Zhang S, Fukunaga T, Oka S, Orita H, Kaji S, Yube Y. et al. Concerns of quality, utility, and reliability of laparoscopic gastrectomy for gastric cancer in public video sharing platform. Ann Transl Med 2020; 8 (05) 196
- 12 Chang M, Canseco JA, Nicholson KJ, Patel N, Vaccaro AR. The role of machine learning in spine surgery: The future is now. Front Surg 2020; 7: 54
- 13 Schmidhuber J. Deep learning in neural networks: an overview. Neural Netw 2015; 61: 85-117
- 14 Kim JS, Merrill RK, Arvind V, Kaji D, Pasik SD, Nwachukwu CC. et al. Examining the ability of artificial neural networks machine learning models to accurately predict complications following posterior lumbar spine fusion. Spine 2018; 43 (12) 853-860
- 15 Al-Mefty O, Harkey LH, Middleton TH, Smith RR, Fox JL. Myelopathic cervical spondylotic lesions demonstrated by magnetic resonance imaging. J Neurosurg 1988; 68 (02) 217-222
- 16 Zhou Y, Kim SD, Vo K, Riew KD. Prevalence of cervical myelomalacia in adult patients requiring a cervical magnetic resonance imaging. Spine 2015; 40 (04) E248-E252
- 17 Emery SE. Cervical spondylotic myelopathy: diagnosis and treatment. J Am Acad Orthop Surg 2001; 9 (06) 376-388
- 18 Chen CJ, Lyu RK, Lee ST, Wong YC, Wang LJ. Intramedullary high signal intensity on T2-weighted MR images in cervical spondylotic myelopathy: prediction of prognosis with type of intensity. Radiology 2001; 221 (03) 789-794
- 19 Rajasekaran S, Vaccaro AR, Kanna RM, Schroeder GD, Oner FC, Vialle L. et al. The value of CT and MRI in the classification and surgical decision-making among spine surgeons in thoracolumbar spinal injuries. Eur Spine J 2017; 26 (05) 1463-1469
- 20 Hopkins BS, Weber II KA, Kesavabhotla K, Paliwal M, Cantrell DR, Smith ZA. Machine learning for the prediction of cervical spondylotic myelopathy: A post hoc pilot study of 28 participants. World Neurosurg 2019; 127: e436-e442
- 21 Jin R, Luk KD, Cheung JPY, Hu Y. Prognosis of cervical myelopathy based on diffusion tensor imaging with artificial intelligence methods. NMR Biomed 2019; 32 (08) e4114
- 22 Merali ZG, Witiw CD, Badhiwala JH, Wilson JR, Fehlings MG. Using a machine learning approach to predict outcome after surgery for degenerative cervical myelopathy. PLoS One 2019; 14 (04) e0215133
Endereço para correspondência
Publication History
Received: 08 March 2023
Accepted: 05 May 2023
Article published online:
07 December 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution 4.0 International License, permitting copying and reproduction so long as the original work is given appropriate credit (https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referências
- 1 Klineberg E. Cervical spondylotic myelopathy: a review of the evidence. Orthop Clin North Am 2010; 41 (02) 193-202
- 2 Cook C, Brown C, Isaacs R, Roman M, Davis S, Richardson W. Clustered clinical findings for diagnosis of cervical spine myelopathy. J Manual Manip Ther 2010; 18 (04) 175-180
- 3 Kadanka Z, Bednarík J, Vohánka S, Vlach O, Stejskal L, Chaloupka R. et al. Conservative treatment versus surgery in spondylotic cervical myelopathy: a prospective randomised study. Eur Spine J 2000; 9 (06) 538-544
- 4 Nagata K, Kiyonaga K, Ohashi T, Sagara M, Miyazaki S, Inoue A. Clinical value of magnetic resonance imaging for cervical myelopathy. Spine 1990; 15 (11) 1088-1096
- 5 Kanna RM, Kamal Y, Mahesh A, Venugopal P, Shetty AP, Rajasekaran S. The impact of routine whole spine MRI screening in the evaluation of spinal degenerative diseases. Eur Spine J 2017; 26 (08) 1993-1998
- 6 Maki S, Koda M, Kitamura M, Inada T, Kamiya K, Ota M. et al. Diffusion tensor imaging can predict surgical outcomes of patients with cervical compression myelopathy. Eur Spine J 2017; 26 (09) 2459-2466
- 7 Lee JG, Jun S, Cho YW, Lee H, Kim GB, Seo JB, Kim N. Deep Learning in Medical Imaging: General Overview. Korean J Radiol 2017; 18 (04) 570-584
- 8 Lundervold AS, Lundervold A. An overview of deep learning in medical imaging focusing on MRI. Z Med Phys 2019; 29 (02) 102-127
- 9 Galbusera F, Casaroli G, Bassani T. Artificial intelligence and machine learning in spine research. JOR Spine 2019; 2 (01) e1044
- 10 Abdelhafiz D, Yang C, Ammar R, Nabavi S. Deep convolutional neural networks for mammography: advances, challenges and applications. BMC Bioinformatics 2019; 20 (Suppl. 11) 281
- 11 Zhang S, Fukunaga T, Oka S, Orita H, Kaji S, Yube Y. et al. Concerns of quality, utility, and reliability of laparoscopic gastrectomy for gastric cancer in public video sharing platform. Ann Transl Med 2020; 8 (05) 196
- 12 Chang M, Canseco JA, Nicholson KJ, Patel N, Vaccaro AR. The role of machine learning in spine surgery: The future is now. Front Surg 2020; 7: 54
- 13 Schmidhuber J. Deep learning in neural networks: an overview. Neural Netw 2015; 61: 85-117
- 14 Kim JS, Merrill RK, Arvind V, Kaji D, Pasik SD, Nwachukwu CC. et al. Examining the ability of artificial neural networks machine learning models to accurately predict complications following posterior lumbar spine fusion. Spine 2018; 43 (12) 853-860
- 15 Al-Mefty O, Harkey LH, Middleton TH, Smith RR, Fox JL. Myelopathic cervical spondylotic lesions demonstrated by magnetic resonance imaging. J Neurosurg 1988; 68 (02) 217-222
- 16 Zhou Y, Kim SD, Vo K, Riew KD. Prevalence of cervical myelomalacia in adult patients requiring a cervical magnetic resonance imaging. Spine 2015; 40 (04) E248-E252
- 17 Emery SE. Cervical spondylotic myelopathy: diagnosis and treatment. J Am Acad Orthop Surg 2001; 9 (06) 376-388
- 18 Chen CJ, Lyu RK, Lee ST, Wong YC, Wang LJ. Intramedullary high signal intensity on T2-weighted MR images in cervical spondylotic myelopathy: prediction of prognosis with type of intensity. Radiology 2001; 221 (03) 789-794
- 19 Rajasekaran S, Vaccaro AR, Kanna RM, Schroeder GD, Oner FC, Vialle L. et al. The value of CT and MRI in the classification and surgical decision-making among spine surgeons in thoracolumbar spinal injuries. Eur Spine J 2017; 26 (05) 1463-1469
- 20 Hopkins BS, Weber II KA, Kesavabhotla K, Paliwal M, Cantrell DR, Smith ZA. Machine learning for the prediction of cervical spondylotic myelopathy: A post hoc pilot study of 28 participants. World Neurosurg 2019; 127: e436-e442
- 21 Jin R, Luk KD, Cheung JPY, Hu Y. Prognosis of cervical myelopathy based on diffusion tensor imaging with artificial intelligence methods. NMR Biomed 2019; 32 (08) e4114
- 22 Merali ZG, Witiw CD, Badhiwala JH, Wilson JR, Fehlings MG. Using a machine learning approach to predict outcome after surgery for degenerative cervical myelopathy. PLoS One 2019; 14 (04) e0215133




