

Subscribe to RSS
DOI: 10.1055/s-0044-1781459
Anal and Perianal Masses: The Common, the Uncommon, and the Rare
Authors
Funding None.


Abstract
A variety of tumors involve the anal canal because the anal canal forms the transition between the digestive system and the skin, and this anatomical region is made of a variety of different cells and tissues. Magnetic resonance imaging (MRI) is the modality of choice for diagnosis and local staging of the anal canal and perianal neoplasms. In this pictorial review, we demonstrate the MRI anatomy of the anal canal and perianal region and display the imaging spectrum of tumors in the region along with an overview of its management. Imaging appearances of many tumorlike lesions that can cause diagnostic dilemmas are also demonstrated with pointers to differentiate between them.
Introduction
The anal canal has a mixture of different coexisting types of cells and tissues, which predispose to the development of a wide variety of neoplasms. Squamous cell carcinomas (SCCs) are the most common anal canal carcinomas, accounting for 80% of all anal canal carcinomas.[1] The less common anal canal malignancies include adenocarcinoma and melanoma, which account for 15 and 4% cases, respectively. Lymphoma, neuroendocrine tumors (NETs), and mesenchymal neoplasms are even rarer in the anal canal. Tumors originating from the adjacent structures and organs can also secondarily involve the anal canal. These include lesions arising in the ischioanal fossa, vagina, vulva, urethra, and pelvic musculoskeletal system.
The perianal region refers to the skin surrounding a perimeter of 5 cm around the anal verge.[2] Tumors of the perianal region are at least five times less common than tumors of the anal canal.[1] Any cancer occurring in the skin elsewhere can occur in this region, with SCC being the most common. Less common neoplasms of perianal skin include verrucous carcinoma (VC), giant condyloma acuminatum (Buschke–Löwenstein tumor), basal cell carcinoma, Bowen's disease, and Paget's disease.
Although anal and perianal neoplasms can be clinically evaluated and biopsied easily, imaging with magnetic resonance imaging (MRI) is done to define the anatomical origin and the internal characteristics of the mass, and for staging.[2] Through this pictorial review, we demonstrate the anal canal and perianal anatomy on MRI and exhibit the imaging spectrum of tumors and tumorlike lesions in these regions. We also review the radiologist's role in staging and treatment planning of common neoplasms.
MR Imaging Technique
MR imaging performed with phased array coils provides excellent anatomical detail of the anal sphincters and the anatomical boundaries of the pelvis. High-resolution (HR) T2-weighted imaging (T2WI) in three orthogonal planes are the key sequences for knowing the extent of the lesion and proper assessment of the anal sphincter complex.[3] These are obtained with a slice thickness of 3 to 3.5 mm, with a small field of view (FOV) of 18 to 20 cm and high matrix (e.g., 320 × 256). Because of the forward tilt of the anal canal, the axial and coronal planes for HR imaging should be aligned orthogonal and parallel to the long axis of the anal canal, respectively ([Fig. 1]). Large FOV (covering the whole of the pelvis) T1 weighted imaging (T1WI), T1 fat-suppressed imaging, short tau inversion recovery (STIR) imaging, and diffusion weighted imaging (DWI) are other useful imaging sequences for disease characterization, determination of the extent of disease, and nodal spread. Intravenous gadolinium contrast may not be needed in most cases but can be used in selected cases to characterize uncommon lesions.

MRI Anatomy of Anal Region
The anal region includes the anal canal, anal verge (anus), and perianal skin ([Fig. 1]). The anal canal is the terminal part of the intestine that lies between the rectum above and the anal verge below.[2] The anorectal junction is at the superior limit of the puborectalis muscle, which forms a U-shaped sling around the superior portion of the anal canal. The anal verge is a band of squamous epithelial tissue that lacks hair follicles.[2] The anal canal has the following layers from inside-out: the mucosa, submucosa, and the sphincter muscles. An important landmark of the anal canal mucosa is the dentate line, which marks the junction of the endoderm-derived upper two-thirds and ectoderm-derived lower one-third of the anal canal.[2] The lining epithelium, the lymphatic and venous drainage, and nerve supply above and below the dentate line are hence different. The lining epithelium in the lower third of the anal canal is nonkeratinized squamous epithelium, that in the upper one-third is the columnar epithelium, and the middle third is a mix of both and is hence called the transitional zone.[2] The difference in lymphatic drainage above and below the dentate line will be seen in nodal spread of anal canal tumors. Tumors above the dentate line drain into the perirectal and internal iliac nodes, whereas tumors below the dentate line and the anal margin drain into the inguinal and femoral lymph nodes.[4]
Deep to the anal canal mucosa is the submucosa followed by two muscular layers, namely, the internal anal sphincter (IAS) and the external anal sphincter (EAS). The IAS is an involuntary muscle that is the thickened extension of the circular smooth muscle layer of the rectum. On MRI, IAS appears homogenous and moderately hyperintense on T2WI.[5] The EAS, which is a voluntary muscle, along with the puborectalis sling (PS), forms the outermost layer of the anal canal. The PS surrounds the upper third of the anal canal, while the EAS surrounds the lower two-thirds. According to the traditional description, EAS the is made of three muscle bundles, namely, deep, superficial, and subcutaneous bundles.[2] The deep bundle surrounds the middle two-thirds anal canal. The superficial bundle sweeps around and encircles the lower one-third of the anal canal. The subcutaneous bundle lies inferolateral to the IAS and beneath the anal verge. On MRI, the EAS complex has low signal intensity with “striated” appearance on T2WI. On HR T2WI, it may be possible to distinguish the three components of EAS. The dentate line, although not visible on MRI, is located at the level between the upper one-third and the lower two-thirds anal canal.[5] [6]
The perianal skin, also known as the anal margin, is the hair-bearing skin surrounding the anal verge for a radius of 5 cm2. The ischioanal fossa is a pyramid-shaped space situated on both sides of the anal sphincter complex with its base directed to the surface of the perineum and its apex directed anteromedially toward the pubic symphysis.[2] It is bounded superiorly by the levator ani muscle, medially by the EAS muscles, laterally by the obturator internus muscle and its fascia, and inferiorly by skin of the perineum.
Classification and Staging of Anal and Perianal Neoplasms
The World Health Organization (WHO) classifies tumors of the anal canal broadly into two categories: (1) benign epithelial tumors and precursors and (2) malignant epithelial tumors.[7] They are further divided based on the histologic type. Perianal tumors are classified just like skin tumors elsewhere.
Staging of cancers arising from both the anal canal and perianal regions is based on the 8th edition of the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) TNM (tumor size, node involvement, and metastasis status) classification ([Table 1]).[8] [9] The T stage is based on size of the lesion and not based on the depth of invasion. Regional lymph nodes for N staging include inguinal, mesorectal, superior rectal, internal iliac, and external iliac nodes.
Abbreviations: AJCC, American Joint Committee on Cancer; TNM, tumor size, node involvement, and metastasis status; UICC, Union for International Cancer Control.
Tumors Arising in the Anal Canal
Squamous Cell Carcinoma of the Anal Canal
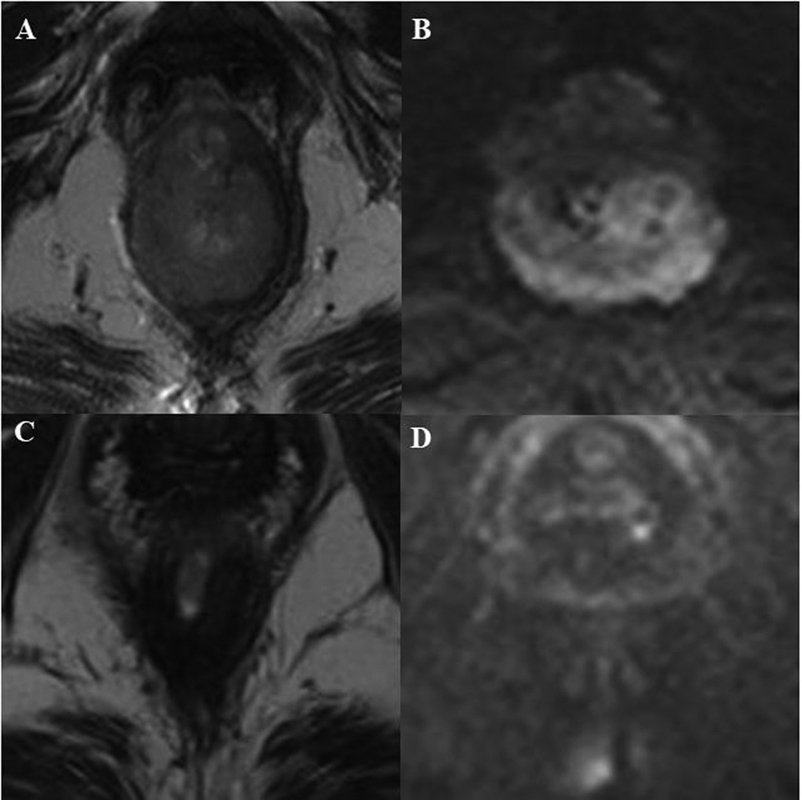
SCC is the most common neoplasm of the anal canal, accounting for nearly 80% of all neoplasms.[4] It can affect adults of any age group but peaks in sixth decade of life.[4] No gender predilection is seen. Human papillomavirus (HPV) infection (mainly HPV-16 and HPV-18 subtypes) and human immunodeficiency virus (HIV) infection remain the most common risk factors for anal SCC.[4] Some of the other known risk factors include cervical dysplasia, autoimmune disorders, immune suppression in transplant recipients, cigarette smoking, and long-standing perianal fistulizing Crohn's disease. Typical imaging appearance of SCC is as an infiltrative, usually circumferentially spreading lesion in the anal canal and the lower rectum, which is intermediate on T2WI and mildly hypointense on T1WI, and shows restricted diffusion ([Fig. 2]).[6] , Lymph node involvement, if present, is commonly seen at the inguinal, internal, and external iliac and mesorectal stations.[4] [8] Metastasis can occur to any organ, but the liver and lungs are most frequently involved.[4] [8]
Curative intent chemoradiotherapy (CRT) is the treatment of choice in most cases as it preserves the anal sphincter function.[6] Following CRT, response assessment is done with MRI or fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) 6 months after CRT.[10] [11] Complete response to CRT on MRI is indicated by loss of the bulk of the lesion with T2 hypointense signal without restricted diffusion replacing it, indicating posttreatment fibrosis ([Fig. 2]). There may be increased T2 signal intensity if there is edema, inflammation, and necrosis following treatment, which can mimic residual tumor. Kochhar et al have described “tram track” sign on post-CRT MRI scans, which is defined as parallel linear low signal at the inner and outer margins of the internal sphincter at the site of the original tumor.[10] This sign was present in more than half the patients studied at 6 months post-CRT and had a negative predictive value for early local relapse of 83%. Absence of residual metabolic activity (complete metabolic response) at posttreatment FDG-PET/CT suggests low risk of recurrence and longer progression-free survival.[11] Salvage surgery as abdominoperineal resection is reserved for incomplete responders to CRT.[6]
Adenocarcinoma of Anal Canal
Anal adenocarcinoma accounts for around 15% of all anal canal cancers.[12] Like SCC, it affects an adult of any age group with no gender predilection.[4] [12] However, it has a lower peak age than SCC, occurring at the fifth decade of life.[4] In the majority of the cases, they are rectal adenocarcinomas that extend to the anal canal. Adenocarcinomas arising from the anal gland are thought to be rare.[2] The differentiation between them is challenging, especially in large tumors where both anal and low rectal involvement is observed. The AJCC uses the anatomical location to differentiate between them. They recommend that if the epicenter of the tumor is located more than 2 cm proximal to the dentate line or proximal to the anorectal ring on digital examination, the tumor should be classified as rectal cancer. If the epicenter of the tumor is located ≤2 cm from the dentate line, the tumor should be classified as anal cancer.[8] TNM staging of rectal adenocarcinoma extending into the anal canal is like rectal carcinoma, while adenocarcinoma arising from the anal gland is similar to anal SCC.[8] The differentiation, however, has no relevant implication as their pathological characteristics and natural history are similar and hence they are managed similarly.[13] The European Society for Medical Oncology (ESMO) therefore includes all anorectal adenocarcinomas as low rectal cancer, if the distance from the anal verge to the lower margin of the tumor is less than 5 cm.[14]
Adenocarcinomas can be mucinous and nonmucinous.[15] Nonmucinous adenocarcinomas are the common subtype. They cannot be distinguished from SCCs of the anal canal and appear as an infiltrative, circumferentially spreading T2 intermediate lesion in the rectum and anal canal, and show restricted diffusion.[15] Mucinous adenocarcinomas are the less common subtype with worst prognosis and are defined as tumors with extracellular mucin greater than 50% of tumor volume. On MRI, mucinous tumors are characteristically T2 hyperintense lesions that show facilitated diffusion. Following contrast, it will show a lacelike peripheral contrast enhancement ([Fig. 3]).[15] Mucin has low attenuation at CT and usually will be false negative on PET examinations ([Fig. 3]). Mesorectal lymph node involvement is very common for adenocarcinomas, while inguinal, internal, and external iliac node involvements are less common.[4] Metastasis to the liver and lungs are most frequently observed.[4]

Imaging in restaging of adenocarcinomas with MRI is error prone because of difficulties in distinguishing residual cellular from acellular mucin and persistent tumor bulk despite potential treatment response.[16] Nonmucinous tumors can develop acellular mucin following neoadjuvant CRT, which is a good prognostic sign and indicates response.[17]
The standard of care for nonmetastatic anorectal adenocarcinoma is neoadjuvant long-course CRT followed by surgical resection.[17] Various abdominoperineal excision (APE) techniques are used for resection of low rectal/anal adenocarcinoma. They include standard APE, intersphincteric APE, and extralevator APE.[18] [19] The technique is chosen, depending on the accurate assessment of the anal sphincter involvement using an MRI-based low rectal cancer staging system ([Table 2]).[2] [5]
Abbreviations: MRI, magnetic resonance imaging.
Anal Melanoma
Anal melanoma is rare, comprising less than 1% of all melanomas and 4% of anal malignancies.[20] It commonly occurs in the elderly and has a slight female predominance. The lesion can be sessile or polypoidal in nature. Patients present with nonspecific symptoms of rectal bleeding, anal lump, and tenesmus.[21] On clinical examination, polypoidal melanoma of anal canal can be easily mistaken as a thrombosed hemorrhoid and often diagnosed only after pathologic examination of hemorrhoidectomy specimens. Around 70% of anal melanomas are pigmented and hence are called melanocytic melanomas, and the remaining are amelanotic melanomas.[20]
The imaging features of anal melanomas depend on the melanin content and the presence or absence of hemorrhage. Melanocytic melanomas demonstrate T1 and T2 shortening ([Fig. 4]), which is seen as T1 hyperintensity and T2 hypointensity, respectively, whereas amelanotic melanomas do not show substantial T1 or T2 shortening.[20] Most lesions show a homogenous enhancement pattern. The management of nonmetastatic disease is surgical, either with APE or wide local excision, followed by adjuvant chemotherapy, immunotherapy, radiation therapy, or a combination of these.[22]

Anal Neuroendocrine Neoplasms
Neuroendocrine neoplasms, formerly known as carcinoid tumors, are rare in the anal canal, occurring in individuals older than 50 years.[23] The new WHO classification of 2022 ([Table 3]) classifies them into NETs, if they are well differentiated, and as neuroendocrine carcinoma (NEC), if they are poorly differentiated.[24] They are further subclassified based on the number of mitoses, Ki-67 proliferation index, and cytomorphology. NETs, being well differentiated, have low cellular atypia and express neuroendocrine markers including chromogranin, synaptophysin, and hormones, while NECs with marked cellular atypia, frequent necrosis, and high proliferative activity will have variable and usually low sensitivity and specificity for the common neuroendocrine markers.[24] NECs can also have a coexisting conventional carcinoma (i.e., adenocarcinoma or SCC) in them. NETs of the anorectum are usually clinically asymptomatic unless metastatic, while NECs present with signs and symptoms of an aggressive neoplasm and often disseminated.[23]
On MRI, the lesions can be of varied morphology, from small submucosal nodule to large polypoidal ulcerating mass.[25] No specific MRI characteristics are present to differentiate them from other common cancers of the anal canal. Functional imaging with 68-Gallium DOTA peptide (DOTATOC, DOTATATE, DOTANOC) PET scan is used to stage NETs as they show high avidity.[25] NECs are commonly nonavid on 68 - Gallium DOTA PET imaging and hence FDG-PET/CT is the preferred modality for staging.
Surgery (endoscopic or open) remains the cornerstone of treatment of a localized neuroendocrine neoplasm. However, many patients develop metastases and require a multidisciplinary approach for optimal management.[23] [26] Chemotherapy is also recommended along with surgery, especially in cases of metastatic NET and in NEC.[23]
Lymphoma
Primary anorectal lymphomas account for only 3% of all gastrointestinal lymphomas and only approximately 0.1% of all anal malignancies.[16] HIV infection is a well-known risk factor due to the interplay between poor immune response and infection by oncologic viruses, especially Epstein–Barr virus (EBV) infection. The most common histologic subtype is diffuse large B-cell non-Hodgkin's lymphoma.[16]
At MRI, anal lymphoma usually appears as isointense on T1WI and intermediate signal on T2WI, solid mass causing focal and/or circumferential thickening of the anal canal ([Fig. 5]).[27] They also show restricted diffusion on DWI and mild postcontrast enhancement. FDG-PET/CT will show avid uptake and is the preferred modality for staging.

The treatment for anal lymphoma is not without confusion due to its rarity.[28] [29] Medical management with chemotherapy is considered the primary treatment for most cases.
Smooth Muscle Neoplasms
Common benign smooth muscle tumors include leiomyomas and myofibromas, while leiomyosarcomas (LMS) are malignant tumors.[21] [30] They originate from the muscularis mucosae or muscularis propria. These lesions, being submucosal in origin, show a submucosal bulge with normal overlying mucosa, unless the lesion is large and/or malignant.[31]
Both leiomyoma and myofibroma appear as smooth marginated and well-defined T2 mildly hypointense and T1 isointense lesions, which usually grow exophytically ([Fig. 6]).[21] [31] Myofibromas demonstrate intense postcontrast enhancement, whereas leiomyomas show mild to moderate homogenous enhancement. LMS, like leiomyomas, are exophytically growing lesions that are T1 isointense, but with irregular margins, heterogeneous on T2WI, and demonstrate a heterogeneous enhancement ([Fig. 7]).[21]


Surgical excision is the treatment of choice for benign lesions.[32] The mainstay treatment of LMS is surgery; however, neoadjuvant radiotherapy and adjuvant chemotherapy are recommended as they decrease local and distant recurrence and improve survival.[21]
Gastrointestinal Stromal Tumor
Anal gastrointestinal stromal tumors (GISTs) are rare (accounting for 5–10% of all GISTs), but are one of the most common mesenchymal tumors of the anal canal.[33] These tumors arise from the interstitial cells of Cajal in the myenteric plexus. The biologic behavior of these tumors is variable with the majority presenting with local disease only and less than 20% of patients develop distant metastases.[33] Aggressive lesions are usually greater than 5 cm in size, while lesions of size 2 to 5 cm have an intermediate risk profile and lesions less than 2 cm seem to remain consistently free of metastases.
On MRI, a GIST appears as a large smoothly marginated T1 iso- to hypointense and T2 hyperintense mass from the anal canal with a large exophytic component ([Fig. 8]).[33] Following contrast administration, larger tumors show central necrosis. Lymph node metastases are generally absent.

Surgery is the definitive curative treatment.[34] Imatinib mesylate, a tyrosine kinase inhibitor, is routinely used for unresectable tumors as neoadjuvant or salvage therapy.[34]
Malignancy Associated with Fistula-in-Ano
Malignancies associated with fistula-in-ano are rare. It can be due to a malignancy presenting as fistula-in-ano (malignancy first and fistula later) or malignancy developing within a chronic fistula (fistula first and malignancy later).[35] The former type is thought to be more common and occurs when the tumor blocks the opening of the anal gland resulting in formation of a perianal abscess and fistula.[35] The second type, where malignancy develops within a chronic fistula, is very rare with only a few reports in the literature. In 1934, Rosser et al[35] proposed the following three criteria to diagnose this entity: (1) the fistula should antedate the carcinoma by a minimum of 10 years, (2) the tumor should be the only tumor in the anorectum, and (3) the internal opening of the fistula should not be into the lesion. Tumors arising from such nonhealing fistulas are either adenocarcinomas or SCCs.[36]
MRI can easily identify cases of malignancy presenting as fistula-in-ano ([Fig. 9]). However, diagnosing malignancy developing within a fistula is challenging by imaging and has demonstrated low sensitivity unless in advanced stages.[36] The presence of focal wall thickening as T2 intermediate signal nodularity or enhancing soft tissue within a chronic fistula is suspicious for malignant transformation of a fistula ([Fig. 9]). The management guidelines for a malignancy developing in a fistula has not been established, and many times radical resection combined with chemo radiation is generally practiced.[36] [37]

Tumors Secondarily Involving anal Canal
Mesenchymal Tumors from Ischioanal Fossa
Mesenchymal tumors rarely can develop in the ischioanal fossa, arising from vascular, neural, muscular, fibrous, and fatty elements.[38] [Table 4] shows a simple classification of the ischioanal fossa tumors based on tissue of origin. Among them aggressive angiomyxoma is the most common primary tumor of ischioanal fossa and is discussed below. Lipomas and well-differentiated liposarcomas have predominant fatty components and can be diagnosed easily on imaging.[38] Most other tumors have nonspecific MRI features and may need biopsy for a definitive diagnosis.[38]
Abbreviations: PEComa, perivascular epithelioid cell tumor.
Aggressive Angiomyxoma
An aggressive angiomyxoma, although rare, is the most common tumor of the ischioanal fossa and has a predilection for females of reproductive age.[38] These tumors present as a painless mass that can sometimes cause local pressure on adjacent structures. They spread in multiple compartments without invading adjacent organs.[39]
MRI features are very typical ([Fig. 10]) and include iso- to hypointense signal intensity relative to the muscle on T1WI, and a characteristic “laminated” pattern on T2WI due to high signal intensity background myxoid stroma with low signal intensity parallel lines representing collagen fibrils. The lesion shows a heterogeneous postcontrast enhancement.[9]

The treatment of choice is wide surgical resection; however, due to infiltrative growth and poor circumscription, it is difficult to excise this tumor completely, resulting in high risk of local recurrences.[39]
Developmental Cysts
Congenital cysts, which can occur in the ischioanal fossa, include tailgut cyst, epidermoid cyst, and dermoid cysts. Differentiation among them may be possible based on imaging.[40]
Tailgut cysts are usually multicystic lesions with the locules having variable intensity due to the presence of mucin and blood ([Fig. 11]).[40] The signal intensity of mucinous fluid is variable and depends on protein concentration. As protein concentration increases, T1 signal intensity changes from hypointense to hyperintense, while T2 signal intensity shows inverse trend from hyperintense to hypointense signals. Tailgut cysts can be complicated by infection and on rare occasions by malignant transformation. Malignant transformation is suspected when there is focal irregular wall thickening with enhancement.[40]

Epidermoid and dermoid cysts are often unilocular cysts lined by a stratified squamous epithelium.[40] Epidermoid cysts contain a mixture of desquamated debris, cholesterol, keratin, and water, but it lacks the skin appendages such as sweat glands, hair follicles, and sebaceous glands, which are seen in dermoid cysts. On MRI, epidermoid cysts are unilocular thin-walled cysts with low signal intensity on T1WI and high signal intensity on T2WI, and may contain multiple T2 hypointense debris representing aggregates of keratin ([Fig. 11]).[38] Dermoid cysts are similar to epidermoid cysts except that they can have fat components within. Loss of signal intensity in these cysts on out-phase images as opposed to in-phase images confirms their fatty nature.[40]
These cysts, if symptomatic, may need surgical excision.
Secondary Neoplasms from Adjacent Structures
Secondary tumors arising in the vagina, vulva, urethra, and pelvic musculoskeletal system can involve the anal canal. Cancer of the vagina, if it involves the mucosa of the anorectum, is considered T4 according to the eighth edition of the TNM (2018) classification and stage IVa on the International Federation of Gynecology and Obstetrics (FIGO) staging.[8] Vulval cancer with extension to the anal canal is T2 according to the eighth edition of the TNM (2018) staging and stage II according to FIGO stage.[8] Urethral cancer (in both males and females) if fixed or invading the sphincter of the anal canal is T4 according to the eighth edition of the TNM (2018) staging.[8]
Perianal Neoplasms
Bowen's Disease
Bowen's disease is an intraepithelial SCC that occurs most frequently on the face, hands, and trunk, and less commonly in the perianal region.[41] In the perianal region, it probably represents severe anal intraepithelial neoplasia (AIN) and is associated with HPV-16 and HPV-18 infections.[40] Like anal canal SCCs, Bowen's disease is much more common in patients with HIV.[41] In 2 to 6% of cases, the disease progress to an invasive SCC. Bowen's disease has the highest incidence during the sixth and seventh decades of life.[41] Common symptoms include itching, burning, and occasionally bleeding, and on examination, the lesion appears as a well-defined erythematous, scaly plaque.[41] Diagnosis is made by obtaining several full-thickness biopsy from the central portion and edges of the lesion. Imaging is generally not done. The treatment of choice is wide local excision.[41]
Perianal Paget's Disease
Perianal Paget's disease is quite an uncommon intraepithelial adenocarcinoma arising from the dermal apocrine sweat glands and can be associated with underlying apocrine or eccrine carcinoma, colorectal adenocarcinoma, and anal carcinoma in 38 to 69% of patients.[41] It is most commonly found in older patients, averaging 66 years, and shows a preponderance for women. The lesions are erythematous and crusty, eczematoid, or scaly appearing, and present with nonspecific symptoms like pain, bleeding, and itching.[41] Diagnosis is made with full-thickness biopsies of the affected skin. FDG-PET/CT or MRI is done before treatment to exclude associated underlying malignancy.[41] If the disease appears to be locally confined on preoperative workup and is noninvasive on biopsy, wide local excision is the treatment of choice. When the tumor is invasive or located close to the anal canal, and sufficient surgical margin cannot be achieved, a combined modality treatment with chemoradiation may be needed.[41] If underlying malignancy is identified, it will also require appropriate treatment.
Squamous Cell Carcinoma of Perianal Skin
Perianal SCCs are at least five times less common than cancers of the anal canal and have a more favorable prognosis as they are typically well differentiated, slow growing, and without distant metastases.[41] The risk factors for perianal SCC are the same as for SCCs of the anal canal.[41] Most patients present after the fifth decade with an approximately equal male-to-female predominance.[41] Symptoms of perianal SCC are nonspecific and include bleeding, pain, discharge, and pruritus. On examination, they are usually hard, raised, and ulcerated skin lesions with rolled, everted edges.[41] The anal canal can become involved late in the disease, although the sphincter complex is rarely invaded. A VC is a rare histologic subtype of SCC characterized by highly differentiated squamous cells and appears as a large locally aggressive tumor with a cauliflowerlike appearance.[42] It is often associated and confused with a giant condyloma acuminatum (GCA), also called Buschke–Löwenstein tumor due to similar clinical and imaging appearance. A GCA has been linked to HPV, whereas a VC is negative for HPV.[42] On histological evaluation, VCs have no koilocytic atypia, whereas GCAs have koilocytic atypia.[42] On the other hand, distinguishing VCs from conventional SCCs is also important because, although large and in some cases locally aggressive, VCs are often amenable to wide local resection since nodal metastases are extremely rare. However, there are published reports showing that VCs and conventional SCCs can coexist in the same lesion.[41]
Any patient with a suspicious lesion needs biopsy for definitive diagnosis. Pretreatment evaluation should include a full staging workup with imaging.[41] MRI of the pelvis can demonstrate the extent of lesion, anal canal involvement, and regional nodes ([Fig. 12]). VCs on MRI appear as T2 hyperintense cauliflowerlike lesion from the perianal skin ([Fig. 13]).[43]


Perianal SCCs are generally treated as skin cancers with wide local excision.[41] Lesions involving the anal canal needs combined modality of chemoradiation as initial treatment approach followed by salvage surgery if recurrent or residual disease is present.[41] VCs are also treated with wide local excision; however, high recurrence rates (as high as 66%) after excision have prompted the use of neoadjuvant or adjuvant chemoradiation therapy.[41]
Tumorlike Lesions
Prolapsed Hemorrhoids
Hemorrhoids are vascular cushions surrounding the anastomoses between the superior rectal artery and the superior, middle, and inferior rectal veins.[44] Internal hemorrhoids arise above the dentate line and external hemorrhoids arise below the dentate line. External hemorrhoids are innervated by somatic nerves and cause pain, whereas internal hemorrhoids are innervated by visceral nerve fibers and are painless. Most hemorrhoids are a combined type of internal and external hemorrhoids.[44] Hemorrhoidal disease is commonly diagnosed on clinical examination but can also be seen on MRI. On T2WI, hemorrhoids are seen as moderately hyperintense polypoidal lesion. They may also show increased signal on T1WI ([Fig. 14]).[45]

Vascular Malformations
Rectal bleeding is the most common presentation in vascular malformation (VM) and can mimic neoplasms. Colonoscopy in such cases may reveal nodular submucosal tumorlike lesion in the anorectum with normal or edematous overlying mucosa.[46] They can also be divided into high- and low-flow lesions.[46] High-flow lesions should have an arterial component. MRI can help in diagnosing VM and help in defining its extent.[46] Low-flow malformations have cluster of cystic spaces with or without fluid debris layer ([Fig. 14]), whereas high-flow malformations contain signal voids. On dynamic postcontrast MRI, high-flow lesions show rapid filling, whereas low-flow lesions show late filling. Calcification and phleboliths can be mistaken as flow void; however, they appear as focal signal void and are not tortuous as flow void. In case of doubt in differentiating them on MRI, a noncontrast CT can be done to identify calcification.
Endometriosis
Perianal endometriosis is extremely rare. It usually occurs in childbearing women following obstetric or gynecological procedures most commonly following delivery at episiotomy scar.[47] A patient typically presents with cyclical pain. Many times, the diagnosis may not be made on physical examination, and MRI may be needed.[48] On MRI ([Fig. 14]), endometriosis manifests as a nodular or plaquelike lesion with intermediate signal intensity on T1WI and low signal intensity on T2WI. Small T2 and T1 hyperintense foci corresponding to endometrial glands and hemorrhagic foci are almost always recognized within the endometriotic lesions.[48]
Infections
A typical fistula-in-ano is mostly an idiopathic process thought to be caused by obstruction of anal glands and its diagnosis via an MRI is straightforward due to the presence of well-defined fluid contained tracts. Perianal infection in immunosuppressed patients with hematological malignancy is atypical on MRI as they have extensive anal and perianal edema and rarely have defined fistula tracts, creating confusing imaging appearance ([Fig. 14]).[32]
Common infections of the anorectum includes nonsexually transmitted infections due to Escherichia coli, Shigella spp., Campylobacter spp., and Clostridium difficile, and sexually transmitted infections due to Neisseria gonorrhoeae, Chlamydia trachomatis, Treponema pallidum, and herpes simplex virus (HSV).[49] Most of these infections do no need imaging for diagnosis and if done may show nonspecific anorectal inflammation.
Inflammatory Phlegmon
A fistula-in-ano is commonly complicated by abscesses and ramifications. Atypical findings of solid enhancing masslike lesions with no fluid component can represent inflammatory phlegmon in partly treated fistulas and can mimic a malignancy developing in chronic fistulas ([Fig. 14]).[50] If differentiating them is not possible on imaging, tissue sampling needs to be done to confirm the difference.
Clues to Differential Diagnosis and Algorithmic Approach
A stepwise algorithmic approach to diagnose anal and perianal lesions based on imaging is highlighted in [Fig. 15].

Conclusion
In this article, we showed a plethora of pathological conditions in the anal and perianal region. MRI is the modality of choice for assessing the extent of anal and perianal lesions. Some tumors have characteristic imaging findings that may permit accurate diagnosis; however, tissue sampling is often needed to confirm the diagnosis. Accurate diagnosis needs good knowledge of anal and perianal anatomy as well as knowledge of the spectrum of imaging findings of common and uncommon neoplasms.
Conflict of Interest
None declared.
Note
A part of this article including images were presented as electronic poster with the same title during the 33rd Annual Meeting and Postgraduate Course of European Society of Gastrointestinal and Abdominal Radiology (ESGAR), 2022, and was selected as a recommended poster.
-
References
- 1 Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin 2022; 72 (01) 7-33
- 2 Solan P, Davis B. Anorectal anatomy and imaging techniques. Gastroenterol Clin North Am 2013; 42 (04) 701-712
- 3 Brown G, Daniels IR, Richardson C, Revell P, Peppercorn D, Bourne M. Techniques and trouble-shooting in high spatial resolution thin slice MRI for rectal cancer. Br J Radiol 2005; 78 (927) 245-251
- 4 Chandramohan A. et al. MRI staging of anorectal malignancy—a reporting dilemma: is it adenocarcinoma or squamous cell carcinoma?. J Gastrointestinal Abdominal Radiol 2023; 6: 136-145
- 5 deSouza NM, Williams AD, Gilderdale DJ. High-resolution magnetic resonance imaging of the anal sphincter using a dedicated endoanal receiver coil. Eur Radiol 1999; 9 (03) 436-443
- 6 Kochhar R, Plumb AA, Carrington BM, Saunders M. Imaging of anal carcinoma. AJR Am J Roentgenol 2012; 199 (03) W335-W344
- 7 World Health Organization Classification of Tumours Editorial Board. WHO Classification of Tumours. Vol. 1: Digestive System Tumours. Lyon:: IARC; 2019
- 8 Amin MB, Edge SB, Greene FL. et al, eds. AJCC Cancer Staging Manual. 8th ed. New York, NY:: Springer International Publishing;; 2017
- 9 Surabhi VR, Menias CO, Amer AM. et al. Tumors and tumorlike conditions of the anal canal and perianal region: MR imaging findings. Radiographics 2016; 36 (05) 1339-1353
- 10 Kochhar R, Renehan AG, Mullan D, Chakrabarty B, Saunders MP, Carrington BM. The assessment of local response using magnetic resonance imaging at 3- and 6-month post chemoradiotherapy in patients with anal cancer. Eur Radiol 2017; 27 (02) 607-617
- 11 Jones M, Hruby G, Solomon M, Rutherford N, Martin J. The role of FDG-PET in the initial staging and response assessment of anal cancer: a systematic review and meta-analysis. Ann Surg Oncol 2015; 22 (11) 3574-3581
- 12 Tarazi R, Nelson RL. Anal adenocarcinoma: a comprehensive review. Semin Surg Oncol 1994; 10 (03) 235-240
- 13 Benson AB, Venook AP, Al-Hawary MM. et al. Anal carcinoma, Version 2.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2018; 16 (07) 852-871
- 14 Rao S, Guren MG, Khan K. et al; ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Anal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up☆ . Ann Oncol 2021; 32 (09) 1087-1100
- 15 Hussain SM, Outwater EK, Siegelman ES. Mucinous versus nonmucinous rectal carcinomas: differentiation with MR imaging. Radiology 1999; 213 (01) 79-85
- 16 Ambrosio MR, Rocca BJ, Barone A. et al. Primary anorectal Hodgkin lymphoma: report of a case and review of the literature. Hum Pathol 2014; 45 (03) 648-652
- 17 Horvat N, Rocha CCT, Oliveira BC, Petkovska I, Gollub MJ. MRI of rectal cancer: tumor staging, imaging techniques, and management. Radiographics 2019; 39 (02) 367-387
- 18 Valadão M, Câmara ERZ, de Castro Araujo RO. et al. Low rectal cancer: current approach based on magnetic resonance imaging. BJ Oncology 2017; 13 (45) 1-5
- 19 Santiago I, Figueiredo N, Parés O, Matos C. MRI of rectal cancer-relevant anatomy and staging key points. Insights Imaging 2020; 11 (01) 100
- 20 Park HJ, Kim HJ, Park SH. et al. Journal Club: primary anorectal melanoma: MRI findings and clinicopathologic correlations. AJR Am J Roentgenol 2018; 211 (02) W98-W108
- 21 Nassif MO, Habib RA, Almarzouki LZ, Trabulsi NH. Systematic review of anorectal leiomyosarcoma: current challenges and recent advances. World J Gastrointest Surg 2019; 11 (08) 334-341
- 22 Matsuda A, Miyashita M, Matsumoto S. et al. Abdominoperineal resection provides better local control but equivalent overall survival to local excision of anorectal malignant melanoma: a systematic review. Ann Surg 2015; 261 (04) 670-677
- 23 Ueberroth BE, Liu AJ, Starr JS. et al. Neuroendocrine carcinoma of the anus and rectum: patient characteristics and treatment options. Clin Colorectal Cancer 2021; 20 (02) e139-e149
- 24 Rindi G, Mete O, Uccella S. et al. Overview of the 2022 WHO classification of neuroendocrine neoplasms. Endocr Pathol 2022; 33 (01) 115-154
- 25 Ganeshan D, Bhosale P, Yang T, Kundra V. Imaging features of carcinoid tumors of the gastrointestinal tract. AJR Am J Roentgenol 2013; 201 (04) 773-786
- 26 Juhlin CC, Falhammar H, Kjellman M, Åhlén J, Welin S, Calissendorff J. Highly proliferative anal neuroendocrine carcinoma: molecular and clinical features of a rare, recurrent case in complete remission. BMC Gastroenterol 2020; 20 (01) 290
- 27 Schwenzer NF, Pfannenberg AC. PET/CT, MR, and PET/MR in lymphoma and melanoma. Semin Nucl Med 2015; 45 (04) 322-331
- 28 Rubinstein PG, Aboulafia DM, Zloza A. Malignancies in HIV/AIDS: from epidemiology to therapeutic challenges. AIDS 2014; 28 (04) 453-465
- 29 Cuffy M, Abir F, Longo WE. Management of less common tumors of the colon, rectum, and anus. Clin Colorectal Cancer 2006; 5 (05) 327-337
- 30 Kusminsky RE, Bailey W. Leiomyomas of the rectum and anal canal: report of six cases and review of the literature. Dis Colon Rectum 1977; 20 (07) 580-599
- 31 Kim H, Kim JH, Lim JS. et al. MRI findings of rectal submucosal tumors. Korean J Radiol 2011; 12 (04) 487-498
- 32 Haliloglu N, Gulpinar B, Ozkavukcu E, Erden A. Typical MR imaging findings of perianal infections in patients with hematologic malignancies. Eur J Radiol 2017; 93: 284-288
- 33 Koch MR, Jagannathan JP, Shinagare AB. et al. Imaging features of primary anorectal gastrointestinal stromal tumors with clinical and pathologic correlation. Cancer Imaging 2013; 12 (03) 557-565
- 34 Hassan I, You YN, Shyyan R. et al. Surgically managed gastrointestinal stromal tumors: a comparative and prognostic analysis. Ann Surg Oncol 2008; 15 (01) 52-59
- 35 Kline RJ, Spencer RJ, Harrison Jr. EG. Carcinoma associated with fistula-in-ano. Arch Surg 1964; 89 (06) 989-994
- 36 Chandramohan K, Mathew AP, Muralee M, Anila KR, Ramachandran K, Ahamed I. Squamous cell carcinoma arising from long-standing perianal fistula. Int Wound J 2010; 7 (06) 515-518
- 37 Yang B-L, Shao W-J, Sun G-D, Chen Y-Q, Huang J-C. Perianal mucinous adenocarcinoma arising from chronic anorectal fistulae: a review from single institution. Int J Colorectal Dis 2009; 24 (09) 1001-1006
- 38 Faria SC, Elsherif SB, Sagebiel T. et al. Ischiorectal fossa: benign and malignant neoplasms of this “ignored” radiological anatomical space. Abdom Radiol (NY) 2019; 44 (05) 1644-1674
- 39 Hajjar R, Alharthi M, Richard C, Gougeon F, Loungnarath R. Pelvic aggressive angiomyxoma: major challenges in diagnosis and treatment. Cureus 2019; 11 (04) e4419
- 40 Loock MT, Fornès P, Soyer P, Rousset P, Azizi L, Hoeffel C. MR imaging features of nongynaecologic cystic lesions of the pelvis. Clin Imaging 2013; 37 (02) 211-218
- 41 Jiang Y, Ajani JA. Anal margin cancer: current situation and ongoing trials. Curr Opin Oncol 2012; 24 (04) 448-453
- 42 Bambao C, Nofech-Mozes S, Shier M. Giant condyloma versus verrucous carcinoma: a case report. J Low Genit Tract Dis 2010; 14 (03) 230-233
- 43 Takezawa Y, Shimizu N, Kurokawa K, Suzuki K, Yamanaka H. Appearance on magnetic resonance imaging of Buschke-Lowenstein tumour. Br J Urol 1996; 78 (02) 308-309
- 44 Rubbini M, Ascanelli S. Classification and guidelines of hemorrhoidal disease: Present and future. World J Gastrointest Surg 2019; 11 (03) 117-121
- 45 Erden A. MRI of anal canal: common anal and perianal disorders beyond fistulas: part 2. Abdom Radiol (NY) 2018; 43 (06) 1353-1367
- 46 Erdemli S, Aris D, Çiçek B. et al. Revisiting imaging features of rectosigmoid vascular malformation with emphasis on multiparametric MRI: a case report. Egypt J Radiol Nucl Med 2022; 53: 173
- 47 Chen N, Zhu L, Lang J. et al. The clinical features and management of perineal endometriosis with anal sphincter involvement: a clinical analysis of 31 cases. Hum Reprod 2012; 27 (06) 1624-1627
- 48 Lorusso F, Scioscia M, Rubini D. et al. Magnetic resonance imaging for deep infiltrating endometriosis: current concepts, imaging technique and key findings. Insights Imaging 2021; 12 (01) 105
- 49 de Vries HJC, Nori AV, Kiellberg Larsen H. et al. 2021 European guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens. J Eur Acad Dermatol Venereol 2021; 35 (07) 1434-1443
- 50 Dsouza RG, Al Rasheed MRH, Low G. Perianal inflammation or something more?. J Clin Imaging Sci 2021; 11: 47
Address for correspondence
Publication History
Article published online:
23 March 2024
© 2024. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin 2022; 72 (01) 7-33
- 2 Solan P, Davis B. Anorectal anatomy and imaging techniques. Gastroenterol Clin North Am 2013; 42 (04) 701-712
- 3 Brown G, Daniels IR, Richardson C, Revell P, Peppercorn D, Bourne M. Techniques and trouble-shooting in high spatial resolution thin slice MRI for rectal cancer. Br J Radiol 2005; 78 (927) 245-251
- 4 Chandramohan A. et al. MRI staging of anorectal malignancy—a reporting dilemma: is it adenocarcinoma or squamous cell carcinoma?. J Gastrointestinal Abdominal Radiol 2023; 6: 136-145
- 5 deSouza NM, Williams AD, Gilderdale DJ. High-resolution magnetic resonance imaging of the anal sphincter using a dedicated endoanal receiver coil. Eur Radiol 1999; 9 (03) 436-443
- 6 Kochhar R, Plumb AA, Carrington BM, Saunders M. Imaging of anal carcinoma. AJR Am J Roentgenol 2012; 199 (03) W335-W344
- 7 World Health Organization Classification of Tumours Editorial Board. WHO Classification of Tumours. Vol. 1: Digestive System Tumours. Lyon:: IARC; 2019
- 8 Amin MB, Edge SB, Greene FL. et al, eds. AJCC Cancer Staging Manual. 8th ed. New York, NY:: Springer International Publishing;; 2017
- 9 Surabhi VR, Menias CO, Amer AM. et al. Tumors and tumorlike conditions of the anal canal and perianal region: MR imaging findings. Radiographics 2016; 36 (05) 1339-1353
- 10 Kochhar R, Renehan AG, Mullan D, Chakrabarty B, Saunders MP, Carrington BM. The assessment of local response using magnetic resonance imaging at 3- and 6-month post chemoradiotherapy in patients with anal cancer. Eur Radiol 2017; 27 (02) 607-617
- 11 Jones M, Hruby G, Solomon M, Rutherford N, Martin J. The role of FDG-PET in the initial staging and response assessment of anal cancer: a systematic review and meta-analysis. Ann Surg Oncol 2015; 22 (11) 3574-3581
- 12 Tarazi R, Nelson RL. Anal adenocarcinoma: a comprehensive review. Semin Surg Oncol 1994; 10 (03) 235-240
- 13 Benson AB, Venook AP, Al-Hawary MM. et al. Anal carcinoma, Version 2.2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2018; 16 (07) 852-871
- 14 Rao S, Guren MG, Khan K. et al; ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Anal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up☆ . Ann Oncol 2021; 32 (09) 1087-1100
- 15 Hussain SM, Outwater EK, Siegelman ES. Mucinous versus nonmucinous rectal carcinomas: differentiation with MR imaging. Radiology 1999; 213 (01) 79-85
- 16 Ambrosio MR, Rocca BJ, Barone A. et al. Primary anorectal Hodgkin lymphoma: report of a case and review of the literature. Hum Pathol 2014; 45 (03) 648-652
- 17 Horvat N, Rocha CCT, Oliveira BC, Petkovska I, Gollub MJ. MRI of rectal cancer: tumor staging, imaging techniques, and management. Radiographics 2019; 39 (02) 367-387
- 18 Valadão M, Câmara ERZ, de Castro Araujo RO. et al. Low rectal cancer: current approach based on magnetic resonance imaging. BJ Oncology 2017; 13 (45) 1-5
- 19 Santiago I, Figueiredo N, Parés O, Matos C. MRI of rectal cancer-relevant anatomy and staging key points. Insights Imaging 2020; 11 (01) 100
- 20 Park HJ, Kim HJ, Park SH. et al. Journal Club: primary anorectal melanoma: MRI findings and clinicopathologic correlations. AJR Am J Roentgenol 2018; 211 (02) W98-W108
- 21 Nassif MO, Habib RA, Almarzouki LZ, Trabulsi NH. Systematic review of anorectal leiomyosarcoma: current challenges and recent advances. World J Gastrointest Surg 2019; 11 (08) 334-341
- 22 Matsuda A, Miyashita M, Matsumoto S. et al. Abdominoperineal resection provides better local control but equivalent overall survival to local excision of anorectal malignant melanoma: a systematic review. Ann Surg 2015; 261 (04) 670-677
- 23 Ueberroth BE, Liu AJ, Starr JS. et al. Neuroendocrine carcinoma of the anus and rectum: patient characteristics and treatment options. Clin Colorectal Cancer 2021; 20 (02) e139-e149
- 24 Rindi G, Mete O, Uccella S. et al. Overview of the 2022 WHO classification of neuroendocrine neoplasms. Endocr Pathol 2022; 33 (01) 115-154
- 25 Ganeshan D, Bhosale P, Yang T, Kundra V. Imaging features of carcinoid tumors of the gastrointestinal tract. AJR Am J Roentgenol 2013; 201 (04) 773-786
- 26 Juhlin CC, Falhammar H, Kjellman M, Åhlén J, Welin S, Calissendorff J. Highly proliferative anal neuroendocrine carcinoma: molecular and clinical features of a rare, recurrent case in complete remission. BMC Gastroenterol 2020; 20 (01) 290
- 27 Schwenzer NF, Pfannenberg AC. PET/CT, MR, and PET/MR in lymphoma and melanoma. Semin Nucl Med 2015; 45 (04) 322-331
- 28 Rubinstein PG, Aboulafia DM, Zloza A. Malignancies in HIV/AIDS: from epidemiology to therapeutic challenges. AIDS 2014; 28 (04) 453-465
- 29 Cuffy M, Abir F, Longo WE. Management of less common tumors of the colon, rectum, and anus. Clin Colorectal Cancer 2006; 5 (05) 327-337
- 30 Kusminsky RE, Bailey W. Leiomyomas of the rectum and anal canal: report of six cases and review of the literature. Dis Colon Rectum 1977; 20 (07) 580-599
- 31 Kim H, Kim JH, Lim JS. et al. MRI findings of rectal submucosal tumors. Korean J Radiol 2011; 12 (04) 487-498
- 32 Haliloglu N, Gulpinar B, Ozkavukcu E, Erden A. Typical MR imaging findings of perianal infections in patients with hematologic malignancies. Eur J Radiol 2017; 93: 284-288
- 33 Koch MR, Jagannathan JP, Shinagare AB. et al. Imaging features of primary anorectal gastrointestinal stromal tumors with clinical and pathologic correlation. Cancer Imaging 2013; 12 (03) 557-565
- 34 Hassan I, You YN, Shyyan R. et al. Surgically managed gastrointestinal stromal tumors: a comparative and prognostic analysis. Ann Surg Oncol 2008; 15 (01) 52-59
- 35 Kline RJ, Spencer RJ, Harrison Jr. EG. Carcinoma associated with fistula-in-ano. Arch Surg 1964; 89 (06) 989-994
- 36 Chandramohan K, Mathew AP, Muralee M, Anila KR, Ramachandran K, Ahamed I. Squamous cell carcinoma arising from long-standing perianal fistula. Int Wound J 2010; 7 (06) 515-518
- 37 Yang B-L, Shao W-J, Sun G-D, Chen Y-Q, Huang J-C. Perianal mucinous adenocarcinoma arising from chronic anorectal fistulae: a review from single institution. Int J Colorectal Dis 2009; 24 (09) 1001-1006
- 38 Faria SC, Elsherif SB, Sagebiel T. et al. Ischiorectal fossa: benign and malignant neoplasms of this “ignored” radiological anatomical space. Abdom Radiol (NY) 2019; 44 (05) 1644-1674
- 39 Hajjar R, Alharthi M, Richard C, Gougeon F, Loungnarath R. Pelvic aggressive angiomyxoma: major challenges in diagnosis and treatment. Cureus 2019; 11 (04) e4419
- 40 Loock MT, Fornès P, Soyer P, Rousset P, Azizi L, Hoeffel C. MR imaging features of nongynaecologic cystic lesions of the pelvis. Clin Imaging 2013; 37 (02) 211-218
- 41 Jiang Y, Ajani JA. Anal margin cancer: current situation and ongoing trials. Curr Opin Oncol 2012; 24 (04) 448-453
- 42 Bambao C, Nofech-Mozes S, Shier M. Giant condyloma versus verrucous carcinoma: a case report. J Low Genit Tract Dis 2010; 14 (03) 230-233
- 43 Takezawa Y, Shimizu N, Kurokawa K, Suzuki K, Yamanaka H. Appearance on magnetic resonance imaging of Buschke-Lowenstein tumour. Br J Urol 1996; 78 (02) 308-309
- 44 Rubbini M, Ascanelli S. Classification and guidelines of hemorrhoidal disease: Present and future. World J Gastrointest Surg 2019; 11 (03) 117-121
- 45 Erden A. MRI of anal canal: common anal and perianal disorders beyond fistulas: part 2. Abdom Radiol (NY) 2018; 43 (06) 1353-1367
- 46 Erdemli S, Aris D, Çiçek B. et al. Revisiting imaging features of rectosigmoid vascular malformation with emphasis on multiparametric MRI: a case report. Egypt J Radiol Nucl Med 2022; 53: 173
- 47 Chen N, Zhu L, Lang J. et al. The clinical features and management of perineal endometriosis with anal sphincter involvement: a clinical analysis of 31 cases. Hum Reprod 2012; 27 (06) 1624-1627
- 48 Lorusso F, Scioscia M, Rubini D. et al. Magnetic resonance imaging for deep infiltrating endometriosis: current concepts, imaging technique and key findings. Insights Imaging 2021; 12 (01) 105
- 49 de Vries HJC, Nori AV, Kiellberg Larsen H. et al. 2021 European guideline on the management of proctitis, proctocolitis and enteritis caused by sexually transmissible pathogens. J Eur Acad Dermatol Venereol 2021; 35 (07) 1434-1443
- 50 Dsouza RG, Al Rasheed MRH, Low G. Perianal inflammation or something more?. J Clin Imaging Sci 2021; 11: 47