
Subscribe to RSS
DOI: 10.1055/s-0044-1787131
Locking Volar Plate in Distal Radius Fractures: Minimally Invasive Technique versus Conventional Technique
Article in several languages: español | English
Abstract
Introduction In recent years, surgery has gained relevance in the treatment of distal radius fractures (DRF). Among the surgical techniques, minimally-invasive plate osteosynthesis (MIPO) is becoming popular, and its indications are increasing compared to the conventional technique.
Material and Methods A retrospective study that included 81 patients who went through surgery for DRF during 2021, corresponding to fractures of types I, II, and III in the Fernández classification. Radiological, clinical, and functional results, as well as the appearance of complications, were compared at the end of the 6-month follow-up.
Results The MIPO group was composed of 21 patients (8 men and 13 women) with a mean age of 57.3 years, and the conventional group, 60 patients (11 men and 49 women) with a mean age of 60.8 years. The Castaing Radiological Scale showed a favorable overall result for the MIPO technique compared to the conventional technique (p = 0.049), with statistically significance for the MIPO group in terms of sagittal/volar inclination (10.5 vs. 7.3°; p = 0.0006). The Visual Analogue Scale (VAS) yielded a result of 1.5 for the MIPO technique and of 2.9 for the conventional technique (p = 0.0141). The score on the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) questionnaire was slightly higher in the MIPO group (13.5%) compared to the conventional group (19.6%), but it was not statistically significant. Similar results were found for the range of motion (ROM), except for pronation and grip strength, which were favorable for the MIPO group. Complications, including nerve injury, chronic pain, tendon injury, and esthetic sequelae, were higher in percentage with the conventional technique.
Conclusion For the treatment of DRF, the MIPO technique, using an extra-short plate through a biological approach, can achieve functional results at least as good as those achieved with the conventional technique, with better radiological results, lower levels of postoperative pain, a lower rate of complications, and better esthetic results.
#
Introduction and Objective
Distal radius fractures (DRFs) represent 17.5% of all fractures;[1] their incidence is of 125 per 10 thousand people per year,[2] and it is estimated that this figure will double over the next 25 years. They present a bimodal distribution depending on the age at which they occur: firstly, during childhood, because bone growth exceeds its own mineralization capacity; and, secondly, in people older than 50 years of age, predominantly postmenopausal women around 65 years of age, due to osteoporosis.[2] [3]
There are multiple studies that compare the conservative and the surgical treatments of DRF; however, there is no consensus on its management.[4] [5] [6] Currently, surgery as an initial treatment is gaining relevance compared to the conservative management.[7] [8] [9] [10] One of the main reasons for the increase in the number of surgeries is the aging of society, and age is not a contraindication for surgical treatment of DRF.[11] There are different methods, such as Kirschner wires, open reduction and internal fixation (ORIF), or the use of an external fixator. The ORIF method enables early recovery and yields better clinical and functional results compared to the others, because it achieves a better anatomical reduction of the fracture.[12] [13] [14]
On the other hand, open reduction presents certain disadvantages, such as: disinsertion of the pronator quadratus, damage to soft tissues, and deperiostization and devascularization of the fracture.[15] As a solution to these drawbacks, the minimally-invasive plate osteosynthesis (MIPO) technique and its biological approach are receiving increasing attention. There are several benefits in preserving the pronator quadratus, such as conservation of strength and range of pronation, greater and better coverage of the osteosynthesis material, respecting the vascularization of the fracture fragments through the anterior interosseous artery, which runs through the pronator quadratus, and provide greater stability to the distal radioulnar joint while preserving the deep fascicle of said muscle.[16] [17] [18] [19]
The level of evidence on which the surgeon can rely to choose the MIPO technique over the conventional technique is low. Several authors[20] [21] [22] [23] [24] [25] [26] [27] have studied and compared both techniques: some of them show favorable results for the MIPO technique, while others do not find significant differences.
The ideal implant designed specifically for minimally-invasive surgery is one that provides and facilitates the surgeon a rapid learning curve without a significant lengthening of operative time. The design of the extra-short plate used in the MIPO group, with the distal screws in a divergent position, which results in the use of fewer screws, as well as its implantation technique, provides great safety and comfort to the surgeon for the internal fixation of the DRF.
Regarding our objectives in the present study, the first is to present the technique and the advantages of a biological approach compared to the conventional approach for DRFs. The second objective is to demonstrate that the extra-short volar locked plate used in the MIPO technique; smaller in size and with fewer holes, it has the capacity to achieve radiographic indices at least similar to those achieved with the usual plates, without losing fracture reduction during follow-up. The third objective is to compare both techniques regarding clinical results and patient satisfaction at the end of the follow-up.
#
Materials and Methods
Study Design
The present is a retrospective study in which we report the results of 81 patients who had suffered a DRF between January 1st, 2021, and December 31, 2021, who underwent surgery at our hospital center. The patients were divided into two groups according to the surgical technique used: MIPO or the conventional technique.
The case selection criteria were: patients with unilateral FDRs classified into groups I, II or III according to the Fernández classification, who underwent surgical intervention as the definitive treatment through the implantation of a locking volar plate through the MIPO or the conventional techniques.
The exclusion criteria were: pediatric age, concurrent fracture in the ipsilateral upper limb, bilateral DRF, comminuted or highly-displaced fractures, fracture classified as groups IV or V according to the Fernández classification, complementary use of another type of osteosynthesis material (Kirschner wires, screws, more than one volar plate or dorsal plate, or external fixator).
The assignment of patients to each surgeon was carried out by a person not related to the study, randomly and independently of the surgeon themselves. The decision regarding the surgical technique used in each patient depended solely on the surgeon; no criteria were used for the choice of technique.
The radiological results were compared using the Castaing Radiological Scale, pain, using the Visual Analogue Scale (VAS), functional parameters, through the score on the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH), as well as range of motion (ROM) and grip strength, and the appearance of complications, all of them evaluated six months after the surgical intervention, corresponding to the end of the follow-up period.
#
Surgical Technique of Osteosynthesis with Minimally-Invasive Plate
The patient is placed on the surgical table in the supine position, with the upper limb that is going to be operated on extended on a hand table. Under regional anesthesia, the limb is sterilized and isolated from the rest of the body. An ischemia cuff is placed on the arm at a pressure of 250 mmHg.
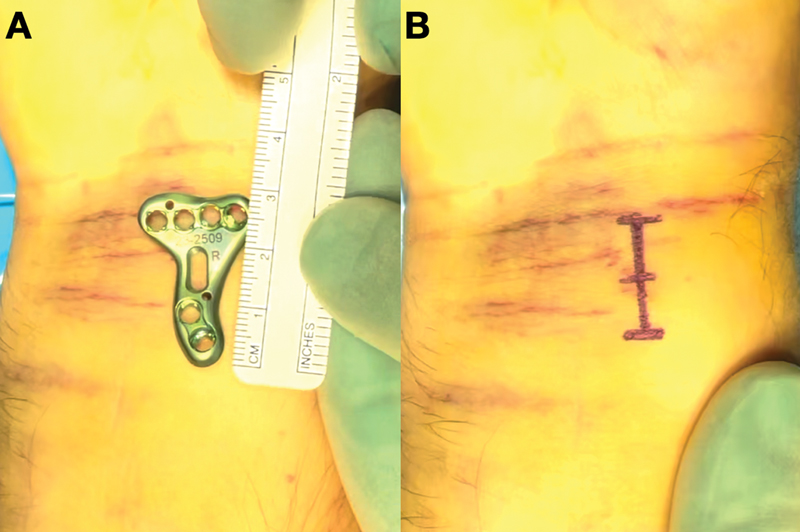
First, the radiocarpal joint is located with an intramuscular needle and, 1 cm proximal to it, the skin incision is made over the flexor carpi radialis in a proximal direction of approximately 2.5 centimeters in length ([Fig. 1]). Thanks to the small size of the incision, we can avoid the use of automatic retractors. A longitudinal incision is made in the sheath of the same tendon and is deepened, separating the flexor carpi radialis towards the ulnar side, protecting the flexor pollicis longus. The deep fascia is opened until the pronator quadratus is located. The watershed line is identified with an intramuscular needle, which serves as a reference to delimit the distal margin of the pronator quadratus, located 1 cm proximal to it ([Fig. 2-A]). Without sectioning the pronator quadratus, a dissection of its distal edge is performed, protecting its radial and ulnar insertions ([Fig. 2-B]). Next, the pronator quadratus is released by introducing a periostotome underneath it, creating a space between the pronator quadratus and the volar aspect of the radius, where the plate will subsequently be placed ([Fig. 2-C]).

Elevation of the distal end of the pronator quadratus in a tent shape enables the visualization of the radiocarpal joint and the distal 3 mm of the radius, which makes it possible to assess the reduction and facilitates the osteosynthesis of the fracture ([Fig. 2-D]).
Opening of the pronator quadratus will be necessary in cases in which it is damaged by the trauma itself, in surgeries delayed three weeks or more after the fracture, or in certain male patients, due to their lower laxity compared to women. We perform disinsertion in a reverse “L” shape by sectioning the radial insertion or, if the muscle is damaged, in a “T” shape by sectioning it longitudinally in its central portion.
This is followed by scope-guided indirect reduction of the fracture and provisional fixation with Kirschner wires. Then, the plate is slid retrogradely through the opening made in the distal margin of the pronator quadratus, like a pocket, and temporarily fixed with Kirschner wires. The watershed line marks the distal limit, where the plate should be placed at a distance between 0 and 1 cm proximally. The correct placement of the plate is verified with a scope. After this, the proximal screws are introduced, in this order, transmuscularly or percutaneously, depending on the elasticity of the skin; and the distal screws, through direct vision, starting from the medial one, corresponding to the intermediate column, when the fracture is intraarticular ([Fig. 3]).

In selected cases in which the fracture is intraarticular, prior to locking the distal screws, a wrist arthroscopy can be associated with surgery to assess the reduction of the fracture.
Finally, the Kirschner wires are removed and a new scope examination is performed to confirm the correct reduction of the fracture and placement of the implant. Skin closure is performed, and a dorsal antebrachiopalmar splint is placed.
#
Postoperative Protocol
Two weeks after the surgical intervention, the immobilization is removed and a rehabilitation protocol begins, developed jointly between surgeons and rehabilitators specializing in hand and wrist pathology. During follow-up, new clinical and radiographic controls are carried out at the first, second, third and sixth months ([Fig. 4]).

#
Statistical analysis
To carry out the statistical analysis, the sample was subjected to the Kolmogorov-Smirnov normality test, which indicated that the sample had a normal distribution. To evaluate differences between groups independently, parametric tests were performed: the Student t test for the quantitative variables, and the Chi-Squared test for the qualitative variables. The level of statistical significance was established at p < 0.05, and the two-tailed hypothesis contrast was carried out.
#
#
Results
A total of 81 patients were included, 21 cases operated on using the MIS technique and 60, using the conventional technique with the Henry approach. The results are presented regarding the analysis of demographic, radiological, clinical, and functional parameters, and the appearance of complications.
Demographic Results
Regarding the descriptive analysis of the demographic variables studied, the results are shown in [Table 1]. The MIPO group was composed of 8 men and 13 women with an average age of 57.3 (range: 41–74) years, and the conventional group, of 11 men and 49 women with an average age of 60.8 (range: 26–79) years.
|
MIPO group |
Conventional group |
p-value |
||
|---|---|---|---|---|
|
Average age in years (range) |
57.3 (41–74) |
60.8 (26–79) |
0.2718 |
|
|
Sex: n (%) |
Male |
8 (38.1%) |
11 (18.3%) |
0.065 |
|
Female |
13 (61.9%) |
49 (81.7%) |
||
|
Fracture type: n (%) |
I |
6 (28.6%) |
19 (31.7%) |
0.7524 |
|
II |
2 (9.5%) |
3 (5%) |
||
|
III |
13 (61.9%) |
38 (63.3%) |
||
|
Delay in days (range) |
10 (5–22) |
11 (2–33) |
0.5744 |
|
According to the Fernández classification, the distribution of patients in terms of fracture type was similar in both groups: the MIPO group contained 6 cases of type-I fracture (28.5%), 2 cases of type-II fracture (9.5%), and 13 cases of type-III fracture (61%); in turn, the conventional group contained 19 cases of type-I fracture (31.7%), 3 cases of type-II fracture (5%), and 38 cases of type-III fracture (63.3%).
On the other hand, the time delay from the moment the fracture occurred until the surgery was performed was similar in both groups: the MIPO group had a mean surgical delay of 10 (range: 5–22) days, and the conventional group, 11 (range: 2–33) days.
#
Radiological Results
To compare both groups in terms of radiological parameters, we used the Castaing Radiological Scale ([Table 2]). Regarding the frontal or radial inclination, averages of 20.9° (confidence interval [CI]: 17.9–24.9°) and 21.1° (CI: 17.3–24.9°) were obtained with the MIPO and conventional techniques respectively, and no statistically significant differences were observed (p = 0.8015). Regarding sagittal or volar inclination, the MIPO group presented a mean result of 10.5° (CI: 8.9–12.1°), and the conventional group, 7.3° (CI: 3.3–11.3°), with statistically significant differences (p = 0.0006). No differences were detected for the radioulnar interline (MIPO: 0.7 [CI −0.8 to −2.2] mm versus conventional: 0.75 [CI: −1.45 to −2.95] mm; p = 0. 9245), nor for the radiocarpal interline (p = 0.075). The global result of the Castaing Radiological Scale and its statistical analysis are shown in [Table 2], and it was favorable to the MIS group compared to the conventional group, with statistically significant differences (p = 0.049).
|
MIPO group |
Conventional group |
p-value |
||
|---|---|---|---|---|
|
*Front/Radial tilt: X ± SD |
20.9 ± 3 |
21.1 ± 3.8 |
0.8015 |
|
|
*Sagittal/Volar tilt: X ± SD |
10.5 ± 1.6 |
7.3 ± 4 |
0.0006 |
|
|
**Radioulnar Interline: X ± SD |
0.7 ± 1.5 |
0.75 ± 2.2 |
0.9245 |
|
|
Radiocarpal interline: n (%) |
Stage 0 |
12 (57.1%) |
35 (58.3%) |
0.075 |
|
Stage 1 |
9 (42.9%) |
15 (25%) |
||
|
Stage 2 |
0 (0%) |
10 (16.7%) |
||
|
Overall rating: n (%) |
Poor |
0 (0%) |
1 (1.7%) |
0.049 |
|
Fair |
0 (0%) |
12 (20%) |
||
|
Good |
8 (38.1%) |
27 (45%) |
||
|
Excellent |
13 (61.9%) |
20 (33.3%) |
||
#
Clinical and Functional Results
Regarding the evaluation of pain 6 months after surgery, the mean VAS score was of 1.5 (CI: 0–3) with the MIS technique, and of 2.9 (CI: 0.6–5.3) with the conventional technique, with statistically significant differences (p = 0.0141).
The score on the QuickDASH in the MIS group was of 13.5% (CI: 2.6–24.4%), which was slightly higher compared to 19.6% (CI: 4.3–34.9%) in the conventional group, although this difference did not reach statistical significance (p = 0.0955).
Regarding the joint ROM, both groups were measured and compared in terms of the averages obtained for flexion, extension, pronation, and supination, expressed in degrees ([Table 3]). No differences were detected for flexion (MIPO: 73.6° [CI: 70.2–77°] vs. conventional: 71.9° [CI: 66–77.8°]; p = 0.2162), nor for extension (MIPO: 67.4° [CI: 62–72.8°] vs. conventional: 64.4° [CI: 56.4–72.4°]; p = 0.1159). Regarding pronation, means of 88.8° (CI: 86.7–90.9°) were obtained for the MIPO group, and of 84.3° (CI: 76.6–92°) for the conventional group, with statistically significant differences (p = 0.0097). The supination was of 88.2° (CI: 85.4–91°) and of 85.1° (CI: 77.7–92.8°) with the MIPO and conventional techniques respectively, with no statistically significant differences observed (p = 0.0637).
|
MIPO group: X ± SD |
Conventional group: X ± SD |
p-value |
|
|---|---|---|---|
|
*Flexion |
73.6 ± 3.4 |
71.9 ± 5.9 |
0.2162 |
|
*Extension |
67.4 ± 5.4 |
64.4 ± 8 |
0.1159 |
|
*Pronation |
88.8 ± 2.1 |
84.3 ± 7.7 |
0.0097 |
|
*Supination |
88.2 ± 2.8 |
85.1 ± 7.7 |
0.0637 |
|
**Grip strength |
93.5 ± 3.4 |
87.8 ± 10.7 |
0.0195 |
In addition, grip strength was assessed and expressed as percentages with respect to the healthy contralateral side. The results obtained were of 93.5% (CI: 90.1–96.9%) for the MIPO group, and of 87.8% (CI: 77.1–98.5%) for the conventional group, with statistically significant differences (p = 0.0195; [Table 3]).
#
Complications
Both groups were compared regarding the incidence of nerve and tendon injuries, cases of chronic pain or complex regional pain syndrome (CRPS), as well as esthetic sequelae ([Table 4]).
|
MIPO group: n (%) |
Conventional group: n (%) |
|
|---|---|---|
|
Nerve injury |
0 (0%) |
3 (5%) |
|
Tendon injury |
0 (0%) |
2 (3.3%) |
|
Chronic pain or CRPS |
1 (4.8%) |
5 (8.3%) |
|
Adhesive scar |
2 (9.5%) |
12 (20%) |
We diagnose nerve injury when a patient expresses symptoms or signs of neuropathy, and the electromyogram is pathological. No cases were observed with the MIPO technique, but 3 cases (5%) occurred with the conventional technique.
A tendon injury is diagnosed when the patient shows a mobility deficit and surgery is performed, revealing a tendon rupture. No cases occurred with the MIS technique, while 2 cases (3.3%) were diagnosed with the conventional technique.
Regarding CRPS, 1 patient (4.8%) was diagnosed in the MIPO group, and 5 patients (8.3%), in the conventional group. Regarding esthetic sequelae and adhered scar, there were 2 cases (9.5%) in the MIPO group and 12 (20%) in the conventional group.
#
#
Discussion
Distal radius fractures are the most common fracture, representing 17.5% of the total. They occur at an average age of 55.5 years, predominating in women (69%) over men (31%).[1]
The estimated incidence is of 125 per 10 thousand people per year,[2] and it is estimated that this figure will double in the next 25 years. According to age, it shows a bimodal distribution: a first peak in childhood, between the ages of 10 and 14 years, because during this period bone growth exceeds its mineralization capacity, giving rise to a weaker bone susceptible to suffering a fracture due to minor trauma; subsequently, in adolescents, the typical injury mechanism is high impact, causing comminuted and/or highly-displaced fractures. The second age peak corresponds to adults older than 50 years, with a higher incidence in postmenopausal women around 65 years of age, with osteoporosis being the main cause.[2] [3]
Regarding the conservative treatment of DRF, there are multiple studies that compare it with surgery, without reaching a consensus on its management. Arora et al.[4] reported that an anatomical reconstruction does not offer any benefit in terms of ROM or functional outcome on activities of daily living. Likewise, Song et al.[5] demonstrated that the surgical treatment is superior to the conservative treatment in terms of radiological parameters; however they are similar regarding functional results and range of complications. Along the same lines, Chen et al.[6] showed that surgery can achieve better radiographic results and in terms of grip strength, although they cannot support that the functional results are superior compared to those of the conservative treatment.
On the other hand, Chung et al.[7] reported the progressive increase in surgery using ORIF with plates in the management of DRFs, which was supported by hand surgeons, and a decrease in the conservative treatment. Many authors[8] [9] [10] have written about this trend. There is no clear cause that justifies the increase in the surgical management of DRF. Some of the reasons that may explain this are the increases in life expectancy and quality of life of the elderly population. Chung et al.[11] reported that ORIF achieves similar results without increasing the number of complications in DRF treatment in elderly patients compared to young patients
Regarding surgical treatment, there are different options: Kirschner wires, ORIF with plates, or the external fixator. Regarding Kirschner wires, Oshige et al.[12] reported superior results for ORIF in terms of the ability to maintain fracture reduction, and early recovery of ROM and grip strength. On the other hand, Wright et al.[13] demonstrated the superiority of ORIF with a plate over the external fixator in early recovery, without loss of fracture reduction. In turn, Williksen et al.[14] showed favorable clinical (ROM, grip strength, Mayo Wrist Score) and radiological results for ORIF compared to the external fixator.
Discussing ORIF, Wagner[15] described certain iatrogenic biological complications caused by a conventional plate osteosynthesis technique, such as loss of blood supply due to damage to small vessels, or soft tissue injury in of the attempt to achieve anatomical reduction. This can lead to necrotic areas, which tend to evolve into nonunion or infection.
The explanation of the benefits of a biological approach lies in the anatomy of the operated region. Haerle et al.[16] [17] defined the importance of the anterior interosseous artery in the periosteal and endosteal irrigation of the distal ends of the radius and ulna; they also showed its intimate relationship with the pronator quadratus, both in its path and in the generation of numerous collateral vessels that cross its muscular belly.
About the MIPO for DRF, dos Remedios et al.[18] defined the surgical technique, concluding that it is possible to carry it out in most DRFs in which ORIF with a plate is indicated. They[18] also highlighted the importance of preserving the pronator quadratus as a stabilizer of the distal radioulnar joint and its importance in pronation strength, in addition to constituting a protection mechanism for the flexor tendons against impingement with the plate, thus avoiding adhesions, tenosynovitis, and breaks. In turn, Armangil et al.[19] demonstrated, through biomechanical tests, that the disinsertion of the pronator quadratus implies a significant loss in pronation force.
On the other hand, and in terms of our experience, the main drawback of the technique with preservation of the pronator quadratus is a possible worse visualization of the joint, which is especially important in intraarticular fractures. We correct this problem through three complementary solutions: elevating the distal end of the pronator quadratus in the shape of a “tent” using a clamp or separator, without disinserting its radial and ulnar insertions, which enables visualization of the radiocarpal joint and the 2 to 3 mm distal to the radius; the other two options are intraoperative radiography and arthroscopy. Even so, sometimes it is impossible; in those cases, we recommend changing the approach to a conventional one, which is easily achieved by widening the proximal and distal ends of the surgical incision.
In 2005, Imatani et al.[20] published for the first time a series of cases in which the MIPO was used in metaphyseal (not intraarticular) fractures of the distal radius. Their objective was to apply the MIPO-type surgery that was already being performed in the lower extremity, in the upper extremity, to avoid complications that are common to both, such as pseudoarthrosis, infection or refracture. They mentioned the importance of respecting the vascularization of the fracture focus by preserving the pronator quadratus and the anterior interosseous artery, and reported results consisting in lower levels of postoperative pain and early return to activities of daily living.
Later, Orbay et al.[21] defined the MIPO technique using a dorsal approach for DRFs, achieving an anatomical reduction and stable fixation of the fracture along with a reduction in operative time and a less aggressive surgery, minimizing the patient's surgical risks and achieving early recovery.
Similarly, in 2008, Sen. et al.[22] described the MIPO technique using a volar approach, with preservation of the pronator quadratus, for DRFs. The main problem they found with this technique was that, on some occasions, it was difficult to achieve an adequate reduction of the fracture; in these cases, they advised changing the approach to a conventional one.
One of the first comparative studies of the MIPO and conventional techniques was conducted by Zenke et al.[23] in 2011; they assessed radiological and clinical results, without finding statistically significant differences.
In 2014, Lebailly et al.[24] performed the MIPO technique through a single 15-mm volar incision in a series of cases that included intraarticular fractures, associating arthroscopic surgery in certain cases.
In a literature review, Liverneaux et al.,[25] defined several aspects of the MIPO technique based on studies conducted so far: it is indicated for both extra- and intraarticular fractures, it requires a single volar incision shorter than 20 mm, it can be associated with arthroscopic surgery, the radiological and clinical outcomes are similar to those of the conventional technique, and, in cases of difficult reduction, the incision can be easily expanded.
More current studies are reporting favorable results regarding the MIPO technique compared to the conventional technique. Read. et al.[26] demonstrated better results with the MIPO technique in terms of patient satisfaction. Recently, Asmar et al.[27] used the same extra-short plate used in the present study, inserted through the MIPO technique, demonstrating that this implant is capable of maintaining the initial reduction measured with radiographic indices, avoiding secondary displacement. Furthermore, they obtained satisfactory functional results.
The results obtained in the present study demonstrate that radiographic parameters such as sagittal or volar inclination and the overall result on the Castaing Radiological Scale, as well as functional and satisfaction parameters such as pronation, grip strength and the VAS score, together with morbidity and esthetic sequelae, are higher for the MIPO group compared to the conventional group. The MIPO technique offers advantages associated with the type of implant used, as well as others, inherent to the biological approach. The design of the plate used, which has different medial and lateral curvature radii, partly explains the difference in the optimization of volar inclination. On the other hand, the MIPO technique facilitates reduction by ligamentotaxis, and improves the intrinsic biology of the fracture through a smaller incision and minimal dissection, preserving the pronator quadratus, and avoiding deperiostization and devascularization of the bone tissue. The preservation of the pronator quadratus, in addition to the benefit in the range and strength of pronation, also avoids impingement of the flexor tendons with the plate, which translates into a lower incidence of tendon injury. Along with this, another reason for the lower morbidity of both tendons and nerves in the MIPO group is the fact that automatic distractors or separators are not used due to the small surgical incision.
The present work has some limitations, such as its retrospective nature, or the short- and mid-term period of evolution, which prevents us from assessing possible late complications. Furthermore, it is advisable to increase the number of patients in the study to confirm these results.
#
Conclusion
For the surgical treatment of DRFs, the MIPO technique with preservation of the pronator quadratus may be superior to the conventional technique in terms of radiographic, functional, and satisfaction outcomes, reducing morbidity and esthetic sequelae. Since it is a novel technique, the literature is scarce, and prospective studies with a larger number of participants are needed to confirm these data.
#
#
-
References
- 1 Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury 2006; 37 (08) 691-697
- 2 Corsino CB, Reeves RA, Sieg RN. Distal Radius Fractures. 2023 Aug 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Jan–
- 3 Bentohami A, Bosma J, Akkersdijk GJ, van Dijkman B, Goslings JC, Schep NW. Incidence and characteristics of distal radial fractures in an urban population in The Netherlands. Eur J Trauma Emerg Surg 2014; 40 (03) 357-361
- 4 Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am 2011; 93 (23) 2146-2153
- 5 Song J, Yu AX, Li ZH. Comparison of conservative and operative treatment for distal radius fracture: a meta-analysis of randomized controlled trials. Int J Clin Exp Med 2015; 8 (10) 17023-17035
- 6 Chen Y, Chen X, Li Z, Yan H, Zhou F, Gao W. Safety and Efficacy of Operative Versus Nonsurgical Management of Distal Radius Fractures in Elderly Patients: A Systematic Review and Meta-analysis. J Hand Surg Am 2016; 41 (03) 404-413
- 7 Chung KC, Shauver MJ, Birkmeyer JD. Trends in the United States in the treatment of distal radial fractures in the elderly. J Bone Joint Surg Am 2009; 91 (08) 1868-1873
- 8 Fanuele J, Koval KJ, Lurie J, Zhou W, Tosteson A, Ring D. Distal radial fracture treatment: what you get may depend on your age and address. J Bone Joint Surg Am 2009; 91 (06) 1313-1319
- 9 Mellstrand-Navarro C, Pettersson HJ, Tornqvist H, Ponzer S. The operative treatment of fractures of the distal radius is increasing: results from a nationwide Swedish study. Bone Joint J 2014; 96-B (07) 963-969
- 10 Mattila VM, Huttunen TT, Sillanpää P, Niemi S, Pihlajamäki H, Kannus P. Significant change in the surgical treatment of distal radius fractures: a nationwide study between 1998 and 2008 in Finland. J Trauma 2011; 71 (04) 939-942 , discussion 942–943
- 11 Chung KC, Squitieri L, Kim HM. Comparative outcomes study using the volar locking plating system for distal radius fractures in both young adults and adults older than 60 years. J Hand Surg Am 2008; 33 (06) 809-819
- 12 Oshige T, Sakai A, Zenke Y, Moritani S, Nakamura T. A comparative study of clinical and radiological outcomes of dorsally angulated, unstable distal radius fractures in elderly patients: intrafocal pinning versus volar locking plating. J Hand Surg Am 2007; 32 (09) 1385-1392
- 13 Wright TW, Horodyski M, Smith DW. Functional outcome of unstable distal radius fractures: ORIF with a volar fixed-angle tine plate versus external fixation. J Hand Surg Am 2005; 30 (02) 289-299
- 14 Williksen JH, Husby T, Hellund JC, Kvernmo HD, Rosales C, Frihagen F. External Fixation and Adjuvant Pins Versus Volar Locking Plate Fixation in Unstable Distal Radius Fractures: A Randomized, Controlled Study With a 5-Year Follow-Up. J Hand Surg Am 2015; 40 (07) 1333-1340
- 15 Wagner M. General principles for the clinical use of the LCP. Injury 2003; 34 (Suppl. 02) B31-B42
- 16 Haerle M, Schaller HE, Mathoulin C. Vascular anatomy of the palmar surfaces of the distal radius and ulna: its relevance to pedicled bone grafts at the distal palmar forearm. J Hand Surg [Br] 2003; 28 (02) 131-136
- 17 Haerle M, Häfner HM, Dietz K, Schaller HE, Brunelli F. Vascular dominance in the forearm. Plast Reconstr Surg 2003; 111 (06) 1891-1898
- 18 Dos Remedios C, Nebout J, Benlarbi H, Caremier E, Sam-Wing JF, Beya R. Préservation du muscle carré pronateur dans les ostéosynthèses des fractures de l'extrémité distale du radius par plaque palmaire verrouillée. Technique chirurgicale. Chir Main 2009; 28 (04) 224-229 French
- 19 Armangil M, Bezirgan U, Başarır K, Bilen G, Demirtaş M, Bilgin SS. The pronator quadratus muscle after plating of distal radius fractures: is the muscle still working?. Eur J Orthop Surg Traumatol 2014; 24 (03) 335-339
- 20 Imatani J, Noda T, Morito Y, Sato T, Hashizume H, Inoue H. Minimally invasive plate osteosynthesis for comminuted fractures of the metaphysis of the radius. J Hand Surg [Br] 2005; 30 (02) 220-225
- 21 Orbay JL, Touhami A, Orbay C. Fixed angle fixation of distal radius fractures through a minimally invasive approach. Tech Hand Up Extrem Surg 2005; 9 (03) 142-148
- 22 Sen MK, Strauss N, Harvey EJ. Minimally invasive plate osteosynthesis of distal radius fractures using a pronator sparing approach. Tech Hand Up Extrem Surg 2008; 12 (01) 2-6
- 23 Zenke Y, Sakai A, Oshige T. et al. Clinical results of volar locking plate for distal radius fractures: conventional versus minimally invasive plate osteosynthesis. J Orthop Trauma 2011; 25 (07) 425-431
- 24 Lebailly F, Zemirline A, Facca S, Gouzou S, Liverneaux P. Distal radius fixation through a mini-invasive approach of 15 mm. PART 1: a series of 144 cases. Eur J Orthop Surg Traumatol 2014; 24 (06) 877-890
- 25 Liverneaux P, Ichihara S, Facca S, Hidalgo Diaz JJ. [Outcomes of minimally invasive plate osteosynthesis (MIPO) with volar locking plates in distal radius fractures: A review]. Hand Surg Rehabil 2016; 35S: S80-S85 French
- 26 Lee DY, Park YJ, Park JS. A Meta-analysis of Studies of Volar Locking Plate Fixation of Distal Radius Fractures: Conventional versus Minimally Invasive Plate Osteosynthesis. Clin Orthop Surg 2019; 11 (02) 208-219
- 27 Asmar G, Bellity J, Falcone MO. Surgical comfort and clinical outcomes of MIPO with an extra-short plate designed for distal radius fractures. Eur J Orthop Surg Traumatol 2021; 31 (03) 481-490
Dirección para correspondencia
Publication History
Received: 09 January 2024
Accepted: 01 April 2024
Article published online:
07 June 2024
© 2024. SECMA Foundation. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury 2006; 37 (08) 691-697
- 2 Corsino CB, Reeves RA, Sieg RN. Distal Radius Fractures. 2023 Aug 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Jan–
- 3 Bentohami A, Bosma J, Akkersdijk GJ, van Dijkman B, Goslings JC, Schep NW. Incidence and characteristics of distal radial fractures in an urban population in The Netherlands. Eur J Trauma Emerg Surg 2014; 40 (03) 357-361
- 4 Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am 2011; 93 (23) 2146-2153
- 5 Song J, Yu AX, Li ZH. Comparison of conservative and operative treatment for distal radius fracture: a meta-analysis of randomized controlled trials. Int J Clin Exp Med 2015; 8 (10) 17023-17035
- 6 Chen Y, Chen X, Li Z, Yan H, Zhou F, Gao W. Safety and Efficacy of Operative Versus Nonsurgical Management of Distal Radius Fractures in Elderly Patients: A Systematic Review and Meta-analysis. J Hand Surg Am 2016; 41 (03) 404-413
- 7 Chung KC, Shauver MJ, Birkmeyer JD. Trends in the United States in the treatment of distal radial fractures in the elderly. J Bone Joint Surg Am 2009; 91 (08) 1868-1873
- 8 Fanuele J, Koval KJ, Lurie J, Zhou W, Tosteson A, Ring D. Distal radial fracture treatment: what you get may depend on your age and address. J Bone Joint Surg Am 2009; 91 (06) 1313-1319
- 9 Mellstrand-Navarro C, Pettersson HJ, Tornqvist H, Ponzer S. The operative treatment of fractures of the distal radius is increasing: results from a nationwide Swedish study. Bone Joint J 2014; 96-B (07) 963-969
- 10 Mattila VM, Huttunen TT, Sillanpää P, Niemi S, Pihlajamäki H, Kannus P. Significant change in the surgical treatment of distal radius fractures: a nationwide study between 1998 and 2008 in Finland. J Trauma 2011; 71 (04) 939-942 , discussion 942–943
- 11 Chung KC, Squitieri L, Kim HM. Comparative outcomes study using the volar locking plating system for distal radius fractures in both young adults and adults older than 60 years. J Hand Surg Am 2008; 33 (06) 809-819
- 12 Oshige T, Sakai A, Zenke Y, Moritani S, Nakamura T. A comparative study of clinical and radiological outcomes of dorsally angulated, unstable distal radius fractures in elderly patients: intrafocal pinning versus volar locking plating. J Hand Surg Am 2007; 32 (09) 1385-1392
- 13 Wright TW, Horodyski M, Smith DW. Functional outcome of unstable distal radius fractures: ORIF with a volar fixed-angle tine plate versus external fixation. J Hand Surg Am 2005; 30 (02) 289-299
- 14 Williksen JH, Husby T, Hellund JC, Kvernmo HD, Rosales C, Frihagen F. External Fixation and Adjuvant Pins Versus Volar Locking Plate Fixation in Unstable Distal Radius Fractures: A Randomized, Controlled Study With a 5-Year Follow-Up. J Hand Surg Am 2015; 40 (07) 1333-1340
- 15 Wagner M. General principles for the clinical use of the LCP. Injury 2003; 34 (Suppl. 02) B31-B42
- 16 Haerle M, Schaller HE, Mathoulin C. Vascular anatomy of the palmar surfaces of the distal radius and ulna: its relevance to pedicled bone grafts at the distal palmar forearm. J Hand Surg [Br] 2003; 28 (02) 131-136
- 17 Haerle M, Häfner HM, Dietz K, Schaller HE, Brunelli F. Vascular dominance in the forearm. Plast Reconstr Surg 2003; 111 (06) 1891-1898
- 18 Dos Remedios C, Nebout J, Benlarbi H, Caremier E, Sam-Wing JF, Beya R. Préservation du muscle carré pronateur dans les ostéosynthèses des fractures de l'extrémité distale du radius par plaque palmaire verrouillée. Technique chirurgicale. Chir Main 2009; 28 (04) 224-229 French
- 19 Armangil M, Bezirgan U, Başarır K, Bilen G, Demirtaş M, Bilgin SS. The pronator quadratus muscle after plating of distal radius fractures: is the muscle still working?. Eur J Orthop Surg Traumatol 2014; 24 (03) 335-339
- 20 Imatani J, Noda T, Morito Y, Sato T, Hashizume H, Inoue H. Minimally invasive plate osteosynthesis for comminuted fractures of the metaphysis of the radius. J Hand Surg [Br] 2005; 30 (02) 220-225
- 21 Orbay JL, Touhami A, Orbay C. Fixed angle fixation of distal radius fractures through a minimally invasive approach. Tech Hand Up Extrem Surg 2005; 9 (03) 142-148
- 22 Sen MK, Strauss N, Harvey EJ. Minimally invasive plate osteosynthesis of distal radius fractures using a pronator sparing approach. Tech Hand Up Extrem Surg 2008; 12 (01) 2-6
- 23 Zenke Y, Sakai A, Oshige T. et al. Clinical results of volar locking plate for distal radius fractures: conventional versus minimally invasive plate osteosynthesis. J Orthop Trauma 2011; 25 (07) 425-431
- 24 Lebailly F, Zemirline A, Facca S, Gouzou S, Liverneaux P. Distal radius fixation through a mini-invasive approach of 15 mm. PART 1: a series of 144 cases. Eur J Orthop Surg Traumatol 2014; 24 (06) 877-890
- 25 Liverneaux P, Ichihara S, Facca S, Hidalgo Diaz JJ. [Outcomes of minimally invasive plate osteosynthesis (MIPO) with volar locking plates in distal radius fractures: A review]. Hand Surg Rehabil 2016; 35S: S80-S85 French
- 26 Lee DY, Park YJ, Park JS. A Meta-analysis of Studies of Volar Locking Plate Fixation of Distal Radius Fractures: Conventional versus Minimally Invasive Plate Osteosynthesis. Clin Orthop Surg 2019; 11 (02) 208-219
- 27 Asmar G, Bellity J, Falcone MO. Surgical comfort and clinical outcomes of MIPO with an extra-short plate designed for distal radius fractures. Eur J Orthop Surg Traumatol 2021; 31 (03) 481-490



