
RSS-Feed abonnieren
DOI: 10.1055/s-0044-1787270
Early Diagnosis of Sepsis: The Role of Biomarkers and Rapid Microbiological Tests
Funding None.
- Abstract
- Sepsis Suspicion: Reasoning on a Case-by-Case Basis Is Crucial
- Sepsis as a Clinical Syndrome: Delayed Recognition of a Time-Dependent Condition
- Improved Understanding of Sepsis Pathobiology for Earlier Detection
- Biomarkers for “Early” Sepsis Diagnosis
- Prediction of Sepsis: Detecting Occult Processes Leading to Sepsis and Organ Dysfunction
- Novel Molecular Biomarkers for Prediction or Early Diagnosis
- Rapid Microbiological Diagnosis as an Element for Sepsis Prediction
- Conclusion
- References
Abstract
Sepsis is a medical emergency resulting from a dysregulated response to an infection, causing preventable deaths and a high burden of morbidity. Protocolized and accurate interventions in sepsis are time-critical. Therefore, earlier recognition of cases allows for preventive interventions, early treatment, and improved outcomes. Clinical diagnosis of sepsis by clinical scores cannot be considered an early diagnosis, given that underlying molecular pathophysiological mechanisms have been activated in the preceding hour or days. There is a lack of a widely available tool enhancing preclinical diagnosis of sepsis. Sophisticated technologies for sepsis prediction have several limitations, including high costs. Novel technologies for fast molecular and microbiological diagnosis are focusing on bedside point-of-care combined testing to reach most settings where sepsis represents a challenge.
Keywords
sepsis - septic shock - severe sepsis - diagnosis - biomarkers - screening - early diagnosis - molecular diagnostic techniques - molecular testingSepsis represents a medical condition associated with preventable deaths, a high burden of morbidity, and long-term sequelae. Global epidemiological data have shown that 48.9 million people develop sepsis yearly, and 11 million deaths are attributable to septic shock worldwide, accounting for almost 20% of all global deaths.[1] Consequently, the World Health Organization has urged for actions to improve sepsis prognosis. Delayed diagnosis and treatment of sepsis have consistently been considered independent risk factors for the progression of organ dysfunction and death, particularly in patients with septic shock.[2] [3] [4] [5] According to the updated sepsis definition proposed by the last Surviving Sepsis Campaign (SSC) guidelines in 2021,[6] which defines sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection, an arsenal of theragnostic tools has been developed to increase the specificity of sepsis detection.
Protocolized and accurate interventions are time-critical. These include early adequate empirical antimicrobial therapy, infection source control, and optimal hemodynamic resuscitation.[5] [6] Current challenges in early detection of sepsis before clinical signs develop contribute to delays in implementing standard-of-care SSC recommendations for the early approach to sepsis and septic shock.[7] [8] In some settings, evidence of the adverse outcomes of late-recognized cases has been insufficient to perceive sepsis as a medical emergency that requires prompt treatment.
There is a wide variety of other contributing factors or barriers to improving early diagnosis and treatment of sepsis.[9] Some studies have found barriers are often related to the lack of availability of some resources, such as microbiology laboratory that processes blood cultures and other microbiological detection tests. Still, advances in quality of care in sepsis and a better understanding of underlying pathobiological processes leading to organ dysfunction will aid in developing accurate, fast, and widely available point-of-care tests. Bedside accurate tools help the development of future quality improvements for the practical implementation of stand-of-care interventions, which have been consistently demonstrated to decrease mortality when implemented on time.[5]
Over the last few years, sepsis biomarkers and rapid microbiological diagnostic tests (RDTs) have been considered a paradigm for novel strategies to improve earlier sepsis detection. Herein, we gathered the best available evidence on this topic. Biomarkers used for phenotyping, prognosis, and stratification of patients already diagnosed with sepsis, insights into machine-learning models, and other artificial intelligence tools are out of the scope of this review.
For this narrative review, we performed a comprehensive literature search in the Cochrane, PubMed, CINAHL, and Scopus databases from no start date to September 2023. The search criteria included the following Medical Subject Headings (MeSH) terms: sepsis OR Septic shock OR Severe sepsis AND diagnosis OR biomarkers OR screening OR early diagnosis OR molecular diagnostic techniques OR molecular testing. We reviewed articles written in Spanish and English. We obtained all full-text versions of the selected manuscripts. The first draft of the manuscript was reviewed and modified by all authors. All authors approved the final manuscript.
Sepsis Suspicion: Reasoning on a Case-by-Case Basis Is Crucial
When considering the pathophysiological events leading to sepsis, clinicians should acknowledge that clinical signs of sepsis are the ultimate consequence of complex underlying molecular and inflammatory derangements that culminate in measurable clinical signs. The main challenges when trying to diagnose sepsis in its early stages using clinical variables are the ability to differentiate sepsis from infection, the detection of occult organ dysfunction in the presence of infection, differentiating sepsis from local organ dysfunction as a consequence of specific infection (e.g., pneumonia), attributing a new-onset organ dysfunction to sepsis, organ dysfunction as the consequence of an unrecognized infection, and the variability of sepsis phenotypes (clinical and biological), which are influenced by recent interventions, and other noninfectious causes of inflammation with apparently close to similar clinical and biological host response (e.g., trauma, burns, autoimmune disease, pancreatitis, major surgery, comorbidities, age, gender, concurrent medications).[10]
The most appropriate workflow is the one that first rules out sepsis using objective data in the context of any infection to manage the patient accordingly. However, this is a real challenge with the available validated tools, and most cases are classified as “suspicious of sepsis” after a clinical evaluation. Recognition of sepsis cases before the occurrence of hypotension requires wise evaluations to prevent further organ dysfunction, given that a significant proportion of sepsis patients present subtle clinical signs and appear less sick at the time of presentation. The inadequate recognition of these cases and delayed treatment are associated with high mortality rates (up to 25% in some studies) due to the progression of illness to irreversible organ dysfunction.[11] New organ dysfunction or overt inflammatory response in the context of infection should prompt early evaluation to rule out sepsis. However, specific infectious conditions may lead to local organ dysfunction without causing a dysregulated systemic host response.
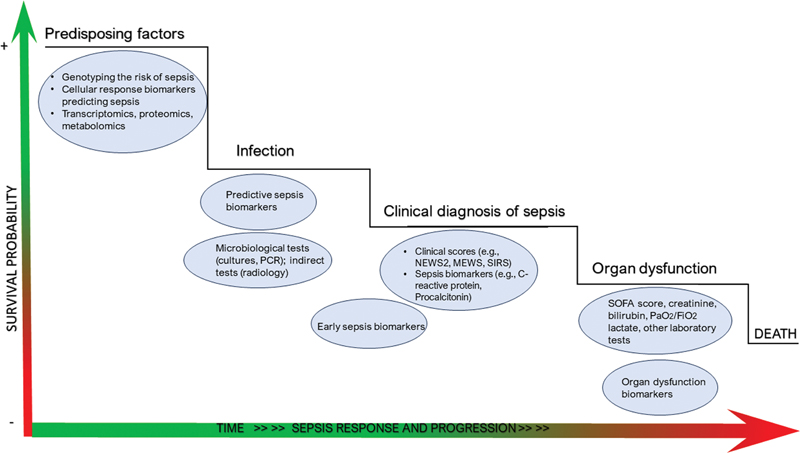
Before discussing the potential biomarkers available for clinical purposes, we should define “early” when discussing sepsis diagnosis. The literature has no valid and widely accepted definition of early sepsis. Most studies have considered early sepsis before septic shock develops, for cases in which clinical signs are evident and the infection is not confirmed, or during the early (reversible) stages of organ dysfunction. In our view, those considerations are inaccurate and should be considered “sepsis diagnosis” or, more precisely, late sepsis diagnosis. Some studies define early sepsis when sepsis-3 criteria are present (infection + sequential organ failure assessment [SOFA] score ≥ 2), but septic shock is not present yet.[12] All tools detecting sepsis after clinical data are present should be considered diagnostic tools if organ dysfunction is already present, or there is a clinically evident process possibly linked to infection progressing to organ dysfunction (e.g., systemic inflammatory response syndrome [SIRS], SOFA score 0–1). For the purpose of this review, we will consider prediction of sepsis to any preclinical condition in which there is an infection in a host in whom different pathophysiological pathways, particularly immunological status, will irreversibly lead to organ dysfunction if untreated. All screening tools detecting sepsis in this phase are predictors of sepsis (see [Fig. 1]).
Sepsis as a Clinical Syndrome: Delayed Recognition of a Time-Dependent Condition
Interestingly, clinical scores are currently recommended as the best widely available tools in our arsenal for sepsis screening.[6] However, studies in prehospital settings have shown that up to one-third of patients with documented infection who develop sepsis have normal vital signs.[13] Sepsis results from complex host interactions and dysregulated response, amplified by endogenous factors, to a given pathogen. Therefore, recognizing sepsis from parameters that reflect its clinical consequences can be considered as a delayed strategy for detection. Clinical scores may not be ideal for sepsis prediction before organ dysfunction is clinically overt. However, an accurate clinical assessment remains the core strategy to detect potential sepsis cases in some low-resource settings.[14]
The lack of validity of SIRS as a tool for the early detection of sepsis has been demonstrated. The classic systemic SIRS criteria for diagnosing sepsis focus only on bedside clinical variables and laboratory parameters. The need for two or more SIRS criteria excludes 12.5% of sepsis cases with the same organ dysfunction and mortality risk as cases that fulfill SIRS criteria.[15] In the same study, the authors found SIRS criteria failed to define the transition point in the overall risk of death.
Sepsis-3 criteria have not proven beneficial to decrease overall mortality or to improve sepsis recognition and screening. Adding lactate, procalcitonin (PCT), or other clinical variables improves its sensitivity. In the study of Machado et al,[16] the authors conducted a prospective study of two cohorts, with mortality as the primary outcome. They included patients with suspected infection but without sepsis and patients with sepsis. The predictive accuracy of quick sequential organ failure assessment (qSOFA) score was assessed, considering the worst values prior to the suspicion of infection or sepsis. One cohort had 5,460 patients, 78.3% had a qSOFA score ≤1, and crude mortality was of 14%. The sensitivity of qSOFA score ≥2 for predicting mortality was 53.9% (95% confidence interval [CI]: 50.3–57.5). The sensitivity was higher for a qSOFA ≥1 (85%), a qSOFA score ≥1 or lactate ≥2 mmol/L, and SIRS plus organ dysfunction. The second cohort included 4,711 patients, and 62.3% had a qSOFA score ≤1, and a mortality rate of 17.3%. In public hospitals, the mortality rate was higher, 39.3%. In a previous study, approximately one-quarter of infected patients had a qSOFA score ≥2, with 70% of them having poor outcomes.[17] When using sepsis-3 criteria to detect sepsis, patients in the early phase of sepsis are missed. The SOFA score performs better in diagnosing sepsis later in clinical stages and predicting intensive care unit (ICU) admission.[12] [16] [18] [19]
As previously mentioned, the qSOFA score is far from being a predictive tool, as clinical repercussions of sepsis should be evident for a positive score. The frequency of patients having hyperlactatemia who are still normotensive can be as common as 26% of sepsis cases.[20] Different studies have demonstrated that qSOFA is less sensitive than SIRS to identify organ dysfunction due to sepsis.[21] [22] [23] Despite the National Early Warning Score (NEWS; and the updated version NEWS2) and the Modified Early Warning Score (MEWS) being better tools than qSOFA[24] [25] and recommended by the current SSC guidelines,[6] clinicians still lack a specific bedside tool to differentiate sepsis from other conditions in patients with unclear medical history or to predict sepsis in some subsets of patients prone to develop sepsis in the following hours after infection. Clinical scores are more useful for predicting mortality in sepsis than early predictors of the risk for developing sepsis.
In-hospital quality-of-care programs often use automated sepsis screening tools in electronic health records, which have been studied to detect sepsis early. However, their accuracy is variable, given that some studies have shown low predictive values while others show improvements in sepsis care processes.[26] [27] [28] There are studies showing no mortality benefits from sepsis screening tools.[29] [30] [31] In many settings, improvements in sepsis screening have been made by developing and implementing performance improvement programs, which have been shown to standardize and improve the standards of care for the management of sepsis patients. These programs generally focus on sepsis screening, sepsis bundle performance metrics, health care staff education and adherence to sepsis bundles, patient outcomes, and actions for identified opportunities.[9] [32] [33] [34] [35] [36] Parameters reflecting the underlying pathophysiology of sepsis are not included in this type of clinical screening tools.
Improved Understanding of Sepsis Pathobiology for Earlier Detection
The early diagnosis of sepsis should be based on the early diagnosis of an infection, along with the identification of a dysregulated response that may subsequently lead to organ dysfunction.[6] [37] Sepsis involves the early activation of pro- and anti-inflammatory molecular responses and other nonimmunologic pathways triggered by a pathogen (e.g., neuronal, cardiovascular, metabolic, bioenergetic, autonomic, hormonal, and coagulation) with outstanding prognostic significance.[38] According to this framework, the ideal biomarker should have enough sensitivity to rule out sepsis early during the triage of suspicious cases presenting to the emergency department (ED) and enough specificity to differentiate sepsis from other conditions. Accurate tools that improve clinical judgment are the game changer for improving sepsis diagnosis, management, and prognosis. Host response biomarkers have been extensively studied, as they play a critical role in diagnosis, early detection, phenotyping, risk of organ dysfunction and death, personalized patient management, and antibiotic stewardship.
Biomarkers for “Early” Sepsis Diagnosis
Early diagnosis of sepsis based on biomarkers has evolved to enhance the accuracy of our clinical assessments. Acceptable reliability of early diagnosis of sepsis using only clinical scores is not feasible, as they have low sensitivity and specificity for sepsis detection in the absence of a severe illness or organ dysfunction and have important limitations to predicting the mortality risk.[39] Diagnostic biomarkers should add value and be able to change the pretest probability and reclassify patients when there is diagnostic uncertainty, increasing specificity and providing a high negative predictive value. Ideal biomarkers should be able to detect sepsis even before clinical suspicion (predictive biomarkers), enabling presymptomatic diagnosis. In real life, most clinicians use a combination of widely available laboratory biomarkers to diagnose sepsis (e.g., white blood cell and neutrophil count, lactate, C-reactive protein [CRP]), more than clinical scores; only 36% use the Sepsis-3 definition alone, 34.2% still calculate the qSOFA, and 44.7% use the SOFA score.[40]
PCT has been extensively studied as a diagnostic tool for sepsis. Three meta-analyses evaluating the diagnostic utility of PCT reported a pooled sensitivity and specificity of 77 to 85% and 75 to 83%, respectively.[41] [42] [43] Of note, most studies reporting a lack of PCT usefulness for sepsis diagnosis have included patients with a low pretest probability for sepsis of bacterial origin, and international guidelines do not support the use of PCT to initiate antibiotics in sepsis.[6] [44] [45] PCT is thought to be more accurate than CRP for detecting patients with suspected sepsis; however, studies have shown PCT is not beneficial to early diagnose sepsis cases with a less severe clinical condition.
Illness severity and pretest probability for sepsis influence the usefulness and cut-off of PCT as a diagnostic tool.[46] A reliable cut-off value of 1.1 ng/mL with sensitivity and specificity of 77% and 79%, respectively (area under the receiver operating characteristic curve [AUROC] of 0.85, 95% CI: 0.81–0.88) can be used to support sepsis diagnosis,[43] depending on pretest probability, the presence of clinical criteria, and severity of illness.[12] [18] In an interesting retrospective study by Kim et al, PCT was a useful biomarker for sepsis and septic shock diagnosis in the ED when used in patients who fulfilled sepsis-3 criteria.[12] In other words, it was useful to enhance the diagnosis of sepsis when clinical repercussions and organ dysfunction are already established, with a proposed cut-off of 0.41 ng/dL for sepsis (sensitivity and specificity of 74.8% and 63.8%, respectively; AUROC: 0.745), and 4.7 ng/dL for septic shock (sensitivity and specificity of 66.1% and 79.0%, respectively; AUROC: 0.784). The lack of effectiveness of PCT to rule out or predict early sepsis has been recognized, and the current SSC guidelines do not recommend its use to start antibiotics.[6]
Consequently, early diagnosis or prediction of sepsis using PCT is unreliable.[12] The less severe the condition, the less likely sepsis will be diagnosed early before overt clinical signs or organ dysfunction develop. Previous studies on this matter have assessed PCT usefulness compared to clinical criteria as the gold standard.[47] International guidelines do not recommend using PCT in ventilator-associated pneumonia, a common condition related to sepsis in critically ill patients.[48] [49] [50] There is no agreed PCT cut-off value for diagnosis of infection regardless of the presence of sepsis; some studies used PCT values from 0.5 to 2 μg/L, as previous studies of community-acquired pneumonia (CAP).[51] A recent meta-analysis of patients with diverse etiologies of CAP showed that PCT has low sensitivity during early CAP and cannot reliably distinguish viral from bacterial pneumonia.[52] A previous study on PCT kinetics in patients with bacteriemia showed poor diagnostic accuracy and a low PCT reliability to guide the initiation of therapy.[53] Moreover, PCT is not specific to sepsis; it increases in other conditions often confused with sepsis, such as trauma, pancreatitis, or autoimmune disease.[46] [54] The most widely accepted applicability of PCT in the context of sepsis is antimicrobial stewardship and prognosis assessment.[46] [55] [56] [57]
Various individual biomarkers are developed to enhance the clinical diagnosis of sepsis. In a recent meta-analysis, soluble urokinase plasminogen activator receptor (suPAR) was observed to have an AUROC of 0.83 for predicting sepsis (95% CI: 0.80–0.86).[58] In addition, AUROC for differentiating sepsis from non-sepsis SIRS was 0.81 (95% CI: 0.77–0.84), and the sensitivity and specificity were 0.67 (95% CI: 0.58–0.76) and 0.82 (95% CI: 0.73–0.88), respectively. Soluble triggering receptor expressed on myeloid cells (sTREM-1) is expressed in innate immune cells (e.g., monocytes and neutrophils). This protein reflects important processes of the inflammatory and cytotoxic response to sepsis, such as the synergic activation of Toll-like receptors and the augmented production of pro-inflammatory cytokines.[59] Serum levels of sTREM-1 have been studied as a biomarker for early sepsis.[60] Previous studies have shown an AUROC of 0.78 (95% CI: 0.69–0.86) to differentiate sepsis from other causes of SIRS,[61] and an AUROC of 0.95 for septic shock diagnosis. In a study of 90 patients with SIRS due to sepsis and other etiologies,[61] a PCT cut-off value of 1.57 ng/mL and sTREM-1 cut-off value ≥133 pg/mL yielded a sensitivity of 71.1 and 67.33%, and specificity of 73.3 and 65.79%, respectively, for the differentiation of sepsis from other causes of SIRS.
Biomarker-enhanced clinical scores may improve specificity of diagnosis, though sensitivity remained low.[12] Other biomarkers have been more beneficial in predicting prognosis in sepsis, such as pro-MR-adrenomedullin.[62] [63] [64]
Sepsis often presents a hyperinflammatory response pattern followed by an immunosuppressive state, during which multiple organ dysfunction develops.[65] [66] A biomarker or a combination of biomarkers could be a new alternative to predict, identify, or provide new approaches to manage sepsis patients. In some settings, the combination of biomarkers has been used as a strategy to increase the sensitivity for early diagnosis and improved outcomes.[63] [67] The combination of two or more biomarkers increases the diagnostic accuracy of sepsis diagnosis in some studies.[68] Seeking more accurate therapeutic interventions and patient outcomes in this condition should be the goal of any combination of biomarkers.
Still, association of different biomarkers reflecting the same pathophysiological pathway may have no added value in terms of diagnostic accuracy. An important study of ICU patients with SIRS showed no combination of biomarkers performed better than CRP alone to diagnose sepsis.[69] Increased costs, complexities in interpreting results, lack of validation studies, and inadequate training in the obtention and implementation in different settings are other disadvantages of combining biomarkers. Standardization of sample collection, analysis, and processing are needed for their reliability regardless of the laboratory performing the tests. Combining point-of-care inflammatory biomarkers would solve all those issues related to the usual measurement of biomarkers. This innovative strategy needs to be further validated in clinical studies.[70]
Machine learning tools and biomarker-enhanced scores that involve the combination of laboratory and clinical biomarkers have been overwhelming in recent years. Machine-learning models using artificial intelligence have been studied over the last few years to improve the usefulness of clinical and laboratory biomarkers by combining them for early sepsis detection.[30] [31] [71] The performance of these models has been variable, and some limitations have been identified due to the lack of availability of some biomarkers or clinical measurements. Electronic alerts are more useful in emergency settings to reduce hospital length of stay, improve time to treatment, and reduce mortality, though sometimes they are poorly generalizable.[72]
Prediction of Sepsis: Detecting Occult Processes Leading to Sepsis and Organ Dysfunction
As we have discussed before, even machine learning models that use clinical variables and relevant host factors with characteristics that progress over time are not sufficiently accurate to diagnose early sepsis, as they rely on clinical consequences and common laboratory tests resulting from underlying molecular derangements leading to an aberrant or dysregulated host response and organ dysfunction. The logical pathway would be to find preclinical biomarkers of systems that accurately predict the risk of sepsis once the infection is established (or before) and combine microbiological and inflammatory panels. This review will not discuss biomarkers that have been studied as predictors of organ dysfunction in sepsis and increased mortality.
Novel Molecular Biomarkers for Prediction or Early Diagnosis
Extensive research in the field of biomarkers is being performed to validate new molecules detecting sepsis underlying processes at early stages, with the intention to facilitate effective sepsis prediction at the time of infection, allowing for preventive rather than early interventions and ultimately reducing the number of deaths. Interesting studies on earlier biomarkers, including serial measurements of pancreatic stone protein, demonstrated an increase of this marker 3 days preceding the onset of signs necessary to diagnose sepsis clinically.[73] As discussed above, some studies propose using panels of biomarkers to predict or diagnose sepsis early as the most pragmatic strategy, so far, to improve clinical diagnosis of sepsis.[68] [Table 1] gathers a summary of novel predictive biomarkers in sepsis; PCT was added to the table as a comparator.
|
Biomarker |
Clinical applicability |
|---|---|
|
PCT |
Classic biomarker, not useful for sepsis prediction or early diagnosis of sepsis. Diagnosis of bacterial sepsis or infection. More accurate in more severe illness.[61] PCT cut-off for sepsis, 1.1 ng/mL[43]; 1.57 ng/mL[61] • ↑ Concentrations in patients with sepsis and infection[77] • Distinction between patients with sepsis and patients without sepsis in the ICU ↑ values in septic shock, sepsis, and controls (17.1, 1.8, and 0.04 ng/mL, respectively)[78] |
|
sTREM-1 |
Sepsis indicator.[61] [79] [80] An early distinction between sepsis and SIRS predictive of septic shock. |
|
Pancreatic stone protein (PSP) |
C-type lectin protein that triggers polymorphonuclear cell activation. Serial measurements are potentially useful to predict sepsis 3 days before clinical diagnosis.[73] |
|
sPD-L1 |
Indicates sepsis-associated immunoparalysis (immunosuppression)[81] [82] Cut-off of 0.16 ng/mL, ↑ sPD-L1 immunosuppression phenotype.[82] |
|
IL-10 |
Levels correlate with the hypoinflammatory phenotype.[82] [83] |
|
IL-1β and IL-6 |
|
|
Pentraxin-3 |
Predicts the risk of sepsis in patients with suspected infection in the emergency department.[86] Sepsis versus SIRS.[87] |
|
Calprotectin |
Better distinction between sepsis versus nonsepsis patients in the ICU than PCT. Distinction between sepsis and trauma patients.[88] |
|
Bio-adrenomedullin |
Useful to distinguish sepsis, septic shock, and nonsepsis patients (74, 107, and 29 pg/mL, respectively).[89] |
|
Resistin (and eNamp) |
|
|
suPAR |
Risk of patients with suspected infection.[92] |
|
LDL-C |
Protective effect against sepsis.[93] Low values can reflect a risk of sepsis and admission to the ICU. Risk of sepsis (OR: 0.86) and admission to the ICU (OR: 0.85). The lower quartile had a greater risk of sepsis (OR: 1.48) and admission to the ICU (OR: 1.45) vs. the highest quartile, considering other comorbidities. |
|
Presepsin |
Plasma levels are considered a biomarker of the activation of innate immune effector cells in response to invasive organisms. Biomarker of phagocytosis.[94] [95] High accuracy (AUROC 0.954) for prediction of sepsis risk, an early diagnosis.[96] [97] ↑ Presepsin in sepsis patients compared to nonsepsis SIRS. |
|
CD64 |
High-affinity Fcγ receptor I in neutrophils upregulated in the early stages of activation of the innate immune response. AUROC 0.879 of nCD64 for diagnosis of bacterial infection.[78] |
|
↑CD68 |
Increased in the hippocampus, putamen, and cerebellum in patients with sepsis.[98] |
|
VLA-3 (a3β1) |
Indicative of sepsis.[99] [100] Discrimination of sepsis and SIRS. Increased α3β1 (VLA-3, CD49c/CD29) on neutrophils of septic patients. ↑ β1 (CD29), on neutrophils of sepsis patients.[100] |
|
↑ sTNFR-1 |
Distinguish sepsis from nonsepsis SIRS.[101] |
|
↓ miR-125 |
Good predictive values for sepsis risk.[102] |
|
↑lnc-ANRIL/miR-125a axis |
Determine the risk for sepsis.[103] |
|
miR-125a and miR-125b |
Useful to distinguish sepsis from other SIRS states.[103] |
|
↑ Lnc-MALAT1/miR-125a |
Increased levels in sepsis and risk of sepsis.[76] |
|
Lnc-MALAT1/miRNA-125a |
Discriminates sepsis patients from healthy controls. Reflects inflammation level.[76] |
|
lnc-MEG3 |
Increased values are predictive of sepsis risk. Lnc-MEG3 is a potential biomarker for the prediction of sepsis via interacting with miR-21.[104] |
|
Genetic polymorphisms |
The expressions of inflammatory mediators, microRNA expression, and other mechanisms have been described as a tool for predicting sepsis responses in infected patients.[74] |
Abbreviations: ICU, intensive care unit; OR, odds ratio; PCT, procalcitonin; SIRS, systemic inflammatory response syndrome.
Advances in the understanding of the genetic basis for sepsis activation of the innate immune response,[74] the release of acute phase reactants, knowledge of biomarkers involved in the pathophysiology of sepsis, and the serum levels of glycoproteins on cell membranes have allowed for the study of different molecules and genes encoding those molecules (e.g., proteins, cytokines, soluble receptors, chemokines) as sepsis-predictive biomarkers. Of note, newer potentially predictive biomarkers have been validated in comparison with the gold standard for screening in sepsis (clinical scores), though others have been studied prospectively as predictors of sepsis risk, which correlate with mortality risk.[75]
More recent advances in gene expression and transcriptomics have led to the identification of new classes of biomarkers, such as microRNAs, long-noncoding RNAs, or the human microbiome. Noncoding RNAs have been studied as early predictive sepsis biomarkers. The expression of the Lnc-MALAT1/miR-125a axis discriminates between sepsis patients and healthy controls and is associated with an excellent diagnostic yield (AUROC of 0.931, 95% CI: 0.908–0.954).[76]
Given that a significant proportion of patients with early sepsis do not show clinical signs but do develop an immunopathogenic phenotype leading to dysregulated organ dysfunction and increased mortality, the most sophisticated prediction models have proposed the use of clinical parameters with a panel of genes encoding inflammatory biomarkers.[105] The most important disadvantages of these models are the high cost and difficulties in sample processing, laboratory testing, and lack of availability for all hospital (or prehospital) settings. Predictive biomarkers have been studied compared to clinical scores rather than in prospective cohorts of infected patients and their clinical trajectories.
Novel technologies are poorly affordable in middle- or low-resource settings, which account for 85% of sepsis cases.[1] Their lack of validity in prehospital settings or ED is outstanding. In such settings, an objective and quick tool is highly needed for the early triage of patients. Important studies exist on the potential immune response biomarkers for the prediction of sepsis. However, they have been performed preferably in hospitalized patients or later in the ICU.[82] [88]
Heterogeneity in critically ill patients with sepsis involves a new paradigm with clinical applications, as it has contributed to the challenging task of finding a perfect combination of biomarkers. Novel genetic studies may enable better characterization of different panels of biomarkers at the time of a specific infection to predict the risk of sepsis. Identifying unique biological signatures in patients could enhance selected enrollment in clinical trials and strengthen our diagnosis and early detection approaches.[106] Most importantly, the clinical applicability of new discoveries is a sine qua non to revolutionize sepsis management and reduce deaths.
Rapid Microbiological Diagnosis as an Element for Sepsis Prediction
Early identification of causative microorganisms in suspected sepsis is needed to optimize antimicrobial use and patient survival. However, current culture-based pathogen identification often takes at least 24 to 48 hours to give meaningful results, weakening their usefulness in decision-making to start antimicrobial treatment, thus, broad-spectrum antibiotics are often used to ensure coverage of all potential organisms, implying risks of overtreatment, toxicity, and selection of multidrug-resistant bacteria. Furthermore, previous or current antimicrobial treatment decreases these tests' sensitivity. Empirical broad-spectrum antimicrobial treatment leads to overtreatment in 60 to 70% of conditions that mimic sepsis, such as other inflammatory states, or secondary to less severe viral or susceptible bacterial infections.[107]
The clinical need for a faster microbiological approach to target treatments early in the course of infections potentiated the therapeutic advantages of new microbiological technologies, such as RDT.[108] Pathogen molecular diagnostic tests speed up the time to identification of pathogens and their susceptibility to antibiotic and eventually targeted treatment.[109] There is a lack of evidence on the clinical impact of RDT in sepsis patients. Most data have been extracted from studies performed in infections, such as bacteremia or pneumonia, that could lead to sepsis.
Previous studies of matrix-associated laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) have been successful in the management of bloodstream infections.[110] [111] [112] A previous meta-analysis and other studies showed that antimicrobial stewardship programs are associated with reduced mortality, time to optimal treatment and length of stay, and are cost-effective.[112] [113] [114] Patients with sepsis and gram-negative bacteremia may benefit from RDT due to the wide range of possible infecting pathogens and the implications of inappropriate treatment in the context of drug resistance. Previous studies of patients with drug-resistant gram-negative bacteremia have shown earlier initiation of appropriate therapy, shortened length of stay, and reduced 30-day mortality.[115] MALDI-TOF MS has been studied for rapid identification of antimicrobial susceptibility; however, some misclassifications have been observed, and the accuracy of this method needs to be improved.[108] [116] There is a lack of studies evaluating MALDI-TOF MS in sepsis. In the study of Verroken et al,[117] the authors assessed the impact of MALDI-TOF MS results in the management workflow of antimicrobial stewardship in sepsis patients with positive blood cultures to Enterobacteriaceae, Pseudomonas aeruginosa, and Staphylococcus aureus. The mean time to pathogen identification was reduced by 61 to 65% (10.8 hours). The mean time to optimal treatment was decreased significantly. The impact on mortality was not assessed.
Multiplex polymerase chain reaction (PCR) has been previously studied for the rapid identification of S. aureus and its resistance patterns. The FilmArray Blood Culture ID Panel (BCID), which can identify 24 different bacteria, fungi, and common antimicrobial resistance genes (KPC, mecA, and vanA/B) within 1 hour of organism growth in blood cultures, was evaluated in the randomized Blood Culture Identification trial.[118] In this study, the molecular technique reduced the time to targeted treatment, decreased the use of broad-spectrum antibiotics, and contributed to antimicrobial de-escalation.
There is a paucity of evidence on gram-negative pathogen identification in sepsis using PCR.[118] [119] [120] [121] [122] In the study of Vincent et al,[123] the use of culture-independent PCR/electrospray ionization-mass spectrometry technology resulted in rapid pathogen identification in critically ill patients. The authors tested different sources of infection (e.g., pneumonia: 185 cases, blood stream: 616 cases, sterile fluid: 110 cases, and tissue infection: 529 cases) in critically ill patients. The study reported the effectiveness of PCR to rule out infection within 6 hours compared with standard culture-based microbiological testing, with a sensitivity of 81%, a specificity of 69%, and a negative predictive value of 97%. In a study of 617 patients with positive Gram stains in blood cultures, BCID resulted in faster pathogen identification than standard blood cultures and usual susceptibility testing, which improved antimicrobial de-escalation. The T2Bacteria Panel (including the identification of Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Enterococcus faecium, and S. aureus), identified the causative pathogen in whole blood samples at a mean of 3.6 to 7.7 hours compared with almost 72 hours with standard blood cultures.[122]
Ideally, RDT should provide pathogen species and data on antimicrobial susceptibility, such as Accelerate Pheno system (APS; Accelerate Diagnostics, Denver, CO), an automated system that reduces the time to pathogen identification and gives susceptibility data (at 27 and 40 hours, respectively) compared with conventional cultures.[124] This system has been approved by the Food and Drug Administration in 2017 for testing in blood.
There are some drawbacks regarding the use of RDT. These tests are not specific to sepsis and are not useful for making a differential diagnosis between three conditions: colonization, infection, and sepsis. Likewise, RDTs have led to overdiagnosis and overtreatment.[125] Data on clinical benefit and cost-effectiveness are still emerging. Costs and microbiology lab expertise in molecular techniques are also seen as a barrier to their widespread use, particularly in low-resource settings. None of these technologies have approached the point of care, nor can they be described as genuinely culture-independent diagnostic tests. Evidence on their effectiveness in improving mortality is conflicting and should be further studied.[121] A recent systematic review of RDT in sepsis[126] reported improvements in appropriate antimicrobial therapy, nonsignificant change in time to targeted therapy, decreased length of stay in two studies, and a significant decrease in antimicrobial cost in six studies. The impact on mortality was unclear. This study has important limitations on the number of studies included and high heterogeneity.
RDTs per se are not useful for diagnosing a specific immunopathogenic state that predisposes patients to a significant risk of death, such as sepsis. More specific biomarkers recently identified reflect the immunopathologic state leading to sepsis, which is triggered by the interaction of infectious agents and the innate immune system.
Inflammatory biomarker-enhanced RDT will aid in very early diagnosis or prediction of sepsis before overt clinical consequences, differentiating sepsis from other acute inflammatory conditions, identifying and quantifying the causative organism, determining resistance patterns early to target treatments from time zero, improving antimicrobial stewardship practices, and monitoring patient progression. Combining point-of-care RDT tests and more specific inflammatory biomarkers is a novel strategy to enhance biomarkers' availability and affordability for earlier sepsis diagnosis in ED. This can improve time to diagnosis (up to 10 times faster when compared with the gold standard),[73] faster detection of pathogens,[127] quick resistance profiles, and detection and rapid monitoring of specific biomarkers. Precision medicine has developed tools to identify new cases, predict prognosis, and target treatments according to their clinical and molecular phenotypes.[128] [129] Multiplex point-of-care devices and other theragnostic approaches are integrated approaches that gather data for early diagnosis and classification of sepsis (e.g., inflammatory and organ dysfunction biomarkers and microbiological diagnosis).[130]
Monitoring different biomarkers gives a holistic view of patients' clinical status and prognosis. Integrated point-of-care biomarkers are promising for democratizing novel theragnostic tools and developing precision medicine elsewhere. To improve their applicability in different settings, further clinical studies assessing the effectiveness of these innovative techniques are needed. Widely available and affordable combinations of RDT and predictive biomarkers (e.g., predictive biomarker-enhanced RDT point-of-care tests) should be further studied and clinically validated and promise to be the game changer in sepsis diagnosis.
Conclusion
Early sepsis prediction is still in its first stages, and it remains a complex field for clinicians and researchers. In recent years, an increasing interest has evolved in techniques to improve sepsis definition, prediction, early diagnosis, classification of patients, defining prognosis, and personalizing treatment. Novel developments and deep study of point-of-care biomarkers have been promising to enhance the accuracy of near-patient diagnoses. The continuous developments of point-of-care tools using widely applicable and affordable combinations of biomarkers and faster techniques for accurate microbiological information have driven new insights for sepsis management.
Conflict of interest
R.F. and J.C.R. have received honoraria from Biomerieux. E.P.P. has shares in Loop Diagnostics. However, the authors do not recommend any specific product or brand in this review.
-
References
- 1 Rudd KE, Johnson SC, Agesa KM. et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet 2020; 395 (10219): 200-211
- 2 Rüddel H, Thomas-Rüddel DO, Reinhart K. et al; MEDUSA study group. Adverse effects of delayed antimicrobial treatment and surgical source control in adults with sepsis: results of a planned secondary analysis of a cluster-randomized controlled trial. Crit Care 2022; 26 (01) 51
- 3 Mensa J, Barberán J, Ferrer R. et al. Recommendations for antibiotic selection for severe nosocomial infections. Rev Esp Quimioter 2021; 34 (05) 511-524
- 4 Prescott HC, Angus DC. Enhancing recovery from sepsis: a review. JAMA 2018; 319 (01) 62-75
- 5 Seymour CW, Gesten F, Prescott HC. et al. Time to treatment and mortality during mandated emergency care for sepsis. N Engl J Med 2017; 376 (23) 2235-2244
- 6 Evans L, Rhodes A, Alhazzani W. et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med 2021; 47 (11) 1181-1247
- 7 Carlbom DJ, Rubenfeld GD. Barriers to implementing protocol-based sepsis resuscitation in the emergency department–results of a national survey. Crit Care Med 2007; 35 (11) 2525-2532
- 8 Simmonds M, Hutchinson A, Chikhani M. et al. Surviving sepsis beyond intensive care: a retrospective cohort study of compliance with the international guidelines. J Intensive Care Soc 2008; 9: 124-127
- 9 Ferrer R, González Del Castillo J, Martínez-Martínez M, Plata-Menchaca EP, Larrosa MN. Time to decision in sepsis. Rev Esp Quimioter 2023; 36 (01) 82-87
- 10 Singer M, Deutschman CS, Seymour CW. et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016; 315 (08) 801-810
- 11 Prescott HC, Cope TM, Gesten FC. et al. Reporting of sepsis cases for performance measurement versus for reimbursement in New York State. Crit Care Med 2018; 46 (05) 666-673
- 12 Kim SJ, Hwang SO, Kim YW, Lee JH, Cha KC. Procalcitonin as a diagnostic marker for sepsis/septic shock in the emergency department; a study based on Sepsis-3 definition. Am J Emerg Med 2019; 37 (02) 272-276
- 13 Suffoletto B, Frisch A, Prabhu A, Kristan J, Guyette FX, Callaway CW. Prediction of serious infection during prehospital emergency care. Prehosp Emerg Care 2011; 15 (03) 325-330
- 14 Kwizera A, Adhikari NKJ, Angus DC. et al. Recognition of sepsis in resource-limited settings. 2019 Feb 9. In: Dondorp AM, Dünser MW, Schultz MJ. eds. Sepsis Management in Resource-limited Settings [Internet]. Cham: Springer; 2019. . Chapter 4
- 15 Kaukonen KM, Bailey M, Pilcher D, Cooper DJ, Bellomo R. Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med 2015; 372 (17) 1629-1638
- 16 Machado FR, Cavalcanti AB, Monteiro MB. et al; Instituto Latino-Americano de Sepsis network investigators. Predictive accuracy of the quick sepsis-related organ failure assessment score in Brazil. a prospective multicenter study. Am J Respir Crit Care Med 2020; 201 (07) 789-798
- 17 Seymour CW, Liu VX, Iwashyna TJ. et al. Assessment of clinical criteria for sepsis: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016; 315 (08) 762-774
- 18 Briassoulis G, Briassoulis P, Miliaraki M. et al; Combined Approach for The eArly diagnosis of INfection in sepsis (CAPTAIN) study group. Biomarker cruises in sepsis: who is the CAPTAIN? Discussion on “Circulating biomarkers may be unable to detect infection at the early phase of sepsis in ICU patients: the CAPTAIN prospective multicenter cohort study”. Intensive Care Med 2019; 45 (01) 132-133
- 19 Klimpel J, Weidhase L, Bernhard M, Gries A, Petros S. The impact of the Sepsis-3 definition on ICU admission of patients with infection. Scand J Trauma Resusc Emerg Med 2019; 27 (01) 98
- 20 Peake SL, Delaney A, Bailey M. et al; ARISE Investigators, ANZICS Clinical Trials Group. Goal-directed resuscitation for patients with early septic shock. N Engl J Med 2014; 371 (16) 1496-1506
- 21 Herwanto V, Shetty A, Nalos M. et al. Accuracy of quick sequential organ failure assessment score to predict sepsis mortality in 121 studies including 1,716,017 individuals: a systematic review and meta-analysis. Crit Care Explor 2019; 1 (09) e0043
- 22 Serafim R, Gomes JA, Salluh J, Póvoa P. A comparison of the Quick-SOFA and systemic inflammatory response syndrome criteria for the diagnosis of sepsis and prediction of mortality: a systematic review and meta-analysis. Chest 2018; 153 (03) 646-655
- 23 Fernando SM, Tran A, Taljaard M. et al. Prognostic accuracy of the quick sequential organ failure assessment for mortality in patients with suspected infection: a systematic review and meta-analysis. Ann Intern Med 2018; 168 (04) 266-275
- 24 Liu VX, Lu Y, Carey KA. et al. Comparison of early warning scoring systems for hospitalized patients with and without infection at risk for in-hospital mortality and transfer to the intensive care unit. JAMA Netw Open 2020; 3 (05) e205191
- 25 Inada-Kim M. NEWS2 and improving outcomes from sepsis. Clin Med (Lond) 2022; 22 (06) 514-517
- 26 Alberto L, Marshall AP, Walker R, Aitken LM. Screening for sepsis in general hospitalized patients: a systematic review. J Hosp Infect 2017; 96 (04) 305-315
- 27 Bhattacharjee P, Edelson DP, Churpek MM. Identifying patients with sepsis on the hospital wards. Chest 2017; 151 (04) 898-907
- 28 Makam AN, Nguyen OK, Auerbach AD. Diagnostic accuracy and effectiveness of automated electronic sepsis alert systems: a systematic review. J Hosp Med 2015; 10 (06) 396-402
- 29 Downing NL, Rolnick J, Poole SF. et al. Electronic health record-based clinical decision support alert for severe sepsis: a randomised evaluation. BMJ Qual Saf 2019; 28 (09) 762-768
- 30 Hooper MH, Weavind L, Wheeler AP. et al. Randomized trial of automated, electronic monitoring to facilitate early detection of sepsis in the intensive care unit*. Crit Care Med 2012; 40 (07) 2096-2101
- 31 Shimabukuro DW, Barton CW, Feldman MD, Mataraso SJ, Das R. Effect of a machine learning-based severe sepsis prediction algorithm on patient survival and hospital length of stay: a randomised clinical trial. BMJ Open Respir Res 2017; 4 (01) e000234
- 32 Esteban E, Belda S, García-Soler P. et al. A multifaceted educational intervention shortened time to antibiotic administration in children with severe sepsis and septic shock: ABISS Edusepsis pediatric study. Intensive Care Med 2017; 43 (12) 1916-1918
- 33 Ferrer R, Artigas A, Levy MM. et al; Edusepsis Study Group. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA 2008; 299 (19) 2294-2303
- 34 Yébenes JC, Lorencio C, Esteban E. et al; Comisión Asesora para la Atención al Paciente con Sepsis y Grup de Treball de Sèpsia i Xoc Sèptic (GTSiXS) SOCMIC-SOCMUE. Interhospital Sepsis Code in Catalonia (Spain): territorial model for initial care of patients with sepsis. Med Intensiva (Engl Ed) 2020; 44 (01) 36-45
- 35 Damiani E, Donati A, Serafini G. et al. Effect of performance improvement programs on compliance with sepsis bundles and mortality: a systematic review and meta-analysis of observational studies. PLoS One 2015; 10 (05) e0125827
- 36 Ferrer R, Ruiz-Rodriguez JC, Larrosa N, Llaneras J, Molas E, González-López JJ. Sepsis code implementation at Vall d'Hebron University Hospital: rapid diagnostics key to success. ICU Management & Practice 2017; 17 (04) 214-215
- 37 Weiss SL, Peters MJ, Alhazzani W. et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Med 2020; 46 (Suppl. 01) 10-67
- 38 Chiscano-Camón L, Plata-Menchaca E, Ruiz-Rodríguez JC, Ferrer R. Fisiopatología del shock séptico. Med Intensiva (Engl Ed) 2022; 46 (Suppl. 01) 1-13
- 39 Wang C, Xu R, Zeng Y, Zhao Y, Hu X. A comparison of qSOFA, SIRS and NEWS in predicting the accuracy of mortality in patients with suspected sepsis: a meta-analysis. PLoS One 2022; 17 (04) e0266755
- 40 Ventura F, Pugin J, Tissieres P. ICU Management & Practice, 2021; 23. Accessed July 2, 2023 at: https://healthmanagement.org/c/icu/issuearticle/sepsis-diagnosis-clinical-signs-scores-and-biomarkers
- 41 Simon L, Gauvin F, Amre DK, Saint-Louis P, Lacroix J. Serum procalcitonin and C-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysis. Clin Infect Dis 2004; 39 (02) 206-217
- 42 Kondo Y, Umemura Y, Hayashida K, Hara Y, Aihara M, Yamakawa K. Diagnostic value of procalcitonin and presepsin for sepsis in critically ill adult patients: a systematic review and meta-analysis. J Intensive Care 2019; 7: 22
- 43 Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis. Lancet Infect Dis 2013; 13 (05) 426-435
- 44 Plata-Menchaca EP, Ferrer R. Procalcitonin is useful for antibiotic deescalation in sepsis. Crit Care Med 2021; 49 (04) 693-696
- 45 Layios N, Lambermont B, Canivet JL. et al. Procalcitonin usefulness for the initiation of antibiotic treatment in intensive care unit patients. Crit Care Med 2012; 40 (08) 2304-2309
- 46 Schuetz P, Beishuizen A, Broyles M. et al. Procalcitonin (PCT)-guided antibiotic stewardship: an international experts consensus on optimized clinical use. Clin Chem Lab Med 2019; 57 (09) 1308-1318
- 47 Yu H, Nie L, Liu A. et al. Combining procalcitonin with the qSOFA and sepsis mortality prediction. Medicine (Baltimore) 2019; 98 (23) e15981
- 48 Kalil AC, Metersky ML, Klompas M. et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis 2016; 63 (05) e61-e111
- 49 Torres A, Niederman MS, Chastre J. et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J 2017; 50 (03) 50
- 50 Póvoa P, Coelho L, Dal-Pizzol F. et al. How to use biomarkers of infection or sepsis at the bedside: guide to clinicians. Intensive Care Med 2023; 49 (02) 142-153
- 51 Christ-Crain M, Opal SM. Clinical review: the role of biomarkers in the diagnosis and management of community-acquired pneumonia. Crit Care 2010; 14 (01) 203
- 52 Kamat IS, Ramachandran V, Eswaran H, Guffey D, Musher DM. Procalcitonin to distinguish viral from bacterial pneumonia: a systematic review and meta-analysis. Clin Infect Dis 2020; 70 (03) 538-542
- 53 Meier MA, Branche A, Neeser OL. et al. Procalcitonin-guided antibiotic treatment in patients with positive blood cultures: a patient-level meta-analysis of randomized trials. Clin Infect Dis 2019; 69 (03) 388-396
- 54 Kennis B, Ali A, Lasoff D, Sweeney DA, Wardi G. The diagnostic utility of procalcitonin is limited in the setting of methamphetamine toxicity. Am J Emerg Med 2022; 54: 36-40
- 55 Wirz Y, Meier MA, Bouadma L. et al. Effect of procalcitonin-guided antibiotic treatment on clinical outcomes in intensive care unit patients with infection and sepsis patients: a patient-level meta-analysis of randomized trials. Crit Care 2018; 22 (01) 191
- 56 Kyriazopoulou E, Liaskou-Antoniou L, Adamis G. et al. Procalcitonin to reduce long-term infection-associated adverse events in sepsis: a randomized trial. Am J Respir Crit Care Med 2021; 203 (02) 202-210
- 57 de Jong E, van Oers JA, Beishuizen A. et al. Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: a randomised, controlled, open-label trial. Lancet Infect Dis 2016; 16 (07) 819-827
- 58 Huang Q, Xiong H, Yan P. et al. The diagnostic and prognostic value of suPAR in patients with sepsis: a systematic review and meta-analysis. Shock 2020; 53 (04) 416-425
- 59 Bleharski JR, Kiessler V, Buonsanti C. et al. A role for triggering receptor expressed on myeloid cells-1 in host defense during the early-induced and adaptive phases of the immune response. J Immunol 2003; 170 (07) 3812-3818
- 60 Gómez-Piña V, Soares-Schanoski A, Rodríguez-Rojas A. et al. Metalloproteinases shed TREM-1 ectodomain from lipopolysaccharide-stimulated human monocytes. J Immunol 2007; 179 (06) 4065-4073
- 61 Aksaray S, Alagoz P, Inan A, Cevan S, Ozgultekin A. Diagnostic value of sTREM-1 and procalcitonin levels in the early diagnosis of sepsis. North Clin Istanb 2017; 3 (03) 175-182
- 62 Julián-Jiménez A, Yañez MC, González-Del Castillo J. et al; en representación del grupo INFURG-SEMES. Prognostic power of biomarkers for short-term mortality in the elderly patients seen in Emergency Departments due to infections. Enferm Infecc Microbiol Clin (Engl Ed) 2019; 37 (01) 11-18
- 63 Baldirà J, Ruiz-Rodríguez JC, Wilson DC. et al. Biomarkers and clinical scores to aid the identification of disease severity and intensive care requirement following activation of an in-hospital sepsis code. Ann Intensive Care 2020; 10 (01) 7
- 64 Baldirà J, Ruiz-Rodríguez JC, Ruiz-Sanmartin A. et al. Use of biomarkers to improve 28-day mortality stratification in patients with sepsis and SOFA ≤ 6. Biomedicines 2023; 11 (08) 11
- 65 Hotchkiss RS, Moldawer LL, Opal SM, Reinhart K, Turnbull IR, Vincent JL. Sepsis and septic shock. Nat Rev Dis Primers 2016; 2: 16045
- 66 Munoz C, Carlet J, Fitting C, Misset B, Blériot JP, Cavaillon JM. Dysregulation of in vitro cytokine production by monocytes during sepsis. J Clin Invest 1991; 88 (05) 1747-1754
- 67 Shapiro NI, Trzeciak S, Hollander JE. et al. A prospective, multicenter derivation of a biomarker panel to assess risk of organ dysfunction, shock, and death in emergency department patients with suspected sepsis. Crit Care Med 2009; 37 (01) 96-104
- 68 Dolin HH, Papadimos TJ, Stepkowski S, Chen X, Pan ZK. A novel combination of biomarkers to herald the onset of sepsis prior to the manifestation of symptoms. Shock 2018; 49 (04) 364-370
- 69 Parlato M, Philippart F, Rouquette A. et al; Captain Study Group. Circulating biomarkers may be unable to detect infection at the early phase of sepsis in ICU patients: the CAPTAIN prospective multicenter cohort study. Intensive Care Med 2018; 44 (07) 1061-1070
- 70 Teggert A, Datta H, Ali Z. Biomarkers for point-of-care diagnosis of sepsis. Micromachines (Basel) 2020; 11 (03) 11
- 71 Kim M, Song KH, Kim CJ. et al. Electronic alerts with automated consultations promote appropriate antimicrobial prescriptions. PLoS One 2016; 11 (08) e0160551
- 72 Adams R, Henry KE, Sridharan A. et al. Prospective, multi-site study of patient outcomes after implementation of the TREWS machine learning-based early warning system for sepsis. Nat Med 2022; 28 (07) 1455-1460
- 73 Pugin J, Daix T, Pagani JL. et al. Serial measurement of pancreatic stone protein for the early detection of sepsis in intensive care unit patients: a prospective multicentric study. Crit Care 2021; 25 (01) 151
- 74 David VL, Ercisli MF, Rogobete AF. et al. Early prediction of sepsis incidence in critically ill patients using specific genetic polymorphisms. Biochem Genet 2017; 55 (03) 193-203
- 75 D'Onofrio V, Heylen D, Pusparum M. et al. A prospective observational cohort study to identify inflammatory biomarkers for the diagnosis and prognosis of patients with sepsis. J Intensive Care 2022; 10 (01) 13
- 76 Liu W, Geng F, Yu L. Long non-coding RNA MALAT1/microRNA 125a axis presents excellent value in discriminating sepsis patients and exhibits positive association with general disease severity, organ injury, inflammation level, and mortality in sepsis patients. J Clin Lab Anal 2020; 34 (06) e23222
- 77 Assicot M, Gendrel D, Carsin H, Raymond J, Guilbaud J, Bohuon C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet 1993; 341 (8844) 515-518
- 78 Yin WP, Li JB, Zheng XF, An L, Shao H, Li CS. Effect of neutrophil CD64 for diagnosing sepsis in emergency department. World J Emerg Med 2020; 11 (02) 79-86
- 79 Brenner T, Uhle F, Fleming T. et al. Soluble TREM-1 as a diagnostic and prognostic biomarker in patients with septic shock: an observational clinical study. Biomarkers 2017; 22 (01) 63-69
- 80 Su L, Liu D, Chai W, Liu D, Long Y. Role of sTREM-1 in predicting mortality of infection: a systematic review and meta-analysis. BMJ Open 2016; 6 (05) e010314
- 81 Liu M, Zhang X, Chen H. et al. Serum sPD-L1, upregulated in sepsis, may reflect disease severity and clinical outcomes in septic patients. Scand J Immunol 2017; 85 (01) 66-72
- 82 Yende S, Kellum JA, Talisa VB. et al. Long-term host immune response trajectories among hospitalized patients with sepsis. JAMA Netw Open 2019; 2 (08) e198686
- 83 Hoppensteadt D, Tsuruta K, Hirman J, Kaul I, Osawa Y, Fareed J. Dysregulation of inflammatory and hemostatic markers in sepsis and suspected disseminated intravascular coagulation. Clin Appl Thromb Hemost 2015; 21 (02) 120-127
- 84 Matsumoto H, Ogura H, Shimizu K. et al. The clinical importance of a cytokine network in the acute phase of sepsis. Sci Rep 2018; 8 (01) 13995
- 85 Barre M, Behnes M, Hamed S. et al. Revisiting the prognostic value of monocyte chemotactic protein 1 and interleukin-6 in the sepsis-3 era. J Crit Care 2018; 43: 21-28
- 86 Uusitalo-Seppälä R, Huttunen R, Aittoniemi J. et al. Pentraxin 3 (PTX3) is associated with severe sepsis and fatal disease in emergency room patients with suspected infection: a prospective cohort study. PLoS One 2013; 8 (01) e53661
- 87 Hamed S, Behnes M, Pauly D. et al. Pentraxin-3 predicts short- and mid-term mortality in patients with sepsis and septic shock during intensive care treatment. Clin Lab 2018; 64 (06) 999-1011
- 88 Larsson A, Tydén J, Johansson J. et al. Calprotectin is superior to procalcitonin as a sepsis marker and predictor of 30-day mortality in intensive care patients. Scand J Clin Lab Invest 2020; 80 (02) 156-161
- 89 Lundberg OHM, Lengquist M, Spångfors M. et al. Circulating bioactive adrenomedullin as a marker of sepsis, septic shock and critical illness. Crit Care 2020; 24 (01) 636
- 90 Karampela I, Christodoulatos GS, Kandri E. et al. Circulating eNampt and resistin as a proinflammatory duet predicting independently mortality in critically ill patients with sepsis: a prospective observational study. Cytokine 2019; 119: 62-70
- 91 Saboktakin L, Bilan N, Ghalehgolab Behbahan A, Poorebrahim S. Relationship between resistin levels and sepsis among children under 12 years of age: a case control study. Front Pediatr 2019; 7: 355
- 92 Eugen-Olsen J, Giamarellos-Bourboulis EJ. suPAR: the unspecific marker for disease presence, severity and prognosis. Int J Antimicrob Agents 2015; 46 (Suppl. 01) S33-S34
- 93 Feng Q, Wei WQ, Chaugai S. et al. Association between low-density lipoprotein cholesterol levels and risk for sepsis among patients admitted to the hospital with infection. JAMA Netw Open 2019; 2 (01) e187223
- 94 Urbonas V, Eidukaitė A, Tamulienė I. The predictive value of soluble biomarkers (CD14 subtype, interleukin-2 receptor, human leucocyte antigen-G) and procalcitonin in the detection of bacteremia and sepsis in pediatric oncology patients with chemotherapy-induced febrile neutropenia. Cytokine 2013; 62 (01) 34-37
- 95 Arai Y, Mizugishi K, Nonomura K, Naitoh K, Takaori-Kondo A, Yamashita K. Phagocytosis by human monocytes is required for the secretion of presepsin. J Infect Chemother 2015; 21 (08) 564-569
- 96 Lu B, Zhang Y, Li C. et al. The utility of presepsin in diagnosis and risk stratification for the emergency patients with sepsis. Am J Emerg Med 2018; 36 (08) 1341-1345
- 97 Memar MY, Baghi HB. Presepsin: a promising biomarker for the detection of bacterial infections. Biomed Pharmacother 2019; 111: 649-656
- 98 Westhoff D, Engelen-Lee JY, Hoogland ICM. et al. Systemic infection and microglia activation: a prospective postmortem study in sepsis patients. Immun Ageing 2019; 16: 18
- 99 Lerman YV, Lim K, Hyun Y-M. et al. Sepsis lethality via exacerbated tissue infiltration and TLR-induced cytokine production by neutrophils is integrin α3β1-dependent. Blood 2014; 124 (24) 3515-3523
- 100 Sarangi PP, Hyun YM, Lerman YV, Pietropaoli AP, Kim M. Role of β1 integrin in tissue homing of neutrophils during sepsis. Shock 2012; 38 (03) 281-287
- 101 Mikacenic C, Hahn WO, Price BL. et al. Biomarkers of endothelial activation are associated with poor outcome in critical illness. PLoS One 2015; 10 (10) e0141251
- 102 Gui F, Peng H, Liu Y. Elevated circulating lnc-ANRIL/miR-125a axis level predicts higher risk, more severe disease condition, and worse prognosis of sepsis. J Clin Lab Anal 2019; 33 (06) e22917
- 103 Zhao D, Li S, Cui J, Wang L, Ma X, Li Y. Plasma miR-125a and miR-125b in sepsis: Correlation with disease risk, inflammation, severity, and prognosis. J Clin Lab Anal 2020; 34 (02) e23036
- 104 Na L, Ding H, Xing E. et al. Lnc-MEG3 acts as a potential biomarker for predicting increased disease risk, systemic inflammation, disease severity, and poor prognosis of sepsis via interacting with miR-21. J Clin Lab Anal 2020; 34 (04) e23123
- 105 Tuerxun K, Eklund D, Wallgren U. et al. Predicting sepsis using a combination of clinical information and molecular immune markers sampled in the ambulance. Sci Rep 2023; 13 (01) 14917
- 106 Leligdowicz A, Matthay MA. Heterogeneity in sepsis: new biological evidence with clinical applications. Crit Care 2019; 23 (01) 80
- 107 Klein Klouwenberg PM, Cremer OL, van Vught LA. et al. Likelihood of infection in patients with presumed sepsis at the time of intensive care unit admission: a cohort study. Crit Care 2015; 19 (01) 319
- 108 Luethy PM, Johnson JK. The use of matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) for the identification of pathogens causing sepsis. J Appl Lab Med 2019; 3 (04) 675-685
- 109 Timbrook TT, Morton JB, McConeghy KW, Caffrey AR, Mylonakis E, LaPlante KL. The effect of molecular rapid diagnostic testing on clinical outcomes in bloodstream infections: a systematic review and meta-analysis. Clin Infect Dis 2017; 64 (01) 15-23
- 110 Vlek AL, Bonten MJ, Boel CH. Direct matrix-assisted laser desorption ionization time-of-flight mass spectrometry improves appropriateness of antibiotic treatment of bacteremia. PLoS One 2012; 7 (03) e32589
- 111 Clec'h C, Ferriere F, Karoubi P. et al. Diagnostic and prognostic value of procalcitonin in patients with septic shock. Crit Care Med 2004; 32 (05) 1166-1169
- 112 Huang AM, Newton D, Kunapuli A. et al. Impact of rapid organism identification via matrix-assisted laser desorption/ionization time-of-flight combined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia. Clin Infect Dis 2013; 57 (09) 1237-1245
- 113 Bookstaver PB, Nimmich EB, Smith III TJ. et al. Cumulative effect of an antimicrobial stewardship and rapid diagnostic testing bundle on early streamlining of antimicrobial therapy in gram-negative bloodstream infections. Antimicrob Agents Chemother 2017; 61 (09) 61
- 114 Perez KK, Olsen RJ, Musick WL. et al. Integrating rapid pathogen identification and antimicrobial stewardship significantly decreases hospital costs. Arch Pathol Lab Med 2013; 137 (09) 1247-1254
- 115 Perez KK, Olsen RJ, Musick WL. et al. Integrating rapid diagnostics and antimicrobial stewardship improves outcomes in patients with antibiotic-resistant Gram-negative bacteremia. J Infect 2014; 69 (03) 216-225
- 116 Jung JS, Hamacher C, Gross B. et al. Evaluation of a semiquantitative matrix-assisted laser desorption ionization-time of flight mass spectrometry method for rapid antimicrobial susceptibility testing of positive blood cultures. J Clin Microbiol 2016; 54 (11) 2820-2824
- 117 Verroken A, Defourny L, le Polain de Waroux O. et al. Clinical Impact of MALDI-TOF MS Identification and Rapid Susceptibility Testing on Adequate Antimicrobial Treatment in Sepsis with Positive Blood Cultures. PLoS One 2016; 11: e0156299
- 118 Banerjee R, Teng CB, Cunningham SA. et al. Randomized trial of rapid multiplex polymerase chain reaction-based blood culture identification and susceptibility testing. Clin Infect Dis 2015; 61 (07) 1071-1080
- 119 Hill JT, Tran KD, Barton KL, Labreche MJ, Sharp SE. Evaluation of the nanosphere Verigene BC-GN assay for direct identification of gram-negative bacilli and antibiotic resistance markers from positive blood cultures and potential impact for more-rapid antibiotic interventions. J Clin Microbiol 2014; 52 (10) 3805-3807
- 120 Altun O, Almuhayawi M, Ullberg M, Ozenci V. Clinical evaluation of the FilmArray blood culture identification panel in identification of bacteria and yeasts from positive blood culture bottles. J Clin Microbiol 2013; 51 (12) 4130-4136
- 121 Dodémont M, De Mendonça R, Nonhoff C, Roisin S, Denis O. Performance of the Verigene Gram-negative blood culture assay for rapid detection of bacteria and resistance determinants. J Clin Microbiol 2014; 52 (08) 3085-3087
- 122 Nguyen MH, Clancy CJ, Pasculle AW. et al. Performance of the T2Bacteria panel for diagnosing bloodstream infections: a diagnostic accuracy study. Ann Intern Med 2019; 170 (12) 845-852
- 123 Vincent JL, Brealey D, Libert N. et al; Rapid Diagnosis of Infections in the Critically Ill Team. Rapid diagnosis of infection in the critically ill, a multicenter study of molecular detection in bloodstream infections, pneumonia, and sterile site infections. Crit Care Med 2015; 43 (11) 2283-2291
- 124 Marschal M, Bachmaier J, Autenrieth I, Oberhettinger P, Willmann M, Peter S. Evaluation of the accelerate pheno system for fast identification and antimicrobial susceptibility testing from positive blood cultures in bloodstream infections caused by gram-negative pathogens. J Clin Microbiol 2017; 55 (07) 2116-2126
- 125 Meltzer AC, Newton S, Lange J. et al. A randomized control trial of a multiplex gastrointestinal PCR panel versus usual testing to assess antibiotics use for patients with infectious diarrhea in the emergency department. J Am Coll Emerg Physicians Open 2022; 3 (01) e12616
- 126 D'Onofrio V, Salimans L, Bedenić B, Cartuyvels R, Barišić I, Gyssens IC. The clinical impact of rapid molecular microbiological diagnostics for pathogen and resistance gene identification in patients with sepsis: a systematic review. Open Forum Infect Dis 2020; 7 (10) ofaa352
- 127 Oeschger T, McCloskey D, Kopparthy V, Singh A, Erickson D. Point of care technologies for sepsis diagnosis and treatment. Lab Chip 2019; 19 (05) 728-737
- 128 Ruiz-Rodriguez JC, Plata-Menchaca EP, Chiscano-Camón L. et al. Precision medicine in sepsis and septic shock: from omics to clinical tools. World J Crit Care Med 2022; 11 (01) 1-21
- 129 Bermejo-Martin JF, Andaluz-Ojeda D, Almansa R. et al. Defining immunological dysfunction in sepsis: a requisite tool for precision medicine. J Infect 2016; 72 (05) 525-536
- 130 Dey P, Fabri-Faja N, Calvo-Lozano O. et al. Label-free bacteria quantification in blood plasma by a bioprinted microarray based interferometric point-of-care device. ACS Sens 2019; 4 (01) 52-60
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
01. Juli 2024
© 2024. Thieme. All rights reserved.
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Rudd KE, Johnson SC, Agesa KM. et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet 2020; 395 (10219): 200-211
- 2 Rüddel H, Thomas-Rüddel DO, Reinhart K. et al; MEDUSA study group. Adverse effects of delayed antimicrobial treatment and surgical source control in adults with sepsis: results of a planned secondary analysis of a cluster-randomized controlled trial. Crit Care 2022; 26 (01) 51
- 3 Mensa J, Barberán J, Ferrer R. et al. Recommendations for antibiotic selection for severe nosocomial infections. Rev Esp Quimioter 2021; 34 (05) 511-524
- 4 Prescott HC, Angus DC. Enhancing recovery from sepsis: a review. JAMA 2018; 319 (01) 62-75
- 5 Seymour CW, Gesten F, Prescott HC. et al. Time to treatment and mortality during mandated emergency care for sepsis. N Engl J Med 2017; 376 (23) 2235-2244
- 6 Evans L, Rhodes A, Alhazzani W. et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med 2021; 47 (11) 1181-1247
- 7 Carlbom DJ, Rubenfeld GD. Barriers to implementing protocol-based sepsis resuscitation in the emergency department–results of a national survey. Crit Care Med 2007; 35 (11) 2525-2532
- 8 Simmonds M, Hutchinson A, Chikhani M. et al. Surviving sepsis beyond intensive care: a retrospective cohort study of compliance with the international guidelines. J Intensive Care Soc 2008; 9: 124-127
- 9 Ferrer R, González Del Castillo J, Martínez-Martínez M, Plata-Menchaca EP, Larrosa MN. Time to decision in sepsis. Rev Esp Quimioter 2023; 36 (01) 82-87
- 10 Singer M, Deutschman CS, Seymour CW. et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016; 315 (08) 801-810
- 11 Prescott HC, Cope TM, Gesten FC. et al. Reporting of sepsis cases for performance measurement versus for reimbursement in New York State. Crit Care Med 2018; 46 (05) 666-673
- 12 Kim SJ, Hwang SO, Kim YW, Lee JH, Cha KC. Procalcitonin as a diagnostic marker for sepsis/septic shock in the emergency department; a study based on Sepsis-3 definition. Am J Emerg Med 2019; 37 (02) 272-276
- 13 Suffoletto B, Frisch A, Prabhu A, Kristan J, Guyette FX, Callaway CW. Prediction of serious infection during prehospital emergency care. Prehosp Emerg Care 2011; 15 (03) 325-330
- 14 Kwizera A, Adhikari NKJ, Angus DC. et al. Recognition of sepsis in resource-limited settings. 2019 Feb 9. In: Dondorp AM, Dünser MW, Schultz MJ. eds. Sepsis Management in Resource-limited Settings [Internet]. Cham: Springer; 2019. . Chapter 4
- 15 Kaukonen KM, Bailey M, Pilcher D, Cooper DJ, Bellomo R. Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med 2015; 372 (17) 1629-1638
- 16 Machado FR, Cavalcanti AB, Monteiro MB. et al; Instituto Latino-Americano de Sepsis network investigators. Predictive accuracy of the quick sepsis-related organ failure assessment score in Brazil. a prospective multicenter study. Am J Respir Crit Care Med 2020; 201 (07) 789-798
- 17 Seymour CW, Liu VX, Iwashyna TJ. et al. Assessment of clinical criteria for sepsis: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016; 315 (08) 762-774
- 18 Briassoulis G, Briassoulis P, Miliaraki M. et al; Combined Approach for The eArly diagnosis of INfection in sepsis (CAPTAIN) study group. Biomarker cruises in sepsis: who is the CAPTAIN? Discussion on “Circulating biomarkers may be unable to detect infection at the early phase of sepsis in ICU patients: the CAPTAIN prospective multicenter cohort study”. Intensive Care Med 2019; 45 (01) 132-133
- 19 Klimpel J, Weidhase L, Bernhard M, Gries A, Petros S. The impact of the Sepsis-3 definition on ICU admission of patients with infection. Scand J Trauma Resusc Emerg Med 2019; 27 (01) 98
- 20 Peake SL, Delaney A, Bailey M. et al; ARISE Investigators, ANZICS Clinical Trials Group. Goal-directed resuscitation for patients with early septic shock. N Engl J Med 2014; 371 (16) 1496-1506
- 21 Herwanto V, Shetty A, Nalos M. et al. Accuracy of quick sequential organ failure assessment score to predict sepsis mortality in 121 studies including 1,716,017 individuals: a systematic review and meta-analysis. Crit Care Explor 2019; 1 (09) e0043
- 22 Serafim R, Gomes JA, Salluh J, Póvoa P. A comparison of the Quick-SOFA and systemic inflammatory response syndrome criteria for the diagnosis of sepsis and prediction of mortality: a systematic review and meta-analysis. Chest 2018; 153 (03) 646-655
- 23 Fernando SM, Tran A, Taljaard M. et al. Prognostic accuracy of the quick sequential organ failure assessment for mortality in patients with suspected infection: a systematic review and meta-analysis. Ann Intern Med 2018; 168 (04) 266-275
- 24 Liu VX, Lu Y, Carey KA. et al. Comparison of early warning scoring systems for hospitalized patients with and without infection at risk for in-hospital mortality and transfer to the intensive care unit. JAMA Netw Open 2020; 3 (05) e205191
- 25 Inada-Kim M. NEWS2 and improving outcomes from sepsis. Clin Med (Lond) 2022; 22 (06) 514-517
- 26 Alberto L, Marshall AP, Walker R, Aitken LM. Screening for sepsis in general hospitalized patients: a systematic review. J Hosp Infect 2017; 96 (04) 305-315
- 27 Bhattacharjee P, Edelson DP, Churpek MM. Identifying patients with sepsis on the hospital wards. Chest 2017; 151 (04) 898-907
- 28 Makam AN, Nguyen OK, Auerbach AD. Diagnostic accuracy and effectiveness of automated electronic sepsis alert systems: a systematic review. J Hosp Med 2015; 10 (06) 396-402
- 29 Downing NL, Rolnick J, Poole SF. et al. Electronic health record-based clinical decision support alert for severe sepsis: a randomised evaluation. BMJ Qual Saf 2019; 28 (09) 762-768
- 30 Hooper MH, Weavind L, Wheeler AP. et al. Randomized trial of automated, electronic monitoring to facilitate early detection of sepsis in the intensive care unit*. Crit Care Med 2012; 40 (07) 2096-2101
- 31 Shimabukuro DW, Barton CW, Feldman MD, Mataraso SJ, Das R. Effect of a machine learning-based severe sepsis prediction algorithm on patient survival and hospital length of stay: a randomised clinical trial. BMJ Open Respir Res 2017; 4 (01) e000234
- 32 Esteban E, Belda S, García-Soler P. et al. A multifaceted educational intervention shortened time to antibiotic administration in children with severe sepsis and septic shock: ABISS Edusepsis pediatric study. Intensive Care Med 2017; 43 (12) 1916-1918
- 33 Ferrer R, Artigas A, Levy MM. et al; Edusepsis Study Group. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA 2008; 299 (19) 2294-2303
- 34 Yébenes JC, Lorencio C, Esteban E. et al; Comisión Asesora para la Atención al Paciente con Sepsis y Grup de Treball de Sèpsia i Xoc Sèptic (GTSiXS) SOCMIC-SOCMUE. Interhospital Sepsis Code in Catalonia (Spain): territorial model for initial care of patients with sepsis. Med Intensiva (Engl Ed) 2020; 44 (01) 36-45
- 35 Damiani E, Donati A, Serafini G. et al. Effect of performance improvement programs on compliance with sepsis bundles and mortality: a systematic review and meta-analysis of observational studies. PLoS One 2015; 10 (05) e0125827
- 36 Ferrer R, Ruiz-Rodriguez JC, Larrosa N, Llaneras J, Molas E, González-López JJ. Sepsis code implementation at Vall d'Hebron University Hospital: rapid diagnostics key to success. ICU Management & Practice 2017; 17 (04) 214-215
- 37 Weiss SL, Peters MJ, Alhazzani W. et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Med 2020; 46 (Suppl. 01) 10-67
- 38 Chiscano-Camón L, Plata-Menchaca E, Ruiz-Rodríguez JC, Ferrer R. Fisiopatología del shock séptico. Med Intensiva (Engl Ed) 2022; 46 (Suppl. 01) 1-13
- 39 Wang C, Xu R, Zeng Y, Zhao Y, Hu X. A comparison of qSOFA, SIRS and NEWS in predicting the accuracy of mortality in patients with suspected sepsis: a meta-analysis. PLoS One 2022; 17 (04) e0266755
- 40 Ventura F, Pugin J, Tissieres P. ICU Management & Practice, 2021; 23. Accessed July 2, 2023 at: https://healthmanagement.org/c/icu/issuearticle/sepsis-diagnosis-clinical-signs-scores-and-biomarkers
- 41 Simon L, Gauvin F, Amre DK, Saint-Louis P, Lacroix J. Serum procalcitonin and C-reactive protein levels as markers of bacterial infection: a systematic review and meta-analysis. Clin Infect Dis 2004; 39 (02) 206-217
- 42 Kondo Y, Umemura Y, Hayashida K, Hara Y, Aihara M, Yamakawa K. Diagnostic value of procalcitonin and presepsin for sepsis in critically ill adult patients: a systematic review and meta-analysis. J Intensive Care 2019; 7: 22
- 43 Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis. Lancet Infect Dis 2013; 13 (05) 426-435
- 44 Plata-Menchaca EP, Ferrer R. Procalcitonin is useful for antibiotic deescalation in sepsis. Crit Care Med 2021; 49 (04) 693-696
- 45 Layios N, Lambermont B, Canivet JL. et al. Procalcitonin usefulness for the initiation of antibiotic treatment in intensive care unit patients. Crit Care Med 2012; 40 (08) 2304-2309
- 46 Schuetz P, Beishuizen A, Broyles M. et al. Procalcitonin (PCT)-guided antibiotic stewardship: an international experts consensus on optimized clinical use. Clin Chem Lab Med 2019; 57 (09) 1308-1318
- 47 Yu H, Nie L, Liu A. et al. Combining procalcitonin with the qSOFA and sepsis mortality prediction. Medicine (Baltimore) 2019; 98 (23) e15981
- 48 Kalil AC, Metersky ML, Klompas M. et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis 2016; 63 (05) e61-e111
- 49 Torres A, Niederman MS, Chastre J. et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J 2017; 50 (03) 50
- 50 Póvoa P, Coelho L, Dal-Pizzol F. et al. How to use biomarkers of infection or sepsis at the bedside: guide to clinicians. Intensive Care Med 2023; 49 (02) 142-153
- 51 Christ-Crain M, Opal SM. Clinical review: the role of biomarkers in the diagnosis and management of community-acquired pneumonia. Crit Care 2010; 14 (01) 203
- 52 Kamat IS, Ramachandran V, Eswaran H, Guffey D, Musher DM. Procalcitonin to distinguish viral from bacterial pneumonia: a systematic review and meta-analysis. Clin Infect Dis 2020; 70 (03) 538-542
- 53 Meier MA, Branche A, Neeser OL. et al. Procalcitonin-guided antibiotic treatment in patients with positive blood cultures: a patient-level meta-analysis of randomized trials. Clin Infect Dis 2019; 69 (03) 388-396
- 54 Kennis B, Ali A, Lasoff D, Sweeney DA, Wardi G. The diagnostic utility of procalcitonin is limited in the setting of methamphetamine toxicity. Am J Emerg Med 2022; 54: 36-40
- 55 Wirz Y, Meier MA, Bouadma L. et al. Effect of procalcitonin-guided antibiotic treatment on clinical outcomes in intensive care unit patients with infection and sepsis patients: a patient-level meta-analysis of randomized trials. Crit Care 2018; 22 (01) 191
- 56 Kyriazopoulou E, Liaskou-Antoniou L, Adamis G. et al. Procalcitonin to reduce long-term infection-associated adverse events in sepsis: a randomized trial. Am J Respir Crit Care Med 2021; 203 (02) 202-210
- 57 de Jong E, van Oers JA, Beishuizen A. et al. Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: a randomised, controlled, open-label trial. Lancet Infect Dis 2016; 16 (07) 819-827
- 58 Huang Q, Xiong H, Yan P. et al. The diagnostic and prognostic value of suPAR in patients with sepsis: a systematic review and meta-analysis. Shock 2020; 53 (04) 416-425
- 59 Bleharski JR, Kiessler V, Buonsanti C. et al. A role for triggering receptor expressed on myeloid cells-1 in host defense during the early-induced and adaptive phases of the immune response. J Immunol 2003; 170 (07) 3812-3818
- 60 Gómez-Piña V, Soares-Schanoski A, Rodríguez-Rojas A. et al. Metalloproteinases shed TREM-1 ectodomain from lipopolysaccharide-stimulated human monocytes. J Immunol 2007; 179 (06) 4065-4073
- 61 Aksaray S, Alagoz P, Inan A, Cevan S, Ozgultekin A. Diagnostic value of sTREM-1 and procalcitonin levels in the early diagnosis of sepsis. North Clin Istanb 2017; 3 (03) 175-182
- 62 Julián-Jiménez A, Yañez MC, González-Del Castillo J. et al; en representación del grupo INFURG-SEMES. Prognostic power of biomarkers for short-term mortality in the elderly patients seen in Emergency Departments due to infections. Enferm Infecc Microbiol Clin (Engl Ed) 2019; 37 (01) 11-18
- 63 Baldirà J, Ruiz-Rodríguez JC, Wilson DC. et al. Biomarkers and clinical scores to aid the identification of disease severity and intensive care requirement following activation of an in-hospital sepsis code. Ann Intensive Care 2020; 10 (01) 7
- 64 Baldirà J, Ruiz-Rodríguez JC, Ruiz-Sanmartin A. et al. Use of biomarkers to improve 28-day mortality stratification in patients with sepsis and SOFA ≤ 6. Biomedicines 2023; 11 (08) 11
- 65 Hotchkiss RS, Moldawer LL, Opal SM, Reinhart K, Turnbull IR, Vincent JL. Sepsis and septic shock. Nat Rev Dis Primers 2016; 2: 16045
- 66 Munoz C, Carlet J, Fitting C, Misset B, Blériot JP, Cavaillon JM. Dysregulation of in vitro cytokine production by monocytes during sepsis. J Clin Invest 1991; 88 (05) 1747-1754
- 67 Shapiro NI, Trzeciak S, Hollander JE. et al. A prospective, multicenter derivation of a biomarker panel to assess risk of organ dysfunction, shock, and death in emergency department patients with suspected sepsis. Crit Care Med 2009; 37 (01) 96-104
- 68 Dolin HH, Papadimos TJ, Stepkowski S, Chen X, Pan ZK. A novel combination of biomarkers to herald the onset of sepsis prior to the manifestation of symptoms. Shock 2018; 49 (04) 364-370
- 69 Parlato M, Philippart F, Rouquette A. et al; Captain Study Group. Circulating biomarkers may be unable to detect infection at the early phase of sepsis in ICU patients: the CAPTAIN prospective multicenter cohort study. Intensive Care Med 2018; 44 (07) 1061-1070
- 70 Teggert A, Datta H, Ali Z. Biomarkers for point-of-care diagnosis of sepsis. Micromachines (Basel) 2020; 11 (03) 11
- 71 Kim M, Song KH, Kim CJ. et al. Electronic alerts with automated consultations promote appropriate antimicrobial prescriptions. PLoS One 2016; 11 (08) e0160551
- 72 Adams R, Henry KE, Sridharan A. et al. Prospective, multi-site study of patient outcomes after implementation of the TREWS machine learning-based early warning system for sepsis. Nat Med 2022; 28 (07) 1455-1460
- 73 Pugin J, Daix T, Pagani JL. et al. Serial measurement of pancreatic stone protein for the early detection of sepsis in intensive care unit patients: a prospective multicentric study. Crit Care 2021; 25 (01) 151
- 74 David VL, Ercisli MF, Rogobete AF. et al. Early prediction of sepsis incidence in critically ill patients using specific genetic polymorphisms. Biochem Genet 2017; 55 (03) 193-203
- 75 D'Onofrio V, Heylen D, Pusparum M. et al. A prospective observational cohort study to identify inflammatory biomarkers for the diagnosis and prognosis of patients with sepsis. J Intensive Care 2022; 10 (01) 13
- 76 Liu W, Geng F, Yu L. Long non-coding RNA MALAT1/microRNA 125a axis presents excellent value in discriminating sepsis patients and exhibits positive association with general disease severity, organ injury, inflammation level, and mortality in sepsis patients. J Clin Lab Anal 2020; 34 (06) e23222
- 77 Assicot M, Gendrel D, Carsin H, Raymond J, Guilbaud J, Bohuon C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet 1993; 341 (8844) 515-518
- 78 Yin WP, Li JB, Zheng XF, An L, Shao H, Li CS. Effect of neutrophil CD64 for diagnosing sepsis in emergency department. World J Emerg Med 2020; 11 (02) 79-86
- 79 Brenner T, Uhle F, Fleming T. et al. Soluble TREM-1 as a diagnostic and prognostic biomarker in patients with septic shock: an observational clinical study. Biomarkers 2017; 22 (01) 63-69
- 80 Su L, Liu D, Chai W, Liu D, Long Y. Role of sTREM-1 in predicting mortality of infection: a systematic review and meta-analysis. BMJ Open 2016; 6 (05) e010314
- 81 Liu M, Zhang X, Chen H. et al. Serum sPD-L1, upregulated in sepsis, may reflect disease severity and clinical outcomes in septic patients. Scand J Immunol 2017; 85 (01) 66-72
- 82 Yende S, Kellum JA, Talisa VB. et al. Long-term host immune response trajectories among hospitalized patients with sepsis. JAMA Netw Open 2019; 2 (08) e198686
- 83 Hoppensteadt D, Tsuruta K, Hirman J, Kaul I, Osawa Y, Fareed J. Dysregulation of inflammatory and hemostatic markers in sepsis and suspected disseminated intravascular coagulation. Clin Appl Thromb Hemost 2015; 21 (02) 120-127
- 84 Matsumoto H, Ogura H, Shimizu K. et al. The clinical importance of a cytokine network in the acute phase of sepsis. Sci Rep 2018; 8 (01) 13995
- 85 Barre M, Behnes M, Hamed S. et al. Revisiting the prognostic value of monocyte chemotactic protein 1 and interleukin-6 in the sepsis-3 era. J Crit Care 2018; 43: 21-28
- 86 Uusitalo-Seppälä R, Huttunen R, Aittoniemi J. et al. Pentraxin 3 (PTX3) is associated with severe sepsis and fatal disease in emergency room patients with suspected infection: a prospective cohort study. PLoS One 2013; 8 (01) e53661
- 87 Hamed S, Behnes M, Pauly D. et al. Pentraxin-3 predicts short- and mid-term mortality in patients with sepsis and septic shock during intensive care treatment. Clin Lab 2018; 64 (06) 999-1011
- 88 Larsson A, Tydén J, Johansson J. et al. Calprotectin is superior to procalcitonin as a sepsis marker and predictor of 30-day mortality in intensive care patients. Scand J Clin Lab Invest 2020; 80 (02) 156-161
- 89 Lundberg OHM, Lengquist M, Spångfors M. et al. Circulating bioactive adrenomedullin as a marker of sepsis, septic shock and critical illness. Crit Care 2020; 24 (01) 636
- 90 Karampela I, Christodoulatos GS, Kandri E. et al. Circulating eNampt and resistin as a proinflammatory duet predicting independently mortality in critically ill patients with sepsis: a prospective observational study. Cytokine 2019; 119: 62-70
- 91 Saboktakin L, Bilan N, Ghalehgolab Behbahan A, Poorebrahim S. Relationship between resistin levels and sepsis among children under 12 years of age: a case control study. Front Pediatr 2019; 7: 355
- 92 Eugen-Olsen J, Giamarellos-Bourboulis EJ. suPAR: the unspecific marker for disease presence, severity and prognosis. Int J Antimicrob Agents 2015; 46 (Suppl. 01) S33-S34
- 93 Feng Q, Wei WQ, Chaugai S. et al. Association between low-density lipoprotein cholesterol levels and risk for sepsis among patients admitted to the hospital with infection. JAMA Netw Open 2019; 2 (01) e187223
- 94 Urbonas V, Eidukaitė A, Tamulienė I. The predictive value of soluble biomarkers (CD14 subtype, interleukin-2 receptor, human leucocyte antigen-G) and procalcitonin in the detection of bacteremia and sepsis in pediatric oncology patients with chemotherapy-induced febrile neutropenia. Cytokine 2013; 62 (01) 34-37
- 95 Arai Y, Mizugishi K, Nonomura K, Naitoh K, Takaori-Kondo A, Yamashita K. Phagocytosis by human monocytes is required for the secretion of presepsin. J Infect Chemother 2015; 21 (08) 564-569
- 96 Lu B, Zhang Y, Li C. et al. The utility of presepsin in diagnosis and risk stratification for the emergency patients with sepsis. Am J Emerg Med 2018; 36 (08) 1341-1345
- 97 Memar MY, Baghi HB. Presepsin: a promising biomarker for the detection of bacterial infections. Biomed Pharmacother 2019; 111: 649-656
- 98 Westhoff D, Engelen-Lee JY, Hoogland ICM. et al. Systemic infection and microglia activation: a prospective postmortem study in sepsis patients. Immun Ageing 2019; 16: 18
- 99 Lerman YV, Lim K, Hyun Y-M. et al. Sepsis lethality via exacerbated tissue infiltration and TLR-induced cytokine production by neutrophils is integrin α3β1-dependent. Blood 2014; 124 (24) 3515-3523
- 100 Sarangi PP, Hyun YM, Lerman YV, Pietropaoli AP, Kim M. Role of β1 integrin in tissue homing of neutrophils during sepsis. Shock 2012; 38 (03) 281-287
- 101 Mikacenic C, Hahn WO, Price BL. et al. Biomarkers of endothelial activation are associated with poor outcome in critical illness. PLoS One 2015; 10 (10) e0141251
- 102 Gui F, Peng H, Liu Y. Elevated circulating lnc-ANRIL/miR-125a axis level predicts higher risk, more severe disease condition, and worse prognosis of sepsis. J Clin Lab Anal 2019; 33 (06) e22917
- 103 Zhao D, Li S, Cui J, Wang L, Ma X, Li Y. Plasma miR-125a and miR-125b in sepsis: Correlation with disease risk, inflammation, severity, and prognosis. J Clin Lab Anal 2020; 34 (02) e23036
- 104 Na L, Ding H, Xing E. et al. Lnc-MEG3 acts as a potential biomarker for predicting increased disease risk, systemic inflammation, disease severity, and poor prognosis of sepsis via interacting with miR-21. J Clin Lab Anal 2020; 34 (04) e23123
- 105 Tuerxun K, Eklund D, Wallgren U. et al. Predicting sepsis using a combination of clinical information and molecular immune markers sampled in the ambulance. Sci Rep 2023; 13 (01) 14917
- 106 Leligdowicz A, Matthay MA. Heterogeneity in sepsis: new biological evidence with clinical applications. Crit Care 2019; 23 (01) 80
- 107 Klein Klouwenberg PM, Cremer OL, van Vught LA. et al. Likelihood of infection in patients with presumed sepsis at the time of intensive care unit admission: a cohort study. Crit Care 2015; 19 (01) 319
- 108 Luethy PM, Johnson JK. The use of matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) for the identification of pathogens causing sepsis. J Appl Lab Med 2019; 3 (04) 675-685
- 109 Timbrook TT, Morton JB, McConeghy KW, Caffrey AR, Mylonakis E, LaPlante KL. The effect of molecular rapid diagnostic testing on clinical outcomes in bloodstream infections: a systematic review and meta-analysis. Clin Infect Dis 2017; 64 (01) 15-23
- 110 Vlek AL, Bonten MJ, Boel CH. Direct matrix-assisted laser desorption ionization time-of-flight mass spectrometry improves appropriateness of antibiotic treatment of bacteremia. PLoS One 2012; 7 (03) e32589
- 111 Clec'h C, Ferriere F, Karoubi P. et al. Diagnostic and prognostic value of procalcitonin in patients with septic shock. Crit Care Med 2004; 32 (05) 1166-1169
- 112 Huang AM, Newton D, Kunapuli A. et al. Impact of rapid organism identification via matrix-assisted laser desorption/ionization time-of-flight combined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia. Clin Infect Dis 2013; 57 (09) 1237-1245
- 113 Bookstaver PB, Nimmich EB, Smith III TJ. et al. Cumulative effect of an antimicrobial stewardship and rapid diagnostic testing bundle on early streamlining of antimicrobial therapy in gram-negative bloodstream infections. Antimicrob Agents Chemother 2017; 61 (09) 61
- 114 Perez KK, Olsen RJ, Musick WL. et al. Integrating rapid pathogen identification and antimicrobial stewardship significantly decreases hospital costs. Arch Pathol Lab Med 2013; 137 (09) 1247-1254
- 115 Perez KK, Olsen RJ, Musick WL. et al. Integrating rapid diagnostics and antimicrobial stewardship improves outcomes in patients with antibiotic-resistant Gram-negative bacteremia. J Infect 2014; 69 (03) 216-225
- 116 Jung JS, Hamacher C, Gross B. et al. Evaluation of a semiquantitative matrix-assisted laser desorption ionization-time of flight mass spectrometry method for rapid antimicrobial susceptibility testing of positive blood cultures. J Clin Microbiol 2016; 54 (11) 2820-2824
- 117 Verroken A, Defourny L, le Polain de Waroux O. et al. Clinical Impact of MALDI-TOF MS Identification and Rapid Susceptibility Testing on Adequate Antimicrobial Treatment in Sepsis with Positive Blood Cultures. PLoS One 2016; 11: e0156299
- 118 Banerjee R, Teng CB, Cunningham SA. et al. Randomized trial of rapid multiplex polymerase chain reaction-based blood culture identification and susceptibility testing. Clin Infect Dis 2015; 61 (07) 1071-1080
- 119 Hill JT, Tran KD, Barton KL, Labreche MJ, Sharp SE. Evaluation of the nanosphere Verigene BC-GN assay for direct identification of gram-negative bacilli and antibiotic resistance markers from positive blood cultures and potential impact for more-rapid antibiotic interventions. J Clin Microbiol 2014; 52 (10) 3805-3807
- 120 Altun O, Almuhayawi M, Ullberg M, Ozenci V. Clinical evaluation of the FilmArray blood culture identification panel in identification of bacteria and yeasts from positive blood culture bottles. J Clin Microbiol 2013; 51 (12) 4130-4136
- 121 Dodémont M, De Mendonça R, Nonhoff C, Roisin S, Denis O. Performance of the Verigene Gram-negative blood culture assay for rapid detection of bacteria and resistance determinants. J Clin Microbiol 2014; 52 (08) 3085-3087
- 122 Nguyen MH, Clancy CJ, Pasculle AW. et al. Performance of the T2Bacteria panel for diagnosing bloodstream infections: a diagnostic accuracy study. Ann Intern Med 2019; 170 (12) 845-852
- 123 Vincent JL, Brealey D, Libert N. et al; Rapid Diagnosis of Infections in the Critically Ill Team. Rapid diagnosis of infection in the critically ill, a multicenter study of molecular detection in bloodstream infections, pneumonia, and sterile site infections. Crit Care Med 2015; 43 (11) 2283-2291
- 124 Marschal M, Bachmaier J, Autenrieth I, Oberhettinger P, Willmann M, Peter S. Evaluation of the accelerate pheno system for fast identification and antimicrobial susceptibility testing from positive blood cultures in bloodstream infections caused by gram-negative pathogens. J Clin Microbiol 2017; 55 (07) 2116-2126
- 125 Meltzer AC, Newton S, Lange J. et al. A randomized control trial of a multiplex gastrointestinal PCR panel versus usual testing to assess antibiotics use for patients with infectious diarrhea in the emergency department. J Am Coll Emerg Physicians Open 2022; 3 (01) e12616
- 126 D'Onofrio V, Salimans L, Bedenić B, Cartuyvels R, Barišić I, Gyssens IC. The clinical impact of rapid molecular microbiological diagnostics for pathogen and resistance gene identification in patients with sepsis: a systematic review. Open Forum Infect Dis 2020; 7 (10) ofaa352
- 127 Oeschger T, McCloskey D, Kopparthy V, Singh A, Erickson D. Point of care technologies for sepsis diagnosis and treatment. Lab Chip 2019; 19 (05) 728-737
- 128 Ruiz-Rodriguez JC, Plata-Menchaca EP, Chiscano-Camón L. et al. Precision medicine in sepsis and septic shock: from omics to clinical tools. World J Crit Care Med 2022; 11 (01) 1-21
- 129 Bermejo-Martin JF, Andaluz-Ojeda D, Almansa R. et al. Defining immunological dysfunction in sepsis: a requisite tool for precision medicine. J Infect 2016; 72 (05) 525-536
- 130 Dey P, Fabri-Faja N, Calvo-Lozano O. et al. Label-free bacteria quantification in blood plasma by a bioprinted microarray based interferometric point-of-care device. ACS Sens 2019; 4 (01) 52-60