

Subscribe to RSS
DOI: 10.1055/s-0044-1787531
“Unveiling Unique Pathologies in Obstructive Sleep Apnea: Two Intriguing Case Reports”
Authors
Funding Source This article has not received any funding.

Abstract
Obstructive sleep apnea (OSA) is often associated with reduced pharyngeal muscle tone and an anatomically narrowed pharyngeal airspace. We try to describe two cases with OSA that were diagnosed with vascular lesions during DISE: One of them was an aberrant internal carotid artery, and the second one was a glomus tumor. These anatomic anomalies contribute to airspace narrowing in these patients. These two cases describe an exciting presentation of sleep apnea and remind us of the importance of clinically recognizing vascular alterations to avoid damage during routine oropharyngeal procedures.
Keywords
drug-induced sleep endoscopy - obstructive sleep apnea - glomus tumor - aberrant internal carotid arteryIntroduction
OSA is a frequent disease associated with airway collapse. Many factors might produce the collapse of the airway, and they are usually centered in soft tissue, like fat deposition or muscle impairment. However, we must keep in mind that structures related to vascular lesions may also produce obstruction and have an essential role when surgery is indicated.
Currently, DISE (Drug-Induced sleep endoscopy) is a crucial tool to evaluate the site and type of airway collapse in patients suffering from OSA, especially in patients not tolerating the CPAP (Continuous positive airway pressure).
The importance of DISE is shown not only for the regular recognition of the area of obstruction but also for diagnosing vascular changes that predispose to airway collapse and might have a significant role in treatment.
We present two unique cases in which DISE impacted the patient́s OSA treatment decision. Vascular head and neck alterations are infrequently encountered.
The internal carotid artery (ICA) usually follows a straight path from the bifurcation of the common carotid artery to the skull base.[1] An aberrant ICA is susceptible to devastating injury during routine ENT procedures such as tonsillectomy and drainage of peritonsillar abscess.[2]
Glomus tumors are rare neoplasms derived from the paraganglion cells of the autonomic nervous system.[3] They occur in various locations throughout the body, and their presence in the upper airway, particularly in the context of OSA, is an uncommon finding.
Both cases had classic symptoms of OSA,[4] and were diagnosed during DISE. Understanding the clinical significance of detecting vascular tumors during DISE is crucial,[5] as it may impact patient management and treatment decisions. Informed consent and Ethical committee approval were obtained (Cómite de ética CUN 2022–206).
Case Reports
Case 1
A 42-year-old female presented with a history of chronic snoring, excessive daytime sleepiness, and fatigue. The patient had previously undergone septoplasty and limited endoscopic sinus surgery for sinus-related symptoms. A comprehensive assessment was conducted to evaluate suspected sleep-disordered breathing,[6] including a physical examination, risk factor assessment, and overnight polysomnography (PSG). The patient had a body mass index (BMI) of 28 Kg/m2, a neck circumference of 40 cm, and a waist circumference of 110 cm. Physical examination did not reveal any other significant findings. The appearance of the patient's oropharynx was unremarkable under direct visual inspection. Her Mallampati score was 4, her thyromental distance was 4 cm, and her tonsils were extended beyond the palatopharyngeal arch. The initial PSG results showed an apnea-hypopnea index (AHI) of 20 events per hour (e/h). The lowest oxygen saturation was 89%. Based on these findings, the patient was prescribed continuous positive airway pressure (CPAP) therapy.
Despite the progress with CPAP therapy, she continued to experience residual symptoms of daytime sleepiness and fatigue. Further evaluation and management options were discussed, including the possibility of mask adjustment, CPAP pressure titration, or alternative treatment modalities such as oral appliance therapy or surgical interventions. DISE was performed and showed a lateral collapse grade 2 at the oropharynx related to tonsils and palatopharyngeal muscles and a large, pulsatile mass in the posterior nasopharynx left side ([Fig. 1]).

Computed tomographic angiography (CTA) identified an aberrant ICA with a medial deviation to a retropharyngeal position ([Fig. 1]).
CPAP therapy was the initial treatment approach[7]; however, had poor benefits. Considering the CTA, a tonsillectomy was performed without any complications. Three months later, a PSG showed improved symptoms and normal AHI 4,1 e/h. ([Table 1])
Abbreviations: AHÍ, Apnea-Hypopnea Index; ODI, Oxygen desaturation index 3%.
Case 2
A 27-year-old male, a well-known professional singer, complained of poor night rest, apneas, frequent awakenings, and nasal obstruction. The patient had no history of smoking and no notable personal medical history. A sleep study result revealed an apnea-hypopnea index (AHI) of 89.8 e/h, The minimum recorded oxygen saturation during the study was 53%.
Considering the severity of the apnea, empirical CPAP therapy was indicated as the initial treatment approach. However, the patient was unable to tolerate CPAP therapy.
A DISE procedure was performed. The DISE findings revealed a lateral pulsating collapse in the oropharynx, indicating a potential structural abnormality contributing to sleep apnea symptoms ([Fig. 2]).

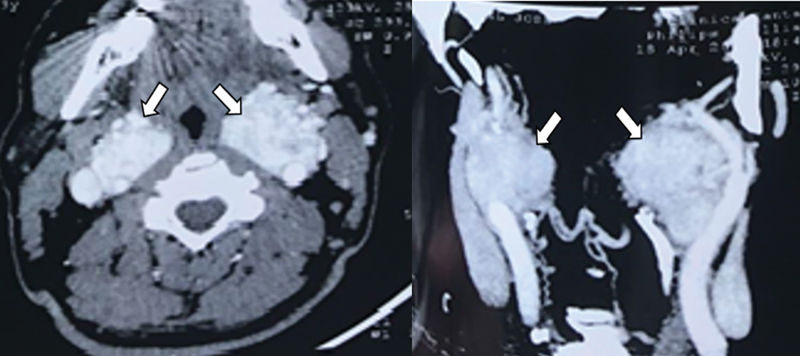
Considering the DISE findings, the patient underwent angiography and contrast-enhanced computed tomography (CT) scans to evaluate the upper airway in more detail. These imaging studies revealed the presence of lateral structures, which caused a symmetrical wall collapse in the oropharynx. ([Fig. 3]).
Given the diagnosis of a glomus tumor and its significant impact on the upper airway, further management options were discussed.[8] The patient was referred to a multidisciplinary team consisting of an otolaryngologist, vascular surgeon, and sleep specialist. Treatment options, such as surgical excision of the glomus tumor, embolization, or radiation therapy, were considered based on the tumor's size, location, and characteristics.
Embolization of the tumor was performed and treated by a vascular surgeon. Once it was resolved, the symptoms of OSA disappeared, confirming that this anatomical issue was the reason for his disease ([Table 1]). DISE, angiography, and contrast-enhanced CT played a crucial role in identifying the underlying cause of sleep apnea, leading to the discovery of a glomus tumor.
Discussion
The presence of vascular alterations that may partially obstruct the airway or compromise treatment must be kept in mind in patients with OSA. These lesions may produce a partial or complete airway obstruction, contributing to the presence of OSA.
DISE contributed uniquely to the diagnosis, probably related to the observational time spent watching the areas of collapse compared with in-office evaluation. Also, the effect of being in decubitus supine and the absence of swallowing allowed a favorable view of the pulsation of the vascular elements.
Aberrant arteries, including variations during the cervical ICA, are not uncommon and have been reported in a significant percentage of the general population. These arterial abnormalities are typically asymptomatic but can be detected through palpation and visual inspection during preoperative evaluations. Thus, a complementary radiology test should be performed. They have been described as a possible cause of airway narrowing in cases of obstructive sleep apnea and should be considered to avoid its damage in case of surgery.[9]
The exact etiology of ICA aberrations is not fully understood but is likely a combination of embryologic maldevelopments and acquired diseases, such as atherosclerosis or fibromuscular dysplasia.[10]
While the association between glomus tumors and OSA is not well-established, the presence of this tumor in the upper airway may contribute to airway narrowing and exacerbation of OSA symptoms.[11]
Glomus tumors are typically slow-growing and can remain asymptomatic for an extended period. the symptoms of poor night rest, apneas, frequent awakenings, and almost complete nasal obstruction prompted further investigation. The association between OSA and arterial aberrations is intriguing. Glomus tumors are rare, and their association with OSA is not well-documented in the literature.[12] Further research is needed to understand the underlying mechanisms better and establish a more precise correlation between glomus tumors and OSA.[13] Some studies show that these tumors do produce more symptoms of OSA, especially when they are bilateral and related to airway obstruction.
Long-term studies evaluating the outcomes of surgical intervention and the impact on OSA symptomatology in patients with glomus tumors would provide valuable insights into managing these cases.
The treatment approach for glomus tumors in the upper airway often involves surgical intervention.[14] The primary goal of surgery is the complete resection of the tumor, which can alleviate airway obstruction and improve OSA symptoms.
The specific surgical technique may vary depending on the location extent of the tumor, and expertise of the surgical team. Close postoperative follow-up is necessary to assess the resolution of OSA symptoms and the overall efficacy of the treatment.
Surgical correction of vascular anomalies, including aberrant arteries, carries high morbidity and is usually reserved for patients with neurologic symptoms or an increased risk of stroke. It is crucial for treating physicians to be aware of this condition to avoid accidental injury during surgical procedures and monitor for potential neurologic sequelae.
Finally, DISE is essential in viewing the collapsibility of the airway and allows us to have a better image of other possible vascular alterations that will impact the patient́s treatment.
Conclusion
An aberrant internal carotid artery may have contributed to airspace narrowing, exacerbating the symptoms of OSA. This case highlights the interesting association between OSA and arterial aberrations and emphasizes the importance of recognizing and documenting ICA aberrations to guide surgical procedures and monitor for potential complications. On the other hand, identifying a glomus tumor during the evaluation of OSA highlights the need for a comprehensive assessment of the upper airway in patients with significant symptoms. The surgical removal of the glomus tumor offers a potential solution to alleviate upper airway obstruction and improve OSA symptoms. However, further research is warranted to elucidate the relationship between glomus tumors and OSA and optimize treatment strategies for these unique cases.
Conflict of Interest
The authors declare no conflict of interest related to this article or cases.
-
References
- 1 Ozgur Z, Celik S, Govsa F, Aktug H, Ozgur T. A study of the course of the internal carotid artery in the parapharyngeal space and its clinical importance. Eur Arch Otorhinolaryngol 2007; 264 (12) 1483-1489
- 2 Wasserman JM, Sclafani SJ, Goldstein NA. Intraoperative evaluation of a pulsatile oropharyngeal mass during adenotonsillectomy. Int J Pediatr Otorhinolaryngol 2006; 70 (02) 371-375
- 3 Jackson CG, Glasscock ME, Harris PF. et al. Glomus jugulare tumors. J Neurosurg 1982; 57 (06) 700-704
- 4 Yucel A, Unlu M, Haktanir A, Acar M, Fidan F. Evaluation of the upper airway cross-sectional area changes in different degrees of severity of obstructive sleep apnea syndrome: cephalometric and dynamic CT study. AJNR Am J Neuroradiol 2005; 26 (10) 2624-2629
- 5 Lee JH, Baek BJ, Kim KW. et al. Glomus tumor in the parapharyngeal space. Eur Arch Otorhinolaryngol 2004; 261 (08) 441-444
- 6 Patil SP, Schneider H, Schwartz AR, Smith PL. Adult obstructive sleep apnea: pathophysiology and diagnosis. Chest 2007; 132 (01) 325-337
- 7 Paulsen F, Tillmann B, Christofides C, Richter W, Koebke J. Curving and looping of the internal carotid artery in relation to the pharynx: frequency, embryology and clinical implications. J Anat 2000; 197 (Pt 3): 373-381
- 8 Lim HJ, Sharma S, Sheahan P. Head and neck paragangliomas: An overview. J Clin Neurosci 2010; 17 (05) 595-600
- 9 Picel AC, Davidson TM. An aberrant internal carotid artery discovered during evaluation of obstructive sleep apnea: a report of 2 cases with consideration of a possible association. Ear Nose Throat J 2011; 90 (01) 29-31
- 10 Duygulu G. Relationship of aberrant internal carotid artery with pharyngeal wall in obstructive sleep apnea. Sleep Breath 2023; 27 (06) 2415-2422
- 11 Marks SC, Rimmer J, Anand VK. et al. Paragangliomas of the head and neck: Treatment outcomes and novel approaches for the difficult-to-treat tumors. Skull Base Surg 2009; 19 (02) 129-137
- 12 Havekes B, Kastelein F, van der Klaauw AA. et al. Head-and-neck paragangliomas are associated with sleep-related complaints, especially in the presence of carotid body tumors. Sleep Breath 2012; 16 (02) 527-534
- 13 van Hulsteijn LT, van Duinen N, Ninaber MK. et al. Carotid body tumors are not associated with an increased risk for sleep-disordered breathing. Sleep Breath 2014; 18 (01) 103-109
- 14 Vrabec DP, Dedo HH, Cole JW, Ogura JH. Glomus jugulare tumors: Diagnosis, treatment, and results. Ann Otol Rhinol Laryngol 1981; 90 (3 Pt 1): 197-201
Address for correspondence
Publication History
Received: 20 August 2023
Accepted: 07 February 2024
Article published online:
05 June 2024
© 2024. Brazilian Sleep Academy. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Ozgur Z, Celik S, Govsa F, Aktug H, Ozgur T. A study of the course of the internal carotid artery in the parapharyngeal space and its clinical importance. Eur Arch Otorhinolaryngol 2007; 264 (12) 1483-1489
- 2 Wasserman JM, Sclafani SJ, Goldstein NA. Intraoperative evaluation of a pulsatile oropharyngeal mass during adenotonsillectomy. Int J Pediatr Otorhinolaryngol 2006; 70 (02) 371-375
- 3 Jackson CG, Glasscock ME, Harris PF. et al. Glomus jugulare tumors. J Neurosurg 1982; 57 (06) 700-704
- 4 Yucel A, Unlu M, Haktanir A, Acar M, Fidan F. Evaluation of the upper airway cross-sectional area changes in different degrees of severity of obstructive sleep apnea syndrome: cephalometric and dynamic CT study. AJNR Am J Neuroradiol 2005; 26 (10) 2624-2629
- 5 Lee JH, Baek BJ, Kim KW. et al. Glomus tumor in the parapharyngeal space. Eur Arch Otorhinolaryngol 2004; 261 (08) 441-444
- 6 Patil SP, Schneider H, Schwartz AR, Smith PL. Adult obstructive sleep apnea: pathophysiology and diagnosis. Chest 2007; 132 (01) 325-337
- 7 Paulsen F, Tillmann B, Christofides C, Richter W, Koebke J. Curving and looping of the internal carotid artery in relation to the pharynx: frequency, embryology and clinical implications. J Anat 2000; 197 (Pt 3): 373-381
- 8 Lim HJ, Sharma S, Sheahan P. Head and neck paragangliomas: An overview. J Clin Neurosci 2010; 17 (05) 595-600
- 9 Picel AC, Davidson TM. An aberrant internal carotid artery discovered during evaluation of obstructive sleep apnea: a report of 2 cases with consideration of a possible association. Ear Nose Throat J 2011; 90 (01) 29-31
- 10 Duygulu G. Relationship of aberrant internal carotid artery with pharyngeal wall in obstructive sleep apnea. Sleep Breath 2023; 27 (06) 2415-2422
- 11 Marks SC, Rimmer J, Anand VK. et al. Paragangliomas of the head and neck: Treatment outcomes and novel approaches for the difficult-to-treat tumors. Skull Base Surg 2009; 19 (02) 129-137
- 12 Havekes B, Kastelein F, van der Klaauw AA. et al. Head-and-neck paragangliomas are associated with sleep-related complaints, especially in the presence of carotid body tumors. Sleep Breath 2012; 16 (02) 527-534
- 13 van Hulsteijn LT, van Duinen N, Ninaber MK. et al. Carotid body tumors are not associated with an increased risk for sleep-disordered breathing. Sleep Breath 2014; 18 (01) 103-109
- 14 Vrabec DP, Dedo HH, Cole JW, Ogura JH. Glomus jugulare tumors: Diagnosis, treatment, and results. Ann Otol Rhinol Laryngol 1981; 90 (3 Pt 1): 197-201