

Subscribe to RSS
DOI: 10.1055/s-0044-1791943
Hand Rejuvenation by Autologous Fat Grafting in Post-Hansen's Hand Atrophy: Aesthetic and Psychological Implications
Authors
Funding None.


Abstract
Introduction Contemporary medical science has been using fat grafting in aesthetic and reconstructive procedures, consistently achieving successful outcomes. Hansen's disease, caused by Mycobacterium leprae, leads to hand deformities due to peripheral neuropathy, resulting in soft-tissue atrophy, volume loss, and compromised hand function. Tendon transfer surgery is a common remedy for functionality, but it often does not address aesthetic concerns and the patient's psychological impact of living with an atrophic hand. Autologous fat grafting can effectively address these concerns.
Materials and Methods This prospective study evaluates the efficacy of fat grafting for hand rejuvenation in patients with Hansen's disease posttendon transfer surgery, focusing on aesthetic and psychological outcomes. We recorded data from 12 patients who underwent the procedure between 2015 and 2024. Using the Coleman technique, fat was harvested from the paraumbilical region of the abdomen and injected into various hand regions.
Results Autologous fat grafting showed high patient satisfaction with significant improvements in hand contour, skin texture, and psychological health. The benefits of the procedure included improved self-esteem, enhanced quality of life, reduced social stigma, and psychological well-being.
Conclusion Autologous fat grafting is a safe and effective technique for hand rejuvenation in patients with Hansen's disease, after functional treatment addressing both physical deformities and their psychological impacts. It could be considered one of the components in the comprehensive management of Hansen's disease–related hand deformities, significantly enhancing patients' overall quality of life.
Introduction
Since the dawn of human civilization, the visual appeal of the hands has commanded significant attention and fascination, representing the elevated status of mankind and serving as a direct expression of human ingenuity. Within the sphere of artistic expression, the intricate movements of the hands have been acknowledged as a tangible and expressive form of communication, which, despite displaying discernible variances, has been standardized over successive centuries. In the realm of contemporary medical science, autologous fat grafting has remained a long-standing practice in both aesthetic and reconstructive surgery, consistently delivering favorable outcomes.[1] [2]
The history of using fat grafting to correct concavities goes back over a century.[3] In 1988, the technique of autologous fat grafting for hand rejuvenation was first recorded, which involved depositing a fat bolus in the proximal dorsum of the hand and then massaging to achieve the desired contour.[4] This was followed by innovative strategies such as combining lipofilling with laser resurfacing in 1989 and introducing hand rejuvenation with microlipoinjection for age-related cosmetic improvement in 1990.[5] The first published patient series, reporting excellent patient satisfaction (98.6%), was released in 1992.[6] In 2002, Coleman published a significant study detailing a method for structural fat grafting, which involved making multiple passes with depositions of small quantities to produce more consistent results compared to injecting a lump of fat and manipulating it throughout the hand.[7]
Hansen's disease, attributed to Mycobacterium leprae, is a chronic infectious condition primarily affecting the skin and peripheral nerves. Among the significant complications of Hansen's disease are the resultant hand deformities stemming from peripheral neuropathy, leading to soft-tissue atrophy, loss of volume, contractures, and altered sensation.[8] These deformities not only adversely affect aesthetics but also impede hand function and diminish the patient's overall quality of life.
Tendon transfer surgery is a commonly employed procedure aimed at restoring hand function in individuals affected by Hansen's disease.[9] Despite the successful restoration of function, hand aesthetics may be compromised, leading to psychological distress.[10]
Fat grafting has emerged as a technique for aesthetic enhancement, improving tissue quality, and delivering long-term results like reduction of ulceration risk, softening of contracted areas and reduced fibrosis.[11] Fat grafting entails the extraction of fat from one part of the body, its processing, and subsequent injection into the target area. The adipose tissue serves as a filler, reinstating volume and improving tissue quality.
The purpose of this study was to evaluate the aesthetic and psychological benefits of fat grafting in patients with Hansen's disease with hand atrophy who have undergone tendon transfer surgery by analyzing both clinical outcomes and patient-reported experiences.
Objective
This prospective study aims to evaluate the efficacy of fat grafting for hand rejuvenation in posttendon transfer Hansen's disease patients and its aesthetic and psychological implications on them.
Materials and Methods
We conducted a prospective analysis of 12 patients with Hansen's disease who underwent fat grafting for hand rejuvenation between 2015 and 2024. All the data were collected on patient demographics, disease characteristics, patient's past and surgical history, surgical technique implemented, complications, and outcomes. Subjective analysis for psychological assessment was done using Center for Epidemiologic Studies Depression (CES-D)[12] scale for assessing depression and Generalized Anxiety Disorder 7 (GAD-7)[13] scale for assessing anxiety.
The CES-D scale is a self-reported depression scale designed to measure depressive symptoms in the general population. The CES-D scale consists of 20 items, each rated on a 4-point scale, with the following response options: 0—rarely or none of the time (<1 day); 1—some or a little of the time (1–2 days); 2—occasionally or a moderate amount of time (3–4 days); and 3—most or all of the time (5–7 days).
GAD-7 is a self-reported questionnaire designed to identify whether a person may have generalized anxiety disorder and to assess the severity of their anxiety symptoms. The GAD-7 consists of seven questions, with each question scored from 0 to 3. The total score ranges from 0 to 21, with higher scores indicating more severe anxiety symptoms.
It is unusual for patients with Hansen's disease to show up for cosmetic corrections, but whatever cases we had done were referred to us by a physical therapist who works at a leprosy rehabilitation center and helps with the posttendon transfer exercises to cure patients with Hansen's disease predominantly. Out of all cases the physical therapist encountered, only a few young people who had cosmetic concerns were educated and were referred to us.
Inclusion Criteria
-
All patients tested negative for M. leprae infection.
-
All patients who completed their course of treatment, including medical management, tendon transfers, physical therapy, and rehabilitation, achieving acceptable hand function.
-
All patients who exhibited post-Hansen's disease atrophy of the hands.
Surgical technique: Both general anesthesia and local anesthesia were utilized, depending on the case.
Donor site: The paraumbilical site in the abdomen was used as the donor site in all cases.
Procedure
-
Syringe liposuction was performed using a 2.5-mm cannula and a 20-mL Luer lock syringe.
-
The harvested fat was centrifuged ([Fig. 1A]) and filtered ([Fig. 1B]) to produce microfat.
-
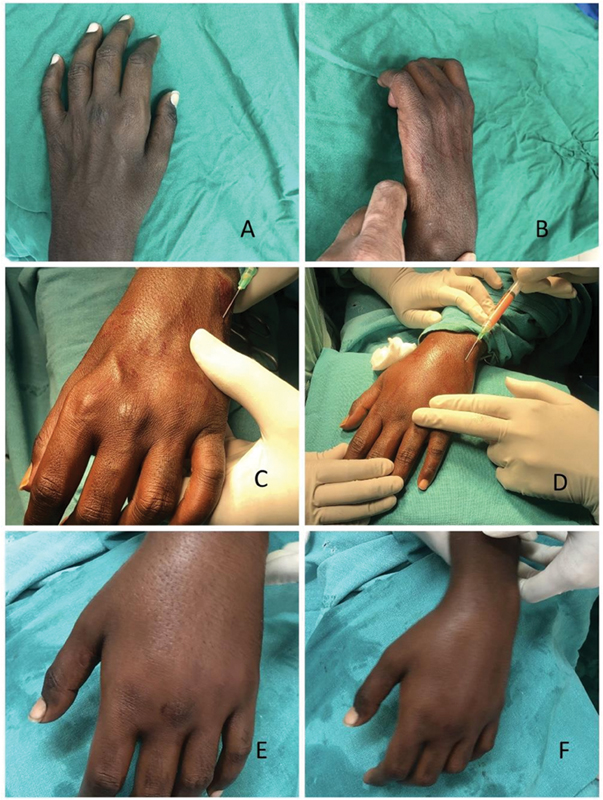
Fat was injected using a 1-mL BD Luer lock syringe with a 26-gauge cannula into the dorsum of the hand, uniformly in subcutaneous plane, paratenon atrophic gutters, the first web space, digital skin (subcutaneously), interphalangeal (IP) joints, and thenar area ([Fig. 2]; [Video 1]).
-
An average volume of 50 to 60 mL of fat was injected into each hand, with a slight overcorrection.


Video 1 Video demonstrating the procedure of autologous fat grafting in Post-Hansen–s hand atrophy.
Postoperative Care
-
A cotton crepe bandage dressing was applied immediately after the procedure.
-
Hand elevation was maintained for 1 week.
Assessment: Evaluations were conducted at 1 week, 4 weeks, and 3 months postoperatively. Subjective assessments of the results were performed, accompanied by photographic comparisons to document outcomes. Psychological improvement was observed through subjective history.
Results
Out of the 12 patients included in the study, 10 were males and 2 were females, with a mean age of 25 years. All the patients were unmarried before the surgery. They completed basic education. The average volume of fat injected into each patient was 50 to 60 mL. Approximately 10 to 15 mL overcorrection was done in all the patients in view of expected atrophy. Only one patient turned up for repeat fat grafting.
Fat grafting was performed using the Coleman technique, which involves careful harvesting, processing, and reinjection of fat to ensure maximal survival and integration of the graft. The mean volume of fat injected was 50 to 60 mL per hand.
Patient satisfaction was high, and all the patients noticed a significant improvement in hand contour and skin texture improvements postoperatively ([Figs. 3] [4] [5]).


All the patients were assessed for complications resulting from the fat grafting procedure.
In one case, infection was noticed at 72 hours postoperatively. Multiple small abscesses were observed, for which incision and drainage were done. On culture sensitivity testing, atypical Mycobacterium was reported, with sensitivity to clarithromycin. Dressings were done twice weekly. Injectable antibiotics were given for 2 weeks and oral antibiotics for another 2 weeks.
No other major complications were reported in other cases. Minor issues like swelling and bruising were noted but resolved within a few weeks. All patients reported improved hand aesthetics on long-term follow-up ([Figs. 6] and [7]).


Repeat procedure was done in only one case after 3 months on the patient's request.
The positive outcomes support the use of fat grafting for hand rejuvenation in patients with Hansen's disease.
Psychological evaluation is done using the CES-D scale for assessing depression and GAD-7 for assessing anxiety levels preoperatively and after 3 months of follow-up.
Our study demonstrated that fat grafting in hand rejuvenation posttendon transfer significantly impacts patients, reducing depression levels as indicated by the CES-D scores. The mean CES-D scores decreased from 20.08 (moderate depressive symptoms) to 9.83 (minimal depressive symptoms) postintervention, highlighting the potential benefits of this procedure for improving psychological well-being.
The GAD-7 scores indicate a significant reduction in anxiety levels postintervention, with mean scores decreasing from 14.58 (moderate anxiety) to 6.67 (mild anxiety). This suggests that fat grafting in hand rejuvenation posttendon transfer has a positive psychological impact, reducing anxiety levels in patients significantly.
Discussion
When we conducted a specific search regarding the aesthetic hand rejuvenation in cases of Hansen's disease, we found no publication to our surprise. This stimulated us to add to the existing literature on indications of autologous fat grafting in Hansens's atrophic hand.
We considered autologous fat grafting as a safe and effective technique for hand rejuvenation in patients with Hansen's disease. It addresses volume loss, improves tissue quality, and enhances hand aesthetics. The procedure involved harvesting fat from areas of excess, such as the abdomen or thighs, and injecting it into the dorsum and the palm of the hand. The fat is carefully injected in small amounts to ensure an even distribution and natural-looking results.
Our study incorporated microfat for the procedure. Microfat, compared with nanofat, does contain whole and viable adipocytes with their surrounding cell milieu. When injected, these adipocytes act like traditional fat grafts incorporating into the sites of injection.[14]
Fat grafting for hand rejuvenation is a procedure developed to address the signs of aging in the hands. The appearance of our hands changes significantly as we age. The five aesthetic characteristics of youthful hands (smooth skin, firmness and elasticity, even skin tone, fullness and volume, and hydrated appearance) change as a result of both intrinsic factors (such as changes in the epidermis and dermis) and extrinsic factors.[15]
Various studies in the literature show the autologous fat grafting procedure provided numerous advantages by effectively restoring lost subcutaneous fat in the hand, concealing visible veins and tendons, and reducing skin flaccidity. The literature also shows that fat grafting can lead to hand rejuvenation by promoting dermal regeneration through the presence of a higher percentage of beneficial fat cells in the subcutaneous region.[12] [16] [17]
There are studies in which autologous fat grafting has been employed for not only aesthetic hand rejuvenation but also the treatment of patients with Raynaud's phenomenon and Dupuytren's disease, utilizing similar techniques.[18] [19]
Our study recorded no allergic adverse reactions. A study conducted by Fantozzi[20] also recorded no allergic reactions because the patient's own fat cells were used. There were reported adverse reactions when using synthetic fillers for hand rejuvenation.[21] However, fat cells represent a biologic filler that a plastic surgeon can safely use for tissue filling.[1] [2]
Fat grafting to the hand of a patient with Hansen's disease is an effective treatment that addresses issues similar to age-related volume loss with subsequent prominence of vasculature and tendons.[22] All patients exhibit volumetric augmentation, with fat retention rates on par with those observed in fat grafting procedures conducted in other anatomical sites. Subjective evaluations align with the objective metrics of transformation.[16] [23] The refinement of methods has substantiated Fournier's assertion regarding the enduring nature of outcomes beyond 4 to 5 years.[4]
In our study, the long-term results after the procedure proved satisfactory. The long-term results of fat grafting in Hansen's disease patients are promising, with minimal complications reported. The literature shows that fat grafting is a valuable procedure that provides long-term results. In some isolated cases, the procedure may need to be repeated.[20]
We observed that edema is the most commonly encountered complication following autologous fat grafting to the hand in our study, but it typically resolves independently, as observed in many other studies.[17] [19] [20] [24] Applying compression dressings and advising the patient to elevate their hand for a few days can help manage the swelling immediately after surgery.[7] [25] Other complications that we did not encounter in our study that may resolve on their own include ecchymoses and paresthesias, as described in other studies, likely due to damage to small blood vessels and nerves.[17] [20]
Our study had one case with postoperative infection, which was treated with antibiotics. Studies have noted that infection is a potential complication following hand autologous fat grafting.[26] [27] This issue is the primary complication that requires prevention in this procedure. To avoid infection, it is crucial to maintain sterility throughout the process. Using sterile or disposable cannulas for both fat extraction and injection is essential. Additionally, prescribing antibiotics for 1 week as a preventive measure is always recommended.[18]
Our study found that physical deformities caused by Hansen's disease can have a significant psychological impact on patients, affecting their self-esteem and quality of life. Hand rejuvenation with fat grafting not only addresses aesthetic concerns but also provides psychological benefits, improving patients' self-image and confidence.
In our study, there was a significant improvement in the psychological status of the patients, assessed by the CES-D and GAD 7 scores.
This improvement helped the patients in having multiple psychological benefits.
The utilization of fat grafting has been instrumental in enhancing patients' self-esteem, thereby fostering a greater sense of confidence and ease in social interactions. This is achieved through the restoration of a more natural appearance to the hands, consequently mitigating feelings of self-consciousness and embarrassment.
Furthermore, fat grafting has proven to significantly improve both the function and aesthetic appearance of the hands, thereby contributing to an enhanced quality of life for patients by facilitating their ability to engage in daily activities.
Moreover, the application of fat grafting in hand rejuvenation has effectively mitigated social stigma and discrimination associated with Hansen's disease. By improving the aesthetic appearance of the hands, fat grafting has enabled patients to integrate more seamlessly into society.
Additionally, the psychological benefits of fat grafting cannot be understated, as evidenced by the reduction in anxiety and depression levels experienced by patients, along with an enhanced sense of body image satisfaction. This underscores the pivotal role of fat grafting in aiding physical recovery and contributing to psychological rehabilitation.
Although this procedure had been used in patients with Hansen's disease in our study, ours is primarily an aesthetic surgery unit. Therefore, we could only treat the cases that were referred to us. We did not come across any posttraumatic nerve palsy with small muscle atrophy patients with aesthetic concerns. It is also true that fat grafting in hand rejuvenation can be safely practiced in these cases as well.
Conclusion
Fat grafting can be a valuable tool for hand rejuvenation in patients with Hansen's disease. It provides a safe and effective means of restoring hand aesthetics, providing hand filling and improving the patient's quality of life after tendon transfer surgery. Given the significant aesthetic and psychological benefits, fat grafting should be considered one of the key components in managing Hansen's disease–related hand deformities.
Conflict of Interest
None declared.
-
References
- 1 Billings Jr E, May Jr JW. Historical review and present status of free fat graft autotransplantation in plastic and reconstructive surgery. Plast Reconstr Surg 1989; 83 (02) 368-381
- 2 Coleman SR. Facial recontouring with lipostructure. Clin Plast Surg 1997; 24 (02) 347-367
- 3 Neuber F. Fettransplantation. Bericht über die Verhandlungen der deutschen Gesellscaft für Chirurgie. Zentralbl Chir 1893; 22: 66
- 4 Fournier PF. Who should do syringe liposculpturing?. J Dermatol Surg Oncol 1988; 14 (10) 1055-1056
- 5 Abergel RP, David LM. Aging hands: a technique of hand rejuvenation by laser resurfacing and autologous fat transfer. J Dermatol Surg Oncol 1989; 15 (07) 725-728
- 6 Aboudib Júnior JH, de Castro CC, Gradel J. Hand rejuvenescence by fat filling. Ann Plast Surg 1992; 28 (06) 559-564
- 7 Coleman SR. Hand rejuvenation with structural fat grafting. Plast Reconstr Surg 2002; 110 (07) 1731-1744 , discussion 1745–1747
- 8 Lastória JC, Abreu MA. Leprosy: review of the epidemiological, clinical, and etiopathogenic aspects: part 1. An Bras Dermatol 2014; 89 (02) 205-218
- 9 Carl DJ, Habusta SF. Hand Tendon Transfers. Treasure Island, FL:: StatPearls Publishing;; 2023
- 10 Johnson SP, Sebastin SJ, Rehim SA, Chung KC. The importance of hand appearance as a patient-reported outcome in hand surgery. Plast Reconstr Surg Glob Open 2015; 3 (11) e552
- 11 Coleman SR. Structural fat grafting: more than a permanent filler. Plast Reconstr Surg 2006; 118 (03) 108S-120S
- 12 Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1977; 1 (03) 385-401
- 13 Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 2006; 166 (10) 1092-1097
- 14 Rihani J. Microfat and nanofat: when and where these treatments work. Facial Plast Surg Clin North Am 2019; 27 (03) 321-330
- 15 Jakubietz RG, Jakubietz MG, Kloss D, Gruenert JG. Defining the basic aesthetics of the hand. Aesthetic Plast Surg 2005; 29 (06) 546-551
- 16 Giunta RE, Eder M, Machens HG, Müller DF, Kovacs L. Structural fat grafting for rejuvenation of the dorsum of the hand. Handchir Mikrochir Plast Chir 2010; 42 (02) 143-147
- 17 Butterwick KJ. Rejuvenation of the aging hand. Dermatol Clin 2005; 23 (03) 515-527 , vii
- 18 Bank J, Fuller SM, Henry GI, Zachary LS. Fat grafting to the hand in patients with Raynaud phenomenon: a novel therapeutic modality. Plast Reconstr Surg 2014; 133 (05) 1109-1118
- 19 Khouri Jr RK, Khouri RK. Current clinical applications of fat grafting. Plast Reconstr Surg 2017; 140 (03) 466e-486e
- 20 Fantozzi F. Hand rejuvenation with fat grafting: a 12-year single-surgeon experience. Eur J Plast Surg 2017; 40 (05) 457-464
- 21 DeLorenzi C. Complications of injectable fillers, part I. Aesthet Surg J 2013; 33 (04) 561-575
- 22 Conlon CJ, Abu-Ghname A, Davis MJ. et al. Fat grafting for hand rejuvenation. Semin Plast Surg 2020; 34 (01) 47-52
- 23 Zhou J, Xie Y, Wang WJ. et al. Hand rejuvenation by targeted volume restoration of the dorsal fat compartments. Aesthet Surg J 2017; 38 (01) 92-100
- 24 Yun-Nan L, Shu-Hung H, Tsung-Ying L. et al. Micro-autologous fat transplantation for rejuvenation of the dorsal surface of the aging hand. J Plast Reconstr Aesthet Surg 2018; 71 (04) 573-584
- 25 illanueva NL, Hill SM, Small KH, Rohrich RJ. Technical refinements in autologous hand rejuvenation. Plast Reconstr Surg 2015; 136 (06) 1175-1179
- 26 Galea LA, Nicklin S. Mycobacterium abscessus infection complicating hand rejuvenation with structural fat grafting. J Plast Reconstr Aesthet Surg 2009; 62 (02) e15-e16
- 27 Vara AD, Miki RA, Alfonso DT, Cardoso R. Hand fat grafting complicated by abscess: a case of a bilateral hand abscess from bilateral hand fat grafting. Hand (N Y) 2013; 8 (03) 348-351
Address for correspondence
Publication History
Article published online:
04 November 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Billings Jr E, May Jr JW. Historical review and present status of free fat graft autotransplantation in plastic and reconstructive surgery. Plast Reconstr Surg 1989; 83 (02) 368-381
- 2 Coleman SR. Facial recontouring with lipostructure. Clin Plast Surg 1997; 24 (02) 347-367
- 3 Neuber F. Fettransplantation. Bericht über die Verhandlungen der deutschen Gesellscaft für Chirurgie. Zentralbl Chir 1893; 22: 66
- 4 Fournier PF. Who should do syringe liposculpturing?. J Dermatol Surg Oncol 1988; 14 (10) 1055-1056
- 5 Abergel RP, David LM. Aging hands: a technique of hand rejuvenation by laser resurfacing and autologous fat transfer. J Dermatol Surg Oncol 1989; 15 (07) 725-728
- 6 Aboudib Júnior JH, de Castro CC, Gradel J. Hand rejuvenescence by fat filling. Ann Plast Surg 1992; 28 (06) 559-564
- 7 Coleman SR. Hand rejuvenation with structural fat grafting. Plast Reconstr Surg 2002; 110 (07) 1731-1744 , discussion 1745–1747
- 8 Lastória JC, Abreu MA. Leprosy: review of the epidemiological, clinical, and etiopathogenic aspects: part 1. An Bras Dermatol 2014; 89 (02) 205-218
- 9 Carl DJ, Habusta SF. Hand Tendon Transfers. Treasure Island, FL:: StatPearls Publishing;; 2023
- 10 Johnson SP, Sebastin SJ, Rehim SA, Chung KC. The importance of hand appearance as a patient-reported outcome in hand surgery. Plast Reconstr Surg Glob Open 2015; 3 (11) e552
- 11 Coleman SR. Structural fat grafting: more than a permanent filler. Plast Reconstr Surg 2006; 118 (03) 108S-120S
- 12 Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1977; 1 (03) 385-401
- 13 Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 2006; 166 (10) 1092-1097
- 14 Rihani J. Microfat and nanofat: when and where these treatments work. Facial Plast Surg Clin North Am 2019; 27 (03) 321-330
- 15 Jakubietz RG, Jakubietz MG, Kloss D, Gruenert JG. Defining the basic aesthetics of the hand. Aesthetic Plast Surg 2005; 29 (06) 546-551
- 16 Giunta RE, Eder M, Machens HG, Müller DF, Kovacs L. Structural fat grafting for rejuvenation of the dorsum of the hand. Handchir Mikrochir Plast Chir 2010; 42 (02) 143-147
- 17 Butterwick KJ. Rejuvenation of the aging hand. Dermatol Clin 2005; 23 (03) 515-527 , vii
- 18 Bank J, Fuller SM, Henry GI, Zachary LS. Fat grafting to the hand in patients with Raynaud phenomenon: a novel therapeutic modality. Plast Reconstr Surg 2014; 133 (05) 1109-1118
- 19 Khouri Jr RK, Khouri RK. Current clinical applications of fat grafting. Plast Reconstr Surg 2017; 140 (03) 466e-486e
- 20 Fantozzi F. Hand rejuvenation with fat grafting: a 12-year single-surgeon experience. Eur J Plast Surg 2017; 40 (05) 457-464
- 21 DeLorenzi C. Complications of injectable fillers, part I. Aesthet Surg J 2013; 33 (04) 561-575
- 22 Conlon CJ, Abu-Ghname A, Davis MJ. et al. Fat grafting for hand rejuvenation. Semin Plast Surg 2020; 34 (01) 47-52
- 23 Zhou J, Xie Y, Wang WJ. et al. Hand rejuvenation by targeted volume restoration of the dorsal fat compartments. Aesthet Surg J 2017; 38 (01) 92-100
- 24 Yun-Nan L, Shu-Hung H, Tsung-Ying L. et al. Micro-autologous fat transplantation for rejuvenation of the dorsal surface of the aging hand. J Plast Reconstr Aesthet Surg 2018; 71 (04) 573-584
- 25 illanueva NL, Hill SM, Small KH, Rohrich RJ. Technical refinements in autologous hand rejuvenation. Plast Reconstr Surg 2015; 136 (06) 1175-1179
- 26 Galea LA, Nicklin S. Mycobacterium abscessus infection complicating hand rejuvenation with structural fat grafting. J Plast Reconstr Aesthet Surg 2009; 62 (02) e15-e16
- 27 Vara AD, Miki RA, Alfonso DT, Cardoso R. Hand fat grafting complicated by abscess: a case of a bilateral hand abscess from bilateral hand fat grafting. Hand (N Y) 2013; 8 (03) 348-351