

Subscribe to RSS
DOI: 10.1055/s-0044-1791953
Circumferential Endoscopic Submucosal Dissection for Barrett's Esophagus with Multifocal High-Grade Dysplasia
Authors

Abstract
A 54-year-old male presented with longstanding history of heartburn and regurgitation. Upper gastrointestinal endoscopy and biopsy performed at the previous center were suggestive of Barrett's esophagus with high-grade dysplasia (HGD). In view of dysplasia with underlying Barrett's esophagus, endoscopic submucosal dissection (ESD) was planned. Multifocal high-grade dysplasia with underlying Barrett's esophagus needs treatment to prevent invasive cancer. Surgery has been the conventional treatment but is associated with morbid complications and mortality. ESD has emerged as a treatment for HGD and superficial adenocarcinoma in Barrett's segment, but circumferential ESD is associated with risk of stricture formation. The present case highlights the role of image-enhanced endoscopy in identifying dysplasia in Barrett's esophagus and minimally invasive endoscopic techniques as an alternative to conventional surgical techniques and prophylactic measures needed to prevent post-ESD complications.
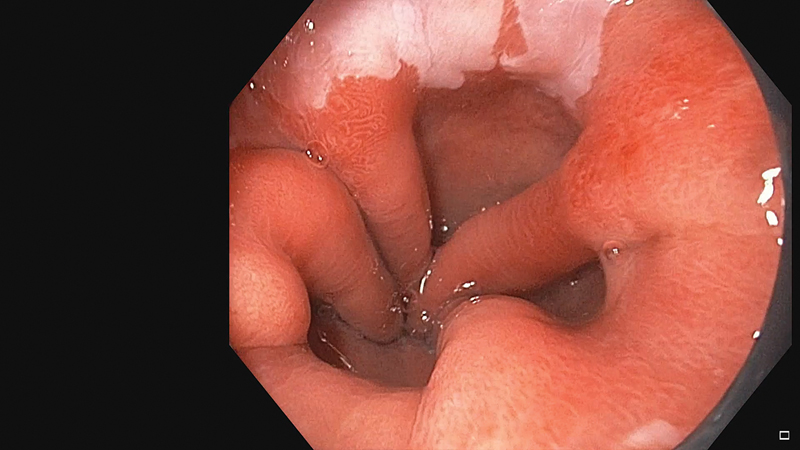
A 54-year-old male presented with longstanding history of heartburn and regurgitation. Upper gastrointestinal endoscopy and biopsy performed at the previous center was suggestive of Barrett's esophagus with high-grade dysplasia). In view of dysplasia with underlying Barrett's esophagus, endoscopic submucosal dissection (ESD) was planned. Positron emission tomography ([Fig. 1]) and computed tomography ([Fig. 2]) revealed normal esophageal wall thickening without any suspicion of lymph node or distant organ involvement. Radial endoscopic ultrasonography (GF-UE160, Olympus, Tokyo, Japan) did not reveal any submucosal layer involvement. Narrow band imaging (NBI) with dual focus and electronic magnification was performed (Gastroscope, GIF-HQ190, Olympus, Tokyo, Japan) prior to ESD to identify the margins of dysplastic area using Asia-Pacific Barrett's Consortium classification[1] ([Figs. 3] and [4]). Long-segment Barrett's esophagus (C2, M5: according to Prague C & M criteria)[2] and multifocal areas of high-grade dysplasia were suspected involving 2, 5 o'clock (at 38 cm from incisors) and 7 o'clock (at 35 cm from incisors) position and circumferential ESD was planned after explaining the possible complications.



Equipment and Procedure
Whole procedure was performed under general anesthesia after endotracheal intubation. Circumferential ESD was performed with a gastroscope (GIF-HQ190, Olympus, Tokyo, Japan) equipped with a transparent distal attachment (D-201–11804, Olympus, Tokyo, Japan). CO2 insufflation with low flow tubing was used throughout the procedure (Olympus CO2 insufflator). Electrosurgical units enabled with a microprocessor was used for the whole procedure (ERBE, VIO 300D, Tübingen, Germany). Dual J knife (KD-655L; Olympus) was used for marking, incision, and submucosal dissection, and Coagrasper (FD-411UR; Olympus) was used for prophylactic coagulation and hemostasis ([Video 1]). Normal saline stained with methylene blue was used for submucosal injection prior to incision and during submucosal dissection. A 25 G sclerotherapy (V-JECTOR; Endo-Med, Uttar Pradesh, India) needle was used to raise submucosal cushion prior to incision. Distal and proximal ends of Barrett's segment were mapped with NBI and marking was performed 5 mm outside the Barrett's segment (Soft coagulation, 60 W, effect 4). Circumferential incision was performed below distal markings (Endocut I, duration 2, interval 2, effect 2). Partial mucosal incision was given above the proximal markings (Endocut I, duration 2, interval 2, effect 2). A submucosal tunnel was created (Forced coagulation, effect 2, 40 W) and proximal and distal incisions were connected. Proximal incision was extended circumferentially and submucosal dissection was completed and en bloc resection was achieved (IT knife 2, KD-611L, Olympus; [Fig. 5]). Prophylactic coagulation was performed (Soft coagulation, 60 W, effect 4) and no bleed occurred during the procedure. The total procedure time was 130 minutes. Histopathological examination confirmed multifocal high-grade dysplasia limited to surface epithelium with complete resection (R 0) and free proximal, distal, and deep margins (pTisN0M0) suggestive of curative resection ([Fig. 6]). No bleed or gas-related complication occurred during the procedure. There was no superficial or deep muscular injury. Extubation was performed in endoscopy suite and patient was shifted to ward after 2 hours of procedure. Injectable pantoprazole and ceftriaxone were started after the procedure, and liquid diet was allowed after 24 hours. After 48 hours of procedure, a fully covered self-expandable metal stent (100 mm × 18 mm; FcSEMS, Wall flex, Boston scientific, Boston, United States) was placed and the stent was fixed with the loop and clip technique as previously[3] described ([Fig. 7]). In this technique, the endoscope was withdrawn, a rat tooth forcep was passed through the accessory channel and 30 mm endoloop (MAJ – 254; Olympus) was grasped and partially pulled into the channel of endoscope. Once the endoscope tip was close to upper margin of esophageal self-expanding metallic stents (SEMS), the endoloop was fixed at one end to the upper margin of stent using the scope clips (HX-610–090L, Olympus). The endoloop was then fixed to the esophageal wall mucosa using six more clips. No complication occurred during hospital stay and the patient was discharged at 72 hours after the procedure. At 12 weeks after placement of the stent, the patient was asymptomatic and SEMS removal was done at 12 weeks. The patient is doing well and under close follow-up. Multifocal high-grade dysplasia with underlying Barrett's esophagus needs treatment to prevent invasive cancer.[4] Surgery has been conventional treatment but is associated with morbid complications and mortality.[5] ESD has emerged as treatment for high-grade dysplasia and superficial adenocarcinoma in Barrett's segment, but circumferential ESD is associated with stricture formation.[6] Multiple sessions of steroid injection or balloon dilatation have been advocated as a preventive strategy. SEMS placement has emerged as a new technique for prevention and treatment of stricture after ESD.[7] The present case highlights the role of image-enhanced endoscopy in identifying dysplasia in Barrett's esophagus and minimally invasive endoscopic techniques as an alternative to conventional surgical techniques and a prophylactic measure needed to prevent post-ESD complications.
Video 1 Circumferential endoscopic submucosal dissection of long-segment Barrett's mucosa with high-grade dysplasia on image-enhanced endoscopy and post-ESD SEMS placement to prevent stricture formation. ESD, endoscopic submucosal dissection.



Conflict of Interest
None declared.
-
References
- 1 Singh R, Jayanna M, Wong J. et al. Narrow-band imaging and white-light endoscopy with optical magnification in the diagnosis of dysplasia in Barrett's esophagus: results of the Asia-Pacific Barrett's Consortium. Endosc Int Open 2015; 3 (01) E-14-E-18
- 2 Sharma P, Dent J, Armstrong D. et al. The development and validation of an endoscopic grading system for Barrett's esophagus: the Prague C & M criteria. Gastroenterology 2006; 131 (05) 1392-1399
- 3 Singla V, Khare S, Arora A. et al. Use of loop and clips to prevent migration of esophageal stent. Endoscopy 2021; 53 (11) E421-E422
- 4 Sharma P, Shaheen NJ, Katzka D, Bergman JJGHM. AGA clinical practice update on endoscopic treatment of barrett's esophagus with dysplasia and/or early cancer: expert review. Gastroenterology 2020; 158 (03) 760-769
- 5 Wright CD, Kucharczuk JC, O'Brien SM, Grab JD, Allen MS. Society of Thoracic Surgeons General Thoracic Surgery Database. Predictors of major morbidity and mortality after esophagectomy for esophageal cancer: a Society of Thoracic Surgeons General Thoracic Surgery Database risk adjustment model. J Thorac Cardiovasc Surg 2009; 137 (03) 587-595 , discussion 596
- 6 Katada C, Muto M, Manabe T, Boku N, Ohtsu A, Yoshida S. Esophageal stenosis after endoscopic mucosal resection of superficial esophageal lesions. Gastrointest Endosc 2003; 57 (02) 165-169
- 7 Martinek J. How to prevent post-ESD esophageal stricture. Endosc Int Open 2019; 7 (06) E771-E773
Address for correspondence
Publication History
Article published online:
26 December 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Singh R, Jayanna M, Wong J. et al. Narrow-band imaging and white-light endoscopy with optical magnification in the diagnosis of dysplasia in Barrett's esophagus: results of the Asia-Pacific Barrett's Consortium. Endosc Int Open 2015; 3 (01) E-14-E-18
- 2 Sharma P, Dent J, Armstrong D. et al. The development and validation of an endoscopic grading system for Barrett's esophagus: the Prague C & M criteria. Gastroenterology 2006; 131 (05) 1392-1399
- 3 Singla V, Khare S, Arora A. et al. Use of loop and clips to prevent migration of esophageal stent. Endoscopy 2021; 53 (11) E421-E422
- 4 Sharma P, Shaheen NJ, Katzka D, Bergman JJGHM. AGA clinical practice update on endoscopic treatment of barrett's esophagus with dysplasia and/or early cancer: expert review. Gastroenterology 2020; 158 (03) 760-769
- 5 Wright CD, Kucharczuk JC, O'Brien SM, Grab JD, Allen MS. Society of Thoracic Surgeons General Thoracic Surgery Database. Predictors of major morbidity and mortality after esophagectomy for esophageal cancer: a Society of Thoracic Surgeons General Thoracic Surgery Database risk adjustment model. J Thorac Cardiovasc Surg 2009; 137 (03) 587-595 , discussion 596
- 6 Katada C, Muto M, Manabe T, Boku N, Ohtsu A, Yoshida S. Esophageal stenosis after endoscopic mucosal resection of superficial esophageal lesions. Gastrointest Endosc 2003; 57 (02) 165-169
- 7 Martinek J. How to prevent post-ESD esophageal stricture. Endosc Int Open 2019; 7 (06) E771-E773