Subscribe to RSS
DOI: 10.1055/s-0044-1793826
Anatomic Posterolateral Corner Reconstruction of the Knee Using Single Semitendinosus Autograft: Technical Note for the Borderline-length Graft
Article in several languages: português | EnglishAuthors
Financial Support The authors declare that they did not receive financial support from agencies in the public, private, or non-profit sectors to conduct the present study.

Abstract
The original LaPrade technique for anatomic reconstruction of the posterolateral corner of the knee uses two separate allografts. More recently, a modification of this technique, using an adjustable-length suspension device with a cortical button for tibial fixation, allows anatomic reconstruction with a single semitendinosus autograft. This modification is of utmost relevance when sources of allograft are not available for multiligament knee reconstruction. In both techniques interference screws are used for femoral fixation of the fibular collateral ligament and popliteus tendon. The minimum length recommended for the anatomic reconstruction with single semitendinosus is 25 cm, but anatomic variations in the population exist, and a longer semitendinosus may be necessary. Indeed, some patients may only reach the necessary length considering the thinnest limb of the semitendinosus. In these patients, femoral fixation of the thinnest limb with a knotless suture anchor, as we describe, for the popliteus tendon limb, allows expansion of this technique to borderline semitendinosus autografts while reducing the risk of tunnel coalition. We also describe a different sequence of steps: fixation of the fibular collateral ligament in the femoral tunnel followed by its tensioning and fixation in the fibular head tunnel, fixation of the popliteus tendon in its femoral footprint with a knotless suture anchor and, finally, tensioning of the popliteofibular ligament and popliteus tendon. This different sequence also helps avoiding tendon waste, which may be left over, allowing more graft incorporation into the tibial tunnel.
Introduction
The posterolateral corner (PLC) of the knee consists of three major static stabilizers which restrain varus and external rotation: the fibular collateral ligament (FCL), the popliteus tendon (PT), and the popliteofibular ligament (PFL). The mechanism of injury involves varus stress, hyperextension and twisting of the knee. Posterolateral corner insufficiency may result in meniscal injuries and accelerated medial compartment osteoarthritis.[1] Posterolateral corner injuries rarely occur in isolation, being typically associated with injury to one or both cruciate ligaments. In the setting of a multiligament injury, failure to address concomitant PLC insufficiency leads to increased forces on the reconstructed cruciate ligaments and may lead to surgical failure.[2] [3]
Many techniques, both anatomic and nonanatomic, have been described. Although some studies present similar clinical outcomes of anatomic and nonanatomic techniques,[4] some biomechanical studies favor anatomic PLC reconstruction.[1] [3] [5] The original anatomic technique, published by LaPrade et al.[1] requires two separate allografts of the Achilles tendon: one for the FCL and PFL and another for the PT. Modifications of the technique, in which two separate hamstrings autografts are used, have also been described.[3] [6] However, since PLC lesions commonly occur in association with other ligament injuries, harvesting two hamstrings for the PLC reconstruction increases graft harvesting morbidity. In 2019, Wood et al. [2] described a modification of the LaPrade et al.[1] technique using an adjustable-length suspension device with a cortical button for tibial fixation of the PFL and PT limbs, allowing PLC reconstruction with a single semitendinosus (ST) autograft. This technique modification is a game changer when sources of allograft are not available for multiligament knee reconstruction. The minimum ST length recommended by the authors is 25 cm.[2] However, there are anatomic variations in the population[7] [8] ([Table 1]), and a longer ST may be necessary. In our experience, some patients may only reach the necessary length considering the thinnest limb of the ST.
|
Anatomic structure |
Graft length needed in millimeters (range) |
|---|---|
|
Fibular collateral ligament |
69.6 (62.6–73.5)[7] |
|
Popliteus tendon |
54.5 (50.5–61.2)[7] |
|
Popliteofibular ligament |
14.7 (12.2–17.2)[8] |
|
Fibular head tunnel |
36.3 (31.2–40.7)[7] |
|
Femoral tunnels |
|
|
Tibial tunnel |
Remaining graft length |
The objective of this technical note is to describe a modification of the Wood et al. [2] technique with femoral fixation of the thinnest limb of the graft with a knotless suture anchor ([Fig. 1]). We also propose a different sequence of steps to help reduce tendon waste and allow more incorporation of the graft into the tibial tunnel.

Surgical Technique
The last author was the leading surgeon and the one who developed the technique.
The patient was positioned supine, with a lateral thigh post and a footrest at 90° flexion. A tourniquet was placed around the proximal thigh and inflated as required.
As described by LaPrade et al.[1] and Wood et al.,[2] a lateral approach including neurolysis of the common peroneal nerve was performed. Then, a horizontal incision was made over the tendon of the long head of the biceps femoris with exposure of the fibular head and identification of the FCL remnant, which was tagged with traction sutures, allowing the identification of its femoral and fibular footprints. Subperiosteal dissection of the lateral aspect of the fibular head was then performed with exposure of the “champagne glass drop-off transition” and the fibular head tunnel was created (6 × 35 mm), from anterolateral to posteromedial, with the aid of a proper fibular head aiming device (Arthrex Inc., Naples, FL, USA). Then, distally and medial to the Gerdy's tubercle, the “flat spot” on the anterior tibia was identified as well as the musculotendinous junction of the popliteus on the posterior tibia, proximally and medially do the fibular head tunnel. A proper tibial aiming device (Arthrex Inc.) was used, and a complete tibial tunnel for the PFL and PT was created. A second horizontal incision was made on the iliotibial band at the level of the lateral epicondyle with identification of the femoral footprint of the FCL, and an L-shaped capsulotomy was made allowing visualization of the PT footprint on the anterior popliteal sulcus.[1] [2]
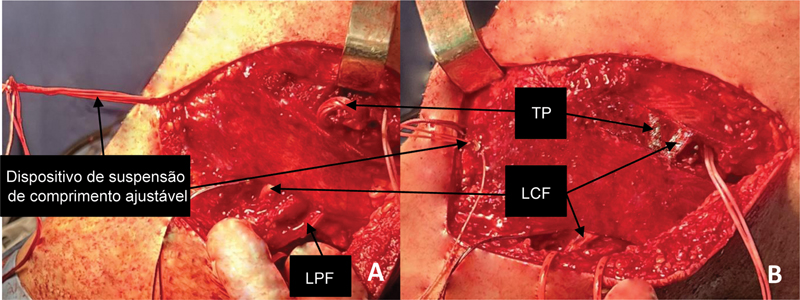
The harvested ST measuring 27 cm, considering its thinnest extremity of 2.5 cm, was tubularized with whipstitched sutures for easy passage into the tunnels of the femur, fibular head, and tibia. The graft was passed into the fibular head tunnel ([Fig. 2A]), and an initial estimation of the necessary length was made ([Fig. 2B]). For femoral fixation of the FCL, after preparation of the FCL footprint ([Fig. 3A]) and proper guide pin placement ([Fig. 3B]), a 6 × 25-mm tunnel was created, and a passing suture was left in place. Sequential fixation of the graft then took place. First, the thickest extremity of the graft was pulled into the femoral tunnel and secured with a 7 × 25-mm interference screw (BioComposite FastThread - Arthrex Inc., [Fig. 4A]). Then, the graft was fixed in the fibular head with a 7 × 25-mm screw (BioCompsite FastThread - Arthrex Inc, [Fig. 4B]) in neutral rotation, 30° flexion and valgus stress. The graft was then passed through the loop of an adjustable-length suspension device (Attachable Button System- Arthrex Inc.). The suspension device was then passed anteriorly through the tibial tunnel, and a cortical button was applied. The PT limb was then passed along the popliteal hiatus to its footprint. Since this extremity of the graft was not thick enough for interference screw fixation, a knotless suture anchor was used instead. In more detail, the popliteus tendon limb was whipstitched and passed through the eyelet of a 4.75 × 19.1-mm knotless suture anchor which was applied in its footprint (BioComposite SwiveLock - Arthrex Inc., [Figs. 5A,B]). The PT and PFL were then tensioned in 60° flexion and neutral rotation ([Figs. 6A,B]). After fixation of all structures, knee stability and range of motion were tested. Following copious irrigation of the tissues, the lateral capsule, iliotibial band, subcutaneous tissue, and skin were closed in a standard fashion. The main surgical steps are summarized in [Table 2].





|
Surgical step |
Details |
|---|---|
|
Positioning |
Supine with a lateral thigh post and a footrest at 90° flexion. |
|
Approach |
Lateral approach as described by LaPrade et al. [1] and Wood et al. [2] including neurolysis of the common peroneal nerve. |
|
Fibular head tunnel preparation |
Subperiosteal dissection of the lateral aspect of the fibular head exposing the “champagne glass drop-off transition” and drilling of the fibular head tunnel from anterolateral to posteromedial. |
|
Tibial tunnel preparation |
Identification of the “flat spot” on the anterior tibia and the popliteus musculotendinous junction on the posterior tibia and drilling of the tibial tunnel. |
|
Femoral tunnel preparation |
Identification of the FCL footprint through traction sutures and creation of the femoral tunnel aiming anteriorly and proximally. Capsulotomy and exposure of the PT footprint on the anterior popliteal sulcus. |
|
Graft fixation sequence |
1. Fixation of the thickest extremity of the graft in the femoral tunnel with an interference screw. 2. Passage of the graft into the fibular head tunnel and fixation with an interference screw in neutral rotation, 30° flexion and valgus. 3. Passage of the graft through the loop of the adjustable-length suspension device. 4. Passage of the suspensory system anteriorly through the tibial tunnel and application of the cortical button. 5. Passage of the thin PT limb through the popliteal hiatus and the eyelet of a knotless suture anchor and fixation in its footprint. 6. Tensioning of the PT and PFL at 60° flexion and neutral rotation. |
Rehabilitation
After PLC reconstruction, patients used a dynamic posterior cruciate ligament hinged knee brace and mobilized non-weight bearing for 6 weeks. Range of motion was initiated postoperatively and gradually progressed to full range of motion. The brace was discontinued at 3 months, and further rehabilitation focused on strength and proprioceptive training. Exercises to prevent posterior sag, as well as external rotation and open-chain exercises, were avoided until this stage. Return to sports was allowed at 9 months, when strength, stability, and knee range of motion were comparable to the contralateral side.
Final Comments
The original anatomic technique by LaPrade et al.[1] using two separate allografts has proven biomechanical and clinical results.[1] [3] [5] The Wood et al.[2] modification of this technique, using an adjustable-length suspension device, has the advantage of using a single ST autograft, reducing multiple graft harvesting morbidity. In a recent cadaveric study, both techniques restored normal native varus. Similar outcomes were obtained for external rotation in extension. However, for external rotation at 60° and 90° of flexion, the knee was overtensioned with the Wood et al.[2] technique, meaning special care should be taken during tensioning with this technique.[9]
The main limitation of the Wood et al.[2] technique is the length of the harvested ST graft.[2] Indeed, some patients may only reach the necessary length considering the thinnest limb of the ST ([Table 1]). Our modification, with femoral fixation of the thinnest limb with a knotless suture anchor, allows expansion of this technique to the borderline length graft. An additional benefit is the reduction of the number of tunnels in the femur, decreasing the risk of tunnels coalition. Finally, our sequence, with reconstruction of the FCL first and tensioning of the PT and PFL only after fixation of the PT in its footprint, avoids tendon waste, which may be left over with the sequence described by Wood et al.,[2] allowing more incorporation of the graft into the tibial tunnel. The advantages and disadvantages of the authors' modifications are summarized in [Table 3].
|
Advantages |
Disadvantages |
|---|---|
|
Knotless suture anchor fixation of the thinnest limb maximizes ST usage allowing anatomic PLC reconstruction with borderline length grafts. |
PLC reconstruction with nonanatomic techniques can be performed with shorter ST autografts and are surgically less demanding and invasive. |
|
Knotless suture anchor fixation of the PT excludes the need for a second femoral tunnel reducing the risk of tunnels coalition. |
Knotless suture anchor fixation of the PT limb may not be as strong as interference screw fixation. Additional biomechanical studies are needed. |
|
The authors' sequence reduces tendon waste which may be left over with the sequence described by Wood et al maximizing graft usage. |
In the presence of a graft too short for the technique, biceps femoris tenodesis for reconstruction of the FCL may be considered.[3]
Like Wood et al.[2] described, in the setting of combined cruciate ligament reconstruction, we recommend performing the approach to the PLC prior to cruciate ligament reconstruction, to prevent fluid extravasation into the soft tissues and distortion of tissue planes.
The main risks associated with our procedure are the same as the ones described by Wood et al.,[2] namely: common peroneal nerve palsy, fibular head fracture, and tunnel coalition with an anterior cruciate ligament femoral tunnel ([Fig. 3]). To avoid coalition, we recommend following the same tips described in their paper: drilling of the femoral tunnels anteriorly and proximally (30°) as well as second look with the arthroscope after pin insertion to verify no coalition exists before tunnel drilling.[2]
Conclusion
In conclusion, in the presence of a borderline ST for single ST anatomic PLC reconstruction, knotless suture anchor fixation of the thinnest limb, and the sequence described by us should be considered to maximize graft usage.
Conflito de Interesses
Os autores não têm conflito de interesses a declarar.
Ethical Approval
Ethical approval was not sought for the present technical note since no patient data can be identified. Informed consent is also not applicable for the aforementioned reason.
Work carried out at the Orthopedics Department, Centro Hospitalar do Tâmega e Sousa, Penafiel, Portugal.
-
Referências
- 1 Serra Cruz R, Mitchell JJ, Dean CS, Chahla J, Moatshe G, LaPrade RF. Anatomic Posterolateral Corner Reconstruction. Arthrosc Tech 2016; 5 (03) e563-e572
- 2 Wood R, Robinson J, Getgood A. Anatomic posterolateral corner reconstruction using single graft plus adjustable-loop suspensory fixation device. Arthrosc Tech 2019; 8 (03) e301-e309
- 3 Franciozi CE, Albertoni LJB, Kubota MS. et al. A hamstring-based anatomic posterolateral knee reconstruction with autografts improves both radiographic instability and functional outcomes. Arthroscopy 2019; 35 (06) 1676-1685.e3
- 4 Boksh K, Ghosh A, Narayan P, Divall P, Aujla R. Fibular- Versus Tibiofibular-Based Reconstruction of the Posterolateral Corner of the Knee: A Systematic Review and Meta-analysis. [published online ahead of print, 2023 Jan 4] Am J Sports Med 2023;•••:3635465221138548
- 5 Pioger C, Bouché PA, Haen TX, Pujol N. Comparison of three surgical techniques of posterolateral knee reconstruction: A cadaver study. Orthop Traumatol Surg Res 2022; 108 (08) 103414
- 6 Pache S, Sienra M, Larroque D. et al. Anatomic posterolateral corner reconstruction using semitendinosus and gracilis autografts: Surgical technique. Arthrosc Tech 2021; 10 (02) e487-e497
- 7 LaPrade RF, Bollom TS, Wentorf FA, Wills NJ, Meister K. Mechanical properties of the posterolateral structures of the knee. Am J Sports Med 2005; 33 (09) 1386-1391
- 8 LaPrade RF, Ly TV, Wentorf FA, Engebretsen L. The posterolateral attachments of the knee: a qualitative and quantitative morphologic analysis of the fibular collateral ligament, popliteus tendon, popliteofibular ligament, and lateral gastrocnemius tendon. Am J Sports Med 2003; 31 (06) 854-860
- 9 Vivacqua T, Vakili S, Willing R, Moatshe G, Degen R, Getgood AM. Biomechanical assessment of knee laxity after a novel posterolateral corner reconstruction technique. Am J Sports Med 2022; 50 (04) 962-967
Endereço para correspondência
Publication History
Received: 08 June 2023
Accepted: 04 September 2023
Article published online:
21 December 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution 4.0 International License, permitting copying and reproduction so long as the original work is given appropriate credit (https://creativecommons.org/licenses/by/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referências
- 1 Serra Cruz R, Mitchell JJ, Dean CS, Chahla J, Moatshe G, LaPrade RF. Anatomic Posterolateral Corner Reconstruction. Arthrosc Tech 2016; 5 (03) e563-e572
- 2 Wood R, Robinson J, Getgood A. Anatomic posterolateral corner reconstruction using single graft plus adjustable-loop suspensory fixation device. Arthrosc Tech 2019; 8 (03) e301-e309
- 3 Franciozi CE, Albertoni LJB, Kubota MS. et al. A hamstring-based anatomic posterolateral knee reconstruction with autografts improves both radiographic instability and functional outcomes. Arthroscopy 2019; 35 (06) 1676-1685.e3
- 4 Boksh K, Ghosh A, Narayan P, Divall P, Aujla R. Fibular- Versus Tibiofibular-Based Reconstruction of the Posterolateral Corner of the Knee: A Systematic Review and Meta-analysis. [published online ahead of print, 2023 Jan 4] Am J Sports Med 2023;•••:3635465221138548
- 5 Pioger C, Bouché PA, Haen TX, Pujol N. Comparison of three surgical techniques of posterolateral knee reconstruction: A cadaver study. Orthop Traumatol Surg Res 2022; 108 (08) 103414
- 6 Pache S, Sienra M, Larroque D. et al. Anatomic posterolateral corner reconstruction using semitendinosus and gracilis autografts: Surgical technique. Arthrosc Tech 2021; 10 (02) e487-e497
- 7 LaPrade RF, Bollom TS, Wentorf FA, Wills NJ, Meister K. Mechanical properties of the posterolateral structures of the knee. Am J Sports Med 2005; 33 (09) 1386-1391
- 8 LaPrade RF, Ly TV, Wentorf FA, Engebretsen L. The posterolateral attachments of the knee: a qualitative and quantitative morphologic analysis of the fibular collateral ligament, popliteus tendon, popliteofibular ligament, and lateral gastrocnemius tendon. Am J Sports Med 2003; 31 (06) 854-860
- 9 Vivacqua T, Vakili S, Willing R, Moatshe G, Degen R, Getgood AM. Biomechanical assessment of knee laxity after a novel posterolateral corner reconstruction technique. Am J Sports Med 2022; 50 (04) 962-967