Keywords
Value-sensitive design - Artificial Intelligence - Ethical value – Universal Design
- Healthcare
1. Introduction
Value Sensitive Design (VSD) represents a comprehensive approach to embed human values
in the creation of technology. A topical and timely area of healthcare innovation,
artificial intelligence (AI) describes the use of computers and technology to simulate
intelligent behavior comparable to human critical thinking [[1]]. Public perception of recent advances in AI and widespread availability of AI-based
tools have catalyzed interest in their clinical application [[2]
[3]
[4]
[5]
[6]]. Current applications of AI in healthcare include medical imaging and diagnostics,
personalized medicine, virtual health assistants and chatbots, and predictive analytics
and risk assessment [[7]]. These applications rely on computational methods ranging from machine learning
(ML), natural language processing (NLP), computer vision (CV), and generative models
such as large language models (LLMs).
Healthcare AI has been a mainstay of predictive and preventive clinical decision support
(CDS) for decades and has been the subject of rigorous evaluation [[9]]. Scalable algorithmic tools present the promise of dramatically improving care
while also risking the perils of harm at scale [[10]]. Creating and deploying AI without robust ethical frameworks and rigorous testing
might perpetuate bias, discrimination, and introduce privacy, security risks [[11]]. Regardless of the nature of underlying AI, generative or not, actionable healthcare
AI requires careful integration of algorithmic insights into clinical workflow, which
can be achieved through effective design that engages patients and healthcare professionals,
including clinicians, nurses, and allied health staff.
Numerous views of design have emerged over the last fifty years [[12]]. Design disciplines emanate from different industries and areas, such as human
factors and interaction design linked to experimental psychology, and design thinking
which is rooted in the science of creativity [[12]] More recently in healthcare, human-centered design (HCD) has emerged as a means
of achieving effective design and lessening potential for risk [[13]
[14]
[15]]. In parallel, concepts like algorithmovigilance for healthcare AI have broadened
the discussion around preventing adverse effects of implemented AI [[16]]. VSD intends to place human values at the heart of technological design. Batya
Friedman et al., first introduced VSD in the 1990s, challenging the prevailing notion of technology
as value-neutral or simply a tool for human activities. Per Friedman et al., values are defined as “what is important to people in their lives, with a focus
on ethics and morality” [[13]]. Commonly recognized examples of such values include autonomy, trust, equity, and
justice. The VSD framework has been applied across various fields and has become a
recognized approach for addressing values in technological design [[17]]. While sharing some similarities with HCD in terms of considering users' needs
and experiences, VSD might complement HCD by considering social and ethical implications
of technology and impacts on various stakeholders and society at large. The framework
emphasizes three main areas of investigation: conceptual, empirical, and technical.
Each area builds on the prior, with conceptual investigations articulating values
and any value conflicts that might result from technology use. Empirical investigations
apply qualitative and quantitative methods to crystallize and document stakeholders'
values, needs, and practices. Finally, technical investigations focus on the design
and features of the technology itself, examining how values are or can be supported.
We emphasize the importance of applying VSD to healthcare AI because of the potentially
rapid development cycle, scalable nature, lack of knowledge among healthcare managers
about how it works, and its potential societal impact. The accelerated pace of AI
advancement has prompted ongoing debate concerning oversight and regulation. Government
entities, professional societies, scientific leadership groups, and other organizations
worldwide have begun issuing principles and guidance to attempt to outline and mitigate
large-scale societal risks [[18]
[19]
[20]
[21]]. Such concerns underline the need to characterize the societal values that should
be represented in the legislation and professional standards that will undoubtedly
emerge. Similarly, while HCD incorporates numerous strengths in the pursuit of effective
AI tools, a recent systematic review suggests key sociotechnical gaps remain: technical
limitations (e.g., predicted AI output will be inaccurate), workflow misalignment (e.g., AI tools will add to workload), attitudinal barriers (e.g., resistance to using AI tools, lack of desire to use AI tools), informational barriers
(e.g., AI output lacks actionable information to make the relevant clinical decision),
usability issues (e.g., lengthy ‘click-throughs’ as inputs to use AI tools), and environmental barriers
(e.g., requirements of AI tools such as high quality retinal imagery not available in routine
practice) [[9]]. Many of these gaps might be lessened by design that centers not just on the performance
of the humans interacting with the technology, but also on their values and the values
of other relevant stakeholders.
To better understand how well values are captured in modern healthcare AI, we conducted
a narrative review of the literature intersecting VSD, AI, and the design and implementation
of AI-driven healthcare technology. We assessed recent literature, 2022 through 2023
against Friedman's tripartite framework including modifications proposed by Umbrello
et al., incorporating Artificial Intelligence for Social Good (AI4SG) [[17],[22]]. We then evaluated all eligible studies for the presence of elements of VSD, critically
doing so regardless of whether VSD was directly acknowledged, as it is a newer and
lesser-known concept in the field than HCD. By demonstrating and dissecting VSD methodology
through real-world case studies, we aim to highlight areas of strength and potential
directions for improvement in the design of AI-driven technology that is both human-centered
and value-sensitive.
2. Methods
We conducted a narrative review informed by the PRISMA guidelines for systematic reviews
[[23]] with expectation that the state of the literature would not permit meta-analysis.
We searched PubMed, using a search query representing AI, design, and value. The PubMed
search query is shown (Box 1).
Box 1. Reproducible Search Query in PubMed.
(value sensitive design[tiab] OR value-sensitive design OR value[tiab] OR social value[tiab]
OR social good[tiab] OR ethical value[tiab] ) AND (“Universal Design”[Mesh] OR universal
design[tiab] OR design[tiab] OR human-centered design[tiab] OR “User-Centered Design”[Mesh]
OR user-centered[tiab] OR user-centred[tiab] OR user-centric[tiab] ) AND (“Artificial
Intelligence”[Mesh] OR artificial intelligence[tiab] OR AI [tiab] OR intelligent design[tiab]
OR intelligence design[tiab] OR machine intelligence[tiab] OR computational intelligence[tiab]
OR “Machine Learning”[Mesh] OR machine learning[tiab] OR learning machine[tiab] OR
“Deep Learning”[Mesh] OR deep learning[tiab] OR “Natural Language Processing”[Mesh]
OR natural language processing[tiab]) AND (2022:2023[pdat])
The initial list of publications was reviewed via title and abstract review by two
authors (Y.L., L.N.) to establish a full-text candidate list. The authors reviewed
initial results to eliminate papers that did not address a healthcare area and/or
were not English-language. Systematic reviews were also excluded though they informed
study design and background as above. Retracted studies identified by initial search
were excluded. The final group of studies was reviewed for elements of VSD and the
presence of a specific AI application, tabulated, and summarized with respect to clinical
application area, geographic diversity, methods, stakeholder engagement methods, and
VSD findings.
3. Results
From 2022 through January 2024, we identified 819 publications via the initial search;
five of the 819 had been retracted and were excluded. The initial reviews resulted
in 70 studies requiring full-text consideration and nine (9) studies being selected
for full-text review and extraction. A flow diagram summarizing the search is shown
([Figure 1]).
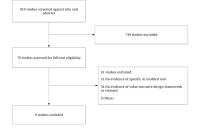 Figure 1. Flow diagram of the search strategy.
Figure 1. Flow diagram of the search strategy.
[Table 1] summarizes all studies reviewed in full-text including study objective and key findings
relevant to our survey. In the final group of studies, most were original research
or case studies. Clinical application area of these studies varied widely from rare
disease [[24]], dementia [[25]], sexual health [[26]], mental health [[27]], to stress management [[28]]. No two studies that met full text eligibility were in the same clinical domain.
In terms of AI application area, use cases primarily described predictive model and
CDS or consumer health informatics applications with mobile devices (smartphones).
Table 1.
Summary of all studies reviewed.
|
Article
|
Stakeholders
|
Sample Size
|
Study Objective
|
Major Findings
|
Examples of Value Discussed
|
AI Methods Studied
|
|
Cagliero et al. (2023)
|
Patients, clinicians, AI designers
|
17
|
Evaluate a „values collision“ approach to identify ethical challenges associated with
ML applications to healthcare (ML-HCA) for advance care planning (ACP).
|
Five key „values collisions“ were identified between stakeholders (patients, clinicians,
designers) regarding the ML-enabled ACP application, marking areas of ethical tension
ranging from end-of life workflow, which stakeholders receive prediction, to how and
if to protect early deployment research. From these findings, the design team prioritized
examining alternative workflow strategies, clarifying that mortality prediction was
only to identify ACP need (not other mortality-related ends), and shielding ongoing
research from social media scrutiny.
|
Article showed value collisions between stakeholders by different ethical concerns
including bias, transparency, patient consent, and patient involvement.
|
Supervised machine learning (tree-based risk models) to predict patient mortality
|
|
Cenci et al. (2023)
|
Danish patients with dementia (referred as „citizens“ in the manuscript), relatives,
volunteers, local authorities, dementia coordinators, healthcare professionals, AI/data
science experts, and social scientists/philosophers)
|
41
|
Demonstrate how a participatory value-sensitive design approach can be used to develop
an AI-based tracking smartphone (mHealth) app targeting Danish citizens with dementia.
|
This illustrative case study explored value construction and elicitation, demonstated
how moral dilemmas and value conflicts result from diverse needs or vested interests
can be resolved in practice. Through interations of focus group-based deliberative
workshops, both expert and non-expert stakeholders including those with dementia directly
contributed to identifying values to guide the app's design to be more ethical and
democratic.
|
Safety, privacy, social support
|
Real-time anomaly detection using spatiotemporal data
|
|
Fischer et al. (2023)
|
Obstetrician-gynecologists (OB-GYNs)
|
13
|
Explore obstetricians' perceptions about the potential value of AI in clinical practice.
|
Perceived usefulness and trust are two major themes identified from the interviews.
The result show 2 paradoxes between what the clinicians found most valuable in an
AI model and and what they considered necessary to trust an AI model. That is, AI
is expected to provide added value by surpassing human capabilities but there is a
great need for explainability. Additionally, participants desire comprehensive models
with many parameters, yet acknowledged that certain contextual factors should only
be considered by humans
|
Trust
|
AI scenarios: diagnosis of intrapartum fetal asphyxia, hospital discharge of women
with pre-term labor, and personalized treatment for gestational diabetes.
|
|
Götzl et al. (2022)
|
Young people and experts (psychologists, educators, respresentives of the digital
industry)
|
Focus group (n=8) Expert interviews (n=5) Online survey (n=666)
|
Explore the subjective needs, attitudes, and preferences of key stakeholders (young
people and experts) towards an AI-informed mobile mental health app (mHealth).
|
Both experts and young people showed general acceptance and interest towards AI-informed
mHealth. Young people showed openness to AI and data sharing, at the same time demanded
transparency and control over personalization. Experts perceived AI-informed mHealth
apps as opportunities to complement on-site delivery of interventions, improving the
chance to reach at-risk youth.
|
Transparency, trust
|
mHealth app using ecological momentary assessment (EMA) data.
|
|
Hallowell et al. (2022)
|
Clinical geneticists, data scientists, bioinformaticians, industry and patient support
group spokespersons
|
20
|
Explore under what conditions medical AI tools that employ machine learning can be
trusted, using the case of computational phenotyping (CP) to support diagnosis of
rare disease.
|
Interviewees emphasized the importance of establishing trust in the use of computational
phenotyping tools in identifying rare disease. Interviewees discussed trust both in
the context of relational trust, trusting those who use and develop AI, and epistemic
trust, trusting in the knowledge produced by the AI technology. Both patients' trust
for clinicians and clinicians' trust for AI developers were discussed. Trust in the
technology itself requires demonstrating reliability and accuracy of algorithm output
and involving trusted individuals in using/developing the tools.
|
Trust
|
Computational phenotyping
|
|
Helenason et al. (2023)
|
Primary care physicians (PCPs)
|
Interviews (n=15) Diagnostic assessment on image interpretation (n=25)
|
Employ qualitative and quantitative methods to investigate the feasibility of an AI-based
clinical decision support system (CDSS) to detect cutaneous melanoma in primary care.
|
Interviews with primary care physicians revealed that trust is a central concern,
which can be improved by evidence of sufficient diagnostic accuracy. „Usability and
user experience“ and „the clinical context“ also emerged as qualitative themes. When
assessing images, adding AI decision support increased physicians' sensitivity and
diagnostic accuracy compared to their assessments without the use of AI.
|
Trust
|
Convolutional neural network for dermatological image analysis
|
|
Helman et al. (2023)
|
Intensive Care Unit (ICU) clinicians (nurses, physician assistants, physicians)
|
23
|
Engage multidisciplinary intensive care unit (ICU) users (physicians, nurse practitioners,
physician assistants) in the development of a graphical user interface (GUI) to present
an AI-derived patient instability risk score.
|
Six themes emerged: analytics transparency, graphical interpretability, impact on
practice, value of trend synthesis of dynamic patient data, decisional weight, and
display location. All disciplines valued synthesized views but were skeptical of heavily
weighing AI output until proven trustworthy.
|
Autonomy, transparency, trust
|
Predictive modeling, clinical decision support
|
|
Kerr et al. (2023)
|
Employees of a Swiss insurance company
|
170
|
Identify relevant values and assess potential users' comprehension of these values
to derive requirements for the value sensitive design of a digital health solution
for workplace stress. This digital stress management intervention at the workplace
relies on ML to continuously predict the user's current stress level using multiple
data modalities: physiological, behavioral, and contextual data sources.
|
The values health and well-being, privacy, autonomy, accountability, and identity
(defined as people's understanding of who they are over time) were identified through
literature search. Employees showed moderate to high intention to use a digital stress
management intervention but had concerns regarding effectiveness and privacy. Privacy
and accountability concerns are higher when machine learning monitoring was involved.
Integrability, user-friendliness, and digital independence emerged as novel values
from the qualitative analysis.
|
Health and well-being, privacy, autonomy, accountability, identity
|
Real-time predictive modeling
|
|
Wang et al. (2022)
|
User of SnehAI (AI chatbot) application: young people in India
|
Qualitative data: 2 in-person group meetings, 4 virtual conference, unspecified number
of participants; Quantitative data: 135, 263 unique chatbot users (8.2 million messages
exchanged)
|
Use Gibson's theory of affordances to examine SnehAI, an AI chatbot for sexual and
reproductive health, and offer guidance on how such chatbots can promote sexual and
reproductive health and advocate for health entitlements of women and girls in India.
Affordances serve as a mechanism to identify values in this case.
|
SnehAI demonstrated strong evidence across fifteen functional affordances, several
of them reflecting social values: accessibility, multimodality, nonlinearity, compellability,
queriosity, editability, visibility, interactivity, customizability, trackability,
scalability, glocalizability, inclusivity, connectivity, and actionability. SnehAi
effectively engaged its users, especially young men. SnehAI presented itself as a
trusted source of educational and entertaining information and its natural language
processing system worked effectively to personalize the response and optimize user
experience.
|
Equitable access, civility, inclusivity
|
NLP Chatbot
|
3.1. Stakeholder Engagement and Methods
Unlike many AI-driven CDS studies aimed at clinician-users, studies in this survey
engaged a wide range of stakeholders from the general public, employees in the workplace,
patients with lived experience, clinicians, managers, and biomedical scientists. Geographic
diversity was limited, however, with the studies set solely in European countries
and the United States. Methods used included interviews (three studies), focus groups
(two studies), participatory design workshops (two studies), surveys (two studies),
and literature review (one study).
3.2. VSD Themes Addressed
The predominant element of VSD addressed in six of nine included studies was that
of value identification. Two addressed context analysis and the same two addressed
prototyping.
3.3. Studies incorporating methods of VSD
Cagliero et al., [[29]] explored the values of stakeholders in the context of a ML tool for advanced care
planning (ACP) using a values-collision approach that describes the tensions or collisions
between various stakeholders' perspectives. Stakeholders included clinicians, designers,
administrators, and patients. They found collisions in the values of the stakeholders
that related to model characteristics, model implementation, and intervention benefits
and harms. The authors propose the values-collision approach as a useful strategy
for using tensions as a source of useful input for the design team to make improvements
with ethical consequences in mind.
Cenci et al., [[25]] used the VSD framework in a citizen science project focused on the design of an
mHealth app for dementia patients that involved location surveillance as a feature.
The investigators used focus groups to elicit values of stakeholders including citizens
with dementia, their family members, clinical staff and volunteers, and leaders of
the local smart city initiative. They describe the use of a procedural-deliberative
method to engage a wide variety of stakeholders in the co-creation of the ultimate
design. Of note, the investigators referred to participants in their study as “citizens”
and not patients.
3.4. Studies identifying trust as a core value
Götzl et al., [[27]] used focus groups, interviews, and a survey to examine the perspectives of key
stakeholders of a mobile mental health app. The investigators documented a variety
of values and related dimensions including acceptability of specific types of data
sharing, perspectives on the role of an app in relation to traditional mental health
providers, and the level of trust in various types of institutions.
Hallowell et al., [[24]] examined a specific domain, trust, in a study that documented the conditions under
which stakeholders felt ML could be trusted in the diagnosis of rare disease. The
authors interviewed geneticists, data scientists, bioinformaticians, industry representatives,
and patient representatives. Participants characterized relational trust between patients
and clinicians as a key element in determining the acceptability of a technology,
and expressed both concerns and enthusiasm about the prospect of commercial involvement
in the process.
Helenason et al., [[30]] engaged primary care physicians in a simulation and interviews that explored feasibility
of AI-based CDS to detect cutaneous melanoma. The physicians expressed concerns about
trusting the technology, and these concerns converged with issues related to the clinical
context, specifically that the providers in this context are responsible for the effective
use of clinical guidelines for a wide variety of clinical issues.
Helman et al., [[31]] engaged various clinical personnel in focus groups in the development of a graphical
user interface (GUI) to display the AI-based risk scores for instability in the intensive
care unit (ICU). Stakeholder values that emerged were trust, the impact of the tool
on practice and decision-making of novice personnel, and weighing of AI outputs during
decision-making.
Fischer et al., [[32]] interviewed Dutch obstetric professionals to gain their perspectives on the use
of AI in obstetric care using three common AI scenarios: diagnosis, workflow optimization/
triage, and personalized treatment. Two key paradoxes emerged: the first was the desire
to know the factors that drive predictive models while acknowledging that models exceed
human capacity in pattern identification, and the second was the desire for the model
to have access to as many parameters as possible for accuracy, while acknowledging
the importance of contextual factors that the model could not capture.
3.5. Studies emphasizing organizational or societal values not addressed above
Kerr et al., [[28]] used a literature review and survey to examine employee concerns about digital
stress management interventions (dSMI), including those with and without ML-based
just-in-time adaptive interventions (JITAI). The literature review identified health
and well-being as a central value, supporting use of dSMI in the workplace. Employees
were concerned about privacy, autonomy, identity, and accountability in relation to
the use of such tools.
Wang et al., [[26]] use Gibson's concept of affordances [[33]] to frame and facilitate a study of features that promote use of a sexual health
chatbot among youth, and to explore actual use of the chatbot. An affordance is a
feature or resource that assists users in appropriate use of an object. The authors'
work resulted in evidence across fifteen affordances they deemed functional (including
new ones that emerged in this study), however several of the affordances reflected
societal values, such as inclusivity and accessibility. The complete list of affordances
included accessibility, multimodality, nonlinearity, compellability, “queriosity”
(encouraging user curiosity), editability, visibility, interactivity, customizability,
trackability, scalability, localizability (enabling linkages between users and services
in their local area), inclusivity, connectivity, and actionability. This study illustrates
how values can be derived using existing frameworks for characterizing human interactions
with technology.
4. Discussion
This narrative review evaluated the recent biomedical literature at the intersection
of applied healthcare AI and VSD. We emphasized applied studies and those with design-focused
research methods, which led to numerous Empirical investigations per the VSD framework.
The literature on design of AI-driven technology largely addressed value identification
across heterogeneous clinical domains. VSD concepts are not common topics in healthcare
AI, so we assessed for elements of the framework regardless of whether the language
of VSD was specifically included in the manuscript. Studies identified were conducted
almost entirely in the United States and Western Europe, leaving significant opportunity
to broaden similar efforts globally. In sum, we identified a small number of heterogeneous
studies emphasizing values relevant to professional or individual practice (see [Figure 2]). While such values are critical to effective healthcare AI, VSD remains understudied
in this highly topical domain of biomedical innovation. As such, we cannot yet recommend
broad uptake of VSD principles into healthcare AI studies but do advocate for more
comprehensive investigations of VSD in future work.
 Figure 2. Classification of values identified in the studies.
Figure 2. Classification of values identified in the studies.
Regarding the specific values identified or explored in the papers, we found that
they largely focused on values relevant to professional or individual practice as
shown in the inner square of [Figure 2]. We found that studies such as Hallowell et al., [[24]], Helanason et al. [[30]], and Kerr et al., [[28]] focused on acceptability or usability of technology and were also positioned methodologically
to identify such practice-based values related to technology. Organizational values
were represented in Kerr et al. [[28]], where employee well-being was the primary driving force for the project. Societal
values were less often elucidated though Wang et al., addressed some in their study of affordances in the context of an educational chatbot.
4.1. Implications for AI development and use in healthcare
AI-driven technology focused on individual or practice level values might implicate
values for organizations or society. While every applied study cannot comprehensively
elucidate and address all possible values, a wider lens on value identification might
identify potential gaps that might widen during or after implementation. This approach
also might lead to more holistic evaluation of AI-driven clinical technology in practice.
For example, clinicians using text generative tools to speed clinical documentation
might note impacts of such technology on their autonomy and need for trust. However,
such tools also might impact the well-being of those working at the organization as
well as broaching concerns around equity depending on how the models were trained,
and whether training corpora were representative of the patient population at that
organization.
Value identification also might reveal value tensions, which arise when multiple human
values that co-exist in a given context come into opposition with one another [[17]]. Per Friedman et al. [[17]], the optimal solution aims to attend to all values intact rather than selecting
one over another. Cagliero et al., [[29]]provided an illustration of value tensions and the resulting effort to address such
tensions. Value tensions can manifest at multiple levels - within individuals attempting
to balance competing values internally, between individuals who prioritize values
differently, and between entire groups who have contradictory perspectives. As use
of AI expands, so will the potential for these tensions and the need for effective
means of resolving them.
4.2. Strengths and limitations
Strengths of this work include a novel focus on the intersection of AI and VSD. We
reviewed recent literature, ensuring the results described are timely and account
at least in part for the emergence in recent years of a focus on human centered design
in informatics [[14]]. We broadened published definitions of VSD based in interpretations by Umbrello
et al., [[22]]. We also reviewed studies for presence of VSD elements regardless of whether the
authors applied VSD directly, as we hypothesized modern HCD would incorporate VSD
concepts given the attention to issues such as trust, autonomy, etc., represented
with variable verbiage as we found here.
Limitations of this study include an emphasis on applied AI-driven technology design
in healthcare, which biased results toward Empirical VSD investigations. The focus
on AI, HCD and VSD, might also have led to relevant studies being excluded from further
review. Our search was limited to PubMed.
5. Conclusions
Elements of VSD have been included in empirical studies of AI-driven technology in
healthcare with clear emphases on values to individual and professional practice,
especially trust. As users gain trust in such technology, system designers might broaden
their design approaches to glean values across organizational and societal dimensions.
This attention might inform more effective tools, more comprehensive evaluation, and
more impactful design.





