
Subscribe to RSS
DOI: 10.1055/s-0044-1800952
Trends of Mortality due to Traumatic Brain Injury in the USA: A Comprehensive Analysis of CDC WONDER Data from 1999 to 2020
Funding None.

Abstract
Traumatic brain injury (TBI) poses a significant public health challenge in the United States, with diverse causes and outcomes. Understanding the trends in TBI-related mortality is crucial for effective prevention and intervention strategies. This comprehensive analysis utilized data from the Centers for Disease Control and Prevention's Wide-ranging Online Data for Epidemiologic Research (CDC WONDER) database, covering the period from 1999 to 2020. Cause-of-death records were examined using the 10th Edition of the International Classification of Diseases and Related Health Problems diagnostic code S06 for TBI-related fatalities. Mortality rates were calculated per 100,000 individuals, adjusted for age and urban/rural status. Joinpoint Regression analysis was employed to identify significant trends over time. Between 1999 and 2020, 1,218,667 TBI-related deaths occurred, with varying mortality rates across demographic groups and geographic regions. Within the overall population, the highest annual average mortality rates were observed in the non-Hispanic (NH) American Indian or Alaska Native cohort, followed by NH white, NH black or African American, Hispanic or Latino, and NH Asian or Pacific Islander groups. Overall, there was an initial decrease in mortality rate from 1999 to 2012, followed by a subsequent significant increase. Males consistently exhibited higher mortality rates than females across all age groups. Disparities were also observed based on race/ethnicity, with NH American Indian or Alaska Native populations showing the highest mortality rates. Regional variations were evident, with the southern region consistently exhibiting the highest mortality rates. Evolving trends in TBI-related mortality in the United States highlight the need for targeted interventions, particularly in high-risk demographic groups and regions.
Keywords
traumatic brain injury - mortality trends - CDC WONDER database - demographic disparities - regional variations.Introduction
Traumatic brain injury (TBI) presents a significant public health challenge in the United States, with an age-standardized mortality rate of 17.71 per 100,000 people reported for 2023.[1] [2] [3] TBI, often characterized as harm to the brain resulting from external mechanical force, encompasses a spectrum of injuries ranging from minor concussions to severe, life-altering trauma.[4] [5] Numerous factors contribute to TBI incidence and mortality, including motor vehicle accidents, falls, sports-related injuries, and assaults. Collectively, these factors contribute to the complex and multifaceted nature of TBI.[6] [7] [8]
The pathogenesis of TBI is multifaceted, involving a cascade of neurochemical, cellular, and inflammatory responses initiated by primary injury.[9] [10] Primary injury mechanisms, such as direct impact or acceleration-deceleration forces, lead to immediate tissue damage and disruption of neuronal integrity.[11] [12] [13] Subsequently, secondary injury processes unfold, encompassing neuroinflammation, oxidative stress, excitotoxicity, and cerebral edema, culminating in neuronal injury and dysfunction.[14] [15] [16]
Despite advancements in medical care and injury prevention strategies, TBI continues to have a significant impact on public health, necessitating ongoing efforts to understand and mitigate this impact.[17] The rationale for our study emerges from this context, that is, to comprehensively analyze the trends of TBI-related mortality in the United States from 1999 to 2020. We aimed to shed light on the dynamics of TBI mortality and its determinants over the past three decades, by utilizing the comprehensive data from the Centers for Disease Control and Prevention (CDC) Wide-ranging Online Data for Epidemiologic Research (WONDER) database. Therefore, this study aimed to examine the fluctuations in mortality rates in the United States related to TBI over time and to investigate the disparities between various demographic groups and geographic regions.
Materials and Methods
Study Setting and Population
The CDC WONDER database was used to analyze TBI-related deaths that occurred between 1999 and 2020. Data on cause-of-death taken from death certificates covering all states and the District of Columbia were analyzed using diagnostic code S06 from the 10th Edition of the International Classification of Diseases and Related Health Problems. The methodology employed in this study has been validated by previous research, particularly in studies concerning cardiovascular disease mortality rates, confirming its reliability and effectiveness. This study identified cases of TBI, whether as the primary cause or a contributing factor, using the Multiple Causes of Death Public Use Registry. As this study employed deidentified public data made available by the government, it was not necessary to obtain formal approval from the regional institutional review board. However, the study adhered to all relevant laws, regulations, and Strengthening the Reporting of Observational Studies in Epidemiology guidelines for observational studies, ensuring adherence to the highest research ethics standards.
Data Extraction Method
The extensive data set provided comprehensive statistics and geographic breakdown, including demographics, year ranges, and comparisons between rural and urban settings. It covers various locations where people might pass away, such as homes, hospitals, nursing homes, and similar establishments. The data set also included demographic information, including race, sex, age, and ethnicity. The racial and ethnic categories used in the study were black or African American, non-Hispanic (NH) white, American Indian, Latino, Pacific Islander, Alaska Native, and Asian NH. Similar to other studies that used the WONDER database, death certificates were the primary data source for the analysis. The population was classified as either urban or rural based on the National Center for Health Statistics Urban-Rural Classification Scheme. Urban areas comprise major metropolitan areas with a population of 1 million or more, as well as smaller metropolitan areas with a population between 50,000 and 999,000. In contrast, according to the 2013 U.S. Census, counties with fewer than 50,000 people are considered to be in rural regions. The Midwest, West, Northeast, and South are divided into four main regions by the U.S. Census Bureau.
Statistical Analysis
Between 1999 and 2020, we calculated mortality rates per 100,000 individuals for both age-adjusted and unadjusted data to examine regional variations in TBI-related deaths across the United States. We provided 95% confidence intervals (CIs) for these rates along with different categories, such as year, sex, urban/rural status, state, and race/ethnicity. To calculate the crude mortality rate for TBI-related deaths, we divided the number of deaths by the total population of the United States annually. Using the Joinpoint Regression Program, we determined the annual percentage change (APC) and its corresponding 95% CI for age-adjusted mortality rates (AAMRs). Our aim was to investigate yearly fluctuations in TBI-related mortality nationwide. To find noteworthy variations in the AAMR across time, this technique uses log-linear regression models. APCs were classified as rising or falling based on the results of a two-tailed t-test, which determined whether the slope representing mortality trends showed a statistically significant departure from zero. The null hypothesis was rejected when the p-value fell below 0.05, indicating statistical significance.
Results
Between 1999 and 2020, a total of 1,218,667 fatalities were linked to head injuries ([Supplementary Table S1], available in the online version). Among these, 559,675 deaths were reported in individuals aged 55 and older ([Supplementary Table S2], available in the online version), while the remaining 658,656 deaths occurred across various age groups, from under 1 year to 54 years old ([Supplementary Table S3], available in the online version).
In all age groups, information about the place of death was available for 1,213,581 cases. Of them, 41.7% occurred in hospitals, 3.37% in assisted living or long-term care facilities, 2.33% in hospice care, and 25.25% occurred at home ([Supplementary Table S4], available in the online version). In particular, statistics on the location of death for 557,738 deaths among individuals 55 years of age and older were recorded; 49.32% of these deaths happened in hospitals, 6.75% in long-term care or nursing homes, 4.78% in hospices, and 26.16% at home ([Supplementary Table S5], available in the online version). Lastly, information on the location of death was available for 655,513 fatalities involving people under the age of 54. Of these, 35.28% occurred in hospitals, 0.50% in long-term care or nursing homes, 0.24% in hospices, and 24.49% at home ([Supplementary Table S6], available in the online version).
Annual Trends in AAMR Associated with Head Injury Across All Ages
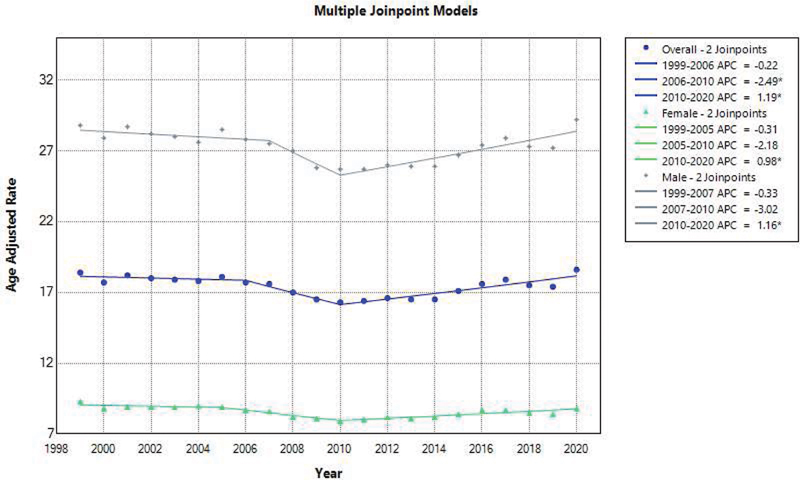
In 1999, the average annual mortality rate (AAMR) for fatalities among all age groups due to head injuries was 18.4 (95% CI: 18.2–18.6). By 2020, this figure had slightly increased to 18.6 (95% CI: 18.4–18.7). Between 1999 and 2012, the AAMR generally declined with an APC of –1.12 (95% CI: –2.44 to –0.22). However, from 2012 to 2020, there was a subsequent rise in AAMR, with an APC of 4.73 (95% CI: 2.99–8.49) ([Fig. 1], [Supplementary Tables S7] and [S8], available in the online version).
Head Injury-Related Annual Trends in AAMR for Individuals Over the Age of 55
For individuals aged 55 and above, the AAMR for fatalities resulting from head injuries was 31.7 (95% CI: 31.3–32.2) up until 2020, where it increased to 38.9 (95% CI: 38.5–39.3). APC of –1.12 (95% CI: –2.44 to –0.22) indicates a general decline in AAMR from 1999 to 2012. This was followed by an increase from 2012 to 2020, with an APC of 4.73 (95% CI: 2.99–8.49) ([Fig. 2], [Supplementary Tables S9] and [S10], available in the online version).

Head Injury-Related Annual Patterns in AAMR for Individuals Under 1 to 54 Years of Age
In 1999, the AAMR for fatalities caused by head injuries in the population aged less than 1 to 54 years was 14.8 (14.6, 14.9). By 2020, this rate had slightly decreased to 13.0 (12.9, 13.2). AAMR indicated a general decline from 1999 to 2012, with an APC of –1.12 (95% CI: –2.44 to –0.22). An increase from 2012 to 2020 with an APC of 4.73 (95% CI: 2.99–8.49) came next ([Fig. 3], [Supplementary Tables S11] and [S12], available in the online version).

Annual Patterns of Head Injury Associated with AAMR, Graded by Gender at All Ages
AAMRs were consistently higher than women in every age group, according to the research. The overall AAMRs for men and women were, respectively, 27.4 (95% CI: 27.3–27.5) and 8.6 (95% CI: 8.6–8.6). The AAMR for males in 1999 was 28.8, with a 95% CI ranging from 28.5 to 29.1, and it dropped to 26.0 (95% CI: 25.8–26.3) in 2012, displaying a decreasing APC of –0.70 (95% CI: –3.51 to 0.46). There was a subsequent increase to 29.2 (95% CI: 28.9–29.5) in 2020, with an APC of 5.05 and a 95% CI ranging from 2.61 to 13.30. In contrast, the AAMR for women of all ages in 1999 was 9.3, with a 95% CI of 9.1 to 9.5. With an APC of –1.78 (–3.50 to –0.82), the AAMR showed a decline from 1999 to 2012. With an APC of 4.09 (2.04–9.43), a more significant rise then occurred until 2020, resulting in an AAMR for females by the end of the study period of 8.8 (95% CI: 8.7–9.0) ([Fig. 1], [Supplementary Tables S7] and [S8], available in the online version).
Annual Trends of Head Injury-Related AAMR, Seen by Gender in Individuals 55 Years of Age and Older
The study conducted on individuals aged 55 and above found that the average AAMR for men of all ages was higher than that of women, with men's overall AAMR at 54.5 (95% CI: 54.3–54.7) and women's overall AAMR at 19.4 (95% CI: 19.3–19.5). The AAMR for men in 1999 was 52.1, with a range of 51.1 to 53.0. By 2012, the AAMR had risen to 54.1 (95% CI: 53.3–54.9), with a slight decreasing trend of –0.70 (95% CI: –3.51 to 0.46). In 2020, there was a substantial increase to 60.6 (95% CI: 59.8–61.4) with an APC of 5.05 (95% CI: 2.61–13.30). Similarly, women aged 55 and above had an AAMR of 17.8 (95% CI: 17.3–18.2) in 1999, which decreased to 15.4 (95% CI: 14.7–16.1) in 2012 with an APC of –1.78 (95% CI: –3.50 to –0.82). However, by 2020, the AAMR had increased significantly to 21.8 (95% CI: 21.4–22.2) with an APC of 4.09 (95% CI: 2.04–9.43). The final AAMR for women was 21.8 (95% CI: 21.4–22.2) ([Fig. 2], [Supplementary Tables S9] and [S10], available in the online version).
Annual Patterns of Head Injury Associated with AAMR, Graded by Gender for Ages 0 to 54 Years
A study on mortality trends for individuals aged between less than 1 year and 54 years found that the AAMRs of males in all age groups were consistently higher than those of females. The overall AAMRs for males were 20.0 (95% CI: 20.0–20.1) and for females, they were 5.6 (95% CI: 5.6–5.7). The AAMR for males in 1999 was 22.4, and it changed to 18.4 (95% CI: 18.2–18.6) in 2012. The APC values showed a slight decreasing trend of –0.70 (95%CI: –3.51 to 0.46). However, there was a significant increase in AAMR to 20.7 (95% CI: 20.4–20.9) in 2020 with an APC of 5.05 (95% CI: 2.61–13.30). Similarly, the AAMR for women aged 54 to less than 1 year in 1999 was 7.0 (95% CI: 6.8–7.2). With an APC of –1.78 (95% CI: –3.50 to –0.82), the AAMR declined from 1999 to 2012. However, with an APC of 4.09 (95% CI: 2.04–9.43), there was a more significant rise until 2020. The AAMR for females by the end of the study period was 5.3 (95% CI: 5.2–5.4) ([Fig. 3], [Supplementary Tables S11] and [S12], available in the online version).
Annual Patterns of Head Injury Associated with AAMR, Graded by Race/Ethnicity for All Ages
Within the overall population, the NH American Indian or Alaska Native cohort exhibited the highest AAMRs, succeeded by the NH white, NH black or African American, Hispanic or Latino, and NH Asian or Pacific Islander groups. The respective AAMR values were as follows: NH American Indian or Alaska Native 26.2 (95% CI: 25.8–26.7), NH white 18.7 (95% CI: 18.7–18.8), NH black or African American 16.8 (95% CI: 16.7–16.9), Hispanic or Latino 12.2 (95% CI: 12.2–12.3), and NH Asian or Pacific Islander 8.7 (95% CI: 8.6–8.8). Notably, a decline in AAMR was observed among NH white individuals between 1999 and 2012, with an APC of –1.02 (95% CI: –2.15 to –0.22), followed by a subsequent increase in mortality trends, with an APC of 4.70 (95% CI: 3.24–7.15) extending to 2020. Conversely, the AAMR for the NH black or African American demographic decreased from 1999 to 2014, showing an APC of –0.48 (95% CI: –9.79 to 1.57), before witnessing a significant increase until 2020, with an APC of 7.80 (95% CI: 2.09–25.05). Likewise, the AAMR for the Hispanic or Latino cohort decreased from 1999 to 2012, registering an APC of –2.13 (95% CI: –15.48 to 0.91), followed by a rise in mortality rates until 2020, with an APC of 3.72 (95% CI: 1.36–14.60). Lastly, the AAMR for the NH Asian or Pacific Islander population demonstrated an increase from 2014 to 2020, with an APC of 2.28 (95% CI: –7.99 to 16.58) ([Fig. 4], [Supplementary Tables S7] and [S13], available in the online version).

Annual Patterns of Head Injury Associated with AAMR, Graded by Race/Ethnicity in Individuals 55 Years of Age and Older
The NH white population exhibited the highest AAMR, trailed by the NH American Indian or Alaska Native, NH Asian or Pacific Islander, Hispanic or Latino, and NH black or African American populations. Their respective AAMR values were as follows: NH white: 37.2 (95% CI: 37.1–37.3), NH American Indian or Alaska Native: 34.0 (95% CI: 32.7–35.3), NH Asian or Pacific Islander: 24.3 (95% CI: 23.9–24.7), Hispanic or Latino: 23.2 (95% CI: 22.9–23.5), and NH black or African American: 21.1 (95% CI: 20.9–21.4). Notably, there was a decline in AAMR among NH white individuals between 1999 and 2012, with an APC of –1.02 (95% CI: –2.15 to –0.22). However, a subsequent rise in mortality trends was observed with an APC of 4.70 (95% CI: 3.24–7.15) through 2020. The AAMR for the NH Asian or Pacific Islander group exhibited an increasing trend from 2014 to 2020, with an APC of 2.28 (95% CI: –7.99 to 16.58). Conversely, the AAMR for Hispanic or Latino populations decreased from 1999 to 2012 with an APC of –2.13 (95% CI: –15.48 to 0.91), followed by a significant increase until 2020 with an APC of 3.72 (95% CI: 1.36–14.60). Lastly, the AAMR for NH black and African American populations decreased from 1999 to 2014 with an APC of –0.48 (95% CI: N9.79 to 1.57), but then increased in mortality until 2020 with an APC of 7.80 (95% CI: 2.09–25.05) ([Fig. 5], [Supplementary Tables S9] and [S14], available in the online version).

Annual Trends in AAMR Correlated with Head Injury and Ages Under 1 to 54 Years, Graded by Race/Ethnicity
The highest AAMR was observed in the NH American Indian or Alaska Native population, followed by the NH black or African American, NH white, Hispanic or Latino, and NH Asian or Pacific Islander groups. The respective AAMR values for each group were as follows: NH American Indian or Alaska Native 24.1 (95% CI: 23.7–24.6), NH black or African American 15.6 (95% CI: 15.5–15.7), NH white 13.7 (95% CI: 13.7–13.7), Hispanic or Latino 9.3 (95% CI: 9.2–9.3), and NH Asian or Pacific Islander 4.5 (95% CI: 4.4–4.5). There was a decline in AAMR for NH black and African American people between 1999 and 2014, with an APC of –0.48 (95% CI: –9.79 to 1.57). Additionally, an increasing mortality trend was observed with an APC of 7.80 (95% CI: 2.09–25.05) through 2020. The AAMR for NH white exhibited a decreasing trend from 1999 to 2012, with an APC of –1.02 (95% CI: –2.15 to –0.22), which then increased from 2012 to 2020, showing an APC of 4.70 (95% CI: 3.24–7.15). The AAMR for Hispanic or Latino populations also revealed a decrease from 1999 to 2012, with an APC of –2.13 (95% CI: –15.48 to 0.91), which exhibited a significant increase until 2020 with an APC of 3.72 (95% CI: 1.36–14.60). Lastly, from 2014 to 2020, the AAMR for the NH Asian or Pacific Islander population showed an increase with APC values ranging from –7.99 to 16.58 ([Fig. 6], [Supplementary Tables S11] and [S15], available in the online version).

Head Injury-Related Annual Trends in AAMR Graded by Geographic Region States in All Ages
The values for AAMR varied considerably across states, ranging from 10.1 (95% CI: 9.9–10.2) in New Jersey and 10.1 (95% CI: 10.0–10.3) in Massachusetts to 33.5 (95% CI: 32.5–34.6) in Wyoming. The differences between the states were evident, with those in the top 90th percentile, including Wyoming and Montana, having AAMRs approximately three times higher than those in the bottom 10th percentile, which included Massachusetts, New Jersey, and New York ([Fig. 7] and [Supplementary Table S16], available in the online version).

Head Injury-Related Annual Trends in AAMR Graded by Geographic Region States in Individuals Aged 55 Years and Above
The average annualized modified risk (AAMR), which ranged between 21.4 (95% CI: 21.0–21.8) in New Jersey and 53.2 (95% CI: 50.5–55.9) in Wyoming, significantly varied across all states. States with AAMRs more than twice as high as those in the bottom 10th percentile, such New Jersey and New York, were those in the top 90th percentile, which included Vermont, Montana, Idaho, and Wyoming ([Fig. 8] and [Supplementary Table S17], available in the online version).

Head Injury-Related Annual Trends in AAMR Graded by Geographic Region States in Ages Less Than 1 to 54 Years
For individuals aged between 1 and 54 years, the AAMR ranged from 6.0 (95% CI: 5.8–6.1) in Massachusetts to 28.2 (95% CI: 27.1–29.3) in Wyoming. States in the top 90th percentile, including Alaska, Mississippi, Montana, South Carolina, and Wyoming, had AAMRs that were almost three times higher than those in the bottom 10th percentile, including Hawaii, Massachusetts, Rhode Island, New Jersey, and New York ([Fig. 9] and [Supplementary Table S18], available in the online version).

Census Region: All Ages
Throughout the study period, the Southern region exhibited the highest mortality rate at 19.9 (95% CI: 19.8–19.9), followed by the Midwestern region at 17.5 (95% CI: 17.5–17.6), the Western region at 17.3 (95% CI: 17.2–17.4), and the Northeastern region at 12.8 (95% CI: 12.8–12.9). In summary, AAMR in the Southern region displayed a decreasing trend from 1999 to 2012, with an APC of –1.83 (95% CI: –3.18 to –0.77). Subsequently, between 2012 and 2020, there was an increase in AAMRs with an APC of 5.78 (95% CI: 4.04–8.75). The AAMR for Midwestern region steadily decreased from 1999 to 2014, with an APC of –1.15 (95% CI: –3.85 to –0.21), followed by an increase with an APC of 4.64 (95% CI: 1.32–14.37) from 2014 to 2020. Similarly, the AAMR for Western region declined from 1999 to 2010, with an APC of –0.98 (95% CI: –4.50 to 0.59), and then increased with an APC of 4.16 (95% CI: 2.73–7.55) from 2010 to 2020. Lastly, the AAMR for Northeastern region showed a slight increase with an APC of 0.98 (95% CI: 0.19–1.87) throughout the study period ([Fig. 10], [Supplementary Table S7] and [S19], available in the online version).

Census Region: Aged 55 Years and Above
Among individuals aged 55 years or older, the Western region recorded the highest mortality rate (36.6, 95% CI: 36.4–36.8), followed by the Southern region (36.4, 95% CI: 36.3–36.6), the Midwestern region (34.7, 95% CI: 34.5–34.9), and the Northeastern region (27.8, 95% CI: 27.6–28.0). To summarize, the AAMR in the Western region exhibited a declining trend from 1999 to 2010, with an APC of –0.98 (95% CI: –4.50 to 0.59). Subsequently, from 2010 to 2020, there was an increase in AAMRs with an APC of 4.16 (95% CI: 2.73–7.55). The AAMR for Southern region decreased from 1999 to 2012, with an APC of –1.83 (95% CI: –3.18 to –0.77), and then displayed a significant increase with an APC of 5.78 (95% CI: 4.04–8.75). Similarly, the AAMR for Midwestern region decreased from 1999 to 2014 with an APC of –1.15 (95% CI: –3.85 to –0.21), followed by an increase with an APC of 4.64 (95% CI: 1.32–14.37) from 2014 to 2020. Lastly, the AAMR for Northeastern region showed a slight increase with an APC of 0.98 (95% CI: 0.19–1.87) from 1999 to 2020 ([Fig. 11], [Supplementary Table S9] and [S20], available in the online version).

Census Region: Ages Less Than 1 to 54 Years
Across all age groups, including individuals less than 1 to 54 years old, the Southern region exhibited the highest mortality rate at 15.4 (95% CI: 15.3–15.4), followed by the Midwestern region at 12.8 (95% CI: 12.8–12.9), the Western region at 12.1 (95% CI: 12.0–12.1), and the Northeastern region at 8.8 (95% CI: 8.7–8.8). To summarize, the age-standardized all-cause mortality rate (AAMR) in the Southern region demonstrated a downward trend from 1999 to 2012, with an APC of –1.83 (95% CI: –3.18 to –0.77). Subsequently, there was a significant increase in AAMRs from 2012 to 2020, with an APC of 5.78 (95% CI: 4.04–8.75). The AAMR in the Midwestern region decreased from 1999 to 2014, with an APC of –1.15 (95% CI: –3.85 to –0.21), before displaying a significant increase with an APC of 4.64 (95% CI: 1.32–14.37). Similarly, the AAMR in the Western region declined from 1999 to 2010, with an APC of –0.98 (95% CI: –4.50 to 0.59), followed by an increase with an APC of 4.16 (95% CI: 2.73–7.55) from 2010 to 2020. Lastly, the AAMR in the Northeastern region showed a slight increase from 1999 to 2020, with an APC of 0.98 (95% CI: 0.19–1.87) ([Fig. 12], [Supplementary Table S11] and [S21], available in the online version).

Urbanization: All Ages
During the study period, nonmetropolitan areas consistently exhibited higher AAMR for head injuries, with an overall AAMR of 24.8 (95% CI: 24.8–24.9), compared with metropolitan areas, which had an AAMR of 16.2 (95% CI: 16.2–16.2). The AAMR in metropolitan areas showed a decrease from 1999 to 2012, with an APC of 0.81 and a 96% CI ranging from –2.22 to 0.11. After that, the AAMR rose to 4.76 with a 95% CI of 3.24 to 7.61 till 2020. The AAMR showed a decline in nonmetropolitan areas between 1999 and 2012, with an APC of –1.65 and a 95% CI spanning from –3.01 to –0.70. Between 2012 and 2020, the mortality trend in nonmetropolitan areas increased significantly, as indicated by an APC of 4.66 (95% CI: 2.96–7.68) ([Fig. 13], [Supplementary Tables S7] and [S22], available in the online version).

Urbanization: Aged 55 Years and Above
In individuals aged 55 years or older, nonmetropolitan areas exhibited higher AAMR values, with an overall AAMR of 41.0 (95% CI: 40.8–41.2), than metropolitan areas, which had AAMRs of 33.0 (95% CI: 32.9–33.1). In nonmetropolitan areas, a declining trend in mortality was observed with an APC of 1.65 and a 95% CI ranging from –3.01 to –0.70 between 1999 and 2012. This trend, however, reversed with an APC of 4.66 (95% CI: 2.96–7.68) from 2012 to 2020. In metropolitan areas, a similar declining trend in mortality was observed with an APC of 0.81 and a 95% CI ranging from –2.22 to 0.11 between 1999 and 2012. However, this trend also showed an increase in mortality with an APC of 4.76 (95% CI: 3.24–7.61) from 2012 to 2020 ([Fig. 14], [Supplementary Table S9] and [S23], available in the online version).

Urbanization: Ages Less Than 1 to 54 Years
In like manner, the nonmetropolitan regions displayed a higher AAMR in relation to head injuries in individuals aged between 1 and 54 years, with a combined AAMR of 20.5 (95% CI: 20.3–20.6), as opposed to the metropolitan areas' AAMRs of 11.6 (95% CI: 11.6–11.7). For APC values, nonmetropolitan regions demonstrated a declining trend from 1999 to 2012, with a rate of 1.65 (95% CI: –3.01 to –0.70). However, this trend began to rise from 2012 to 2020, showing an APC of 4.66 (95% CI: 2.96–7.68). In contrast, metropolitan regions experienced a decrease in mortality rates from 1999 to 2012 with an APC value of –0.81 (95% CI: –2.22 to 0.11). This trend then reversed from 2012 to 2020, with an APC of 4.76 (95% CI: 3.24–7.61) ([Fig. 15], [Supplementary Table S11] and [S24], available in the online version).

Discussion
A thorough and extensive analysis of mortality patterns was performed using data from the CDC between 1999 and 2020. The main objective of this study was to investigate patients with TBI, taking into account factors such as age, sex, ethnicity, and other relevant variables. Early findings indicate a general increase in mortality, with over 1.2 million fatalities recorded. Approximately 50% of fatalities occurred in individuals aged 55 and above, while the remaining occurred in those under 55. Deaths that occurred in medical institutions accounted for nearly 41% of the total, with home deaths accounting for the second-highest proportion at 25%. Notably, the mortality rate decreased with age from 1999 to 2012, before rising sharply between 2012 and 2020. This trend was observed in both age groups, those over 55 and those under 55. Furthermore, the AAMR for males remained higher than that for females throughout the study, emphasizing the greater vulnerability of males to trauma and subsequent death. Regarding mortality trends by race, the Native Hawaiian or Other Pacific Islander population had the highest death and AAMRs, followed by the NH white, NH black or African American, and Hispanic or Latino populations. Additionally, the study delved into other key variables, such as geographic region, census region, and urbanization.
TBI is a severe neurological illness with a global prevalence, often referred to as a hidden epidemic.[18] [19] [20] The increasing trend of TBI in males can be attributed to certain activities in which males engage more frequently than females, such as contact sports like American football, wrestling, hockey, boxing, soccer, lacrosse, and rugby, which increase the risk of concussion.[21] [22] [23] [24] Other contributing factors include falls, assaults, combat, and so on,[25] [26] with diffuse TBI accounting for approximately 80 to 90% of cases.[26] [27] The Glasgow Coma Scale score can be used to clinically define TBI as mild, moderate, or severe, with rates of persistent disability ranging from 10 to 60% and overall mortality rates of 20 to 30%, respectively.[28] [29] [30] The primary harm to the brain is permanent, leading to brain tissue destruction, altered cerebral blood flow regulation, increased inflammatory mediators, oxidative stress, and vasospasm, resulting in cell death and generalized brain edema.[31] [32] The complexity and delicacy of the injury make it impossible to reverse the initial insult, which, combined with the brain's intricate structure and physiology, nearly doubles the mortality rate.[33] The influence of social and environmental factors on the pediatric population after TBI is a crucial discovery,[34] as evidenced by research examining long-term mortality and chronic symptoms in children with TBI.[29] [35]
New studies on adults with mild TBI (mTBI) seeking treatment in emergency rooms have revealed several concerns regarding their care and outcomes. For instance, preinjury factors such as mental health diagnoses, cooccurring medical conditions, and previous TBIs are related to lasting symptoms after mTBI,[36] which can lead to ongoing functional impairments that affect emotional well-being following mTBI.[37] These characteristics can also aggravate other injury-related issues affecting a patient's lifestyle a year after injury. Moreover, they can have an impact on socioeconomic factors, such as employment and insurance, and require follow-up care.[38] It is essential to note that the most common age groups for TBIs are children and the elderly. mTBIs in children can result in long-term behavioral, social, psychological, and academic disorders, whereas in older adults, they are often linked to hospitalization and fatality. In the elderly, they are more frequently associated with cognitive decline, which interferes with daily life. This adverse effect is further compounded by the use of certain medications, such as anticoagulants, which increase the risk of intracranial hemorrhage.[39] [40]
Nevertheless, despite the general increase in TBI mortality trends, we must acknowledge that the population is growing, industries are developing, and medical advancements have prolonged life expectancy. These factors, in addition to various others, may influence the outcomes, although not significantly. To reduce the prevalence, it is essential to establish regulations and raise awareness about measures such as helmet usage, secure sports, and other practices that will ultimately prove to be beneficial in the long term.
Limitations
Despite our best efforts and thorough investigation, our research has been hindered by several confounding variables. To improve the output of our study, we hope to address these issues in future studies. Some of the limitations we encountered include: (1) a lack of clarity regarding the sex, race, and ethnicity causative factors of TBI; (2) an inability to explain the decline and rise in mortality in 2012 in our literature; and (3) the fact that many cases go unreported, which impedes the actualization of data and leaves gaps in the available information.
Conclusion
A comprehensive analysis of TBI-related mortality trends in the United States from 1999 to 2023 revealed dynamic patterns across demographic groups and geographic regions. Despite the initial decline in mortality rates, there has been a subsequent increase, underscoring the persistent public health challenge posed by TBI. Continued surveillance and research are essential for informing evidence-based strategies aimed at preventing TBI and improving outcomes in affected individuals and communities.
Conflict of Interest
None declared.
Authors' Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and have agreed to be held accountable for all aspects of the work.
-
References
- 1 Dams-O'Connor K, Juengst SB, Bogner J. et al. Traumatic brain injury as a chronic disease: insights from the United States Traumatic Brain Injury Model Systems Research Program. Lancet Neurol 2023; 22 (06) 517-528
- 2 Lo J, Chan L, Flynn S. A systematic review of the incidence, prevalence, costs, and activity and work limitations of amputation, osteoarthritis, rheumatoid arthritis, back pain, multiple sclerosis, spinal cord injury, stroke, and traumatic brain injury in the United States: a 2019 update. Arch Phys Med Rehabil 2021; 102 (01) 115-131
- 3 Peterson AB, Kegler SR. Deaths from fall-related traumatic brain injury - United States, 2008-2017. MMWR Morb Mortal Wkly Rep 2020; 69 (09) 225-230
- 4 Brett BL, Gardner RC, Godbout J, Dams-O'Connor K, Keene CD. Traumatic brain injury and risk of neurodegenerative disorder. Biol Psychiatry 2022; 91 (05) 498-507
- 5 Howlett JR, Nelson LD, Stein MB. Mental health consequences of traumatic brain injury. Biol Psychiatry 2022; 91 (05) 413-420
- 6 Posti JP, Cajanus K, Tornio A. et al. Causes of fatal traumatic brain injury in Finland. J Neurosurg 2023; 139 (06) 1506-1513
- 7 Taylor CA, Bell JM, Breiding MJ, Xu L. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths - United States, 2007 and 2013. MMWR Surveill Summ 2017; 66 (09) 1-16
- 8 VanItallie TB. Traumatic brain injury (TBI) in collision sports: possible mechanisms of transformation into chronic traumatic encephalopathy (CTE). Metabolism 2019; 100S: 153943
- 9 Hu J, Wang X, Chen X. et al. Hydroxychloroquine attenuates neuroinflammation following traumatic brain injury by regulating the TLR4/NF-κB signaling pathway. J Neuroinflammation 2022; 19 (01) 71
- 10 Kalra S, Malik R, Singh G. et al. Pathogenesis and management of traumatic brain injury (TBI): role of neuroinflammation and anti-inflammatory drugs. Inflammopharmacology 2022; 30 (04) 1153-1166
- 11 Scarboro M, McQuillan KA. Traumatic brain injury update. AACN Adv Crit Care 2021; 32 (01) 29-50
- 12 Sharma HS, Muresanu DF, Nozari A. et al. Neuroprotective effects of nanowired delivery of cerebrolysin with mesenchymal stem cells and monoclonal antibodies to neuronal nitric oxide synthase in brain pathology following Alzheimer's disease exacerbated by concussive head injury. Adv Neurobiol 2023; 32: 139-192
- 13 Slovis JC, Gupta N, Li NY, Kernie SG, Miles DK. Assessment of recovery following pediatric traumatic brain injury. Pediatr Crit Care Med 2018; 19 (04) 353-360
- 14 Corps KN, Roth TL, McGavern DB. Inflammation and neuroprotection in traumatic brain injury. JAMA Neurol 2015; 72 (03) 355-362
- 15 Sulhan S, Lyon KA, Shapiro LA, Huang JH. Neuroinflammation and blood-brain barrier disruption following traumatic brain injury: pathophysiology and potential therapeutic targets. J Neurosci Res 2020; 98 (01) 19-28
- 16 Thapa K, Khan H, Singh TG, Kaur A. Traumatic brain injury: mechanistic insight on pathophysiology and potential therapeutic targets. J Mol Neurosci 2021; 71 (09) 1725-1742
- 17 Guan B, Anderson DB, Chen L, Feng S, Zhou H. Global, regional and national burden of traumatic brain injury and spinal cord injury, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. BMJ Open 2023; 13 (10) e075049
- 18 Guan L, Tan J, Qi B. et al. The bibliometric and altmetric analysis of chronic traumatic encephalopathy research: how great is the impact?. Front Neurol 2024; 15: 1294125
- 19 Hoffman SW, Harrison C. The interaction between psychological health and traumatic brain injury: a neuroscience perspective. Clin Neuropsychol 2009; 23 (08) 1400-1415
- 20 Wang KK, Yang Z, Zhu T. et al. An update on diagnostic and prognostic biomarkers for traumatic brain injury. Expert Rev Mol Diagn 2018; 18 (02) 165-180
- 21 Aita SL, Muchintala R, Suresh A, Patel S, Schuler B, Lichtenstein JD. Association of use of a mobile tackling dummy during college football practice with reduced sport-related concussion: results of a pilot investigation. Orthop J Sports Med 2024; 12 (02) 23 259671241228316
- 22 McCrea MA, Shah A, Duma S. et al. Opportunities for prevention of concussion and repetitive head impact exposure in college football players: a Concussion Assessment, Research, and Education (CARE) Consortium study. JAMA Neurol 2021; 78 (03) 346-350
- 23 McCrory P, Meeuwisse WH, Aubry M. et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med 2013; 47 (05) 250-258
- 24 Tajima T, Ota O, Nagayama M. et al. Head injury assessment in the Elite Level Rugby Union in Japan: review of 3 seasons. Int J Sports Med 2022; 43 (10) 889-894
- 25 Faul M, Coronado V. Chapter 1 - Epidemiology of traumatic brain injury. In: Grafman J, Salazar AM. eds. Handbook of Clinical Neurology. Elsevier; 2015: 3-13
- 26 Tang CY, Eaves E, Dams-O'Connor K. et al. Diffuse disconnectivity in TBI: a resting state fMRI and DTI study. Transl Neurosci 2012; 3 (01) 9-14
- 27 Blennow K, Brody DL, Kochanek PM. et al. Traumatic brain injuries. Nat Rev Dis Primers 2016; 2 (01) 16084
- 28 Peek-Asa C, Coman MA, Zorn A. et al. Association of traumatic brain injury severity and time to definitive care in three low-middle-income European countries. Inj Prev 2022; 28 (01) 54-60
- 29 Steyerberg EW, Wiegers E, Sewalt C. et al; CENTER-TBI Participants and Investigators. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: a European prospective, multicentre, longitudinal, cohort study. Lancet Neurol 2019; 18 (10) 923-934
- 30 Vella MA, Crandall ML, Patel MB. Acute management of traumatic brain injury. Surg Clin North Am 2017; 97 (05) 1015-1030
- 31 McGinn MJ, Povlishock JT. Pathophysiology of traumatic brain injury. Neurosurg Clin N Am 2016; 27 (04) 397-407
- 32 Yang Y, Lu D, Wang M. et al. Endoplasmic reticulum stress and the unfolded protein response: emerging regulators in progression of traumatic brain injury. Cell Death Dis 2024; 15 (02) 156
- 33 Jeremitsky E, Omert L, Dunham CM, Protetch J, Rodriguez A. Harbingers of poor outcome the day after severe brain injury: hypothermia, hypoxia, and hypoperfusion. J Trauma 2003; 54 (02) 312-319
- 34 Babikian T, Merkley T, Savage RC, Giza CC, Levin H. Chronic aspects of pediatric traumatic brain injury: review of the literature. J Neurotrauma 2015; 32 (23) 1849-1860
- 35 Berry JG, Bloom S, Foley S, Palfrey JS. Health inequity in children and youth with chronic health conditions. Pediatrics 2010; 126 (Suppl. 03) S111-S119
- 36 Haarbauer-Krupa J, Taylor CA, Yue JK. et al. Screening for post-traumatic stress disorder in a civilian emergency department population with traumatic brain injury. J Neurotrauma 2017; 34 (01) 50-58
- 37 Zahniser E, Temkin NR, Machamer J. et al; TRACK-TBI Investigators. The functional status examination in mild traumatic brain injury: a TRACK-TBI sub-study. Arch Clin Neuropsychol 2019; 34 (07) 1165-1174
- 38 Yue JK, Winkler EA, Sharma S. et al; the TRACK-TBI Investigators. Temporal profile of care following mild traumatic brain injury: predictors of hospital admission, follow-up referral and six-month outcome. Brain Inj 2017; 31 (13-14): 1820-1829
- 39 Anderson VA, Catroppa C, Dudgeon P, Morse SA, Haritou F, Rosenfeld JV. Understanding predictors of functional recovery and outcome 30 months following early childhood head injury. Neuropsychology 2006; 20 (01) 42-57
- 40 Nishijima DK, Offerman SR, Ballard DW. et al; Clinical Research in Emergency Services and Treatment (CREST) Network. Immediate and delayed traumatic intracranial hemorrhage in patients with head trauma and preinjury warfarin or clopidogrel use. Ann Emerg Med 2012; 59 (06) 460-8.e1 , 7
Address for correspondence
Publication History
Article published online:
12 December 2024
© 2024. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Dams-O'Connor K, Juengst SB, Bogner J. et al. Traumatic brain injury as a chronic disease: insights from the United States Traumatic Brain Injury Model Systems Research Program. Lancet Neurol 2023; 22 (06) 517-528
- 2 Lo J, Chan L, Flynn S. A systematic review of the incidence, prevalence, costs, and activity and work limitations of amputation, osteoarthritis, rheumatoid arthritis, back pain, multiple sclerosis, spinal cord injury, stroke, and traumatic brain injury in the United States: a 2019 update. Arch Phys Med Rehabil 2021; 102 (01) 115-131
- 3 Peterson AB, Kegler SR. Deaths from fall-related traumatic brain injury - United States, 2008-2017. MMWR Morb Mortal Wkly Rep 2020; 69 (09) 225-230
- 4 Brett BL, Gardner RC, Godbout J, Dams-O'Connor K, Keene CD. Traumatic brain injury and risk of neurodegenerative disorder. Biol Psychiatry 2022; 91 (05) 498-507
- 5 Howlett JR, Nelson LD, Stein MB. Mental health consequences of traumatic brain injury. Biol Psychiatry 2022; 91 (05) 413-420
- 6 Posti JP, Cajanus K, Tornio A. et al. Causes of fatal traumatic brain injury in Finland. J Neurosurg 2023; 139 (06) 1506-1513
- 7 Taylor CA, Bell JM, Breiding MJ, Xu L. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths - United States, 2007 and 2013. MMWR Surveill Summ 2017; 66 (09) 1-16
- 8 VanItallie TB. Traumatic brain injury (TBI) in collision sports: possible mechanisms of transformation into chronic traumatic encephalopathy (CTE). Metabolism 2019; 100S: 153943
- 9 Hu J, Wang X, Chen X. et al. Hydroxychloroquine attenuates neuroinflammation following traumatic brain injury by regulating the TLR4/NF-κB signaling pathway. J Neuroinflammation 2022; 19 (01) 71
- 10 Kalra S, Malik R, Singh G. et al. Pathogenesis and management of traumatic brain injury (TBI): role of neuroinflammation and anti-inflammatory drugs. Inflammopharmacology 2022; 30 (04) 1153-1166
- 11 Scarboro M, McQuillan KA. Traumatic brain injury update. AACN Adv Crit Care 2021; 32 (01) 29-50
- 12 Sharma HS, Muresanu DF, Nozari A. et al. Neuroprotective effects of nanowired delivery of cerebrolysin with mesenchymal stem cells and monoclonal antibodies to neuronal nitric oxide synthase in brain pathology following Alzheimer's disease exacerbated by concussive head injury. Adv Neurobiol 2023; 32: 139-192
- 13 Slovis JC, Gupta N, Li NY, Kernie SG, Miles DK. Assessment of recovery following pediatric traumatic brain injury. Pediatr Crit Care Med 2018; 19 (04) 353-360
- 14 Corps KN, Roth TL, McGavern DB. Inflammation and neuroprotection in traumatic brain injury. JAMA Neurol 2015; 72 (03) 355-362
- 15 Sulhan S, Lyon KA, Shapiro LA, Huang JH. Neuroinflammation and blood-brain barrier disruption following traumatic brain injury: pathophysiology and potential therapeutic targets. J Neurosci Res 2020; 98 (01) 19-28
- 16 Thapa K, Khan H, Singh TG, Kaur A. Traumatic brain injury: mechanistic insight on pathophysiology and potential therapeutic targets. J Mol Neurosci 2021; 71 (09) 1725-1742
- 17 Guan B, Anderson DB, Chen L, Feng S, Zhou H. Global, regional and national burden of traumatic brain injury and spinal cord injury, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. BMJ Open 2023; 13 (10) e075049
- 18 Guan L, Tan J, Qi B. et al. The bibliometric and altmetric analysis of chronic traumatic encephalopathy research: how great is the impact?. Front Neurol 2024; 15: 1294125
- 19 Hoffman SW, Harrison C. The interaction between psychological health and traumatic brain injury: a neuroscience perspective. Clin Neuropsychol 2009; 23 (08) 1400-1415
- 20 Wang KK, Yang Z, Zhu T. et al. An update on diagnostic and prognostic biomarkers for traumatic brain injury. Expert Rev Mol Diagn 2018; 18 (02) 165-180
- 21 Aita SL, Muchintala R, Suresh A, Patel S, Schuler B, Lichtenstein JD. Association of use of a mobile tackling dummy during college football practice with reduced sport-related concussion: results of a pilot investigation. Orthop J Sports Med 2024; 12 (02) 23 259671241228316
- 22 McCrea MA, Shah A, Duma S. et al. Opportunities for prevention of concussion and repetitive head impact exposure in college football players: a Concussion Assessment, Research, and Education (CARE) Consortium study. JAMA Neurol 2021; 78 (03) 346-350
- 23 McCrory P, Meeuwisse WH, Aubry M. et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med 2013; 47 (05) 250-258
- 24 Tajima T, Ota O, Nagayama M. et al. Head injury assessment in the Elite Level Rugby Union in Japan: review of 3 seasons. Int J Sports Med 2022; 43 (10) 889-894
- 25 Faul M, Coronado V. Chapter 1 - Epidemiology of traumatic brain injury. In: Grafman J, Salazar AM. eds. Handbook of Clinical Neurology. Elsevier; 2015: 3-13
- 26 Tang CY, Eaves E, Dams-O'Connor K. et al. Diffuse disconnectivity in TBI: a resting state fMRI and DTI study. Transl Neurosci 2012; 3 (01) 9-14
- 27 Blennow K, Brody DL, Kochanek PM. et al. Traumatic brain injuries. Nat Rev Dis Primers 2016; 2 (01) 16084
- 28 Peek-Asa C, Coman MA, Zorn A. et al. Association of traumatic brain injury severity and time to definitive care in three low-middle-income European countries. Inj Prev 2022; 28 (01) 54-60
- 29 Steyerberg EW, Wiegers E, Sewalt C. et al; CENTER-TBI Participants and Investigators. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: a European prospective, multicentre, longitudinal, cohort study. Lancet Neurol 2019; 18 (10) 923-934
- 30 Vella MA, Crandall ML, Patel MB. Acute management of traumatic brain injury. Surg Clin North Am 2017; 97 (05) 1015-1030
- 31 McGinn MJ, Povlishock JT. Pathophysiology of traumatic brain injury. Neurosurg Clin N Am 2016; 27 (04) 397-407
- 32 Yang Y, Lu D, Wang M. et al. Endoplasmic reticulum stress and the unfolded protein response: emerging regulators in progression of traumatic brain injury. Cell Death Dis 2024; 15 (02) 156
- 33 Jeremitsky E, Omert L, Dunham CM, Protetch J, Rodriguez A. Harbingers of poor outcome the day after severe brain injury: hypothermia, hypoxia, and hypoperfusion. J Trauma 2003; 54 (02) 312-319
- 34 Babikian T, Merkley T, Savage RC, Giza CC, Levin H. Chronic aspects of pediatric traumatic brain injury: review of the literature. J Neurotrauma 2015; 32 (23) 1849-1860
- 35 Berry JG, Bloom S, Foley S, Palfrey JS. Health inequity in children and youth with chronic health conditions. Pediatrics 2010; 126 (Suppl. 03) S111-S119
- 36 Haarbauer-Krupa J, Taylor CA, Yue JK. et al. Screening for post-traumatic stress disorder in a civilian emergency department population with traumatic brain injury. J Neurotrauma 2017; 34 (01) 50-58
- 37 Zahniser E, Temkin NR, Machamer J. et al; TRACK-TBI Investigators. The functional status examination in mild traumatic brain injury: a TRACK-TBI sub-study. Arch Clin Neuropsychol 2019; 34 (07) 1165-1174
- 38 Yue JK, Winkler EA, Sharma S. et al; the TRACK-TBI Investigators. Temporal profile of care following mild traumatic brain injury: predictors of hospital admission, follow-up referral and six-month outcome. Brain Inj 2017; 31 (13-14): 1820-1829
- 39 Anderson VA, Catroppa C, Dudgeon P, Morse SA, Haritou F, Rosenfeld JV. Understanding predictors of functional recovery and outcome 30 months following early childhood head injury. Neuropsychology 2006; 20 (01) 42-57
- 40 Nishijima DK, Offerman SR, Ballard DW. et al; Clinical Research in Emergency Services and Treatment (CREST) Network. Immediate and delayed traumatic intracranial hemorrhage in patients with head trauma and preinjury warfarin or clopidogrel use. Ann Emerg Med 2012; 59 (06) 460-8.e1 , 7