
Subscribe to RSS
DOI: 10.1055/s-0044-1801259
Comparative Results in Bilateral Carpal Tunnel Surgery in 1 and 2 Stages
Article in several languages: español | English
Abstract
Introduction Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy, with 3-5% and 50-70% being bilateral. It is believed that intervening simultaneously in 1 stage is associated with greater discomfort than in 2 stages and is associated with high costs for both the patient and the health systems.
Hypothesis Bilateral carpal tunnel surgical treatment in 1 stage is well tolerated, with similar postoperative evolution time and lower cost.
Methods Retrospective cohort study. Review of bilateral CTS files operated in 1 and 2 stages in 1 center, by the same team, between 2019-2022, follow-up 2 and 41 months. Interthenar open surgical technique.
It evaluated: absenteeism, Quick Dash, satisfaction, and costs. It considered the average income in Chile published by the National Institute of Statistics (INE) 2020 for the valuation of lost workdays (LWD). For the valuation of the cost of intervention, a quote for both surgical modalities were requested from the medical center in June 2022. For cost analysis, the conversion of Chilean pesos to dollars was carried out.
An Excel spreadsheet was used to compare the means of the 2 groups for the different parameters recorded with a significance level P of 0.05.
Results Of 538 surgeries performed at the medical center in the period analyzed, 118 were found to meet inclusion and exclusion criteria:
Group A: bilateral intervention in 1 stage. 26 patients, corresponding to 52 interventions. Average age 49.
Group B: bilateral intervention in 2 stages. 33 patients, corresponding to 66 patients. Average age 49.
Quick DASH group A v/s B average 1.74 v/s 3.23 p value 0.47. LWD 32.88 v/s 84.84; P value 0.00014. Satisfaction 88% vs. 91%, p 0.69. Surgical expense incurred was 4979.37 US v/s 5274.63 US
Considering the LWD difference was US 1503.26
Conclusion Surgical result is comparable without major discomfort. There was a significant difference in lost workdays and costs, favoring intervention in 1 stage.
Level of evidence III
#
Introduction
Carpal tunnel syndrome (CTS) corresponds to the most reported peripheral entrapment neuropathy, corresponding to 2.7%.[1] 50-70%[2] of patients present symptoms bilaterally. Women are 3 times more affected than men. Obesity, diabetes mellitus, thyroid disorders, rheumatoid arthritis, previous wrist fractures, and pregnancy are well-established risk factors. The symptoms observed correspond to paresthesias, hypoesthesia, and pain, especially at night. If conservative treatment fails, surgical release is performed through retinaculotomy.
Surgical treatment is associated with high financial costs for both the patient and the health systems to which they belong, lost workdays, discomfort, and inability to use the hand presented by patients operated on for bilateral carpal tunnel syndrome in both 1 and 2 stages.
It is believed by hand surgeons that the simultaneous intervention of both extremities at one stage entails greater discomfort and disability for activities of daily living than those operated on in 2 stages.[1] [2] [3]
A study carried out by Weber et al.[1] evaluated costs, recovery, and days, lost recommending release in 1 stage.
We propose that 1-stage surgical treatment can be well tolerated,[4] with a similar postoperative evolution time and lower financial cost[3] [5] [7] [8] than 2-stage surgery.
#
Methods
Retrospective cohort study
The clinical records were reviewed to obtain epidemiological data from patients who underwent surgery for bilateral CTS, performed in 1 or 2 stages at a single center by the same surgical team between January 2019 and May 2022. No work compensation was involved. Phone numbers were obtained, along with information on days of work leave and/or absence from regular activities for those who were retired; a subsequent telephone survey was conducted.
Inclusion criteria: Patients with bilateral CTS operated on at the same center by the same surgical team between January 1, 2019, and May 30, 2022, who could be reached by phone during July 2022 and explicitly agreed to participate in the study.
Exclusion criteria: Patients with recurrent carpal tunnel, not reachable by telephone or who refused to participate in the study, and those who did not complete the surveys or follow-up.
The patients were distributed into different groups according to their personal preference for surgical treatment in 1 or 2 stages:
-
Group A: surgical intervention of both hands in 1 stage.
-
Group B: surgical intervention of both hands in 2 stages.
The surgical technique involved a mini-open release of the retinaculum, 1.5–2 cm in length, performed in the interthenar crease.[9] The hand was subsequently covered with a soft dressing. One-week post-intervention, dressing changes were performed, replacing it with a small dressing, and patients were encouraged to mobilize their hands for light activities. The sutures were removed 14 days post-surgery. No follow-up physiotherapy sessions or complications were recorded.
The study evaluated days of absenteeism from work and/or absence from usual activities in retired individuals based on clinical records, the Quick DASH,[7] and the degree of user satisfaction through a telephone survey conducted in May 2022 for all patients included in the study. The time between surgery and the survey ranged from 2 to 41 months. Costs associated with the surgical intervention were assessed through a formal quote provided by the institution in June 2022 for 1 and 2-stage outpatient carpal tunnel surgery. ([Attachment]) The valuation of the LWD was calculated using the average income in Chile for the year 2020, published by the National Institute of Statistics (INE),[9] which corresponds to 635,134 Chilean pesos. For cost analysis, Chilean pesos were converted to US dollars.
For data analysis, an Excel spreadsheet was used, and a Student's t-test was applied to compare the means of the two groups across different parameters, with a significance level set at P ≤ 0.05.
#
#
Results
Of a total of 538 surgeries performed at the medical center by the surgical team between January 1, 2019, and May 30, 2022, 94 patients who corresponded to those operated on for bilateral carpal tunnel were analyzed, of which 59 met the inclusion and exclusion criteria participated, corresponding to 118 surgeries performed, distributed as follows:
Group A: Included 26 patients, with 19 females and 7 males. The age range was 24 to 71 years, with an average of 49 years. The average Quick DASH score was 1.74 (range 0–22.72) ([Chart 1]). The average number of lost workdays was 32.88 days (range 14–60) ([Chart 2]). Regarding satisfaction after the surgical intervention, 88.4% (23 patients) reported being fully satisfied, and 11.6% (3 patients) were moderately satisfied ([Chart 3]). When asked if they would recommend undergoing surgery on both hands in a single stage, 88.4% (23 patients) responded favorably, and 11.6% (3 patients) said "maybe." If they needed surgery again, 96.15% (25 patients) would do it, and the same percentage agreed that the surgery improved their quality of life. The cost of the surgical intervention was $4,979.37 ([Chart 4]), with an additional $765 incurred per lost workday ([Table 1]), resulting in a total cost (surgery plus LWD) of $5,744.37.



|
No |
Age Years |
Quick DASH |
LWD[*] |
Satisfaction |
Surgical costs US |
LWD expenditure US |
Total expenditure Surgery+ LWD US |
|
|---|---|---|---|---|---|---|---|---|
|
Group A Surgery in 1 stage |
26 |
24-71 X 49 |
2.27-22.72 (X 1.7) |
14-60 (X 32.88) |
88.4% |
4979.37 |
765 |
5744.37 |
|
Group B 2 stage surgery |
33 |
14-60 X 49 |
2.27-50 (X 3.23) |
28-196 (84.84) |
91% |
5274.63 |
1973 |
7247.63 |
Grupo B: Included 33 patients, with 20 females and 13 males. The age range was 33 to 71 years, with an average of 49 years. The average Quick DASH score was 3.23 (range 0–50) ([Chart 1]). The average number of lost workdays was 84.84 days (range 28–196) ([Chart 2]). Regarding satisfaction after the surgical intervention, 91% (30 patients) reported being fully satisfied, and 9% (3 patients) were moderately satisfied ([Chart 3]). When asked if they would recommend undergoing surgery in two stages, 100% of patients responded affirmatively. If they needed surgery again, 94% (31 patients) would do it, and 97% (32 patients) agreed that the surgery improved their quality of life. The cost of the surgical intervention was $5,274.63 ([Chart 4]) with an additional $1,973 incurred per lost workdays ([Table 1]), resulting in a total cost (surgery plus LWD) of $7,247.63.
#
Discussion
There were no significant differences in the Quick DASH result with a p-value of 0.47 between both groups, which suggests that the final result of surgical intervention was the same for both groups; although there is a time bias between the performance of surgery and the completion of the telephone survey with a period between 2 and 41 months, the dispersion being similar for both groups.
The evaluation of recommendations to other people to undergo surgery in 1 or 2 stages does not have a statistically significant difference with a p-value of 0.083.
In relation to the degree of satisfaction after surgery, there is no significant difference with a p-value of 0.69 for this variable ([Chart 3]).
When asked if this surgery improved their quality of life, there is no significant evidence between both groups with a p value of 0.86; and if the procedure was performed again, there was no difference between both groups with a p value of 0.69.
In relation to the lost workdays due to surgeries in Group A vs Group B, the result is statistically significant with a p-value of 0.00014, which confirms our hypothesis that having surgery in 1 stage significantly reduces the number of lost workdays ([Chart 2]), this could be explained with the fact that when the patient has one hand operated on, he waits for at least a period of time in which he remains at rest and then the second limb is operated on, adding this rest time to the previous one, a situation that occurs simultaneously in the case of both limbs being operated on in a single surgical procedure.
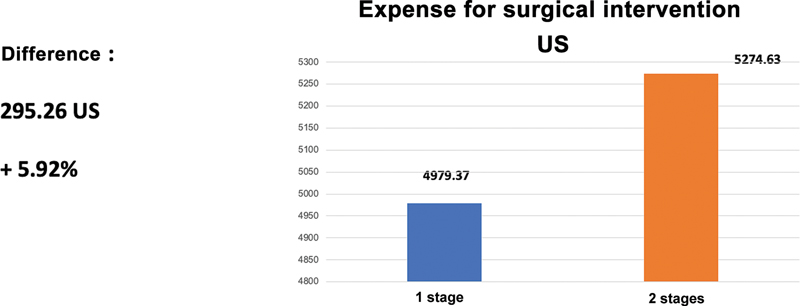
The economic savings in relation to the expense incurred for surgery is lower, corresponding to US 295.26 ([Chart 4]), but when considering the lost workdays ([Chart 5]) plus the difference in the cost of the surgical intervention, this amount rises to US1,503 .26, which corresponds to a difference of 26.17% in favor of intervention in 1 stage ([Chart 6])


#
Conclusion
This study shows that the final outcomes of surgical intervention for carpal tunnel syndrome, whether performed in 1 or 2 stages, are comparable in terms of Quick DASH scores, without significant differences in postoperative discomfort, as indicated by the patients' evaluations of the final results. However, there is a statistically significant difference in the number of lost workdays following surgical interventions, which translates into higher economic costs for the patient's insurance system in 2 stage surgeries. Based on this analysis, the authors recommend performing bilateral CTS surgery in one stage, as it does not present significant disadvantages for patients. It is important to acknowledge that the main limitation of this study is the retrospective collection of cases, a relatively small number of participants, and the administration of the DASH questionnaire long after the surgery in some instances. Future challenges include conducting a prospective study to analyze potential complications associated with one- and two-stage surgeries, as well as considering the type of work performed by the patient.
#
#
Conflicto de interés
Autores no declaran apoyo económico ni conflicto de interés en este estudio.
-
Bibliografía
- 1 Weber RA, Boyer KM. Consecutive versus simultaneous bilateral carpal tunnel release. Ann Plast Surg 2005; 54 (01) 15-19
- 2 Osei DA, Calfee RP, Stepan JG, Boyer MI, Goldfarb CA, Gelberman RH. Simultaneous Bilateral or Unilateral Carpal Tunnel Release? A Prospective Cohort Study of Early Outcomes and Limitations. J Bone Joint Surg Am 2014; 96 (11) 889-896
- 3 Park KW, Boyer MI, Gelberman RH, Calfee RP, Stepan JG, Osei DA. Simultaneous Bilateral Versus Staged Bilateral Carpal Tunnel Release: A Cost-effectiveness Analysis. J Am Acad Orthop Surg 2016; 24 (11) 796-804
- 4 Wang AA, Hutchinson DT, Vanderhooft JE. Bilateral simultaneous open carpal tunnel release: a prospective study of postoperative activities of daily living and patient satisfaction. J Hand Surg Am 2003; 28 (05) 845-848
- 5 Elfar JC, Foad MB, Foad SL, Stern PJ. A cost analysis of staged and simultaneous bilateral carpal tunnel release. Hand (N Y) 2012; 7 (03) 327-332
- 6 Chamorro C, Alvares D, Berger S, Balocci F, Rodríguez X, Soza F. Propiedades Psicométricas de la versión chilena del cuestionario Quick Disabilities of the Arm, Shoulder and Hand en pacientes con patología de hombro. Arch Med Deporte 2020; 37 (05) 305-309
- 7 Gummesson C, Ward MM, Atroshi I. The shortened disabilities of the arm, shoulder and hand questionnaire (QuickDASH): validity and reliability based on responses within the full-length DASH. BMC Musculoskelet Disord 2006; 18 (07) 44
- 8 Pace V, Marzano F, Placella G. Update on surgical procedures for carpal tunnel syndrome: What is the current evidence and practice? What are the future research directions?. World J Orthop 2023; 18; 14 (01) 6-12
- 9 Instituto Nacional de Estadisticas de Chile. https://www.ine.gob.cl/
Address for correspondence
Publication History
Received: 03 April 2023
Accepted: 26 November 2024
Article published online:
26 December 2024
© 2024. Sociedad Chilena de Ortopedia y Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Bibliografía
- 1 Weber RA, Boyer KM. Consecutive versus simultaneous bilateral carpal tunnel release. Ann Plast Surg 2005; 54 (01) 15-19
- 2 Osei DA, Calfee RP, Stepan JG, Boyer MI, Goldfarb CA, Gelberman RH. Simultaneous Bilateral or Unilateral Carpal Tunnel Release? A Prospective Cohort Study of Early Outcomes and Limitations. J Bone Joint Surg Am 2014; 96 (11) 889-896
- 3 Park KW, Boyer MI, Gelberman RH, Calfee RP, Stepan JG, Osei DA. Simultaneous Bilateral Versus Staged Bilateral Carpal Tunnel Release: A Cost-effectiveness Analysis. J Am Acad Orthop Surg 2016; 24 (11) 796-804
- 4 Wang AA, Hutchinson DT, Vanderhooft JE. Bilateral simultaneous open carpal tunnel release: a prospective study of postoperative activities of daily living and patient satisfaction. J Hand Surg Am 2003; 28 (05) 845-848
- 5 Elfar JC, Foad MB, Foad SL, Stern PJ. A cost analysis of staged and simultaneous bilateral carpal tunnel release. Hand (N Y) 2012; 7 (03) 327-332
- 6 Chamorro C, Alvares D, Berger S, Balocci F, Rodríguez X, Soza F. Propiedades Psicométricas de la versión chilena del cuestionario Quick Disabilities of the Arm, Shoulder and Hand en pacientes con patología de hombro. Arch Med Deporte 2020; 37 (05) 305-309
- 7 Gummesson C, Ward MM, Atroshi I. The shortened disabilities of the arm, shoulder and hand questionnaire (QuickDASH): validity and reliability based on responses within the full-length DASH. BMC Musculoskelet Disord 2006; 18 (07) 44
- 8 Pace V, Marzano F, Placella G. Update on surgical procedures for carpal tunnel syndrome: What is the current evidence and practice? What are the future research directions?. World J Orthop 2023; 18; 14 (01) 6-12
- 9 Instituto Nacional de Estadisticas de Chile. https://www.ine.gob.cl/





