

Subscribe to RSS
DOI: 10.1055/s-0045-1802626
Comparative Analysis of Postoperative Radiotherapy Dose Escalation in Oral Cavity Cancer Patients with Positive Margins: A Propensity Score-Matched Study
Authors

Abstract
Introduction
This study aimed to determine the impact of postoperative (PO) radiotherapy (RT) dose escalation in oral cavity squamous cell carcinoma (OCSCC) patients with positive margin (PM) in terms of local control (LC), duration of RT interruption, and toxicity in a tertiary care center.
Materials and Methods
Patients with OCSCC who were candidates for adjuvant RT were categorized into PM and negative margin (NM) arms depending on the margin status as per the histopathology report retrospectively. PM and NM patients received a total dose of 66 Gy to the site of the PM and 60 Gy for the NM. LC, acute and chronic toxicities, and duration of RT interruption were evaluated.
Results
A total of 56 patients were included in the study, of whom 39 had NM and 17 had PM. After propensity score matching, 11 patients were matched in each arm. The mean duration of RT treatment in the PM and NM arms were 49.5 days (standard deviation [SD] = 5.4) and 50.7 days (SD = 10.15) (p = 0.3), with mean interruptions of 3.9 days (SD = 3.9) and 3.8 days (SD = 6.2), respectively (p = 0.39). LC was 72.7% in the PM arm and 81.8% in the NM arm (p = 0.6). Acute and chronic toxicities were comparable between the two arms.
Conclusion
Dose escalation to 66 Gy for PM during adjuvant RT for PO OCSCC can be used as an alternative strategy to reresection, especially in patients who have poor performance status, who have negative consent for surgery, and who have more than one adverse prognostic factor with comparable LC and toxicity as in the NM. However, further prospective studies are needed to establish its role as an alternative, which is highly unlikely in modern oncology practice, as PM patients are rarely seen in clinics currently with good surgical oncology practices.
Keywords
oral cavity squamous cell carcinoma - radiotherapy - positive margin - negative margin - postoperativeIntroduction
Surgical resection is the treatment of choice for oral cavity squamous cell carcinoma (OCSCC), especially for early disease, which is limited to the oral cavity and has good visibility upon oral inspection. Adjuvant radiotherapy (RT) and adjuvant concurrent chemoradiotherapy (CCRT) are used for specific conditions in patients with locally advanced tumors.[1] There are various surgical approaches available for the resection of a primary tumor of the oral cavity—the peroral approach for early-stage cancer and mandibulotomy, the lower cheek flap approach, and the visor flap approach for locally advanced lesions.[2] Although the ultimate aim of every surgery is to provide an R0 margin, at difficult subsites, especially in the retromolar region, lesions situated posteriorly in the anterior two-thirds of the tongue as well as posteriorly situated hard palate lesions are more prone to getting close or positive margin (PM), especially in T2/T3 disease. Resection can be R2, in which gross disease is left after surgery; R1, in which microscopic disease is present; or R0, in which no disease is found at the resection border (or no ink on the tumor).[3]
Although the importance of negative surgical margins cannot be overemphasized, some patients may succumb to PM. The National Comprehensive Cancer Network (NCCN) defines a clear margin as an invasive tumor that is at least 5 mm from the resected margin, a close margin as <5 mm, and a PM as an invasive tumor present at the margin of resection.[4]
PM is a problem in developing countries due to a lack of trained oncologists and frozen sections, difficult anatomy, and locally advanced disease presentation at clinics. PM has been reported in up to 21% of oral cancer resections, and studies have shown that PM is associated with an increased risk of disease recurrence and compromised long-term outcomes in OCSCC.[5]
Postoperative (PO) CCRT is the treatment of choice for OCSCC patients with PM or lymph node metastases with extracapsular extension.[6] [7] The optimal PO dose for improving local control (LC) in resected OCSCC is yet to be determined. Fletcher recommended a radiation dose of 60 Gy.[8] Radiation Therapy Oncology Group (RTOG) trials allowed for an additional boost of 6 Gy in patients with high-risk features such as PM and extranodal extension.[9] [10] Dose escalation in the case of PM remains a perplexing problem in terms of its benefit in LC, overall survival, and acceptable toxicity, as per the available evidence. The guidelines recommend the use of dose escalation according to the clinician's discretion and the patient's condition.
This study aimed to determine the impact of postoperative radiotherapy (PORT) dose escalation in OCSCC patients with PM in terms of LC, duration of RT interruption, and toxicity in a tertiary care center.
Materials and Methods
This was a cross-sectional observational study conducted at the All India Institute of Medical Sciences, Bhopal, between January 2020 and January 2023. The inclusion criteria were PO patients with OCSCC who were candidates for adjuvant RT or adjuvant CCRT irrespective of margin status. For this study, patients were categorized into PM and negative margin (NM) depending on the margin status as per the histopathology report. Additional high-risk pathological risk factors were not taken into account for the study purpose.
Treatment Procedure
All patients were simulated in the supine position by using a head and neck thermoplastic cast as an immobilization device with a computed tomography (CT) scan and a slice thickness of 2.5 mm. The planning CT was coregistered with preoperative imaging, CT or magnetic resonance imaging (MRI), and gross tumor volume-primary (GTV-P) and gross tumor volume-nodal (GTV-N) were delineated and adapted based on anatomical changes following surgery excluding air and uninvolved bone. Clinical target volume-primary (CTV-P) and clinical target volume-nodal (CTV-N) were created by giving 10-mm margins to the GTV-P and GTV-N; these were edited for anatomical barriers, such as bone, fascia, and air; and all PO changes were included in the contour. CTV-N also included areas at high risk of harboring microscopic diseases depending on the site, stage, and extent of disease. The elective CTV 2 was also delineated and included at-risk uninvolved nodal levels according to the site, laterality of the primary tumor, and extent of neck dissection. The planning target volume (PTV) 1 and PTV 2 were delineated by giving 5-mm margins (CTV-P and CTV-N) to CTV 1 and CTV 2, respectively.[11]
All patients with PM were scheduled to receive PO CCRT at a dose of 60 Gy (2 Gy/fraction) to PTV 1 with an additional 6 Gy to the PM site and 54 Gy at 1.8 Gy/fraction to PTV 2 with concurrent weekly cisplatin of 40 mg/m2 and with NM received PORT to a dose of 60 Gy (at 2 Gy/fraction) to PTV 1 and 54 Gy to PTV 2 with concurrent weekly cisplatin, based on high-risk pathological features defined by European Organization for Research and Treatment of Cancer (EORTC) trial extranodal extension (ENE), nodal tumor at levels 4 and 5, perineural disease, or vascular tumor emboli.[7] All patients were planned with volumetric modulated arc therapy with simultaneous integrated boost or intensity-modulated RT in the ELEKTA treatment planning system.
Data collected for all patients included the time of initiation of RT from the date of surgery, duration of RT treatment, duration of interruption of RT, disease status at last follow-up, and acute and chronic toxicities.
Follow-up
Regular follow-up was performed at 1, 3, and 6 months postcompletion of treatment and every 6 months thereafter. Tumor response assessment was performed at 3 months postcompletion of RT with CT/MRI, thereafter patients were assessed yearly consecutively for 3 years. The Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1 was used to assess tumor response.[12] LC was defined as stable disease, partial response, or complete response based on RECIST 1.1 criteria at 1 year postcompletion of RT. Acute and chronic radiation toxicities were assessed using the RTOG/EORTC criteria during and after 1 and 6 months of completion of RT.[13]
Statistical Analysis
Propensity score calculations were used to compare PM patients with NM to address potential bias due to confounding variables: age, sex, Eastern Cooperative Oncology Group performance status, site, and stage. The logistic regression model estimated the propensity score for each individual in the study, providing a numerical value reflecting the likelihood of receiving the treatment. Once the propensity scores were obtained, matched samples were determined using nearest-neighbor matching. Continuous data are presented as the mean ± standard deviation (SD), and regression analysis was performed for the time of RT initiation after surgery, duration of RT, and interruption duration as the dependent variables and covariate variables (age, sex, site, and stage) as the independent variables against the PM arm. Categorical variables are presented as N (%), and the chi-square test was used to compare the LC and toxicity between the two arms.
Results
A total of 56 patients were included in the study; 43 (76.8%) were men, and 13 (23.2%) were women. Four (7%) patients had stage I disease, 12 (21.4%) had stage II disease, and 20 (35.7%) had stage III or stage IV disease. Out of 56 patients, 39 patients had NM, while 17 patients had PM. All but one patient received concurrent cisplatin in both arms with a median of 4 and 5 cycles in the PM and NM arms, respectively. One patient could not receive concurrent cisplatin due to deranged serum creatinine. The median follow-up duration was 14 months. The clinical characteristics of the patients are given in [Table 1].
Abbreviations: ECOG PS, Eastern Cooperative Oncology Group Performance Status; NM, negative margin; PM, positive margin.
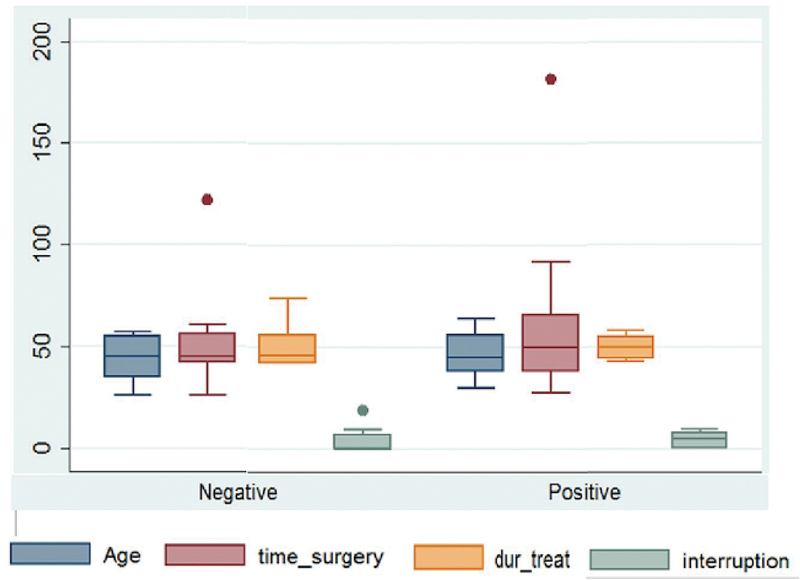
After propensity score-matched analysis, 11 patients in each arm were matched. The mean age in the PM and NM arms were 47.4 years (SD = 11.1) and 44.8 years (SD = 10.8), respectively. The mean interval to RT initiation after surgery in the PM and NM arms were 61.5 days (SD = 43.5) and 51.5 days (SD = 25.7), respectively (p = 0.3). The mean durations of RT in the PM and NM arms were 49.5 days (SD = 5.4) and 50.7 days (SD = 10.15) (p = 0.3), with mean interruptions of 3.9 days (SD = 3.9) and 3.8 days (SD = 6.2), respectively (p = 0.39) ([Fig. 1]).
LC was 72.7% in the PM arm and 81.8% in the NM arm, while 3 (27.27%) patients in the PM arm and 2 (18.18%) patients in the NM arm experienced local recurrence (p = 0.6). There were also no significant differences in acute or chronic toxicities, such as mucositis (p = 0.3), dermatitis (p = 0.2), dysphagia (p = 0.1), xerostomia (p = 0.3), and trismus (p = 0.6), between the two arms. The regression analysis showed that the PM does not independently predict delays in RT initiation, treatment duration, or interruption, F(5,16) = 1.22, R2 = 0.27, p = 0.34. Covariate analysis suggests sex (β= 0.34, p = 0.211), age (β = 0.013, p = 0.24), site (β= −0.05, p = 0.82), and stage (β= −0.17, p = 0.2) do not significantly impact the dependent variables. However, the positive coefficient of sex and age suggests a trend where one gender or increased age may have a longer time-related outcome, but a larger sample size is required to confirm this.
Discussion
Adjuvant RT is the standard of care for PO OCSCC patients with adverse pathological features such as pT3-T4, more than two neck nodes, close margins <5 mm, lymphovascular and perineural invasion, and the worst pattern of invasion -5.[14] Although surgical resection of OCSCC with an adequate surgical margin of at least 5 mm is desirable, some patients will have PM due to many factors, such as inaccessible sites, difficult anatomical information, lack of experience with oncological procedures, very advanced disease status, and postneoadjuvant chemotherapy status. Re-excision with an adequate margin is desirable and recommended, but this approach is not always possible, especially in locally advanced cases. Revising the margin-positive site is associated with many challenges, such as difficulty in finding the remaining tumor in deep margins, difficulty in revisiting the site with the reconstructive flap in situ, and difficulty when adjacent tissues are contracted and distorted. Another factor is the delay in the initiation of PO adjuvant treatment by a second resection, which is associated with compromised locoregional control of the disease.[15] Though NCCN recommends initiation of PORT within 42 days after surgery in head and neck squamous cell carcinoma (HNSCC), our study had a delay of around 10 and 20 days in NM and PM patients due to late referral, PO wound complications such as prolonged wound healing and infections, and waiting list on the treatment machine.[16] The delay in starting PORT happens worldwide despite the physician's best effort. National Cancer Database reported delays in 62% of patients due to lower education, increased PO length of stay, negative surgical margins, and oral cavity sites.[17] Another study by Graboyes et al found more than 50% of patients received delayed PORT.[18] This delay in RT initiation has been associated with a decrease in LC of ∼0.09 to 0.17% for each additional day between surgery and PORT.[19]
Various studies have suggested escalated doses in PM patients. Studies by Cooper et al and Bernier et al have shown that PO CCRT with an RT dose of 60 to 66 Gy in patients with PM and lymph node metastasis with extracapsular extension significantly improves locoregional control and disease-free survival.[6] [7] However, the appropriate RT dose for patients with PM is still a matter of debate. Marcus et al recommended a PORT dose of 65 Gy using 1.7 to 1.8 Gy/fraction; however, for the oral cavity and oropharynx, 70 Gy was recommended, particularly when the margins were positive.[20] A study from the MD Anderson Cancer Center suggested a minimum tumor dose of 57.6 Gy for the whole operative bed with a boost of 63 Gy to areas of increased risk. Dose escalation more than 63 Gy did not improve the therapeutic efficacy.[21]
However, there are limited studies with variable results that have evaluated the benefit of PORT dose escalation in patients with PM. Schiff et al found that treatment delay > 6 weeks did not have a negative impact on locoregional control when the dose of > 60 Gy was delivered postoperatively, indicating the benefit of escalated dose in HNSCC.[22] Avkshtol et al did a retrospective study and found no survival benefit with dose escalation > 60 Gy in PO HNSCC patients with ENE or PM.[23] We retrospectively analyzed the impact of PORT dose escalation of ≥ 66 Gy in OCSCC with PM by propensity score matching with NM patients. We found no statistically significant differences between the two arms in terms of LC rate, treatment interruption days, or acute or chronic toxicities despite dose escalation. This might suggest that an increased dose to the PM site plays a beneficial role in achieving an LC rate with acceptable toxicities comparable to NM patients.
This finding suggested that dose escalation in patients with PM could be a suitable alternative to reresection, as it allows for early initiation of adjuvant treatment, which is associated with improved local and regional control and complements the challenges faced during resurgery. The comprehensive analysis of LC rates, treatment interruption days, and acute and chronic toxicities in our study provide clinicians with valuable information for decision-making. The favorable outcomes observed in terms of LC and toxicity profiles suggest that dose escalation to 66 Gy in PM patients can be a clinically relevant strategy.
While our study sheds light on the benefits of dose escalation in PORT for PM, it is essential to acknowledge certain limitations. The retrospective nature of the analysis introduces inherent biases, and the relatively small sample size may impact the generalizability of our findings. Additionally, the rarity of PM cases in modern clinics poses challenges in conducting large-scale prospective studies. Despite these limitations, our work contributes valuable insights into the potential role of RT in managing PM in OCSCC.
Conclusion
In conclusion, our study contributes to the evolving landscape of managing PM in OCSCC. This highlights the potential of dose escalation in adjuvant RT as a practical alternative to reresection in certain clinical scenarios. By providing evidence of comparable outcomes with those of NM patients, our work supports the consideration of this approach, especially in resource-limited settings where reresection may pose additional challenges, and 66 Gy for a positive microscopic surgical margin (R1) during adjuvant RT for PO patients can be used as a suitable alternative to reresection in OCSCC patients with comparable LC and toxicity as in NM patients. Furthermore, collaborative efforts and prospective studies are warranted to validate and refine this alternative strategy, ensuring its applicability and effectiveness in diverse clinical contexts.
Conflict of Interest
None declared.
Ethical Approval
The study was performed after obtaining approval from the Institutional Review Board (IM22039) and as per the Declaration of Helsinki guidelines.
Authors' Contribution
R.S. and R.P. collected the data and prepared the Excel sheet. R.S. performed the literature review and prepared the draft manuscript. R.P. presented the idea, guided the work, checked the data, and edited the final manuscript for its scientific content. All the other authors read and approved the final manuscript.
-
References
- 1 Montero PH, Patel SG. Cancer of the oral cavity. Surg Oncol Clin N Am 2015; 24 (03) 491-508
- 2 Shah JP. Surgical approaches to the oral cavity primary and neck. Int J Radiat Oncol Biol Phys 2007; 69 (02) S15-S18
- 3 Hermanek P, Wittekind C. The pathologist and the residual tumor (R) classification. Pathol Res Pract 1994; 190 (02) 115-123
- 4 Thomas Robbins K, Triantafyllou A, Suárez C. et al. Surgical margins in head and neck cancer: intra- and postoperative considerations. Auris Nasus Larynx 2019; 46 (01) 10-17
- 5 Luryi AL, Chen MM, Mehra S, Roman SA, Sosa JA, Judson BL. Positive surgical margins in early stage oral cavity cancer: an analysis of 20,602 cases. Otolaryngol Head Neck Surg 2014; 151 (06) 984-990
- 6 Cooper JS, Pajak TF, Forastiere AA. et al; Radiation Therapy Oncology Group 9501/Intergroup. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 2004; 350 (19) 1937-1944
- 7 Bernier J, Domenge C, Ozsahin M. et al; European Organization for Research and Treatment of Cancer Trial 22931. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004; 350 (19) 1945-1952
- 8 Textbook of Radiotherapy | Radiology [Internet]. . [cited December 10, 2024]. Available at: https://pubs.rsna.org/doi/10.1148/88.2.380
- 9 Cooper JS, Zhang Q, Pajak TF. et al. Long-term follow-up of the RTOG 9501/intergroup phase III trial: postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head and neck. Int J Radiat Oncol Biol Phys 2012; 84 (05) 1198-1205
- 10 Rosenthal DI, Mohamed ASR, Garden AS. et al. Final report of a prospective randomized trial to evaluate the dose-response relationship for postoperative radiation therapy and pathologic risk groups in patients with head and neck cancer. Int J Radiat Oncol Biol Phys 2017; 98 (05) 1002-1011
- 11 Evans M, Beasley M. Target delineation for postoperative treatment of head and neck cancer. Oral Oncol 2018; 86: 288-295
- 12 Eisenhauer EA, Therasse P, Bogaerts J. et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45 (02) 228-247
- 13 Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys 1995; 31 (05) 1341-1346
- 14 Loganadane G, Kann BH, Park HS. et al. Clinical outcomes of head and neck cancer patients who undergo resection, but forgo adjuvant therapy. Anticancer Res 2019; 39 (09) 4885-4890
- 15 Gokavarapu S, Rao LMC, Mahajan M, Parvataneni N, Raju KVVN, Chander R. Revision of margins under frozen section in oral cancer: a retrospective study of involved margins in pT1 and pT2 oral cancers. Br J Oral Maxillofac Surg 2015; 53 (09) 875-879
- 16 Pfister DG, Spencer S, Adelstein D. et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2020; 18 (07) 873-898
- 17 Lorenz FJ, Mahase SS, Miccio J, King TS, Pradhan S, Goyal N. Update on adherence to guidelines for time to initiation of postoperative radiation for head and neck squamous cell carcinoma. Head Neck 2023; 45 (07) 1676-1691
- 18 Graboyes EM, Garrett-Mayer E, Sharma AK, Lentsch EJ, Day TA. Adherence to National Comprehensive Cancer Network guidelines for time to initiation of postoperative radiation therapy for patients with head and neck cancer. Cancer 2017; 123 (14) 2651-2660
- 19 Graboyes EM, Kompelli AR, Neskey DM. et al. Association of treatment delays with survival for patients with head and neck cancer: a systematic review. JAMA Otolaryngol Head Neck Surg 2019; 145 (02) 166-177
- 20 Marcus Jr RB, Million RR, Cassissi NJ. Postoperative irradiation for squamous cell carcinomas of the head and neck: analysis of time-dose factors related to control above the clavicles. Int J Radiat Oncol Biol Phys 1979; 5 (11-12): 1943-1949
- 21 Peters LJ, Goepfert H, Ang KK. et al. Evaluation of the dose for postoperative radiation therapy of head and neck cancer: first report of a prospective randomized trial. Int J Radiat Oncol Biol Phys 1993; 26 (01) 3-11
- 22 Schiff PB, Harrison LB, Strong EW. et al. Impact of the time interval between surgery and postoperative radiation therapy on locoregional control in advanced head and neck cancer. J Surg Oncol 1990; 43 (04) 203-208
- 23 Avkshtol V, Handorf EA, Ridge JA. et al. Examining adjuvant radiation dose in head and neck squamous cell carcinoma. Head Neck 2019; 41 (07) 2133-2142
Address for correspondence
Publication History
Received: 11 December 2024
Accepted: 08 January 2025
Article published online:
04 February 2025
© 2025. MedIntel Services Pvt Ltd. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Montero PH, Patel SG. Cancer of the oral cavity. Surg Oncol Clin N Am 2015; 24 (03) 491-508
- 2 Shah JP. Surgical approaches to the oral cavity primary and neck. Int J Radiat Oncol Biol Phys 2007; 69 (02) S15-S18
- 3 Hermanek P, Wittekind C. The pathologist and the residual tumor (R) classification. Pathol Res Pract 1994; 190 (02) 115-123
- 4 Thomas Robbins K, Triantafyllou A, Suárez C. et al. Surgical margins in head and neck cancer: intra- and postoperative considerations. Auris Nasus Larynx 2019; 46 (01) 10-17
- 5 Luryi AL, Chen MM, Mehra S, Roman SA, Sosa JA, Judson BL. Positive surgical margins in early stage oral cavity cancer: an analysis of 20,602 cases. Otolaryngol Head Neck Surg 2014; 151 (06) 984-990
- 6 Cooper JS, Pajak TF, Forastiere AA. et al; Radiation Therapy Oncology Group 9501/Intergroup. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 2004; 350 (19) 1937-1944
- 7 Bernier J, Domenge C, Ozsahin M. et al; European Organization for Research and Treatment of Cancer Trial 22931. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004; 350 (19) 1945-1952
- 8 Textbook of Radiotherapy | Radiology [Internet]. . [cited December 10, 2024]. Available at: https://pubs.rsna.org/doi/10.1148/88.2.380
- 9 Cooper JS, Zhang Q, Pajak TF. et al. Long-term follow-up of the RTOG 9501/intergroup phase III trial: postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head and neck. Int J Radiat Oncol Biol Phys 2012; 84 (05) 1198-1205
- 10 Rosenthal DI, Mohamed ASR, Garden AS. et al. Final report of a prospective randomized trial to evaluate the dose-response relationship for postoperative radiation therapy and pathologic risk groups in patients with head and neck cancer. Int J Radiat Oncol Biol Phys 2017; 98 (05) 1002-1011
- 11 Evans M, Beasley M. Target delineation for postoperative treatment of head and neck cancer. Oral Oncol 2018; 86: 288-295
- 12 Eisenhauer EA, Therasse P, Bogaerts J. et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45 (02) 228-247
- 13 Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys 1995; 31 (05) 1341-1346
- 14 Loganadane G, Kann BH, Park HS. et al. Clinical outcomes of head and neck cancer patients who undergo resection, but forgo adjuvant therapy. Anticancer Res 2019; 39 (09) 4885-4890
- 15 Gokavarapu S, Rao LMC, Mahajan M, Parvataneni N, Raju KVVN, Chander R. Revision of margins under frozen section in oral cancer: a retrospective study of involved margins in pT1 and pT2 oral cancers. Br J Oral Maxillofac Surg 2015; 53 (09) 875-879
- 16 Pfister DG, Spencer S, Adelstein D. et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2020; 18 (07) 873-898
- 17 Lorenz FJ, Mahase SS, Miccio J, King TS, Pradhan S, Goyal N. Update on adherence to guidelines for time to initiation of postoperative radiation for head and neck squamous cell carcinoma. Head Neck 2023; 45 (07) 1676-1691
- 18 Graboyes EM, Garrett-Mayer E, Sharma AK, Lentsch EJ, Day TA. Adherence to National Comprehensive Cancer Network guidelines for time to initiation of postoperative radiation therapy for patients with head and neck cancer. Cancer 2017; 123 (14) 2651-2660
- 19 Graboyes EM, Kompelli AR, Neskey DM. et al. Association of treatment delays with survival for patients with head and neck cancer: a systematic review. JAMA Otolaryngol Head Neck Surg 2019; 145 (02) 166-177
- 20 Marcus Jr RB, Million RR, Cassissi NJ. Postoperative irradiation for squamous cell carcinomas of the head and neck: analysis of time-dose factors related to control above the clavicles. Int J Radiat Oncol Biol Phys 1979; 5 (11-12): 1943-1949
- 21 Peters LJ, Goepfert H, Ang KK. et al. Evaluation of the dose for postoperative radiation therapy of head and neck cancer: first report of a prospective randomized trial. Int J Radiat Oncol Biol Phys 1993; 26 (01) 3-11
- 22 Schiff PB, Harrison LB, Strong EW. et al. Impact of the time interval between surgery and postoperative radiation therapy on locoregional control in advanced head and neck cancer. J Surg Oncol 1990; 43 (04) 203-208
- 23 Avkshtol V, Handorf EA, Ridge JA. et al. Examining adjuvant radiation dose in head and neck squamous cell carcinoma. Head Neck 2019; 41 (07) 2133-2142
