

Subscribe to RSS
DOI: 10.1055/s-0045-1805083
A Rare Case of Gallbladder Tuberculosis Masquerading as Chronic Calculous Cholecystitis
Authors
Funding None.

Abstract
Gallbladder being an uncommon site of tuberculosis, we are presenting a case of tubercular cholecystitis in a 61-year-old female who presented with pain abdomen and was operated for cholelithiasis. The diagnosis was clinched on histopathological examination. She was treated accordingly and has responded well for antitubercular therapy.
This case is unique as the patient had no symptoms of gastrointestinal or pulmonary tuberculosis. It was only after histopathological examination, the diagnosis was reached.
Introduction
Isolated tuberculosis (TB) of the gallbladder (GB) is extremely rare due to its intrinsic resistance to tuberculous infections. GB is one of the uncommon sites of involvement by TB. It might present either with features of chronic cholecystitis, cholelithiasis, or as malignancy.[1] Because GB TB is so uncommon and has nonspecific symptoms, it can be difficult to diagnose preoperatively.[2] Various studies have documented variable manifestations of GB. However, they do not help in providing a precise diagnostic clue.[2] There are different symptoms that people with GB TB infection can experience, including weight loss, vomiting, jaundice, and abdominal discomfort, the right hypochondrium pain. However, gallstones also present with similar symptoms and are also present in approximately 70% of GB TB cases.[3] Due to these reasons, histology is confirmatory, and preoperative predictions of GB TB are neither specific nor verified.[4] It is believed, infection travels to GB from a local focus and travel through the bloodstream or lymphatics.[5] It is challenging to accurately diagnose GB TB before surgery. Consequently, it is critical to differentiate this condition from other GB disorders.[3]
Case Report
A 61-year-old female presented with pain abdomen, feeling of bloating, and indigestion with occasional episode of vomiting. The symptoms were noted vaguely since 6 months and aggravated 2 weeks before they decided to consult at hospital.
Upon taking detailed history, the lady was a homemaker and belonged to low socioeconomic status. Past medical history was unremarkable and no significant findings were observed. The past surgical history revealed minor procedures like dental interventions and gynecological procedures during child birth. No other surgical history was present in the patient. No clinical symptoms of TB like cough, weight loss, or altered bowel habits was noted in the patient.
On examination, some tenderness in the right hypochondrium was noted. No other significant findings were noted. Body mass index was not evaluated for this patient.
Laboratory investigations revealed mild microcytic hypochromic anemia with hemoglobin of 10.5 g/dL. Differential was within normal range. Liver function test showed reversal of A:G ratio (albumin 3.5, globulin 4.35), indicating possibility of some chronic inflammatory process. Erythrocyte sedimentation rate was 30 mm/hour.
X-ray chest, as seen in [Fig. 1A], was unremarkable with no significant findings.
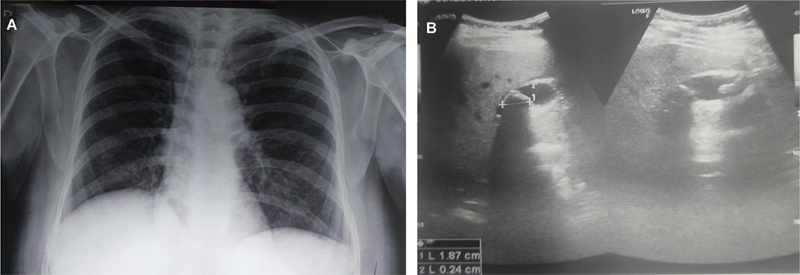
The ultrasonography of the patient was performed, which showed multiple calculi in the GB with increased wall thickness (about 1 cm) and normal common bile duct. There was evidence of cholecystitis and cholelithiasis. An image of the ultrasound can be seen in [Fig. 1B].
Computed tomography (CT) was not done in this case, due to no suspicion of malignancy and poor socioeconomic status of the patient.
Intraoperatively, very dense intraperitoneal adhesions were present between the abdominal wall and omentum, and pericholecystic adhesions between the GB, omentum, stomach, and duodenum. No peritoneal tubercles were present over the GB or other intra-abdominal organs. Ascites was not present. Laparoscopic cholecystectomy with adhesionolysis was performed and the GB specimen was sent to the laboratory for histopathological examination. The operative time was around 2 hours with most of the time being taken in adhesionolysis. The blood loss during surgery was at normal expected levels as per such cases. Postoperative hospital stay was approximately 3 days and no postoperative complications were noted. Patient was discharged in satisfactory state.
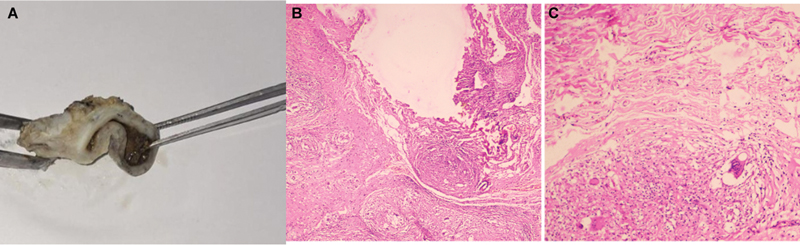
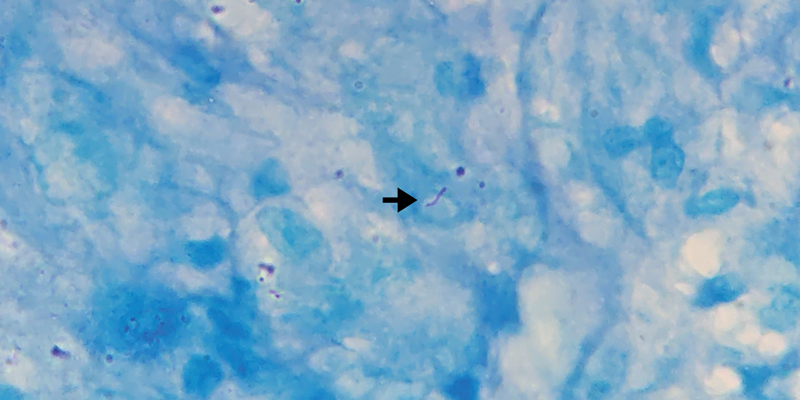
[Fig. 2A] shows gross appearance of the specimen received. Grossly, the GB measured 5 × 3 × 2 cm. Mucosa was mostly ulcerated with few small whitish lesions in the wall of the GB. Wall thickness ranged between 0.6 and 0.8 cm. Multiple stones were present in the lumen. [Fig. 2B] and [C] shows the microphographs of the sections. Microscopy showed denuded lining epithelium. There was abundant fibrosis and multiple coalescing epithelioid cell granulomas having central caseous necrosis. These granulomata exhibited lymphoid cuffing. Langhans-type giant cells were present. Ziehl–Neelsen stain was performed for acid-fast bacilli (AFB), which showed magenta pink beaded bacilli. [Fig. 3] shows microphotograph of the AFB stain done in this case.
After histopathological diagnosis, patient was called back and explained the diagnosis and put on antituberculosis therapy (ATT). The patient was put on ATT for 6 months. After 6 months' course, the patient is asymptomatic till date.
Discussion
D-Mycobacterium tuberculosis is the causative agent of TB. It is a difficult-to-treat pathogen with high worldwide prevalence. It is believed that it latently infects approximately one-quarter of the world's population.[6] Since Robert Koch's discovery of the disease in 1882, the TB epidemic appears to be spreading throughout the world and presently TB is one of the leading causes of death globally and a highly contagious airborne disease. Extrapulmonary (EP) TB is a type of TB that can spread to other parts of the body, even though the disease usually affects the lungs.[6] The majority of these cases of TB occur in middle- and low-income countries.[7] In immunocompetent hosts, EPTB causes approximately 15% of TB cases.[7]
About 1% of cases of abdominal TB are caused by hepatobiliary TB.[1] GB TB is very rare worldwide, with only few cases reported in the literature.[5] The GB's thick walls and naturally alkaline bile make it resistant to TB infection.[6] Bile's inherent essential nature prevents Mycobacterium tuberculosis from growing.[6] However, GB TB is predisposed by GB mucosal injury and low bile acid concentration that can be caused by cystic duct obstruction.[1] The bacillus may reach GB by serosal spread from a peritoneal lesion, by canalicular dissemination or by hematogenous or lymphatic route from nearby positive focus.[1] In our case, tubercular infection was most likely spread from focus in chest. Additionally, approximately two-thirds of patients with GB TB have been documented to have cholelithiasis, which serves as a nidus for the development of TB.[1] In our case also, gallstones were present. GT primarily affects women over 30 years of age.[3] Our case was also above 30 years age (61 years old).
The pathognomonic presentation of GB TB is not well-defined. Clinical symptoms can range from GB perforation to an unexpected histological examination.[5] Patients with GT infection may present with a combination of symptoms, such as weight loss, vomiting, jaundice, and abdominal pain, which can be mistakenly diagnosed as cholecystitis, biliary obstruction, or even carcinomas.[8] Right hypochondriac pain and abdominal mass may also be found.[8] Our case presented with nonspecific symptoms like pain abdomen and vomiting, which could also be attributed to gallstones. There were no symptoms of abdominal TB or systemic involvement of any other organ by TB was seen, indicating the unusual clinical presentation.
There are four different ways that GB TB can present clinically: (1) as a component of miliary TB, (2) as a component of disseminated abdominal TB, (3) as an isolated form of TB that is frequently discovered by chance during microscopic examination of a resected GB, and (4) as a component of an immunocompromised state like uremia, cancer, or acquired immunodeficiency syndrome.[4] We believe our case was due to dissemination of abdominal TB, which was retrospectively concluded by the surgeon due to unexpected extensive peritoneal adhesions and after histopathological report, despite the patient not having any other clinical symptoms of abdominal TB.
The ultrasound examination usually shows nonspecific or wall thickness with stones inside.[6] In our case, the GB wall was thickened with presence of gallstones. Three different kinds of CT findings can help in GB TB diagnosis, according to Xu et al.[12] First type is micronodular type in which there is polypoid or micronodular lesion that exhibits a uniformly enhanced GB wall on a contrast-enhanced CT scan. Second, thickened wall GB TB is the most prevalent variety and is often misinterpreted as GB cancer or cholecystitis. However, in GB TB, the wall is diffuse, homogeneous, and thicker with edema or “halo.” Third kind is the mass-forming type, which shows flecked calcification of GB wall.[4] Our case did not get CT scan performed due to lack of suspicion of any other condition and due to economic reasons.
Due to the lack of specific symptoms and diagnostic testing, the clinical presentation of GB TB is ambiguous and the diagnosis is frequently delayed. A histological study is required to provide a definitive diagnosis.[9] Langhans giant cells and caseous granulomas are characteristic histological findings of GB TB.[6] The AFB can be detected in about 60% of cases.[6] In our case too, presence of granulomas and AFB were detected. Histopathologically, the existence of AFB and caseous granulomas are the gold standard for TB diagnosis.[6] In our case too, the diagnosis was made after histopathological examination and successful treatment was administered due to correct pathological diagnosis. The patient responded well to the treatment and is presently symptom free.
GB TB remains a diagnostic challenge as clinical presentation mimics other GB diseases such as cholecystitis and imaging features may mimic GB carcinoma. GB TB, a rare entity, is difficult to differentiate from other GB diseases such as GB xanthogranulomatous cholecystitis.[10]
As far as management is concerned, treatment protocols for pulmonary and extrapulmonary diseases are identical.[11] Drug-sensitive Mycobacterium tuberculosis strains are treated using a 6-month protocol that consists of four different medications. This must be strictly followed to prevent resistance and recurrence.[7]
Conclusion
GB TB is a rare manifestation of abdominal TB. As there is lack of precise diagnostic tests, preoperative diagnosis is usually not achievable. Our case report also highlights vague and overlapping clinical and radiological features, hence histopathological diagnosis becomes paramount for this infection in endemic areas. Thus, an increased awareness and a high index of suspicion are necessary in endemic areas, especially if there are any unusual surgical findings like peritoneal adhesions.
Conflict of Interest
None declared.
Acknowledgments
None.
Authors' Contributions
P.H.N. and A.N. contributed to the diagnosis and manuscript preparation. A.A.K. and P.K.G. performed the surgery and participated in manuscript preparation. N.G.U. was responsible for the radiological diagnosis and manuscript preparation.
Ethical Statement
Not needed.
Data Availability Statement
There is no data associated with this work.
Consent to Participate and Publication
Standard consent taken from patient.
-
References
- 1 Varshney B, Elhence P, Soni S, Varshney VK, Yadav T, Saha S. Gallbladder tuberculosis presenting as obstructive jaundice. ACG Case Rep J 2020; 7 (06) e00414
- 2 Wolde TG, Jiang K, Miao Y, Wei J. Gallbladder tuberculosis in a dialysis patient: a case-report. BMC Surg 2020; 20 (01) 67
- 3 Liu Y, Wang K, Liu H. Gallbladder tuberculosis mimicking gallbladder carcinoma: a case report and literature review. Case Reports Hepatol 2016; 2016: 3629708
- 4 Chan KS, Shelat VG, Tan CH, Tang YL, Junnarkar SP. Isolated gallbladder tuberculosis mimicking acute cholecystitis: a case report. World J Gastrointest Surg 2020; 12 (03) 123-128
- 5 Verma SK, Mishra AK, Jaiswal AK. Tuberculosis of gallbladder neck: a cause of cholecystitis with cholelithiasis. BMJ Case Rep 2013; 2013: bcr2012008007
- 6 Nugroho NP, Kusmiati T, Santoso S. Gallbladder tuberculosis mimicking cholecystitis: a case report. J Clin Med Kaz 2021; 2 (08) 72-74
- 7 Alsayed SSR, Gunosewoyo H. Tuberculosis: pathogenesis, current treatment regimens and new drug targets. Int J Mol Sci 2023; 24 (06) 5202
- 8 Tarmohamed M, Mremi A, Mkwizu E, Paschal J, Sadiq A, Msuya D. Isolated gallbladder tuberculosis in an 84-year old man: a rare case report. Int J Surg Case Rep 2021; 87: 106471
- 9 Soni S, Sreesanth KS, Varshney V, Swami A. Gall bladder tuberculosis: review of literature. Indian J Tuberc 2022; 69 (04) 421-426
- 10 Jagtap SV, Kulkarni SR, Saini S. et al. Xanthogranulomatous cholecystitis: an uncommon variant. Int J Healthc Biomed Res 2015; 3: 47-50
- 11 Treatment of Tuberculosis. Guidelines. In: Treatment of Extrapulmonary TB and of TB in Special Situations. 4th ed.. Geneva: World Health Organization; 2010: 8
- 12 Xu XF, Yu RS, Qiu LL. et al. Gallbladder tuberculosis: CT findings with histopathologic correlation. Korean J Radiol 2011; Mar-Apr; 12 (02) 196-202
Address for correspondence
Publication History
Received: 16 October 2024
Accepted: 02 February 2025
Article published online:
24 March 2025
© 2025. Gastroinstestinal Infection Society of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Varshney B, Elhence P, Soni S, Varshney VK, Yadav T, Saha S. Gallbladder tuberculosis presenting as obstructive jaundice. ACG Case Rep J 2020; 7 (06) e00414
- 2 Wolde TG, Jiang K, Miao Y, Wei J. Gallbladder tuberculosis in a dialysis patient: a case-report. BMC Surg 2020; 20 (01) 67
- 3 Liu Y, Wang K, Liu H. Gallbladder tuberculosis mimicking gallbladder carcinoma: a case report and literature review. Case Reports Hepatol 2016; 2016: 3629708
- 4 Chan KS, Shelat VG, Tan CH, Tang YL, Junnarkar SP. Isolated gallbladder tuberculosis mimicking acute cholecystitis: a case report. World J Gastrointest Surg 2020; 12 (03) 123-128
- 5 Verma SK, Mishra AK, Jaiswal AK. Tuberculosis of gallbladder neck: a cause of cholecystitis with cholelithiasis. BMJ Case Rep 2013; 2013: bcr2012008007
- 6 Nugroho NP, Kusmiati T, Santoso S. Gallbladder tuberculosis mimicking cholecystitis: a case report. J Clin Med Kaz 2021; 2 (08) 72-74
- 7 Alsayed SSR, Gunosewoyo H. Tuberculosis: pathogenesis, current treatment regimens and new drug targets. Int J Mol Sci 2023; 24 (06) 5202
- 8 Tarmohamed M, Mremi A, Mkwizu E, Paschal J, Sadiq A, Msuya D. Isolated gallbladder tuberculosis in an 84-year old man: a rare case report. Int J Surg Case Rep 2021; 87: 106471
- 9 Soni S, Sreesanth KS, Varshney V, Swami A. Gall bladder tuberculosis: review of literature. Indian J Tuberc 2022; 69 (04) 421-426
- 10 Jagtap SV, Kulkarni SR, Saini S. et al. Xanthogranulomatous cholecystitis: an uncommon variant. Int J Healthc Biomed Res 2015; 3: 47-50
- 11 Treatment of Tuberculosis. Guidelines. In: Treatment of Extrapulmonary TB and of TB in Special Situations. 4th ed.. Geneva: World Health Organization; 2010: 8
- 12 Xu XF, Yu RS, Qiu LL. et al. Gallbladder tuberculosis: CT findings with histopathologic correlation. Korean J Radiol 2011; Mar-Apr; 12 (02) 196-202