

Subscribe to RSS
DOI: 10.1055/s-0045-1806809
Hepatobiliary Phase MRI as a Problem-Solving Sequence for Evaluating Potentially Metastatic Liver Lesions: A Case Series
Authors


Abstract
Background Incidentally detected focal liver lesions in patients with known primary malignancy often pose a diagnostic challenge and are labeled as indeterminate. Utilizing an additional hepatobiliary phase as an adjunct in these cases helps to differentiate potentially metastatic lesions from benign or pseudo lesions.
Aim We share three cases where hepatobiliary phase imaging for an indeterminate hepatic observation helped in differentiating benign from metastatic etiology. We also briefly discuss the different appearances of liver lesions in post-chemotherapy patients.
Results and Conclusion Out of the three cases, one had a hypointense appearance on the hepatobiliary phase suggesting metastasis, while the other two had iso- or hyperintense appearance suggesting a benign or pseudo lesion.
Introduction
The characterization of focal liver lesions is crucial in staging oncology patients and deciding management. The diagnosis of liver metastasis may often convert a patient from curative to palliative treatment. Contrast-enhanced computed tomography (CECT) is often the first line of imaging performed in staging as well as follow-up of a known primary malignancy. We often encounter focal indeterminate liver lesions in these studies. While many get characterized on ultrasonography, some require magnetic resonance imaging (MRI) for further evaluation. Performing a dedicated hepatobiliary phase (HBP) using gadobenate dimeglumine (Gd- BOPTA) as a contrast agent in such cases can often help answer the clinical question. Metastases lack functioning hepatocytes or biliary ducts and do not demonstrate contrast uptake during the HBP. The presence of uptake in the lesion rules out a malignancy; however, there can be atypical appearances, particularly a “targetoid pattern” of enhancement in few cases as discussed later in the article.[1] [2]
Methods
In this series, we discuss three cases with a known malignancy who presented with indeterminate liver lesion(s). All three cases underwent dynamic liver MRI. HBP was obtained as a problem-solving sequence for their characterization. The MRI was performed on a 1.5 Tesla, Philips Ingenia (Amsterdam, The Netherlands), which included the institutional liver imaging protocol ([Table 1]).
Case 1
A 51-year-old female with a history of carcinoma breast operated 17 years ago and on regular follow-up presented with complaints of abdominal pain for 10 days. The ultrasound (USG) performed was normal. However, CECT ([Fig. 1]) showed multiple tiny hypodense lesions in both lobes of the liver. Rest all organs were unremarkable. The various laboratory parameters, including leukocyte count, were also normal.

Multiphasic MRI ([Fig. 2]) showed multiple hepatic lesions which were less prominent on the MRI compared with the CT. These lesions were best appreciated in the diffusion-weighted-imaging sequence as foci of increased signal with an isointense appearance on the corresponding apparent diffusion coefficient map. Further, these lesions were inconspicuous on the HBP images, indicating that they had uptake of the hepatobiliary contrast, thus ruling out metastasis. Differential diagnosis of focal fatty change or resolving abscesses was given. As per the oncologist's request, a repeat targeted USG using a high-frequency linear transducer was done. In the targeted liver USG, we were able to see few subtle sub-centimeter-sized hypoechoic lesions in segments IV and II which were targeted for biopsy, which was suggestive of benign liver parenchyma with periportal inflammation. A follow-up MRI performed after 2 months demonstrated complete resolution of the lesions.

Case 2
A 48-year-old serous ovarian cancer patient treated with total abdominal hysterectomy and bilateral salpingo-oophorectomy 2 years ago presented with fever for 10 days and rising CA-125 levels measuring 241 units/mL. Outside CECT films revealed two hypodense liver lesions in segments IVA and VIII, which were new in comparison to the pretreatment CT study. The multidisciplinary team advised dynamic liver MRI with HBP ([Fig. 3]), which revealed a few (at least five) well-defined T2 W observations in segments VII, IVA, and II, likely simple cysts. Two T2 intermediate signal intensity lesions were also present, one each in segments VII and IVA/VIII, IVB, which were mildly hypointense on T1W images. These appeared suspicious in the regular phases, particularly in the context of rising tumor markers. HBP imaging was accordingly performed. The lesions became isointense to the hepatic parenchyma in the HBP, ruling out the possibility of liver metastasis. No biopsy was done in this case and the liver lesion remained stable on follow-up at 6 months. The patient also had a decline in CA-125 level at 3 and 6 months, and follows up regularly with the local oncologist.

Case 3
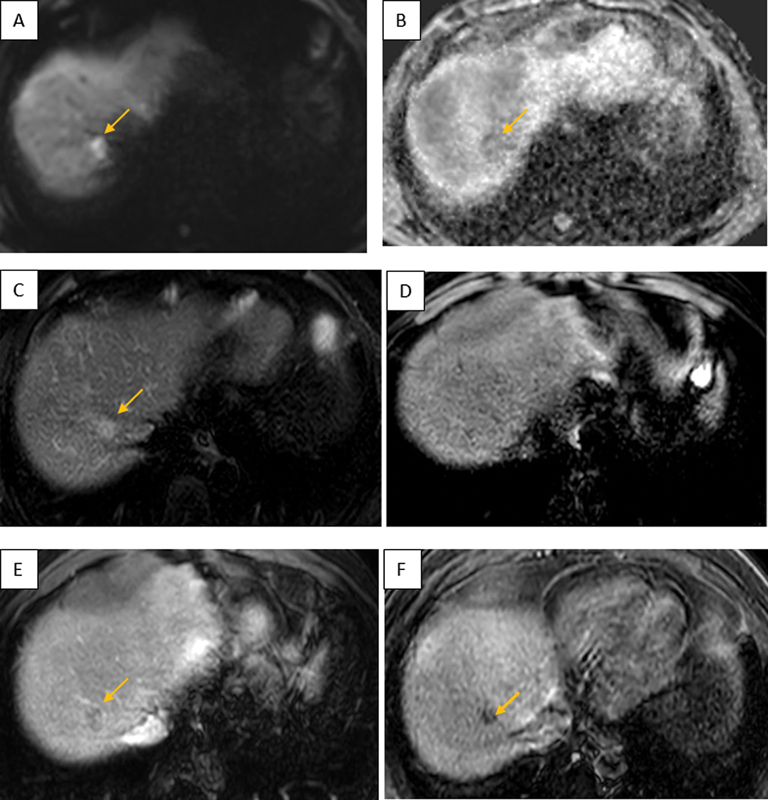
A 39-year-old male was diagnosed with carcinoma rectum (cTNM - T4BN2). Baseline evaluation demonstrated an indeterminate solitary liver lesion of size 15 × 12 mm in segment VIII. Based on a multidisciplinary team discussion, a liver MRI with HBP ([Fig. 4]) was performed, which showed a T2W hyperintense hypo-enhancing lesion with diffusion restriction. It remained hypointense on HBP, consistent with metastasis. The patient was started on neoadjuvant chemotherapy for primary followed by curative surgery, while the liver lesion was considered metastatic and underwent radiofrequency ablation. The patient is on regular follow-up with no recurrence in the ablation zone or elsewhere.
Discussion
The liver is one of the most common sites for metastasis from gastrointestinal, breast, and lung cancers. The use of conventional extracellular contrast agents with dynamic phase imaging helps in characterizing the lesion based on its enhancement pattern. However, HBP contrast agents increase the sensitivity of MRI in detecting a liver lesion, as well as the specificity in differentiating hepatocellular versus nonhepatocellular origin of liver lesions.[2] Given the lack of functional hepatocytes, metastases stand out on the HBP images as hypointense lesions without uptake of the hepatobiliary contrast in the background of hyperintense liver parenchyma.
The majority of literature regarding the pattern of enhancement of liver metastasis on HBP is consistent with a hypointense appearance.[3] [4] [5] In a study conducted by Morana et al[6] to evaluate the efficacy of HBP imaging with Gd- BOPTA for distinguishing benign versus malignant lesions, it was proven that iso- or hyperintense appearance of any lesion on HBP as an indicator for benignity had the sensitivity, specificity, accuracy, PPV, and NPV for benign lesion identification as 96.6, 87.6, 91.4, 85.1, and 97.3%, respectively, with only 2 of 105 metastases being hyperintense or isointense on HBP. In a study performed on 41 patients with liver metastasis by using Gd- BOPTA, a statistically significant increased detection rate was observed with the use of HBP imaging, in comparison with either unenhanced MRI or conventional dynamic contrast-enhanced MRI.[7] A study also compared the diagnostic ability of Gd-BOPTA-enhanced HBP imaging versus superparamagnetic iron oxide (SPIO)-enhanced imaging for the detection of liver metastasis. It concluded that the efficacy of Gd-BOPTA-enhanced HBP was comparable to SPIO agents, however, had a better diagnostic yield over Gd-BOPTA-enhanced dynamic images alone.[8]
Hepatic metastases can also demonstrate some atypical appearances. In a study conducted to determine the imaging features of hepatic metastasis using gadoxetic acid in patients with colorectal cancer, it was concluded that the classic hypointense appearance was seen in 27.9% (22/79 lesions), while the more common appearance on HBP was a heterogenous defect in 63.3% (50/79 lesions).[9] This pattern of residual enhancement on HBP is attributed to prolonged retention of the conventional extracellular contrast component of gadoxetic acid by the intratumoral “intra-acinar necrosis” or “adjoining desmoplastic reaction.”[10] In another study analyzing focal liver lesions using Gd-BOPTA, most of the metastasis (85%) showed a target appearance composed of a central round strong enhancing portion with a peripheral low-signal rim. This pattern of HBP enhancement was attributed to the more fibrotic component of certain metastases, which results in prolonged contrast retention in the interstitial space.[11] Granata et al studied pattern of enhancement of colorectal liver metastasis on MRI, and concluded that 80 lesions (53.3%) were hypointense, while 70 lesions (46.7%) had a target appearance on HBP.[12] This pattern of enhancement refers to a relative low-signal intensity in the center of lesion in comparison to periphery, and is attributed to the desmoplastic changes.[13]
Through our case series, we have highlighted the role of HBP in characterizing indeterminate potentially metastatic liver lesions in patients with breast, ovarian, and rectal cancers. We have also discussed in brief the atypical imaging appearance of liver metastases quoted in the literature as well. HBP imaging is a useful problem-solving tool in patients with indeterminate liver lesions to differentiate benign from metastatic etiology.
Conflicts of Interest
None declared.
Acknowledgment
Not applicable.
-
References
- 1 Seale MK, Catalano OA, Saini S, Hahn PF, Sahani DV. Hepatobiliary-specific MR contrast agents: role in imaging the liver and biliary tree. Radiographics 2009; 29 (06) 1725-1748
- 2 Francisco FAF, de Araújo ALE, Oliveira Neto JA, Parente DB. Hepatobiliary contrast agents: differential diagnosis of focal hepatic lesions, pitfalls and other indications. Radiol Bras 2014; 47 (05) 301-309
- 3 Pirovano G, Vazulli A, Marti-Bonmati L. et al. Evaluation of the accuracy of gadobenate dimeglumine-enhanced MR imaging in the detection and characterization of focal liver lesions. Appl Radiol 2003; 32: 147-159
- 4 Caudana R, Morana G, Pirovano GP. et al. Focal malignant hepatic lesions: MR imaging enhanced with gadolinium benzyloxypropionictetra-acetate (BOPTA)–preliminary results of phase II clinical application. Radiology 1996; 199 (02) 513-520
- 5 Spinazzi A, Lorusso V, Pirovano G, Taroni P, Kirchin M, Davies A. Multihance clinical pharmacology: biodistribution and MR enhancement of the liver. Acad Radiol 1998; 5 (Suppl. 01) S86-S89 , discussion S93–S94
- 6 Morana G, Grazioli L, Kirchin MA. et al. Solid hypervascular liver lesions: accurate identification of true benign lesions on enhanced dynamic and hepatobiliary phase magnetic resonance imaging after gadobenate dimeglumine administration. Invest Radiol 2011; 46 (04) 225-239
- 7 Choi JY, Choi JS, Kim MJ. et al. Detection of hepatic hypovascular metastases: 3D gradient echo MRI using a hepatobiliary contrast agent. J Magn Reson Imaging 2010; 31 (03) 571-578
- 8 Kim YK, Lee JM, Kim CS, Chung GH, Kim CY, Kim IH. Detection of liver metastases: gadobenate dimeglumine-enhanced three-dimensional dynamic phases and one-hour delayed phase MR imaging versus superparamagnetic iron oxide-enhanced MR imaging. Eur Radiol 2005; 15 (02) 220-228
- 9 Kim A, Lee CH, Kim BH. et al. Gadoxetic acid-enhanced 3.0T MRI for the evaluation of hepatic metastasis from colorectal cancer: metastasis is not always seen as a “defect” on the hepatobiliary phase. Eur J Radiol 2012; 81 (12) 3998-4004
- 10 Conti JA, Kendall TJ, Bateman A. et al. The desmoplastic reaction surrounding hepatic colorectal adenocarcinoma metastases aids tumor growth and survival via alphav integrin ligation. Clin Cancer Res 2008; 14 (20) 6405-6413
- 11 Kim YK, Lee JM, Kim CS. Gadobenate dimeglumine-enhanced liver MR imaging: value of dynamic and delayed imaging for the characterization and detection of focal liver lesions. Eur Radiol 2004; 14 (01) 5-13
- 12 Granata V, Catalano O, Fusco R. et al. The target sign in colorectal liver metastases: an atypical Gd-EOB-DTPA “uptake” on the hepatobiliary phase of MR imaging. Abdom Imaging 2015; 40 (07) 2364-2371
- 13 Pozowski P, Misiak P, Szymańska K. et al. Atypical enhancement of gd-bopta on the hepatobiliary phase in hepatic metastasis from carcinoid tumor – case report. Am J Case Rep 2020; 21: e924280
Address for correspondence
Publication History
Article published online:
01 April 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Seale MK, Catalano OA, Saini S, Hahn PF, Sahani DV. Hepatobiliary-specific MR contrast agents: role in imaging the liver and biliary tree. Radiographics 2009; 29 (06) 1725-1748
- 2 Francisco FAF, de Araújo ALE, Oliveira Neto JA, Parente DB. Hepatobiliary contrast agents: differential diagnosis of focal hepatic lesions, pitfalls and other indications. Radiol Bras 2014; 47 (05) 301-309
- 3 Pirovano G, Vazulli A, Marti-Bonmati L. et al. Evaluation of the accuracy of gadobenate dimeglumine-enhanced MR imaging in the detection and characterization of focal liver lesions. Appl Radiol 2003; 32: 147-159
- 4 Caudana R, Morana G, Pirovano GP. et al. Focal malignant hepatic lesions: MR imaging enhanced with gadolinium benzyloxypropionictetra-acetate (BOPTA)–preliminary results of phase II clinical application. Radiology 1996; 199 (02) 513-520
- 5 Spinazzi A, Lorusso V, Pirovano G, Taroni P, Kirchin M, Davies A. Multihance clinical pharmacology: biodistribution and MR enhancement of the liver. Acad Radiol 1998; 5 (Suppl. 01) S86-S89 , discussion S93–S94
- 6 Morana G, Grazioli L, Kirchin MA. et al. Solid hypervascular liver lesions: accurate identification of true benign lesions on enhanced dynamic and hepatobiliary phase magnetic resonance imaging after gadobenate dimeglumine administration. Invest Radiol 2011; 46 (04) 225-239
- 7 Choi JY, Choi JS, Kim MJ. et al. Detection of hepatic hypovascular metastases: 3D gradient echo MRI using a hepatobiliary contrast agent. J Magn Reson Imaging 2010; 31 (03) 571-578
- 8 Kim YK, Lee JM, Kim CS, Chung GH, Kim CY, Kim IH. Detection of liver metastases: gadobenate dimeglumine-enhanced three-dimensional dynamic phases and one-hour delayed phase MR imaging versus superparamagnetic iron oxide-enhanced MR imaging. Eur Radiol 2005; 15 (02) 220-228
- 9 Kim A, Lee CH, Kim BH. et al. Gadoxetic acid-enhanced 3.0T MRI for the evaluation of hepatic metastasis from colorectal cancer: metastasis is not always seen as a “defect” on the hepatobiliary phase. Eur J Radiol 2012; 81 (12) 3998-4004
- 10 Conti JA, Kendall TJ, Bateman A. et al. The desmoplastic reaction surrounding hepatic colorectal adenocarcinoma metastases aids tumor growth and survival via alphav integrin ligation. Clin Cancer Res 2008; 14 (20) 6405-6413
- 11 Kim YK, Lee JM, Kim CS. Gadobenate dimeglumine-enhanced liver MR imaging: value of dynamic and delayed imaging for the characterization and detection of focal liver lesions. Eur Radiol 2004; 14 (01) 5-13
- 12 Granata V, Catalano O, Fusco R. et al. The target sign in colorectal liver metastases: an atypical Gd-EOB-DTPA “uptake” on the hepatobiliary phase of MR imaging. Abdom Imaging 2015; 40 (07) 2364-2371
- 13 Pozowski P, Misiak P, Szymańska K. et al. Atypical enhancement of gd-bopta on the hepatobiliary phase in hepatic metastasis from carcinoid tumor – case report. Am J Case Rep 2020; 21: e924280