

Subscribe to RSS
DOI: 10.1055/s-0045-1808062
Undifferentiated/Dedifferentiated Carcinomas of the Endometrium: A Retrospective Clinicopathological Study of a Series of 11 Cases
Authors
Funding None.

Abstract
Introduction Undifferentiated endometrial carcinomas (UDECs) are rare subtypes of endometrial carcinomas with aggressive clinical behavior. Histologically, UDEC exhibits a solid growth pattern and consists of monomorphic, discohesive, small to medium-sized round cells, with absent to minimal neuroendocrine differentiation. When UDEC is accompanied by a differentiated carcinoma component (usually International Federation of Gynecology and Obstetrics [FIGO] grade 1 or 2), it is termed dedifferentiated endometrial carcinoma (DDEC). The diagnosis of these tumors is challenging because of their close histological similarity to grade 3 endometrioid adenocarcinomas.
Objectives This article aims to understand and elucidate the clinical presentation, pathological findings, treatment options, and outcomes of UDEC/DDEC.
Materials and Methods Diagnosed/suspected cases of UDEC/DDEC, based on pathology reports between January 2018 and January 2023, were retrieved from the pathology database. Clinical, treatment, and follow-up details were retrieved from the electronic medical record database.
Results Out of the 21 cases reviewed, 10 cases were reclassified as “grade 3 endometrioid adenocarcinoma” and 1 case as carcinosarcoma based on histomorphology and immunohistochemical findings. There were 11 cases of undifferentiated carcinoma, out of which 7 were reconfirmed and assigned a DDEC diagnosis. Lower uterine segment involvement was seen in 45% of cases. Out of the 11 patients, 6 patients were diagnosed with stage IIC disease, 4 patients with stage IIIC disease, and 1 patient with stage IV disease (FIGO 2023 staging). Mismatch repair (MMR) protein deficiency was seen in 50% of tested cases and loss of SMARCA4 (BRG1) was seen in one case. Four patients received adjuvant concurrent chemoradiation, one patient received adjuvant chemotherapy, and one patient received neoadjuvant chemotherapy. Six patients had no evidence of disease at follow-up ranging from 6 to 24 months. Two patients had disease progression and one patient died of disease.
Conclusion UDECs and DDECs are rare endometrial tumors that show characteristic histomorphology, weak/absent immunohistochemistry staining for EMA/PAX8, and MMR protein deficiency in a subset of cases. It is important to have a high index of suspicion for these tumors due to close mimickers, their aggressive behavior, and the potential role of treatment with immunotherapy.
Introduction
Undifferentiated endometrial carcinomas (UDECs) and dedifferentiated endometrial carcinomas (DDECs) are rare subtypes of endometrial carcinomas, which comprise 1 to 2% of all endometrial cancers.[1] UDECs were first described by Silva et al[1] in 2006 as tumors with no overt cell lineage differentiation. According to the 2020 World Health Organization (WHO) classification of tumors of the female genital tract, DDECs are described as tumors composed of undifferentiated carcinoma and a juxtaposed differentiated component, typically International Federation of Gynecology and Obstetrics (FIGO) grade 1 or 2 endometrioid adenocarcinoma.[2] DDECs can be misdiagnosed as grade 3 endometrioid adenocarcinoma or carcinosarcoma.[3]
The recognition of these tumors is important given their aggressive clinical course with a high risk of locoregional spread, distant metastasis, and resistance to conventional chemotherapy regimens.[4]
Given the rarity of these tumors, our objective was to assess the histomorphological spectrum, management, and clinical outcomes in these patients at our center.
Materials and Methods
Study Setting and Design
UDECs are rare endometrial tumors that are frequently misdiagnosed as high-grade sarcomas, carcinosarcomas, and grade 3 endometrioid adenocarcinomas. There has been no case series from India about UDECs to date and we aim to study these tumors diagnosed at our institute. A retrospective analysis of 21 UDEC and DDEC cases diagnosed from January 2018 to January 2023 was performed, focusing on their clinicopathological characteristics, management, and follow-up details. Clinical, radiological, and treatment information, where available, was obtained from our institute's electronic medical record database. Hematoxylin and eosin (H&E) and immunohistochemistry (IHC) stains performed on paraffin-embedded tissue blocks were available for review in all cases.
Primary and Secondary Outcomes
As this is a retrospective case series of a rare subtype of endometrial cancer, follow-up and outcome details are limited.
Inclusion and Exclusion criteria
All cases diagnosed as UDECs and DDECs at our center over 5 years (January 2018 to January 2023) were included in the study. The presence of a distinct undifferentiated carcinoma component composed of monomorphic discohesive round/rhabdoid cells with focal/absent keratin and epithelial membrane antigen (EMA)/paired box 8 (PAX8) expression was taken as a diagnostic criterion for inclusion in the study.[5] Tumors with an undifferentiated carcinoma component juxtaposed to a FIGO grade 1 or 2 endometrioid adenocarcinoma component were diagnosed as DDECs.[2]
Statistical Analysis
Descriptive statistics to measure central tendency including median and to measure dispersion in the form of ranges and percentages were performed using Microsoft Office Excel.
Ethical Approval
This study was approved by the Tata Memorial Hospital Institutional Ethics Committee (Project number 4424). A waiver of consent was granted since this was a retrospective study with less than minimal risk. All procedures performed in studies involving human participants were as per the ethical standards of the institutional and/or national research committee and with the Helsinki Declaration of 1964 and its later amendments or comparable ethical standards.
Results
We retrieved and reviewed 21 cases of UDEC and DDEC that were diagnosed/suspected during the study period. Ten cases were reclassified as “grade 3 endometrioid adenocarcinoma” (solid pattern), based on tumor cell cohesion, similar morphology of cells in the solid and glandular areas, and diffuse strong EMA and PAX8 positivity in the high-grade solid component. One case was reclassified as carcinosarcoma, due to biphasic epithelial and spindle cell sarcomatous component. Finally, 11 cases of UDEC were identified and analyzed further. These included seven cases that were associated with a differentiated FIGO grade 1/2 endometrioid adenocarcinoma component, and hence were redesignated as DDECs. Three out of 11 cases were referral cases, and in these, a hysterectomy was done elsewhere. In one patient, only endometrial curettage had been done for diagnosis, which was available for review. The details of these cases are described below.
Clinical Presentation and Investigations
The median age of presentation was 57 years (age range: 27–74 years). All patients presented with abnormal uterine bleeding or postmenopausal bleeding. One patient had a family history of endometrial carcinoma with synchronous carcinoma colon. Clinical and radiological details were available in 8 out of 11 cases and have been tabulated in [Table 1].
Abbreviations: AUB, abnormal uterine bleeding; BPLND, bilateral pelvic lymph node dissection; C, carboplatin; DFI, disease-free interval; DOD, died of disease; EBRT, external beam radiotherapy; ESS, endometrial stromal sarcoma; NA, not available; NACT, neoadjuvant chemotherapy; ND, not done; NED, no evidence of disease; OS, overall survival; P, paclitaxel; PMB, postmenopausal bleeding; RPLND, retroperitoneal lymph node dissection; TH + BSO, total hysterectomy with bilateral salpingo-oophorectomy.
Macroscopic and Microscopic Findings
Detailed gross findings were available in 8 out of 11 cases. The tumor size measured grossly or by radiology ranged from 1.7 to 8.8 cm. The tumor location was the anterior wall of the uterus (n = 3), right lateral wall (n = 1), posterior wall (n = 2), and filled the endometrial cavity in 2 cases. The tumor involved more than half of the myometrium in 4 out of 11 cases (n = 4) with serosal involvement seen in one case. Lower uterine segment (LUS) involvement was seen in five cases (n = 5). Six patients presented with FIGO 2023 stage IIC disease, four with stage IIIC, and one patient with stage IV disease. Corresponding details of biopsy/curettage were available only in 4 out of 10 resection cases. Two cases were diagnosed as grade 3 endometrioid adenocarcinoma and one as DDEC on biopsy. One case came with a referral diagnosis of high-grade endometrial stromal sarcoma.
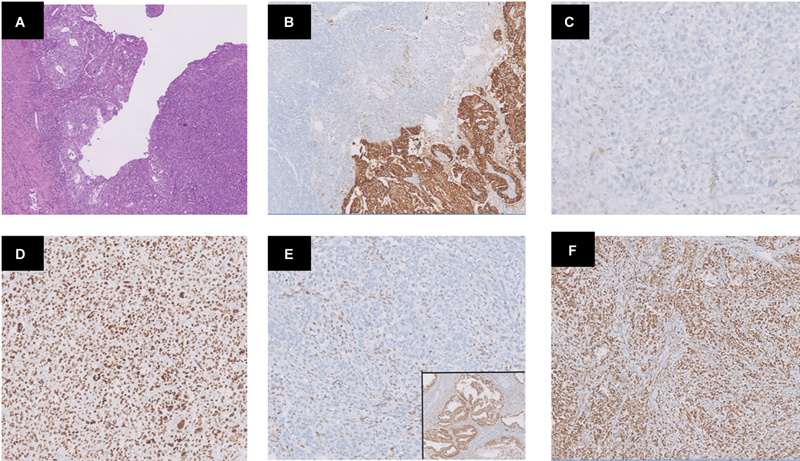
In all the cases (n = 11), the undifferentiated component was composed of sheets of discohesive monomorphic small to medium-sized round cells without any evidence of gland formation. A focal trabecular pattern was seen in two cases (n = 2). Tumor cells were round to ovoid with vesicular nuclei and prominent nucleoli (n = 11). Focal rhabdoid morphology (large cells with eosinophilic inclusion like cytoplasm and prominent nucleoli) was seen in four cases (n = 4; [Fig. 1]). The percentage of undifferentiated components ranged from 50 to 100%. In the DDEC cases, the differentiated component was composed of endometrioid adenocarcinoma FIGO grade 1 (n = 3) and grade 2 (n = 4). Lymphovascular invasion was seen in 54.5% of cases (n = 6). The findings are summarized in [Table 2].

Abbreviations: A, absent; DDEC, dedifferentiated endometrial carcinoma; FIGO, International Federation of Gynecology and Obstetrics; LVSI, lymphovascular space invasion; NA, not available; P, present; UDEC, undifferentiated endometrial carcinoma.
Note: focal: < 5 vessels involved; extensive ≥5 vessels involved.
Immunohistochemical Findings
IHC with various antibodies was performed on all cases, the details of which are summarized in [Table 3]. Undifferentiated components demonstrated focal staining for keratins, AE1/AE3 (n = 9), and EMA (n = 7; [Fig. 2]). Focal positivity for PAX8 was seen in one case. IHC for MMR proteins was performed on eight cases, of which four cases were MMR protein deficient (three cases with MutL protein homolog 1 (MLH1)/postmeiotic segregation increased 2 (PMS2) loss and one case with isolated MSH2 loss; [Fig. 2]). integrase interactor 1 (INI1) was retained in all cases (n = 6/11) and loss of Brahma-related gene 1 (BRG1) expression was seen in one case (1/6; [Fig. 1]).
Abbreviations: BRG1, Brahma-related gene 1; CK, cytokeratins; EMA, epithelial membrane antigen; ER, estrogen receptor; focal, <50% staining (strong staining in the differentiated component); INI1, integrase interactor 1; MLH1, MutL protein homolog 1; MSH2, MutS homolog 2; MSH6, MutS homolog 6; N, negative; NP, not performed; PAX8, paired box 8; PMS2, postmeiotic segregation increased 2; PR, progesterone receptor.
Treatment and Follow-Up
Ten out of the 11 cases underwent total hysterectomy with bilateral salpingo-oophorectomy. Bilateral pelvic and retroperitoneal nodal dissection was done in six cases. Four patients received adjuvant chemotherapy along with radiotherapy (n = 4), of which three patients were disease free at 6, 18, and 24 months of follow-up. One patient had disease progression with lymph node metastasis and was on immunotherapy (pembrolizumab with lenvatinib). Two patients received chemotherapy alone, of which one patient died of disease and one had disease progression at 6 months. One patient who presented with distant metastasis (supraclavicular lymph nodes) was on palliative treatment and was lost to follow-up. Treatment and follow-up details are summarized in [Table 1].
Discussion
Endometrial carcinoma is one of the most common gynecologic cancers worldwide.[6] The recently described UDECs and DDECs are rare, but aggressive subtypes,[7] representing approximately 9% of endometrial carcinomas.[1] In the current FIGO grading system of endometrial carcinomas, tumors are graded by the proportion of solid area within the tumor, without further characterization of the histologic details of the solid component. This may lead to misdiagnosis of these tumors as grade 3 endometrioid adenocarcinomas.[8] Carcinomas with undifferentiated components are consistently reported to be more aggressive than high-grade endometrioid adenocarcinomas.[9]
The median age at diagnosis in our series was evaluated to be 57 years, comparable to a previous study by Tafe et al.[7] However, these tumors can affect young age groups, and constitute 7% of endometrial carcinomas in patients aged younger than 40 years of age.[10] Most common presenting symptoms are postmenopausal bleeding and vaginal discharge.[11]
UDECs usually present as large polypoidal masses in the endometrial cavity with frequent LUS involvement.[7] In our series, LUS involvement was seen in 45% of cases (n = 5). Hence, sampling the LUS while grossing a hysterectomy specimen is a crucial step and ensures that all the components of a tumor are identified, leading to correct diagnosis, more precise treatment planning, and optimal prognostication.
Although histological features of high-grade endometrioid adenocarcinomas and UDEC/DDEC may overlap, careful attention made to the cellular details and architectural patterns can help in differentiating the two entities. In the undifferentiated carcinoma component, the tumor cells lack intercellular cohesion and are arranged in patternless sheets without gland formation and neuroendocrine differentiation (<10%).[11] The tumor cells are monomorphic small to medium-sized cells with vesicular nuclei and prominent eosinophilic nucleoli.[7] Tumors may show nesting or alveolar pattern with intervening delicate fibrovascular septa. Variable amounts of rhabdoid cells in a myxoid background may be seen. Other specific histologic features that were seen in some UDECs were multinucleation, focal nuclear pleomorphism, and prominent tumor-infiltrating lymphocytes. As originally described by Altrabulsi et al,[11] these tumors often do not show mucinous differentiation or spindled growth pattern.
UDECs can be associated with FIGO grade 1/2 endometrioid adenocarcinomas, labeled as DDECs.[12] In our series, 63.6% (n = 7) of cases were associated with a differentiated component. The well-differentiated component is usually superficially located, whereas the undifferentiated component is deep and invades the myometrium. This can lead to misdiagnosis in the endometrial biopsy, which is a critical step in suspected endometrial carcinoma cases. In our series, only two cases were initially diagnosed as dedifferentiated carcinoma in the biopsy specimen, highlighting the issue of under-grading.
In DDECs, histologically, a sharp demarcation is noted between the undifferentiated and differentiated carcinoma components, whereas a seamless transition between the glandular and solid areas is seen in high-grade endometrioid adenocarcinomas. Also, the cells forming the solid area in high-grade endometrioid adenocarcinomas show similar cytological features as those of the glandular component.[13] DDECs can also be misdiagnosed as carcinosarcomas, given their somewhat biphasic appearance. However, carcinosarcomas usually display an admixture of high-grade differentiated component (usually serous carcinoma) and a distinct pleomorphic spindle cell sarcomatous component,[14] unlike the monomorphic undifferentiated component in DDECs.
IHC also plays a key role in the differential diagnosis of these tumors. Among the epithelial markers, EMA and CK 8/18 are shown to be diffusely and strongly positive in the high-grade solid and well-differentiated components of endometrioid adenocarcinomas, whereas show focal, weak dot-like positivity in the undifferentiated component.[7] In our series (n = 11), focal staining for EMA/pancytokeratin (AE1/AE3) was seen in the undifferentiated component, whereas the differentiated component showed diffuse cytoplasmic staining (n = 7). Ramalingam et al suggested PAX8 as the most effective marker to distinguish between undifferentiated and high-grade solid components.[5] In our study, PAX8 was performed in only five cases, of which one case of UDEC showed focal positivity. Estrogen receptor (ER) and progesterone receptor (PR) show focal/absent expression in UDEC, whereas retained expression in the well-differentiated endometrioid carcinoma component,[15] which was consistent with our series. Hoang et al also reported that loss of PAX8 and ER expression may be a fundamental feature of dedifferentiation.[16] The undifferentiated component can show focal neuroendocrine differentiation (synaptophysin and/or chromogranin expression) in less than 10% of tumor cells, in contrast to a more diffuse and strong expression seen in high-grade neuroendocrine carcinomas. In our series, synaptophysin was done only in one case, and showed negative expression.
When tumors involve the LUS, it is essential to rule out high-risk human papillomavirus (HPV) related endocervical adenocarcinoma. These tumors can present with mixed mucinous and endometrioid-like features, resembling endometrioid adenocarcinomas, but they often have more mitotic figures and apoptotic bodies. The standard IHC panel, including ER/PR, p16, and PAX8, may not effectively distinguish between these tumors, as both can be negative for ER and PAX8.[17] In a case series by Saad et al,[18] 50% of uterine differentiated endocervical adenocarcinomas showed strong p16 positivity, similar to endocervical adenocarcinomas. Consequently, differentiating these entities can be challenging and may rely on imaging for tumor epicenter and HPV in situ hybridization studies.
SMARCA4-deficient undifferentiated uterine sarcoma (SDUS) has a morphology that overlaps with UDEC. Both these tumors show sheets of monomorphic rhabdoid-like cells; however, a phyllodiform (leaf-like) architecture favored a diagnosis of SDUS. Compared with SDUS, UDECs were seen in older women, and more frequently showed TP53 mutations, microsatellite instability, and intact SMARCA4 and SMARCB1.[19]
UDECs and DDECs are suggested to be associated with deficiency of mismatch repair (MMR) proteins and have shown association with Lynch syndrome. MMR deficiency is seen in 58% of these tumors, compared to 25 to 30% in other endometrial carcinomas.[20] In our series, 50% of tumors showed MMR deficiency, which is consistent with previous reports.[20] Approximately, 60% of these tumors show loss of expression of switch/sucrose nonfermenting (SWI/SNF) complex proteins, including ARID1B, SMARCA4 (BRG1), and SMARCB1 (INI1).[21] Only one case showed loss of BRG1 expression in our case series.
Owing to the rarity of these tumors, there is limited experience with treatment strategies. Comprehensive staging surgery should be performed in operable cases, including total hysterectomy with bilateral salpingo-oophorectomy, systematic lymphadenectomy, and infracolic omentectomy.[22] UDEC is an aggressive histologic subtype of endometrial carcinoma and warrants adjuvant treatment with chemotherapy (carboplatin/paclitaxel) and external beam radiotherapy with/without vaginal brachytherapy.[22]
Despite intensive treatment regimens, a fulminant recurrence pattern with short survival was reported by Han et al.[13] Disease-related death rate ranges from 41 to 75%, which occurs mostly in the first 5 years after diagnosis. According to Silva et al,[12] of the 25 cases of UDEC/DDEC studied, the frequency of stage I and II disease was 37.5% and that of stage III and IV disease was 62.5%. Our series showed a frequency of 54.5 and 45.4%. Pelvic and para-aortic lymph nodes were the most common sites of metastasis. Silva et al[12] and Tafe et al[7] noted that the presence of even a small undifferentiated component (as low as 5%) leads to poor clinical outcomes.
In The Cancer Genome Atlas (TCGA) classification, the POLE-ultramutated tumors were reported as a subtype of endometrial carcinomas with an excellent prognosis, irrespective of other clinicopathological variables. Espinosa et al[23] found that two UDEC and seven DDEC patients (9/21, 43%) had mutations in the POLE exonuclease domain. These mutations were more common in FIGO stage I tumors and correlated with better outcomes (p = 0.02).
MMR protein-deficient (dMMR) tumors may benefit from combination treatment with immune checkpoint inhibitors.[24] The Keynote-146 phase 1/2 trial showed the combination of pembrolizumab with lenvatinib to have a promising antitumor response in patients with advanced endometrial carcinomas, regardless of their tumor microsatellite (MSI) status.[25] Other PD-1 inhibitors, such as dostarlimab and nivolumab, have also shown antitumor activity against dMMR tumors.[26] SWI/SNF complex deficiency defines a highly aggressive subset of UDEC in which 1-year cancer-specific survival is 26% compared to 75% in SWI/SNF complex-intact tumors.[27] Therefore, the distinction may become clinically relevant as investigational drugs such as EZH2 inhibitors have shown preclinical efficacy in targeting BRG1- and INI1-deficient tumors.[28]
In our present series, three patients (one patient with stage II and two patients with stage III disease) who received adjuvant chemotherapy (paclitaxel and carboplatin) with concurrent radiotherapy are alive with no evidence of disease at 15, 18, and 26 months. Two patients with stage III disease had progression 4 and 8 months after completion of treatment with vault recurrence and regional lymph node metastasis and are on immunotherapy with pembrolizumab and lenvatinib. One patient with stage II disease (who received neoadjuvant chemotherapy) died of disease 7 months after diagnosis.
Most of the studies reporting survival outcomes of UDECs and DDECs in the literature have shown worse outcomes relative to differentiated tumors. The original study by Silva et al,[12] with 25 cases of DDEC, reported a crude survival rate of 46%, with 4 patients alive with progressive disease and only 1 patient with no evidence of disease at 104 months. In the largest previously published series of 26 cases of UDEC by Tafe et al,[7] 72% of patients with stage I/II disease and 60% with stage III/IV disease were alive at a median follow-up of 20 months. Üreyen et al[29] reported on a series of 18 cases of UDEC; after a median of 66 months of follow-up, their results were similar to those of our study, with 33% of cases showing progressive disease and 16% succumbing to disease.
Conclusion
To summarize, UDECs and DDECs are aggressive histological subtypes that should not be underdiagnosed as endometrioid adenocarcinomas and, hence, awareness regarding this entity is necessary. Our study emphasized the distinctive clinical, morphological, and immunohistochemical characteristics of these tumors. Their association with MMR protein and SWI/SNF complex protein deficiency makes them future candidates for immunotherapy and newer therapeutic targets.
Conflict of Interest
None declared.
Patient Consent
A waiver of consent was obtained from Institutional Ethics Committee.
-
References
- 1 Silva EG, Deavers MT, Malpica A. Undifferentiated carcinoma of the endometrium: a review. Pathology 2007; 39 (01) 134-138
- 2 Matias-Guiu X, Longacre TA, McCluggage WG. et al. Tumors of the uterine corpus. In: Female Genital Tumours: WHO Classification of Tumours. 5th ed.. Lyon, France: International Agency for Research on Cancer; 2020
- 3 Murali R, Davidson B, Fadare O. et al. High-grade endometrial carcinomas: morphologic and immunohistochemical features, diagnostic challenges and recommendations. Int J Gynecol Pathol 2019; 38 (1, Suppl 1): S40-S63
- 4 AlHilli M, Elson P, Rybicki L. et al. Undifferentiated endometrial carcinoma: a National Cancer Database analysis of prognostic factors and treatment outcomes. Int J Gynecol Cancer 2019; 29 (07) 1126-1133
- 5 Ramalingam P, Masand RP, Euscher ED, Malpica A. Undifferentiated carcinoma of the endometrium: an expanded immunohistochemical analysis including PAX-8 and basal-like carcinoma surrogate markers. Int J Gynecol Pathol 2016; 35 (05) 410-418
- 6 Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 7 Tafe LJ, Garg K, Chew I, Tornos C, Soslow RA. Endometrial and ovarian carcinomas with undifferentiated components: clinically aggressive and frequently underrecognized neoplasms. Mod Pathol 2010; 23 (06) 781-789
- 8 Abeler VM, Kjørstad KE, Nesland JM. Undifferentiated carcinoma of the endometrium. A histopathologic and clinical study of 31 cases. Cancer 1991; 68 (01) 98-105
- 9 Yokomizo R, Yamada K, Iida Y. et al. Dedifferentiated endometrial carcinoma: a report of three cases and review of the literature. Mol Clin Oncol 2017; 7 (06) 1008-1012
- 10 Garg K, Shih K, Barakat R, Zhou Q, Iasonos A, Soslow RA. Endometrial carcinomas in women aged 40 years and younger: tumors associated with loss of DNA mismatch repair proteins comprise a distinct clinicopathologic subset. Am J Surg Pathol 2009; 33 (12) 1869-1877
- 11 Altrabulsi B, Malpica A, Deavers MT, Bodurka DC, Broaddus R, Silva EG. Undifferentiated carcinoma of the endometrium. Am J Surg Pathol 2005; 29 (10) 1316-1321
- 12 Silva EG, Deavers MT, Bodurka DC, Malpica A. Association of low-grade endometrioid carcinoma of the uterus and ovary with undifferentiated carcinoma: a new type of dedifferentiated carcinoma?. Int J Gynecol Pathol 2006; 25 (01) 52-58
- 13 Han J, Ki EY, Rha SE, Hur S, Lee A. Dedifferentiated endometrioid carcinoma of the uterus: report of four cases and review of literature. World J Surg Oncol 2017; 15 (01) 17
- 14 Ferguson SE, Tornos C, Hummer A, Barakat RR, Soslow RA. Prognostic features of surgical stage I uterine carcinosarcoma. Am J Surg Pathol 2007; 31 (11) 1653-1661
- 15 Li Z, Zhao C. Clinicopathologic and immunohistochemical characterization of dedifferentiated endometrioid adenocarcinoma. Appl Immunohistochem Mol Morphol 2016; 24 (08) 562-568
- 16 Hoang LN, Lee YS, Karnezis AN. et al. Immunophenotypic features of dedifferentiated endometrial carcinoma: insights from BRG1/INI1-deficient tumours. Histopathology 2016; 69 (04) 560-569
- 17 Castrillon DH, Lee KR, Nucci MR. Distinction between endometrial and endocervical adenocarcinoma: an immunohistochemical study. Int J Gynecol Pathol 2002; 21 (01) 4-10
- 18 Saad RS, Mashhour M, Noftech-Mozes S. et al. P16INK4a expression in undifferentiated carcinoma of the uterus does not exclude its endometrial origin. Int J Gynecol Pathol 2012; 31 (01) 57-65
- 19 Kolin DL, Quick CM, Dong F. et al. SMARCA4-deficient uterine sarcoma and undifferentiated endometrial carcinoma are distinct clinicopathologic entities. Am J Surg Pathol 2020; 44 (02) 263-270
- 20 McMeekin DS, Tritchler DL, Cohn DE. et al. Clinicopathologic significance of mismatch repair defects in endometrial cancer: an NRG Oncology/Gynecologic Oncology Group Study. J Clin Oncol 2016; 34 (25) 3062-3068
- 21 Kihara A, Amano Y, Matsubara D, Fukushima N, Fujiwara H, Niki T. BRG1, INI1, and ARID1B deficiency in endometrial carcinoma. Am J Surg Pathol 2020; 44: 1712-1724
- 22 Cancer C. NCCN Guidelines for Patients. Uterine Cancer.; 2024.
- 23 Espinosa I, Lee CH, D'Angelo E, Palacios J, Prat J. Undifferentiated and dedifferentiated endometrial carcinomas with POLE exonuclease domain mutations have a favorable prognosis. Am J Surg Pathol 2017; 41 (08) 1121-1128
- 24 Yamashita H, Nakayama K, Ishikawa M. et al. Microsatellite instability is a biomarker for immune checkpoint inhibitors in endometrial cancer. Oncotarget 2017; 9 (05) 5652-5664
- 25 Makker V, Taylor MH, Aghajanian C. et al. Lenvatinib plus pembrolizumab in patients with advanced endometrial cancer. J Clin Oncol 2020; 38 (26) 2981-2992
- 26 Azad NS, Gray RJ, Overman MJ. et al. Nivolumab is effective in mismatch repair-deficient noncolorectal cancers: results from arm Z1D-A subprotocol of the NCI-MATCH (EAY131) Study. J Clin Oncol 2020; 38 (03) 214-222
- 27 Stewart CJR, Crook ML. SWI/SNF complex deficiency and mismatch repair protein expression in undifferentiated and dedifferentiated endometrial carcinoma. Pathology 2015; 47 (05) 439-445
- 28 Wang Y, Chen SY, Karnezis AN. et al. The histone methyltransferase EZH2 is a therapeutic target in small cell carcinoma of the ovary, hypercalcaemic type. J Pathol 2017; 242 (03) 371-383
- 29 Üreyen I, Ilgin H, Turan T. et al. Undifferentiated uterine carcinoma: analysis of eighteen cases. J Obstet Gynaecol 2015; 35 (04) 372-376
Address for correspondence
Publication History
Article published online:
17 April 2025
© 2025. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Silva EG, Deavers MT, Malpica A. Undifferentiated carcinoma of the endometrium: a review. Pathology 2007; 39 (01) 134-138
- 2 Matias-Guiu X, Longacre TA, McCluggage WG. et al. Tumors of the uterine corpus. In: Female Genital Tumours: WHO Classification of Tumours. 5th ed.. Lyon, France: International Agency for Research on Cancer; 2020
- 3 Murali R, Davidson B, Fadare O. et al. High-grade endometrial carcinomas: morphologic and immunohistochemical features, diagnostic challenges and recommendations. Int J Gynecol Pathol 2019; 38 (1, Suppl 1): S40-S63
- 4 AlHilli M, Elson P, Rybicki L. et al. Undifferentiated endometrial carcinoma: a National Cancer Database analysis of prognostic factors and treatment outcomes. Int J Gynecol Cancer 2019; 29 (07) 1126-1133
- 5 Ramalingam P, Masand RP, Euscher ED, Malpica A. Undifferentiated carcinoma of the endometrium: an expanded immunohistochemical analysis including PAX-8 and basal-like carcinoma surrogate markers. Int J Gynecol Pathol 2016; 35 (05) 410-418
- 6 Sung H, Ferlay J, Siegel RL. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71 (03) 209-249
- 7 Tafe LJ, Garg K, Chew I, Tornos C, Soslow RA. Endometrial and ovarian carcinomas with undifferentiated components: clinically aggressive and frequently underrecognized neoplasms. Mod Pathol 2010; 23 (06) 781-789
- 8 Abeler VM, Kjørstad KE, Nesland JM. Undifferentiated carcinoma of the endometrium. A histopathologic and clinical study of 31 cases. Cancer 1991; 68 (01) 98-105
- 9 Yokomizo R, Yamada K, Iida Y. et al. Dedifferentiated endometrial carcinoma: a report of three cases and review of the literature. Mol Clin Oncol 2017; 7 (06) 1008-1012
- 10 Garg K, Shih K, Barakat R, Zhou Q, Iasonos A, Soslow RA. Endometrial carcinomas in women aged 40 years and younger: tumors associated with loss of DNA mismatch repair proteins comprise a distinct clinicopathologic subset. Am J Surg Pathol 2009; 33 (12) 1869-1877
- 11 Altrabulsi B, Malpica A, Deavers MT, Bodurka DC, Broaddus R, Silva EG. Undifferentiated carcinoma of the endometrium. Am J Surg Pathol 2005; 29 (10) 1316-1321
- 12 Silva EG, Deavers MT, Bodurka DC, Malpica A. Association of low-grade endometrioid carcinoma of the uterus and ovary with undifferentiated carcinoma: a new type of dedifferentiated carcinoma?. Int J Gynecol Pathol 2006; 25 (01) 52-58
- 13 Han J, Ki EY, Rha SE, Hur S, Lee A. Dedifferentiated endometrioid carcinoma of the uterus: report of four cases and review of literature. World J Surg Oncol 2017; 15 (01) 17
- 14 Ferguson SE, Tornos C, Hummer A, Barakat RR, Soslow RA. Prognostic features of surgical stage I uterine carcinosarcoma. Am J Surg Pathol 2007; 31 (11) 1653-1661
- 15 Li Z, Zhao C. Clinicopathologic and immunohistochemical characterization of dedifferentiated endometrioid adenocarcinoma. Appl Immunohistochem Mol Morphol 2016; 24 (08) 562-568
- 16 Hoang LN, Lee YS, Karnezis AN. et al. Immunophenotypic features of dedifferentiated endometrial carcinoma: insights from BRG1/INI1-deficient tumours. Histopathology 2016; 69 (04) 560-569
- 17 Castrillon DH, Lee KR, Nucci MR. Distinction between endometrial and endocervical adenocarcinoma: an immunohistochemical study. Int J Gynecol Pathol 2002; 21 (01) 4-10
- 18 Saad RS, Mashhour M, Noftech-Mozes S. et al. P16INK4a expression in undifferentiated carcinoma of the uterus does not exclude its endometrial origin. Int J Gynecol Pathol 2012; 31 (01) 57-65
- 19 Kolin DL, Quick CM, Dong F. et al. SMARCA4-deficient uterine sarcoma and undifferentiated endometrial carcinoma are distinct clinicopathologic entities. Am J Surg Pathol 2020; 44 (02) 263-270
- 20 McMeekin DS, Tritchler DL, Cohn DE. et al. Clinicopathologic significance of mismatch repair defects in endometrial cancer: an NRG Oncology/Gynecologic Oncology Group Study. J Clin Oncol 2016; 34 (25) 3062-3068
- 21 Kihara A, Amano Y, Matsubara D, Fukushima N, Fujiwara H, Niki T. BRG1, INI1, and ARID1B deficiency in endometrial carcinoma. Am J Surg Pathol 2020; 44: 1712-1724
- 22 Cancer C. NCCN Guidelines for Patients. Uterine Cancer.; 2024.
- 23 Espinosa I, Lee CH, D'Angelo E, Palacios J, Prat J. Undifferentiated and dedifferentiated endometrial carcinomas with POLE exonuclease domain mutations have a favorable prognosis. Am J Surg Pathol 2017; 41 (08) 1121-1128
- 24 Yamashita H, Nakayama K, Ishikawa M. et al. Microsatellite instability is a biomarker for immune checkpoint inhibitors in endometrial cancer. Oncotarget 2017; 9 (05) 5652-5664
- 25 Makker V, Taylor MH, Aghajanian C. et al. Lenvatinib plus pembrolizumab in patients with advanced endometrial cancer. J Clin Oncol 2020; 38 (26) 2981-2992
- 26 Azad NS, Gray RJ, Overman MJ. et al. Nivolumab is effective in mismatch repair-deficient noncolorectal cancers: results from arm Z1D-A subprotocol of the NCI-MATCH (EAY131) Study. J Clin Oncol 2020; 38 (03) 214-222
- 27 Stewart CJR, Crook ML. SWI/SNF complex deficiency and mismatch repair protein expression in undifferentiated and dedifferentiated endometrial carcinoma. Pathology 2015; 47 (05) 439-445
- 28 Wang Y, Chen SY, Karnezis AN. et al. The histone methyltransferase EZH2 is a therapeutic target in small cell carcinoma of the ovary, hypercalcaemic type. J Pathol 2017; 242 (03) 371-383
- 29 Üreyen I, Ilgin H, Turan T. et al. Undifferentiated uterine carcinoma: analysis of eighteen cases. J Obstet Gynaecol 2015; 35 (04) 372-376