

Subscribe to RSS
DOI: 10.1055/s-0045-1814429
Recommendations for Screening, Risk Stratification, and Targeted Treatment for Diabetic Kidney Disease in the UAE
Authors
Funding The convening of the expert group meetings and medical writing assistance were facilitated by an unrestricted grant from Bayer, United Arab Emirates, to the Emirates Diabetes and Endocrine Society. Bayer, United Arab Emirates, did not participate in any of the meetings or the drafting of the manuscript. None of the authors received any individual compensation for their contributions to this work.

Abstract
Background
Diabetes remains the leading cause of diabetic kidney disease (DKD) and end-stage renal disease (ESRD), posing a significant health care burden both globally and in the United Arab Emirates. The coexistence of DKD and cardiovascular risk factors increases morbidity and mortality, necessitating the need for an integrated, evidence-based approach in management.
Methods
In response, a panel of endocrinologists and nephrologists from the United Arab Emirates collaborated to develop regional consensus recommendations focusing on the local clinical needs.
Results
This article focuses on DKD stage 1 to 4, providing practical guidance on screening, diagnosis, referral, glycemic control, and risk factor management to help delay DKD progression and reduce complications. Given the complexity of DKD, additional recommendations covering advanced stages, dialysis, and transplantation will be presented as a forthcoming part of this consensus.
Conclusion
These recommendations support a proactive and comprehensive approach to improve renal–metabolic outcomes and address the escalating burden of DKD in the United Arab Emirates.
Keywords
chronic kidney disease - diabetes mellitus - diabetic kidney disease - end-stage renal disease - reno-metabolic - type 2 diabetesIntroduction
Diabetic kidney disease (DKD), a specific type of chronic kidney disease (CKD) prevalent in people with a history of diabetes, is clinically defined as excessive albuminuria (≥30 mg/g) and/or a progressive decline in kidney function to below 60 mL/min/1.73m2 estimated glomerular filtration rate (eGFR).[1] If untreated, kidney function may continue to decline, leading to end-stage renal disease (ESRD). DKD affects approximately 30% of individuals with type 1 diabetes (T1D) and 40% of those with type 2 diabetes (T2D).[2] In T1D, DKD typically develops after 10 years of diabetes diagnosis, and it is rare for people with T1D to develop kidney disease without retinopathy. In T2D, DKD may already be present at the time of diagnosis, and retinopathy is typically only moderately sensitive and specific for CKD caused by diabetes, as confirmed by a kidney biopsy.[3]
People with DKD also have elevated cardiovascular (CV) risk due to albuminuria, or a decline in eGFR without albuminuria, and high blood pressure (BP) associated with the condition.[4]
DKD can be categorized into two distinct phenotypes: The classical albuminuric phenotype and the non-albuminuric phenotype.[2] Patients with albuminuric DKD may have a higher risk of DKD progression and ESRD incidence compared with those with non-albuminuric DKD.[5] Today, non-albuminuric renal impairment is the prevailing DKD phenotype in patients with T2D who have decreased eGFR.[6] Non-albuminuric DKD presents with reduced kidney function, without albuminuria, suggesting that both the onset and progression of the decline in renal function may also occur independently from the development of albuminuria ([Supplementary Fig. S1] [available in the online version only]).[7] [8]
Prevalence of Diabetic Kidney Disease in the United Arab Emirates
Diabetes
With an overall prevalence of 16% and up to 40% of patients developing DKD each year, diabetes contributes significantly to the United Arab Emirates' annual health care burden. The United Arab Emirates' per-person diabetes expenditure currently exceeds USD 2,000 and is estimated to reach USD 2,099 by 2045.[9]
The Weqaya Program in Abu Dhabi, which screened over 50,000 individuals, reported a diabetes prevalence of 18%. Similarly, the Dubai Health Survey found a prevalence of 19% among Emiratis and 12% among expatriates.[8] Another study reported a diabetes prevalence of 47% among adults aged over 40 years.[10]
Diabetic Kidney Disease
The prevalence of DKD mirrors that of diabetes. Almost one in two United Arab Emirates nationals with T2D has moderately increased albuminuria (formerly microalbuminuria),[11] a key biomarker indicating early DKD.[8] A recent retrospective cross-sectional study in Abu Dhabi identified CKD in 24% of individuals, including 4% in stages 3 to 5 and 2% in stage 1, based on albuminuria alone.[12] A 2017 retrospective study[10] found DKD to be the leading cause of ESRD, accounting for 57% of dialysis patients at the Dubai Hospital HD unit, with 64% among United Arab Emirates nationals and 38% among non-nationals. Another study found DKD in 17% of T2D patients across two diabetes centers in Dubai,[13] while a recent real-world analysis reported a prevalence of CKD ranging from 4% to 20% in various T2D cohorts.[14]
Given the growing burden of DKD in the United Arab Emirates, there is an urgent need for practical and locally relevant guidance to support early detection and management. While international guidelines provide valuable frameworks, they may not fully account for the unique epidemiological patterns, health care infrastructure, and referral dynamics within the United Arab Emirates. To address this gap, a multidisciplinary panel of United Arab Emirates-based endocrinologists and nephrologists came together to develop consensus-driven recommendations. This initiative aimed to standardize the screening, diagnosis, referral, and management of DKD across stages 1 to 4, and ultimately improve the quality of life for people living with diabetes and kidney disease in the United Arab Emirates.
Materials and Methods
In September 2024, a United Arab Emirates-based initiative was launched. A mini-Delphi method was used to achieve consensus among 14 national experts in endocrinology and nephrology. Draft recommendations were developed based on international guidelines (American Diabetes Association, Kidney Disease: Improving Global Outcomes [KDIGO], NICE, UAE Cardiometabolic) and covered key topics, including definitions, screening, treatment, and referral. Experts provided feedback via an online survey, followed by a virtual meeting to review and vote on each statement. Consensus was defined as ≥80% agreement; statements with borderline agreement (∼70%) were revised and re-voted on after further discussion. [Supplementary Material S1] and [S2] (available in the online version only) highlights the salient points (S1) and provides more detailed supporting evidence (S2). Recommendations are presented in the Text Boxes 1 to 15.
Results
Screening and Diagnosis
Recommendation 1: Screening should be performed using both the urine albumin-to-creatinine ratio (UACR) and the eGFR, which together enable a comprehensive assessment of kidney function. Early detection of DKD is fundamental to initiating timely interventions that may slow progression to ESRD and reduce CV morbidity and mortality.
Screening should involve both assessment of eGFR and measurement of UACR. Confirmation of albuminuria, even at levels of 30 to 300 mg/g, requires detection on at least two occasions within a 3- to 6-month period to rule out transient causes, such as fever or uncontrolled hypertension.[15] In high-risk patients, such as those with metabolic syndrome, obesity, hypertension, or CV disease (CVD), more frequent monitoring may be necessary to detect early kidney damage and intervene appropriately.
Recommendation 2: In cases where abnormal findings are confirmed, such as persistent albuminuria or a decline in eGFR, further urine testing is essential to exclude alternative or coexisting non-DKD.
Recommendation 3: In individuals with T2D, screening for DKD should be initiated at diagnosis and conducted at least annually thereafter using both UACR and eGFR. Individuals with T1D should begin screening 5 years following the initial diagnosis.
The frequency of subsequent assessments should be individualized based on baseline kidney function, progression risk, and presence of additional comorbidities.
-
Patients with high-risk profiles, such as those with established CVD, hypertension, or obesity, may warrant more frequent monitoring to ensure early detection of renal or CV complications.
In adults at risk for CKD, we recommend using creatinine-based eGFR ([Fig. 1]). If cystatin C is available, the GFR category should be estimated from the combination of creatinine and cystatin C (creatinine and cystatin C-based estimated glomerular filtration rate).[15] Annual CKD screening is recommended for all patients with diabetes, with earlier and more frequent screening for those with additional risk factors such as hypertension, obesity, or established CVD.[16] The incorporation of cardiovascular risk markers, such as N-terminal pro-B-type natriuretic peptide (NT-proBNP) and high-sensitivity troponin, is recommended to better identify the risk of cardiorenal syndrome.[17] While the wide-reaching benefits of renal screening in people with diabetes are difficult to quantify, screening for CKD in people with diabetes is cost-effective.[18] This evidence aligns with KDIGO recommendations, which support early identification of CKD in at-risk asymptomatic people, particularly when results are used to guide clinical decisions.[15] [19]

Risk Factors for Diabetic Kidney Disease
A variety of metabolic risk factors result in the onset and progression of DKD. Effective management of these risks is crucial for mitigating their contribution to disease progression, identifying patients at risk of progression, and enabling physicians to implement more targeted approaches to managing DKD.[15] [20] Baseline glycated hemoglobin (HbA1c), systolic blood pressure (SBP), proteinuria, serum uric acid, vascular comorbidities, and obesity are significant and independent factors associated with a rapid DKD progression.[21] Elevated body mass index (BMI), waist circumference, and waist-to-height ratio are recognized as independent risk factors for eGFR decline in individuals with normal or reduced eGFR levels.[22] Furthermore, smoking significantly contributes to renal impairment, especially in people with hypertension and T2D, where it increases the risk of developing diabetic nephropathy.[23] [Table 1] summarizes a comparison of key recommendations for managing modifiable DKD risk factors. It has been demonstrated that lower BP levels, as well as lower levels of total cholesterol and triglycerides, are associated with regression from moderate albuminuria to normal UACR, particularly in patients with T2D,[24] while also reducing the risk of progression to severe albuminuria and ESRD.[25] [Supplementary Figure S1] (available in the online version only) demonstrates the acute kidney injury (AKI) induced by medications (adapted from Izzedine et al, 2013[26], and Shahrbaf et al, 2015[27]).
|
Risk factor |
NICE |
KDIGO |
The present consensus |
|---|---|---|---|
|
Glycemic control |
Target blood glucose to reduce HbA1c |
HbA1c ≈7%, individualized |
HbA1c ≈7%, individualized |
|
Hypertension |
BP <140/90 (or 130/80 with kidney/CV risks) |
BP < 120/80 without albuminuria; <130/80 with albuminuria |
BP <120/80 or lower if tolerated |
|
Albuminuria/Proteinuria |
Monitor microalbuminuria (>30 mg/day) |
Routine screening is essential |
Monitor microalbuminuria (>30 mg/day) |
|
Dyslipidemia |
Manage LDL cholesterol |
Statin therapy to reduce risk |
LDL <55 mg/dL for very high risk; ≥50% reduction with high-intensity statin |
|
Obesity |
Manage weight to lower risk |
Emphasize weight control in T2D |
Weight management |
|
Smoking |
Smoking cessation |
Smoking cessation |
Smoking cessation |
|
Nephrotoxic drugs |
Avoid nephrotoxics |
Avoid nephrotoxics; monitor meds |
Avoid nephrotoxics (e.g., NSAIDs, COX2i)[a] |
Abbreviations: BP, blood pressure; CV, cardiovascular; HbA1c, glycated hemoglobin; T2D, type 2 diabetes; LDL: low density lipoprotein, NSAID: non-steroidal anti-inflamatory drug, COX2i: cyclooxygenase-2 inhibitors.
Findings based on international renal guidelines[15] [29] [83] [85] and opinions of the authors of this consensus document.
a Refer to the [Supplementary Fig. S1] (available in the online version only) for more information on nephrotoxic medications and medications to avoid during acute kidney injury.
According to expert consensus, key non-modifiable risk factors include the patient's duration of diabetes, their family history of kidney disease, and potential ethnicity. The risk of DKD rises significantly after 10 to 15 years of diabetes, particularly in individuals with T1D, though both T1D and T2D carry substantial risk. Additionally, experts highlight that South Asians, African-Caribbeans, and Hispanics face a higher risk of developing DKD, an important consideration in regions like the United Arab Emirates, where these ethnic groups form a large proportion of the expatriate population.
Recommendation 4: The progression of DKD is driven by a constellation of modifiable risk factors, including chronic hyperglycemia, hypertension, albuminuria or proteinuria, dyslipidemia, obesity, tobacco use, and exposure to nephrotoxic agents. Rigorous identification and targeted management of these determinants should be prioritized as a central therapeutic strategy to decelerate renal functional decline and attenuate associated cardiovascular morbidity and mortality.
Referral to Nephrology
Prompt detection and referral to nephrology services offer the potential to halt or slow the progression of DKD.[18] Conversely, delayed referrals to a nephrology center for renal replacement therapy (RRT) can worsen the outcomes among CKD patients and increase treatment expenses.[28] [29] [Figure 2] demonstrates the goals of early identification and referral. Several studies have shown that while nephrology referrals increase before dialysis initiation, over half are referred late, typically within 90 days of starting hemodialysis.[29] Similarly, delayed referral to a nephrologist is associated with rising mortality from CKD stages 1 to 4 and an exponential increase in ESRD after CKD stage 3a.[30] Early referrals made 6 to 12 months prior to RRT can potentially delay progression and improve prognosis in CKD patients.[31] [32] An active urinary sediment (containing red or white blood cells or cellular casts) suggests an alternative or additional cause of kidney disease. Patients with refractory hypertension, or those with persistent potassium abnormalities, may benefit from referral to a nephrologist and an endocrinologist. The criteria for referral to nephrology are summarized in [Fig. 3].[15]


Recommendations 5
-
Patients with eGFR <45 mL/min/1.73 m2 or significant albuminuria should be referred to a nephrologist and diabetologist for specialized care and management.
-
Other referral indications include significant albuminuria in diabetes of shorter duration without retinopathy, new-onset proteinuria with decreasing eGFR despite optimal diabetes control, and unexplained low eGFR at initial visit.
Recommendation 6: Ensure timely referral to a nephrologist and a diabetologist to optimize treatment, including potential kidney biopsy, medication adjustments, and planning for RRT. Early identification and referral of patients with DKD to specialist kidney care services have the potential to reverse, delay, or prevent the progression of the disease.
Glycemic Management
Glycemic control has been shown to delay the development of albuminuria, CVD, and DKD progression in patients with diabetes and kidney disease.[33] [34] [35] [36] [37] Glycemic control has been shown to delay the development of albuminuria, CVD, and DKD progression in patients with diabetes and kidney disease.[35] Intensive glycemic control reduces the risk and progression of DKD in both T1D and T2D. The DCCT/EDIC (T1D) and the Kumamoto, UKPDS, VADT, ADVANCE, and ACCORD (T2D) studies reported delayed onset and progression of nephropathy, as well as an association between lower HbA1c levels and reduced albuminuria with intensive glycemic management.[38] [39] [40] [41] [42] [43] [44]
Glycemic Targets
HbA1c should be used as the primary measure of glycemia in patients with diabetes and DKD, except in cases where HbA1c reliability may be limited, such as in advanced renal disease, severe anemia, or concurrent hemoglobinopathies.[40]
Recommendation 7: Each patient's glycemic targets should be individualized based on their stage of DKD, age, comorbidities, and overall health. An HbA1c of 7% is the widely accepted target, although less stringent targets (e.g., <8%) may be appropriate in advanced DKD or in patients at high risk of hypoglycemia. Tight glycemic control may slow CKD progression, but achieving this should be balanced with safety, particularly in the later stages of DKD.
Glycemic Monitoring
Self-monitoring of blood glucose or continuous glucose monitoring (CGM) is advised for all those with DKD to prevent hypoglycemia and improve glycemic variability. Maintaining time in range above 70% is particularly crucial, especially in those with DKD. Intermittent monitoring may suffice for patients with stable DKD and a low risk of hypoglycemia. In contrast, more frequent monitoring is advised for those with advanced DKD or on hypoglycemia-prone therapies, such as insulin or sulfonylureas. HbA1c testing is recommended every 3 months for both early and advanced CKD. However, its reliability decreases in advanced CKD (eGFR <30), and CGM is often beneficial. [Table 2] lists the factors influencing HbA1c measurement in CKD. Findings based on expert opinion are listed as authors of this consensus document.[41]
|
Factor |
Impact on HbA1c measurement |
Influence on HbA1c measurement |
|---|---|---|
|
Iron or vitamin B12 deficiency[42] |
Overestimation |
Decreased RBC turnover leads to longer glycation periods and higher HbA1c |
|
Erythropoietin administration[42] |
Underestimation |
Increased RBC production reduces HbA1c as glycosylation time shortens |
|
Hemodialysis[42] |
Underestimation |
Shortened RBC lifespan in dialysis patients lowers HbA1c levels |
|
Blood urea nitrogen[42] |
Overestimation |
Carbamylated Hb mimics glycated Hb, falsely raising HbA1c |
Abbreviation: HbA1c, glycated hemoglobin.
Findings based on opinion of the authors of this consensus document.
Managing Hypoglycemia Risk by Diabetic Kidney Disease Stage
An expert panel recommends avoiding intensive glucose-lowering strategies in the later stages of DKD (G3b and above) to reduce the risk of hypoglycemia. Instead, prioritize safer glucose-lowering options, such as sodium–glucose cotransporter 2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1 RAs), which provide CV and renal benefits with a lower risk of hypoglycemia. Use medications requiring renal dose adjustments (e.g., insulin, sulfonylureas) with caution in advanced DKD.[42]
Targeted Therapy for Diabetic Kidney Disease
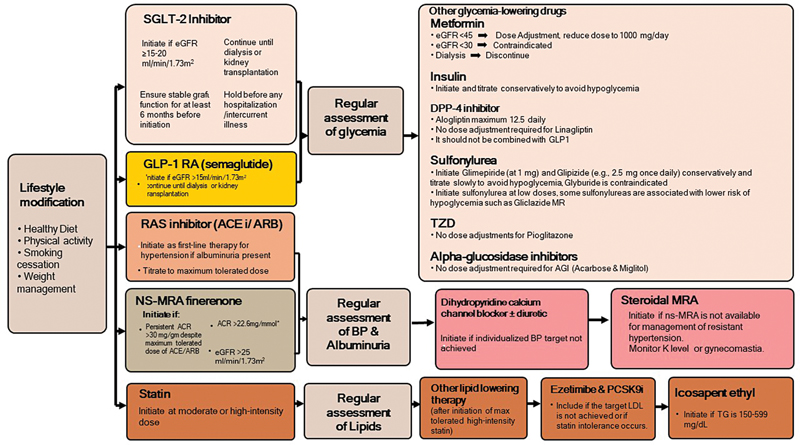
Effective DKD management requires a multifaceted approach, including lifestyle modifications, glycemic control, cardiovascular risk mitigation, and BP regulation with the use of a renin–angiotensin–aldosterone system (RAAS) inhibitor.[43] [44] These foundational strategies represent the established pillars of DKD therapy, along with a fourth emerging pillar—the GLP-1 RAs, which play a significant role in individuals with T2D[45] [46] as illustrated in [Fig. 4].

Sodium–Glucose Cotransporter 2 Inhibitors
SGLT2i were originally approved for use in patients with T2D to improve glycemic control. However, large outcome trials designed to test its cardiovascular safety showed cardiorenal protective benefits.[46] This benefit was subsequently confirmed in landmark trials conducted in patients with albuminuric CKD and T2D. Canagliflozin showed a 30% reduction in the primary outcomes, including ESRD, doubling of serum creatinine, and death from cardiovascular or renal causes, as demonstrated in the CREDENCE trial. A 39% reduction in the primary composite kidney failure outcome was observed with dapagliflozin.[47] Furthermore, empagliflozin therapy led to a lower risk of progression of kidney disease or death from cardiovascular causes than placebo, in a broad range of CKD patients at lower risk of disease progression.[48] [49]
In a collaborative meta-analysis comprising 13 trials with over 90,000 participants, those allocated to an SGLT2i experienced a 37% reduction in the risk of kidney disease progression and a 23% reduction in the risk of AKI, irrespective of diabetes status, compared with placebo.[50] Another meta-analysis highlighted that SGLT2i use in CKD patients was associated with a lower incidence of cardiovascular death, a lower risk of AKI, and treatment discontinuation compared with placebo.[46]
Recommendation 8: Patients with T2D, DKD, and eGFR >20 mL/min/1.73 m2 should receive an SGLT2i regardless of glycemic control to reduce the risk of DKD progression and CVD. A marginal decline in eGFR from baseline is expected within 2 to 4 weeks of starting therapy, but the long-term benefits outweigh this. Once initiated, it is reasonable to continue SGLT2i therapy even if the eGFR declines below 20 mL/min/1.73 m2, unless it becomes intolerable or if kidney replacement therapy (KRT) is initiated.
In patients with CKD stage 4 (eGFR 20–29 mL/min/1.73 m2), SGLT2i have minimal glycemic effects and are primarily used for kidney and cardiovascular protection rather than glycemic control.[51] Additionally, it is important to withhold SGLT2i therapy during prolonged fasting, surgery, or critical medical illness when the risk of ketosis may be elevated.[42] In the EMPA-KIDNEY study, 20% of participants had non-albuminuric DKD and still demonstrated significant benefits from SGLT2i therapy.[49]
Glucagon-Like-Peptide-1 Receptor Agonists
GLP-1 RAs have evolved from promising antihyperglycemic agents to becoming crucial cardiometabolic therapies with notable CV benefits. The SUSTAIN-6 study, which investigated once-weekly semaglutide in patients with eGFR >30 mL/min/1.73 m2, reported improvements in persistent macroalbuminuria, doubling of serum creatinine, and a reduction in creatinine clearance to <45 mL/min or continuous RRT.[52] [53] Additionally, in the REWIND study, dulaglutide therapy in patients with an eGFR greater than 15 mL/min/1.73 m2 resulted in improvements in the incidence of new macroalbuminuria, a sustained decline in eGFR of 30% or more, or the need for chronic RRT.[53] [54] Furthermore, the recent FLOW trial, conducted in individuals with T2D and DKD, suggests that GLP-1 RAs can slow the progression of CKD. It demonstrated a 24% lower risk of the composite primary outcome, which included kidney disease progression, cardiovascular events, and kidney death.[55] Liraglutide, lixisenatide, dulaglutide, and semaglutide have been shown to reduce the development of macroalbuminuria, indicating a renal protective effect.[53] [56] [57]
Recommendation 9: In adults with T2D and DKD, GLP-1 RAs should be initiated either with or after SGLT2i, independent of glycemic control, to attenuate cardiorenal risk synergistically. GLP-1 RAs are additionally indicated in individuals with DKD and obesity to facilitate clinically meaningful weight reduction, particularly when pretransplant BMI thresholds constitute a barrier to renal transplantation eligibility.
Renin–Angiotensin–Aldosterone System Blockers
Activation of the RAAS, driven by the bioactive metabolites angiotensin II and aldosterone, may lead to glomerular injury and proteinuria. Additionally, it contributes to systemic inflammation, generation of reactive oxygen species, and fibrosis in the renal and CV organ systems.[44] Two types of RAAS inhibitors, angiotensin-converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs), are recommended for delaying DKD progression in patients with albuminuria and hypertension.[58]
Recommendation 10: Adults with DKD and high BP should aim for, as tolerated, a target SBP of less than 120 mm Hg. Less intensive BP-lowering therapy should be considered for frail individuals who are at high risk of falls and fractures, have very limited life expectancy, or experience symptomatic postural hypotension.
In a large meta-analysis of 119 randomized controlled trials involving patients with CKD (eGFR <60 mL/min/1.73 m2), the use of RAAS blockade was associated with a reduced risk of progression to ESRD, major adverse cardiovascular events (MACE), and all-cause mortality.[59] [60] The RENAAL trial and the Irbesartan Diabetic Nephropathy trial demonstrated that the use of losartan and irbesartan, respectively, can slow DKD progression.[61] [62] Additionally, the RENAAL also demonstrated a 28% relative reduction in the risk of ESRD.
Recommendation 11: RAAS blockers should be initiated for individuals with DKD and albuminuria (A2-A3) who have diabetes. BP, serum creatinine, and potassium levels should be monitored within 2 to 4 weeks after the initiation or dose adjustment.
ACEi or ARB therapy should be continued unless there is a 30% or greater increase in serum creatinine within 4 weeks of starting or increasing the dose. These medications can be maintained in patients with DKD even if the eGFR falls below 30 mL/min/1.73 m2.
Hyperkalemia associated with RAAS blockers is often manageable through interventions to lower serum potassium levels, rather than reducing the dose or discontinuing the RAAS blocker. A recent individual patient-level data meta-analysis showed a benefit in delaying KRT in patients with eGFR <30 mL/min/1.73 m2.[63] Additionally, two observational studies found poorer outcomes among participants who discontinued RAAS blockers after reaching an eGFR of <30 mL/min/1.73 m2, compared with those who continued the treatment.[64] [65] [Figure 5] depicts the strategy for monitoring of serum creatinine and potassium during ACEi or ARB treatment in DKD.[15] [66]

Non-Steroidal Mineralocorticoid Receptor Antagonists
Non-steroidal mineralocorticoid receptor antagonists (nsMRAs) are recommended in patients with T2D and DKD receiving RAAS inhibition for their potential cardiorenal benefits.[68] [69] They are particularly appropriate for adults who are also at high risk of DKD progression or CV events, as evidenced by persistent albuminuria despite other standard-of-care therapies.[15] To date, two nsMRAs have been approved for clinical use: Finerenone, approved by the U.S. Food and Drug Administration (FDA) in 2021, and esaxerenone, which is approved in Japan.[69] Finerenone is a bulky molecule that acts as an inverse agonist to the mineralocorticoid receptor (MR) by reducing cofactor recruitment, even in the absence of aldosterone. Finerenone exhibits higher selectivity for the MR compared with eplerenone, while retaining potency equivalent to spironolactone.[68]
Recommendation 12: Finerenone, an nsMRA with proven cardiovascular and renal benefits, is recommended for adults with T2D and CKD characterized by
-
An eGFR >25 mL/min/1.73 m2, and
-
Persistent albuminuria UACR >30 mg/g (>3 mg/mmol)
This is despite optimized therapy with a maximally tolerated dose of a RAAS inhibitor (ACEi or ARB). This recommendation is based on high-quality evidence demonstrating a reduction in CKD progression and cardiovascular morbidity.
Finerenone was associated with significantly lower increases in serum/plasma potassium compared with spironolactone, as well as lower incidences of hyperkalemia (serum potassium ≥5.6 mmol/L) or worsening renal function in individuals with T2D.[70] To mitigate the risk of hyperkalemia, it is essential to select individuals with consistently normal serum potassium levels and to monitor potassium levels regularly after initiating an nsMRA.[71] However, a recent post hoc analysis (for 24-hour ambulatory BP) in a subset of patients (n = 240) showed significant reductions in 24-hour, daytime, and night-time SBP with finerenone versus placebo beyond 2 months of treatment.[72]
Recommendation 13: Initiate finerenone according to baseline kidney function.
-
10 mg once daily for patients with eGFR between 25 and 60 mL/min/1.73 m2
-
20 mg once daily for patients with eGFR >60 mL/min/1.73 m2
Dose titration and adjustment should follow monitoring of serum potassium and renal function, with attention to individual tolerability and safety thresholds.
Recommendation 14: In patients with baseline serum potassium between 4.8 and 5.0 mmol/L, initiate finerenone at 10 mg once daily. Monitor serum potassium and renal function within 4 weeks of initiation.
-
If potassium remains ≤5.0 mmol/L, consider uptitrating to 20 mg once daily.
-
If serum potassium rises above 5.0 mmol/L, review the complete medication profile for agents contributing to hyperkalemia (e.g., RAAS inhibitors, potassium-sparing diuretics), and consider the introduction of potassium-lowering strategies, including dietary counseling or pharmacologic agents such as patiromer or sodium zirconium cyclosilicate.
Continue to monitor potassium and renal function regularly throughout treatment, especially after dose adjustments or the addition of interacting medications.
Patients with mild kidney dysfunction (eGFR ≥60 mL/min/1.73 m2) should initiate treatment with the 20 mg/day dose, whereas those with moderate kidney dysfunction (eGFR 25–59 mL/min/1.73 m2) should start with 10 mg/day. Finerenone is not recommended for initiation in patients with severe kidney dysfunction (eGFR <25 mL/min/1.73 m2).[74] Finerenone is also contraindicated in patients receiving a strong cytochrome P450 3A4 inhibitor or those who have adrenal insufficiency.
A sustained decrease of ≥40% in eGFR from baseline, or death from renal causes, was significantly lower with finerenone compared with placebo.[74] Similarly, the primary composite outcome of CVD-related death, non-fatal MI, non-fatal stroke, or heart failure (HF)-related hospitalization was significantly lower with finerenone versus placebo.[70] A significant relative risk reduction of 23% in the composite kidney endpoint was reported for finerenone versus placebo, and of 14% in the composite cardiovascular endpoint, including a 22% relative risk reduction in HF-related hospitalizations, from a prespecified pooled analysis.[75] The ongoing Phase 2 CONFIDENCE study will be important in further defining the role of finerenone in the treatment algorithm for CKD and T2D relative to the SGLT2i.[76]
Recent advancements in DKD treatment options have shown promising results in clinical trials; however, DKD progression remains a continuous challenge.[77] It is reported that combination therapy may delay the progression of CKD by 5.5 years (95% CI, 4.0–6.7) and increase the MACE-free survival by 3.2 years (95% CI, 2.1–4.3) compared with conventional care. Additionally, this approach could improve survival by delaying mortality by 2.4 years (95% CI, 1.4–3).[78] The management of DKD is summarized in a consensus-driven algorithm, as shown in [Fig. 6]. In addition, [Supplementary Table S1] (available in the online version only) provides a summary of the primary outcomes across finerenone, empagliflozin, dapagliflozin, canagliflozin, and semaglutide clinical trials.
Glucose-Lowering Therapies for Use in Patients with Type 2 Diabetes and Diabetic Kidney Disease
In individuals with T2D and established chronic kidney disease (CKD), the selection of glucose-lowering therapies requires careful consideration.[79] As kidney function declines, particularly when eGFR falls below 60 mL/min/1.73 m2, certain medications may become less effective or contraindicated, and dose adjustments are often necessary. [Table 3] summarizes the consensus recommendations for glucose-lowering therapy for use in people with T2D and DKD.
|
Therapy class/drug |
Details |
|---|---|
|
Metformin[15] |
• Recommended initial treatment for patients with T2D and DKD (eGFR 60–30 mL/min/1.73 m2) is dual therapy with metformin and an SGLT2i[15] • Metformin dosing should be adjusted when eGFR falls below 45mL/min/1.73 m2 and discontinued when eGFR <30 mL/min/1.73 m2[15] • Use metformin with dose adjustment in impaired kidney[15] • Metformin elimination half-life of 1.5 to 8.7 hours. About 90% of a dose is excreted within 12 to 24 hours via kidneys. |
|
Sulfonylureas[15] |
• Avoid first-generation agents (e.g., chlorpropamide, tolazamide) due to prolonged half-life and increased hypoglycemia risk. • Choose second-generation agents such as gliclazide (excluding glyburide), primarily metabolized by the liver. • Gliclazide's inactive or weakly active metabolites are excreted in urine, offering a lower risk of hypoglycemia in DKD. |
|
Glinides[79] |
• Repaglinide is preferred due to hepatic metabolism and excretion of inactive metabolites via urine, minimizing hypoglycemia risk. • Can be used with other oral anti-diabetic agents or basal insulin to cover postprandial glucose surges. • Nateglinide is less favored due to active metabolites and higher hypoglycemia risk.[78] |
|
Thiazolidinediones[79] |
• Metabolized by the liver with no renal excretion • Use with caution due to risk of fluid retention, edema, and heart failure, especially in non-dialysis patients. • In patients on pioglitazone, monitor fluid retention every 3 months. |
|
DPP-4 inhibitors[15] |
• Effective in glycemic control and well-tolerated in patients with DKD, including those with concomitant hypertension. • Generally safe in DKD stages G3 to G4; dose adjustments may be required. • Linagliptin, excreted via bile, requires no dose adjustment in dialysis patients. • Sitagliptin requires dose adjustment (DKD G3B: 50 mg/day; DKD G4: 25 mg/day). • Vildagliptin can be used at 50 mg/day in moderate (eGFR:30–50) to severe DKD (eGFR <30). |
|
Alpha-glucosidase inhibitors[79] |
• Take Acarbose and Miglitol at the start of meals to reduce glucose absorption post-meal • Use in stage G3 without dose adjustment • Avoid in stages G4 to G5 due to adverse effect risk. • Miglitol is renally excreted, thus not recommended in patients with significant renal dysfunction. |
|
Insulin[79] |
• Insulin therapy is encouraged in dialysis patients for optimal glycemic control. • Rapid-acting (e.g., aspart, lispro) and long-acting (e.g., glargine, detemir) analogs are unaffected by DKD. • No specific regimen is preferred in the DKD setting. • For T1D, standard treatment is a basal–bolus regimen of 3 daily injections of short-acting insulin with meals combined with one or two injections of long-acting insulin |
Abbreviations: DKD, diabetic kidney disease; eGFR, estimated glomerular filtration rate; SGLT2i, sodium–glucose cotransporter 2 inhibitor; T1D, type 1 diabetes; T2D, type 2 diabetes; DPP-4, dipeptidyl peptidase-4.
The consensus was reached, and recommendations were adapted/modified for regional use based on respective evidence from KDIGO guidelines.[15] [42] [79]
Hypertension and Lipid Management
Hypertension is a major independent risk factor for CKD progression and ESRD, affecting 80% to 85% individuals with CKD.[59] [60] Frequent BP monitoring and therapeutic control of hypertension to protect against DKD progression are crucial.[80] [81] [82] [83] [Table 4] summarizes the evidence-based recommendations for antihypertensive therapy in patients with DKD and albuminuria. The consensus was reached and adapted for regional use based on evidence from KDIGO guidelines, and relevant publications for hypertension management in this group of patients.[15] [42] [79] [Supplementary Table S2] (available in the online version only) details the recommendations relevant to hypertension in CKD patients in the 2021 KDIGO and 2023 ESH Guidelines.
|
Recommendations on antihypertensive therapy in DKD patients with albuminuria |
|---|
|
• Use either an ACEi or an ARB, as first choice antihypertensive therapy for DKD patients with albuminuria (G3–G4, A2-A3) at the maximum tolerated approved dose to ensure optimal nephroprotection. • ACEi with ARB or aliskiren, as combination therapy is not recommended due to increased risks of adverse events, as demonstrated by prematurely terminated outcome trials. • ACEi or ARB therapy should be continued unless there is an increase in serum creatinine by more than 30% within 4 weeks of starting or increasing the dose. These medications can be maintained in patients with DKD even if the eGFR falls below 30 mL/min per 1.73 m2. • Investigate for renovascular disease if eGFR drops consistently or significantly (>30%) and discontinue RAS blockers if necessary.[84] • Be cautious of the increased risk of hyperkalemia associated with RASi in DKD patients, as it is a common reason for dose adjustment or discontinuation. • Use novel potassium binders (e.g., patiromer and sodium zirconium cyclosilicate) to effectively normalize and maintain serum potassium levels in DKD patients on ACEis, ARBs, or MRAs. • Target serum potassium levels <5.5 mmol/L to enable continued optimal treatment with RAAS inhibitor or MRA. |
Abbreviations: ACEi, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; DKD, diabetic kidney disease; eGFR, estimated glomerular filtration rate; MRA, mineralocorticoid receptor antagonist; RAAS, renin–angiotensin–aldosterone system.
The consensus was reached and adapted for regional use based on evidence from KDIGO guidelines, and relevant publications for hypertension management in this group of patients.[15] [42] [85]
DKD exacerbates dyslipidemia and increases the incidence of atherosclerotic CVD.[84] As kidney function declines, lipid abnormalities such as high triglycerides and low density lipoprotein cholesterol (LDL-C), as well as low high density lipoprotein cholesterol (HDL-C), become more pronounced and contribute to atherosclerotic cardiovascular disease (ASCVD) risk.
Recommendation 15: High-intensity statin therapy is recommended as a primary and secondary, respectively, prevention strategy for ASCVD in individuals with DKD. Treatment intensity should be adjusted to target <55 mg/dL LDL-C and at least 50% reduction from baseline for very-high risk individuals.
Statin initiation is recommended for most adults with DKD who are not on dialysis[85]: (a) Adults over 50 years old with eGFR >60 mL/min/1.73 m2, and (b) Adults aged 18 to 49 years with known coronary heart disease, a history of ischemic stroke, or an estimated 10-year risk of coronary heart disease death or non-fatal myocardial infarction greater than 10%. The addition of ezetimibe or a PCSK9 inhibitor is advised to achieve target LDL-C levels (<55 mg/dL or at least 50% reduction from baseline).[86]
In patients with high triglycerides or low HDL-C, lifestyle changes and better glycemic control should be prioritized before using icosapent ethyl. Intensive lipid-lowering may also help slow kidney disease progression, especially in early DKD with albuminuria and preserved eGFR.[80]
Hypertension, dyslipidemia, and T2D are highly prevalent and poorly controlled cardiometabolic diseases in the Middle East, and therapeutic inertia is the major contributor to this suboptimal control.[81] Therapeutic inertia arises from both clinician- and patient-related factors, including concerns about drug side effects, lack of awareness of international guidelines recommendations and new therapeutic options, and perceived complexity of treatment regimens.[82] Through these consensus guidelines, we aim to take a proactive step in overcoming barriers to achieving BP and LDL-C targets by promoting timely treatment intensification, structured care pathways, and supporting greater adherence to evidence-based cardiometabolic management across United Arab Emirates clinical practice.
Management of Obesity in Adults with Stages 3 to 4 Diabetic Kidney Disease
Four FDA-approved antiobesity medications or procedures are currently available for use: GLP-1 RAs, SGLT2i, orlistat, and metabolic surgery.[22] The authors recommend using a combination of SGLT2i and GLP-1 agonists when glycemic control is inadequate in individuals with T2D and DKD. [Supplementary Table S3] (available in the online version only) describes the management of obesity in adults with stage 3 to 4 DKD.
Conclusion
In conclusion, this consensus recommendation sets out a standardized approach for managing DKD in the United Arab Emirates. It highlights the critical role of a multidisciplinary team in ensuring comprehensive care and timely referrals, emphasizing the need for collaboration between nephrologists, endocrinologists, dietitians, and other health care professionals. This collaborative effort and coordination are crucial in advancing DKD management across the United Arab Emirates. Primary health care centers (PHCs) serve as the first point of contact for UACR and eGFR screening, optimization of glycemic and BP control, and reinforcement of adherence to medications before referral to nephrology. DKD screening reminders should be incorporated into PHC electronic records, targeted continuous professional development training should be provided for general practitioners, and these initiatives should be integrated into national chronic disease pathways. To facilitate the dissemination of knowledge, a basic MS PowerPoint Slide Deck with all the recommendations is provided ([Supplementary Material S1] [available in the online version only]).
Given the breadth of the topic, recommendations related to advanced DKD, including dialysis, transplantation, and end-stage kidney care, will be addressed in the forthcoming parts of the DKD guidelines, including additional insights discussed during the consensus meeting.
Conflict of Interest
None declared.
Acknowledgments
The authors would like to acknowledge the leadership role of the Emirates Diabetes and Endocrine Society and Emirates Medical Association – Nephrology and Transplant Society in convening the expert group, MEDCON Middle East, for providing medical writing assistance.
Authors' Contributions
A.B. is the principal author for the manuscript. All authors contributed to the drafting and revising of the manuscript. All authors reviewed the final version of the manuscript and take collective responsibility for all of its contents.
Ethical Approval
No prior ethical approval is needed for a review-type article.
Data Availability Statement
All data, views, and recommendations generated for this initiative are included in this article and its supplementary material files. All primary literature is cited in its bibliography.
-
References
- 1 Satchell SC, Tooke JE. What is the mechanism of microalbuminuria in diabetes: a role for the glomerular endothelium?. Diabetologia 2008; 51 (05) 714-725 . Accessed December 9, 2024 at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2292427/
- 2 Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: Challenges, progress, and possibilities. Clin J Am Soc Nephrol 2017; 12 (12) 2032-2045
- 3 Levey AS, Coresh J, Balk E. et al; National Kidney Foundation. National Kidney Foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann Intern Med 2003; 139 (02) 137-147
- 4 Pálsson R, Patel UD. Cardiovascular complications of diabetic kidney disease. Adv Chronic Kidney Dis 2014; 21 (03) 273-280
- 5 Buyadaa O, Magliano DJ, Salim A, Koye DN, Shaw JE. Risk of rapid kidney function decline, all-cause mortality, and major cardiovascular events in nonalbuminuric chronic kidney disease in type 2 diabetes. Diabetes Care 2020; 43 (01) 122-129
- 6 Gao Z, Zhu Y, Sun X. et al. Establishment and validation of the cut-off values of estimated glomerular filtration rate and urinary albumin-to-creatinine ratio for diabetic kidney disease: A multi-center, prospective cohort study. Front Endocrinol (Lausanne) 2022; 13: 1064665
- 7 Doshi SM, Friedman AN. Diagnosis and management of type 2 diabetic kidney disease. Clin J Am Soc Nephrol 2017; 12 (08) 1366-1373
- 8 Al Awadi F, Hassanein M, Hussain HY, Mohammed H, Ibrahim G, Suliman E. Prevalence of diabetes and associated health risk factors among adults in Dubai, United Arab Emirates: Results from Dubai Household Survey 2019. Dubai Diabetes Endocrinol J 2020; 26 (04) 164-173
- 9 International Diabetes Federation. IDF Diabetes Atlas, 10th edition. Brussels, Belgium: International Diabetes Federation; 2021. . Available at: https://diabetesatlas.org/data/ . Accessed January 3, 2025
- 10 Alalawi F, Ahmed M, AlNour H, Noralla M, Alhadari A. Epidemiology of end-stage renal disease in Dubai: Single-center data. Saudi J Kidney Dis Transpl 2017; 28 (05) 1119-1125
- 11 Arman Rabbani S, Belagodu Sridhar S, Gm Rao P. et al. Prevalence and associations of moderately increased albuminuria in patients with type 2 diabetes in United Arab Emirates. Diabetes Metab Syndr 2020; 14 (06) 1865-1870
- 12 Almadani AK, Ahmed W, Al Obaidli AAK, Holt SG. Gender, age and nationality differences in chronic kidney disease prevalence in the Emirate of Abu Dhabi, UAE. Nephrology (Carlton) 2024; 29 (05) 288-296
- 13 Al-Ghamdi SMG, Bieber B, AlRukhaimi M. et al; GCC-DOPPS Study Group. Diabetes prevalence, treatment, control, and outcomes among hemodialysis patients in the Gulf Cooperation Council countries. Kidney Int Rep 2022; 7 (05) 1093-1102
- 14 Bashier A, Farghaly M, Alali JY. et al. Real-world evaluation of demographics, treatment pattern, and economic burden of heart failure and kidney disease in type 2 diabetes mellitus patient population in Dubai, United Arab Emirates. Dubai Diabetes Endocrinol J 2023; 29 (01) 42-54
- 15 Stevens PE, Ahmed SB, Carrero JJ. et al; Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int 2024; 105 (4S): S117-S314 . Accessed December 10, 2024 at: https://www.kidney-international.org/article/S0085-2538(23)00766-4/fulltext
- 16 Hassanein M, Sabbour H, Al Awadi F. et al. Cardiometabolic guidelines: Cardiovascular risk assessment and management in patients with dysglycemia. Dubai Diabetes Endocrinol J 2023; 29: 67-88 . Karger Publishers. Accessed December 9, 2024 at: https://karger.com/dde/article/29/2/67/854055/Cardiometabolic-Guidelines-Cardiovascular-Risk
- 17 Bansal N, Hyre Anderson A, Yang W. et al. High-sensitivity troponin T and N-terminal pro-B-type natriuretic peptide (NT-proBNP) and risk of incident heart failure in patients with CKD: The Chronic Renal Insufficiency Cohort (CRIC) Study. J Am Soc Nephrol 2015; 26 (04) 946-956 . Accessed December 9, 2024 at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4378105/
- 18 Yeo SC, Wang H, Ang YG, Lim CK, Ooi XY. Cost-effectiveness of screening for chronic kidney disease in the general adult population: A systematic review. Clin Kidney J 2023; 17 (01) sfad137
- 19 Shlipak MG, Tummalapalli SL, Boulware LE. et al; Conference Participants. The case for early identification and intervention of chronic kidney disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2021; 99 (01) 34-47
- 20 Roy S, Schweiker-Kahn O, Jafry B. et al. Risk factors and comorbidities associated with diabetic kidney disease. J Prim Care Community Health 2021;12:21501327211048556. Accessed November 29, 2024 at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8516382/
- 21 Macisaac RJ, Ekinci EI, Jerums G. Markers of and risk factors for the development and progression of diabetic kidney disease. Am J Kidney Dis 2014; 63 (2 Suppl 2): S39-S62
- 22 Friedman AN. Obesity in CKD: A promising path forward. Clin J Am Soc Nephrol 2022; 17 (12) 1817-1819
- 23 Liao D, Ma L, Liu J, Fu P. Cigarette smoking as a risk factor for diabetic nephropathy: A systematic review and meta-analysis of prospective cohort studies. PLoS ONE 2019; 14 (02) e0210213
- 24 Yamanouchi M, Furuichi K, Hoshino J. et al. Two-year longitudinal trajectory patterns of albuminuria and subsequent rates of end-stage kidney disease and all-cause death: A nationwide cohort study of biopsy-proven diabetic kidney disease. BMJ Open Diab Res Care 2021; 9: e002241 . Accessed December 10, 2024: https://drc.bmj.com/content/9/1/e002241
- 25 de Boer IH, Rue TC, Cleary PA. et al; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study Research Group. Long-term renal outcomes of patients with type 1 diabetes mellitus and microalbuminuria: An analysis of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications cohort. Arch Intern Med 2011; 171 (05) 412-420
- 26 Izzedine H, Escudier B, Rouvier P. et al. Acute tubular necrosis associated with mTOR inhibitor therapy: a real entity biopsy-proven. Ann Oncol 2013; 24 (09) 2421-2425
- 27 Ghane Shahrbaf F, Assadi F. Drug-induced renal disorders. J Renal Inj Prev 2015; 4 (03) 57-60
- 28 Vanholder R, Annemans L, Brown E. et al; European Kidney Health Alliance. Reducing the costs of chronic kidney disease while delivering quality health care: A call to action. Nat Rev Nephrol 2017; 13 (07) 393-409
- 29 Blunt I, Bardsley M, Strippoli GFM. Pre-dialysis hospital use and late referrals in incident dialysis patients in England: A retrospective cohort study. Nephrol Dial Transplant 2015; 30 (01) 124-129
- 30 Minutolo R, Lapi F, Chiodini P. et al. Risk of ESRD and death in patients with CKD not referred to a nephrologist: A 7-year prospective study. Clin J Am Soc Nephrol 2014; 9 (09) 1586-1593
- 31 Smart NA, Dieberg G, Ladhani M, Titus T. Early referral to specialist nephrology services for preventing the progression to end-stage kidney disease. Cochrane Database Syst Rev 2014; (06) CD007333
- 32 American Diabetes Association. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021; 44 (Suppl. 01) S73-S84
- 33 Hahr AJ, Molitch ME. Management of diabetes mellitus in patients with CKD: Core Curriculum 2022. Am J Kidney Dis 2022; 79 (05) 728-736 . Accessed November 27, 2024 at: https://linkinghub.elsevier.com/retrieve/pii/S0272638621007629
- 34 King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol 1999; 48 (05) 643-648
- 35 Tran K, Reaven P. Review of the Veteran Affairs diabetes trial: Lessons learned. Rev Endocr Metab Disord 2020; 21 (04) 537-546
- 36 Heller SR. ADVANCE Collaborative Group. A summary of the ADVANCE Trial. Diabetes Care 2009; 32 Suppl 2 (Suppl. 02) S357-S361
- 37 Ginsberg HN. The ACCORD (Action to Control Cardiovascular Risk in Diabetes) Lipid trial: What we learn from subgroup analyses. Diabetes Care 2011; 34 Suppl 2 (Suppl. 02) S107-S108
- 38 Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular outcomes in type 1 diabetes: The DCCT/EDIC Study 30-Year Follow-up. Diabetes Care 2016; 39 (05) 686-693
- 39 Shichiri M, Kishikawa H, Ohkubo Y, Wake N. Long-term results of the Kumamoto Study on optimal diabetes control in type 2 diabetic patients. Diabetes Care 2000; 23 (Suppl. 02) B21-B29
- 40 de Boer IH, Khunti K, Sadusky T. et al. Diabetes management in chronic kidney disease: A Consensus Report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Diabetes Care 2022; 45 (12) 3075-3090
- 41 Gallagher EJ, Bloomgarden ZT, Le Roith D. Review of hemoglobin A1c in the management of diabetes. Journal of Diabetes 2009; 1: 9-17
- 42 Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int 2022; 102 (5S): S1-S127
- 43 Perkovic V, Badve SV, Tuttle KR. Treatment of diabetic kidney disease. UpToDate. Accessed December 9, 2024 at: https://www.uptodate.com/contents/treatment-of-diabetic-kidney-disease
- 44 Triozzi JL, Parker Gregg L, Virani SS, Navaneethan SD. Management of type 2 diabetes in chronic kidney disease. BMJ Open Diab Res Care 2021; 9: e002300 . Accessed November 27, 2024 at: https://drc.bmj.com/lookup/doi/10.1136/bmjdrc-2021-002300
- 45 Agarwal R, Fouque D. The foundation and the four pillars of treatment for cardiorenal protection in people with chronic kidney disease and type 2 diabetes. Nephrol Dial Transplant 2023; 38 (02) 253-257 . Accessed December 10, 2024 at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9923692/
- 46 Mavrakanas TA, Tsoukas MA, Brophy JM, Sharma A, Gariani K. SGLT-2 inhibitors improve cardiovascular and renal outcomes in patients with CKD: A systematic review and meta-analysis. Sci Rep 2023; 13 (01) 15922 . Accessed November 27, 2024 at: https://www.nature.com/articles/s41598-023-42989-z
- 47 Georgianos PI, Eleftheriadis T, Liakopoulos V. Combination therapy with an SGLT-2 inhibitor and finerenone in DKD: Are we there yet?. Eur J Clin Invest 2023; 53 (02) e13864 . Accessed November 27, 2024 at: https://onlinelibrary.wiley.com/doi/abs/10.1111/eci.13864
- 48 Herrington WG, Preiss D, Haynes R. et al. The potential for improving cardio-renal outcomes by sodium-glucose co-transporter-2 inhibition in people with chronic kidney disease: A rationale for the EMPA-KIDNEY study. Clin Kidney J 2018; 11 (06) 749-761
- 49 Herrington WG, Staplin N, Wanner C. et al; The EMPA-KIDNEY Collaborative Group. Empagliflozin in patients with chronic kidney disease. N Engl J Med 2023; 388 (02) 117-127
- 50 Nuffield Department of Population Health Renal Studies Group, SGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists' Consortium. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: Collaborative meta-analysis of large placebo-controlled trials. Lancet 2022; 400 (10365): 1788-1801
- 51 American Diabetes Association Professional Practice Committee. 11. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes-2024. Diabetes Care 2024; 47 (Suppl. 01) S219-S230
- 52 Marso SP, Bain SC, Consoli A. et al; SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016; 375 (19) 1834-1844
- 53 Lin Y, Wang TH, Tsai ML. et al. The cardiovascular and renal effects of glucagon-like peptide 1 receptor agonists in patients with advanced diabetic kidney disease. Cardiovasc Diabetol 2023; 22 (01) 60
- 54 Gerstein HC, Colhoun HM, Dagenais GR. et al; REWIND Investigators. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019; 394 (10193): 121-130
- 55 Perkovic V, Tuttle KR, Rossing P. et al; FLOW Trial Committees and Investigators. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N Engl J Med 2024; 391 (02) 109-121 . Accessed December 10, 2024 at: https://www.nejm.org/doi/full/10.1056/NEJMoa2403347
- 56 Pfeffer MA, Claggett B, Diaz R. et al; ELIXA Investigators. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 2015; 373 (23) 2247-2257
- 57 Marso SP, Daniels GH, Brown-Frandsen K. et al; LEADER Steering Committee, LEADER Trial Investigators. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016; 375 (04) 311-322
- 58 Zhang Y, He D, Zhang W. et al. ACE inhibitor benefit to kidney and cardiovascular outcomes for patients with non-dialysis chronic kidney disease stages 3-5: A network meta-analysis of randomised clinical trials. Drugs 2020; 80 (08) 797-811
- 59 Xie X, Liu Y, Perkovic V. et al. Renin-angiotensin system inhibitors and kidney and cardiovascular outcomes in patients with CKD: A Bayesian network meta-analysis of randomized clinical trials. Am J Kidney Dis 2016; 67 (05) 728-741
- 60 Vendeville N, Lepage MA, Festa MC, Mavrakanas TA. Clinical outcomes of renin-angiotensin-aldosterone blockade in patients with advanced chronic kidney disease: A systematic review and meta-analysis. Can J Cardiol 2024; 40 (09) 1718-1728 . Accessed November 27, 2024 at: https://onlinecjc.ca/article/S0828-282X(24)00192-2/fulltext
- 61 Sarafidis PA, Sharpe CC, Wood E. et al. Prevalence, patterns of treatment, and control of hypertension in predialysis patients with chronic kidney disease. Nephron Clin Pract 2012; 120 (03) c147-c155
- 62 Sarafidis PA, Li S, Chen SC. et al. Hypertension awareness, treatment, and control in chronic kidney disease. Am J Med 2008; 121 (04) 332-340
- 63 Ku E, Inker LA, Tighiouart H, McCulloch C. Initiation of ACE inhibitor and ARBs in patients with advanced CKD: FR-OR44. J Am Soc Nephrol 2023; 34: 40 . Accessed December 11, 2024 at: https://www.researchgate.net/publication/380716999_Initiation_of_ACE_Inhibitor_and_ARBs_in_Patients_with_Advanced_CKD_FR-OR44
- 64 Qiao Y, Shin JI, Chen TK. et al. Association between renin-angiotensin system blockade discontinuation and all-cause mortality among persons with low estimated glomerular filtration rate. JAMA Intern Med 2020; 180 (05) 718-726
- 65 Fu EL, Evans M, Clase CM. et al. Stopping renin-angiotensin system inhibitors in patients with advanced CKD and risk of adverse outcomes: A nationwide study. J Am Soc Nephrol 2021; 32 (02) 424-435
- 66 Bakris GL, Weir MR. Angiotensin-converting enzyme inhibitor-associated elevations in serum creatinine: Is this a cause for concern?. Arch Intern Med 2000; 160 (05) 685-693
- 67 Chen Q, Liang Y, Yan J. et al. Efficacy and safety of non-steroidal mineralocorticoid receptor antagonists for renal outcomes: A systematic review and meta-analysis. Diabetes Res Clin Pract 2023; 195: 110210 . Accessed November 27, 2024 at: https://www.sciencedirect.com/science/article/pii/S0168822722010245
- 68 Lo KB, Rangaswami J, Vaduganathan M. Non-steroidal mineralocorticoid receptor antagonists and cardiorenal outcomes in chronic kidney disease. Nephrol Dial Transplant 2023; 38 (04) 845-854
- 69 Kintscher U, Bakris GL, Kolkhof P. Novel non-steroidal mineralocorticoid receptor antagonists in cardiorenal disease. Br J Pharmacol 2022; 179 (13) 3220-3234
- 70 Pitt B, Filippatos G, Agarwal R. et al; FIGARO-DKD Investigators. Cardiovascular events with finerenone in kidney disease and type 2 diabetes. N Engl J Med 2021; 385 (24) 2252-2263 . Accessed November 27, 2024 at: http://www.nejm.org/doi/10.1056/NEJMoa2110956
- 71 Weir MR, Bakris GL, Pitt B, Agarwal R, Filippatos G, Rossing P. et al. Pharmacotherapy considerations with finerenone in the treatment of chronic kidney disease associated with type 2 diabetes. Am J Health Syst Pharm 2023; 80 (24) e505-18
- 72 Agarwal R, Ruilope LM, Ruiz-Hurtado G. et al. Effect of finerenone on ambulatory blood pressure in chronic kidney disease in type 2 diabetes. J Hypertens 2023; 41 (02) 295-302
- 73 Sarafidis P, Agarwal R, Pitt B. et al; FIDELIO-DKD and FIGARO-DKD Investigators. Outcomes with finerenone in participants with stage 4 CKD and type 2 diabetes: A FIDELITY subgroup analysis. Clin J Am Soc Nephrol 2023; 18 (05) 602-612
- 74 Bakris GL, Agarwal R, Anker SD. et al; FIDELIO-DKD Investigators. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med 2020; 383 (23) 2219-2229
- 75 Agarwal R, Filippatos G, Pitt B. et al; FIDELIO-DKD and FIGARO-DKD investigators. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: The FIDELITY pooled analysis. Eur Heart J 2022; 43 (06) 474-484
- 76 Green JB, Mottl AK, Bakris G. et al. Design of the COmbinatioN effect of FInerenone anD EmpaglifloziN in participants with chronic kidney disease and type 2 diabetes using a UACR Endpoint study (CONFIDENCE). Nephrol Dial Transplant 2023; 38 (04) 894-903
- 77 Singh AK, Farag YMK, Zheng Z, Bakris GL. Clinical trial designs of emerging therapies for diabetic kidney disease (DKD). Postgrad Med 2024; 136 (06) 585-593
- 78 Neuen BL, Heerspink HJL, Vart P. et al. Estimated lifetime cardiovascular, kidney, and mortality benefits of combination treatment with SGLT2 inhibitors, GLP-1 receptor agonists, and nonsteroidal MRA compared with conventional care in patients with type 2 diabetes and albuminuria. Circulation 2024; 149 (06) 450-462
- 79 Sarafidis PA, Persu A, Agarwal R. et al. Hypertension in dialysis patients: A consensus document by the European Renal and Cardiovascular Medicine (EURECA-m) working group of the European Renal Association - European Dialysis and Transplant Association (ERA-EDTA) and the Hypertension and the Kidney working group of the European Society of Hypertension (ESH). J Hypertens 2017; 35 (04) 657-676
- 80 Zac-Varghese S, Mark P, Bain S. et al. Clinical practice guideline for the management of lipids in adults with diabetic kidney disease: Abbreviated summary of the Joint Association of British Clinical Diabetologists and UK Kidney Association (ABCD-UKKA) Guideline 2024. BMC Nephrol 2024; 25 (01) 216
- 81 Almahmeed W, Alabadla Z, Al Awadi F. et al. Improving therapeutic adherence and reducing therapeutic inertia in the management of people with cardiometabolic diseases: A call-to-action from the Middle East. Adv Ther 2025; 42 (03) 1340-1359
- 82 Faggiano A, Gualeni A, Barbieri L. et al. Therapeutic inertia in dyslipidemia management for secondary cardiovascular prevention: Results from the Italian ITACARE-P Network. J Clin Med 2025; 14 (02) 493 . Accessed October 20, 2025 at: https://www.mdpi.com/2077-0383/14/2/493
- 83 NICE. Type 2 diabetes in adults: Management. Accessed August 1, 2025 at: https://www.nice.org.uk/guidance/ng28/resources/type-2-diabetes-in-adults-management-pdf-1837338615493
- 84 Hirano T, Satoh N, Kodera R. et al. Dyslipidemia in diabetic kidney disease classified by proteinuria and renal dysfunction: A cross-sectional study from a regional diabetes cohort. J Diabetes Investig 2022; 13 (04) 657-667
- 85 KDIGO. KDIGO Clinical Practice Guideline for Lipid Management in Chronic Kidney Disease. Kidney International Supplements. 2013. Accessed December 10, 2024 at: https://kdigo.org/wp-content/uploads/2017/02/KDIGO-2013-Lipids-Guideline-English.pdf
- 86 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk | European Heart Journal | Oxford Academic [Internet]. Accessed December 10, 2024 at: https://academic.oup.com/eurheartj/article/41/1/111/5556353
- 87 Chu CD, Lamprea-Montealegre JA, Estrella MM. Too many for too few: Finding appropriate nephrology referrals for patients with CKD that optimize outcomes. Am J Kidney Dis 2022; 79 (03) 330-332 . Accessed December 10, 2024 at: https://www.ajkd.org/article/S0272-6386(21)00994-X/fulltext
Address for correspondence
Publication History
Article published online:
22 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Satchell SC, Tooke JE. What is the mechanism of microalbuminuria in diabetes: a role for the glomerular endothelium?. Diabetologia 2008; 51 (05) 714-725 . Accessed December 9, 2024 at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2292427/
- 2 Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: Challenges, progress, and possibilities. Clin J Am Soc Nephrol 2017; 12 (12) 2032-2045
- 3 Levey AS, Coresh J, Balk E. et al; National Kidney Foundation. National Kidney Foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann Intern Med 2003; 139 (02) 137-147
- 4 Pálsson R, Patel UD. Cardiovascular complications of diabetic kidney disease. Adv Chronic Kidney Dis 2014; 21 (03) 273-280
- 5 Buyadaa O, Magliano DJ, Salim A, Koye DN, Shaw JE. Risk of rapid kidney function decline, all-cause mortality, and major cardiovascular events in nonalbuminuric chronic kidney disease in type 2 diabetes. Diabetes Care 2020; 43 (01) 122-129
- 6 Gao Z, Zhu Y, Sun X. et al. Establishment and validation of the cut-off values of estimated glomerular filtration rate and urinary albumin-to-creatinine ratio for diabetic kidney disease: A multi-center, prospective cohort study. Front Endocrinol (Lausanne) 2022; 13: 1064665
- 7 Doshi SM, Friedman AN. Diagnosis and management of type 2 diabetic kidney disease. Clin J Am Soc Nephrol 2017; 12 (08) 1366-1373
- 8 Al Awadi F, Hassanein M, Hussain HY, Mohammed H, Ibrahim G, Suliman E. Prevalence of diabetes and associated health risk factors among adults in Dubai, United Arab Emirates: Results from Dubai Household Survey 2019. Dubai Diabetes Endocrinol J 2020; 26 (04) 164-173
- 9 International Diabetes Federation. IDF Diabetes Atlas, 10th edition. Brussels, Belgium: International Diabetes Federation; 2021. . Available at: https://diabetesatlas.org/data/ . Accessed January 3, 2025
- 10 Alalawi F, Ahmed M, AlNour H, Noralla M, Alhadari A. Epidemiology of end-stage renal disease in Dubai: Single-center data. Saudi J Kidney Dis Transpl 2017; 28 (05) 1119-1125
- 11 Arman Rabbani S, Belagodu Sridhar S, Gm Rao P. et al. Prevalence and associations of moderately increased albuminuria in patients with type 2 diabetes in United Arab Emirates. Diabetes Metab Syndr 2020; 14 (06) 1865-1870
- 12 Almadani AK, Ahmed W, Al Obaidli AAK, Holt SG. Gender, age and nationality differences in chronic kidney disease prevalence in the Emirate of Abu Dhabi, UAE. Nephrology (Carlton) 2024; 29 (05) 288-296
- 13 Al-Ghamdi SMG, Bieber B, AlRukhaimi M. et al; GCC-DOPPS Study Group. Diabetes prevalence, treatment, control, and outcomes among hemodialysis patients in the Gulf Cooperation Council countries. Kidney Int Rep 2022; 7 (05) 1093-1102
- 14 Bashier A, Farghaly M, Alali JY. et al. Real-world evaluation of demographics, treatment pattern, and economic burden of heart failure and kidney disease in type 2 diabetes mellitus patient population in Dubai, United Arab Emirates. Dubai Diabetes Endocrinol J 2023; 29 (01) 42-54
- 15 Stevens PE, Ahmed SB, Carrero JJ. et al; Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int 2024; 105 (4S): S117-S314 . Accessed December 10, 2024 at: https://www.kidney-international.org/article/S0085-2538(23)00766-4/fulltext
- 16 Hassanein M, Sabbour H, Al Awadi F. et al. Cardiometabolic guidelines: Cardiovascular risk assessment and management in patients with dysglycemia. Dubai Diabetes Endocrinol J 2023; 29: 67-88 . Karger Publishers. Accessed December 9, 2024 at: https://karger.com/dde/article/29/2/67/854055/Cardiometabolic-Guidelines-Cardiovascular-Risk
- 17 Bansal N, Hyre Anderson A, Yang W. et al. High-sensitivity troponin T and N-terminal pro-B-type natriuretic peptide (NT-proBNP) and risk of incident heart failure in patients with CKD: The Chronic Renal Insufficiency Cohort (CRIC) Study. J Am Soc Nephrol 2015; 26 (04) 946-956 . Accessed December 9, 2024 at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4378105/
- 18 Yeo SC, Wang H, Ang YG, Lim CK, Ooi XY. Cost-effectiveness of screening for chronic kidney disease in the general adult population: A systematic review. Clin Kidney J 2023; 17 (01) sfad137
- 19 Shlipak MG, Tummalapalli SL, Boulware LE. et al; Conference Participants. The case for early identification and intervention of chronic kidney disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2021; 99 (01) 34-47
- 20 Roy S, Schweiker-Kahn O, Jafry B. et al. Risk factors and comorbidities associated with diabetic kidney disease. J Prim Care Community Health 2021;12:21501327211048556. Accessed November 29, 2024 at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8516382/
- 21 Macisaac RJ, Ekinci EI, Jerums G. Markers of and risk factors for the development and progression of diabetic kidney disease. Am J Kidney Dis 2014; 63 (2 Suppl 2): S39-S62
- 22 Friedman AN. Obesity in CKD: A promising path forward. Clin J Am Soc Nephrol 2022; 17 (12) 1817-1819
- 23 Liao D, Ma L, Liu J, Fu P. Cigarette smoking as a risk factor for diabetic nephropathy: A systematic review and meta-analysis of prospective cohort studies. PLoS ONE 2019; 14 (02) e0210213
- 24 Yamanouchi M, Furuichi K, Hoshino J. et al. Two-year longitudinal trajectory patterns of albuminuria and subsequent rates of end-stage kidney disease and all-cause death: A nationwide cohort study of biopsy-proven diabetic kidney disease. BMJ Open Diab Res Care 2021; 9: e002241 . Accessed December 10, 2024: https://drc.bmj.com/content/9/1/e002241
- 25 de Boer IH, Rue TC, Cleary PA. et al; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study Research Group. Long-term renal outcomes of patients with type 1 diabetes mellitus and microalbuminuria: An analysis of the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications cohort. Arch Intern Med 2011; 171 (05) 412-420
- 26 Izzedine H, Escudier B, Rouvier P. et al. Acute tubular necrosis associated with mTOR inhibitor therapy: a real entity biopsy-proven. Ann Oncol 2013; 24 (09) 2421-2425
- 27 Ghane Shahrbaf F, Assadi F. Drug-induced renal disorders. J Renal Inj Prev 2015; 4 (03) 57-60
- 28 Vanholder R, Annemans L, Brown E. et al; European Kidney Health Alliance. Reducing the costs of chronic kidney disease while delivering quality health care: A call to action. Nat Rev Nephrol 2017; 13 (07) 393-409
- 29 Blunt I, Bardsley M, Strippoli GFM. Pre-dialysis hospital use and late referrals in incident dialysis patients in England: A retrospective cohort study. Nephrol Dial Transplant 2015; 30 (01) 124-129
- 30 Minutolo R, Lapi F, Chiodini P. et al. Risk of ESRD and death in patients with CKD not referred to a nephrologist: A 7-year prospective study. Clin J Am Soc Nephrol 2014; 9 (09) 1586-1593
- 31 Smart NA, Dieberg G, Ladhani M, Titus T. Early referral to specialist nephrology services for preventing the progression to end-stage kidney disease. Cochrane Database Syst Rev 2014; (06) CD007333
- 32 American Diabetes Association. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021; 44 (Suppl. 01) S73-S84
- 33 Hahr AJ, Molitch ME. Management of diabetes mellitus in patients with CKD: Core Curriculum 2022. Am J Kidney Dis 2022; 79 (05) 728-736 . Accessed November 27, 2024 at: https://linkinghub.elsevier.com/retrieve/pii/S0272638621007629
- 34 King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol 1999; 48 (05) 643-648
- 35 Tran K, Reaven P. Review of the Veteran Affairs diabetes trial: Lessons learned. Rev Endocr Metab Disord 2020; 21 (04) 537-546
- 36 Heller SR. ADVANCE Collaborative Group. A summary of the ADVANCE Trial. Diabetes Care 2009; 32 Suppl 2 (Suppl. 02) S357-S361
- 37 Ginsberg HN. The ACCORD (Action to Control Cardiovascular Risk in Diabetes) Lipid trial: What we learn from subgroup analyses. Diabetes Care 2011; 34 Suppl 2 (Suppl. 02) S107-S108
- 38 Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular outcomes in type 1 diabetes: The DCCT/EDIC Study 30-Year Follow-up. Diabetes Care 2016; 39 (05) 686-693
- 39 Shichiri M, Kishikawa H, Ohkubo Y, Wake N. Long-term results of the Kumamoto Study on optimal diabetes control in type 2 diabetic patients. Diabetes Care 2000; 23 (Suppl. 02) B21-B29
- 40 de Boer IH, Khunti K, Sadusky T. et al. Diabetes management in chronic kidney disease: A Consensus Report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Diabetes Care 2022; 45 (12) 3075-3090
- 41 Gallagher EJ, Bloomgarden ZT, Le Roith D. Review of hemoglobin A1c in the management of diabetes. Journal of Diabetes 2009; 1: 9-17
- 42 Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int 2022; 102 (5S): S1-S127
- 43 Perkovic V, Badve SV, Tuttle KR. Treatment of diabetic kidney disease. UpToDate. Accessed December 9, 2024 at: https://www.uptodate.com/contents/treatment-of-diabetic-kidney-disease
- 44 Triozzi JL, Parker Gregg L, Virani SS, Navaneethan SD. Management of type 2 diabetes in chronic kidney disease. BMJ Open Diab Res Care 2021; 9: e002300 . Accessed November 27, 2024 at: https://drc.bmj.com/lookup/doi/10.1136/bmjdrc-2021-002300
- 45 Agarwal R, Fouque D. The foundation and the four pillars of treatment for cardiorenal protection in people with chronic kidney disease and type 2 diabetes. Nephrol Dial Transplant 2023; 38 (02) 253-257 . Accessed December 10, 2024 at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9923692/
- 46 Mavrakanas TA, Tsoukas MA, Brophy JM, Sharma A, Gariani K. SGLT-2 inhibitors improve cardiovascular and renal outcomes in patients with CKD: A systematic review and meta-analysis. Sci Rep 2023; 13 (01) 15922 . Accessed November 27, 2024 at: https://www.nature.com/articles/s41598-023-42989-z
- 47 Georgianos PI, Eleftheriadis T, Liakopoulos V. Combination therapy with an SGLT-2 inhibitor and finerenone in DKD: Are we there yet?. Eur J Clin Invest 2023; 53 (02) e13864 . Accessed November 27, 2024 at: https://onlinelibrary.wiley.com/doi/abs/10.1111/eci.13864
- 48 Herrington WG, Preiss D, Haynes R. et al. The potential for improving cardio-renal outcomes by sodium-glucose co-transporter-2 inhibition in people with chronic kidney disease: A rationale for the EMPA-KIDNEY study. Clin Kidney J 2018; 11 (06) 749-761
- 49 Herrington WG, Staplin N, Wanner C. et al; The EMPA-KIDNEY Collaborative Group. Empagliflozin in patients with chronic kidney disease. N Engl J Med 2023; 388 (02) 117-127
- 50 Nuffield Department of Population Health Renal Studies Group, SGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists' Consortium. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: Collaborative meta-analysis of large placebo-controlled trials. Lancet 2022; 400 (10365): 1788-1801
- 51 American Diabetes Association Professional Practice Committee. 11. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes-2024. Diabetes Care 2024; 47 (Suppl. 01) S219-S230
- 52 Marso SP, Bain SC, Consoli A. et al; SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016; 375 (19) 1834-1844
- 53 Lin Y, Wang TH, Tsai ML. et al. The cardiovascular and renal effects of glucagon-like peptide 1 receptor agonists in patients with advanced diabetic kidney disease. Cardiovasc Diabetol 2023; 22 (01) 60
- 54 Gerstein HC, Colhoun HM, Dagenais GR. et al; REWIND Investigators. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019; 394 (10193): 121-130
- 55 Perkovic V, Tuttle KR, Rossing P. et al; FLOW Trial Committees and Investigators. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N Engl J Med 2024; 391 (02) 109-121 . Accessed December 10, 2024 at: https://www.nejm.org/doi/full/10.1056/NEJMoa2403347
- 56 Pfeffer MA, Claggett B, Diaz R. et al; ELIXA Investigators. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 2015; 373 (23) 2247-2257
- 57 Marso SP, Daniels GH, Brown-Frandsen K. et al; LEADER Steering Committee, LEADER Trial Investigators. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016; 375 (04) 311-322
- 58 Zhang Y, He D, Zhang W. et al. ACE inhibitor benefit to kidney and cardiovascular outcomes for patients with non-dialysis chronic kidney disease stages 3-5: A network meta-analysis of randomised clinical trials. Drugs 2020; 80 (08) 797-811
- 59 Xie X, Liu Y, Perkovic V. et al. Renin-angiotensin system inhibitors and kidney and cardiovascular outcomes in patients with CKD: A Bayesian network meta-analysis of randomized clinical trials. Am J Kidney Dis 2016; 67 (05) 728-741
- 60 Vendeville N, Lepage MA, Festa MC, Mavrakanas TA. Clinical outcomes of renin-angiotensin-aldosterone blockade in patients with advanced chronic kidney disease: A systematic review and meta-analysis. Can J Cardiol 2024; 40 (09) 1718-1728 . Accessed November 27, 2024 at: https://onlinecjc.ca/article/S0828-282X(24)00192-2/fulltext
- 61 Sarafidis PA, Sharpe CC, Wood E. et al. Prevalence, patterns of treatment, and control of hypertension in predialysis patients with chronic kidney disease. Nephron Clin Pract 2012; 120 (03) c147-c155
- 62 Sarafidis PA, Li S, Chen SC. et al. Hypertension awareness, treatment, and control in chronic kidney disease. Am J Med 2008; 121 (04) 332-340
- 63 Ku E, Inker LA, Tighiouart H, McCulloch C. Initiation of ACE inhibitor and ARBs in patients with advanced CKD: FR-OR44. J Am Soc Nephrol 2023; 34: 40 . Accessed December 11, 2024 at: https://www.researchgate.net/publication/380716999_Initiation_of_ACE_Inhibitor_and_ARBs_in_Patients_with_Advanced_CKD_FR-OR44
- 64 Qiao Y, Shin JI, Chen TK. et al. Association between renin-angiotensin system blockade discontinuation and all-cause mortality among persons with low estimated glomerular filtration rate. JAMA Intern Med 2020; 180 (05) 718-726
- 65 Fu EL, Evans M, Clase CM. et al. Stopping renin-angiotensin system inhibitors in patients with advanced CKD and risk of adverse outcomes: A nationwide study. J Am Soc Nephrol 2021; 32 (02) 424-435
- 66 Bakris GL, Weir MR. Angiotensin-converting enzyme inhibitor-associated elevations in serum creatinine: Is this a cause for concern?. Arch Intern Med 2000; 160 (05) 685-693
- 67 Chen Q, Liang Y, Yan J. et al. Efficacy and safety of non-steroidal mineralocorticoid receptor antagonists for renal outcomes: A systematic review and meta-analysis. Diabetes Res Clin Pract 2023; 195: 110210 . Accessed November 27, 2024 at: https://www.sciencedirect.com/science/article/pii/S0168822722010245
- 68 Lo KB, Rangaswami J, Vaduganathan M. Non-steroidal mineralocorticoid receptor antagonists and cardiorenal outcomes in chronic kidney disease. Nephrol Dial Transplant 2023; 38 (04) 845-854
- 69 Kintscher U, Bakris GL, Kolkhof P. Novel non-steroidal mineralocorticoid receptor antagonists in cardiorenal disease. Br J Pharmacol 2022; 179 (13) 3220-3234
- 70 Pitt B, Filippatos G, Agarwal R. et al; FIGARO-DKD Investigators. Cardiovascular events with finerenone in kidney disease and type 2 diabetes. N Engl J Med 2021; 385 (24) 2252-2263 . Accessed November 27, 2024 at: http://www.nejm.org/doi/10.1056/NEJMoa2110956
- 71 Weir MR, Bakris GL, Pitt B, Agarwal R, Filippatos G, Rossing P. et al. Pharmacotherapy considerations with finerenone in the treatment of chronic kidney disease associated with type 2 diabetes. Am J Health Syst Pharm 2023; 80 (24) e505-18
- 72 Agarwal R, Ruilope LM, Ruiz-Hurtado G. et al. Effect of finerenone on ambulatory blood pressure in chronic kidney disease in type 2 diabetes. J Hypertens 2023; 41 (02) 295-302
- 73 Sarafidis P, Agarwal R, Pitt B. et al; FIDELIO-DKD and FIGARO-DKD Investigators. Outcomes with finerenone in participants with stage 4 CKD and type 2 diabetes: A FIDELITY subgroup analysis. Clin J Am Soc Nephrol 2023; 18 (05) 602-612
- 74 Bakris GL, Agarwal R, Anker SD. et al; FIDELIO-DKD Investigators. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med 2020; 383 (23) 2219-2229
- 75 Agarwal R, Filippatos G, Pitt B. et al; FIDELIO-DKD and FIGARO-DKD investigators. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: The FIDELITY pooled analysis. Eur Heart J 2022; 43 (06) 474-484
- 76 Green JB, Mottl AK, Bakris G. et al. Design of the COmbinatioN effect of FInerenone anD EmpaglifloziN in participants with chronic kidney disease and type 2 diabetes using a UACR Endpoint study (CONFIDENCE). Nephrol Dial Transplant 2023; 38 (04) 894-903
- 77 Singh AK, Farag YMK, Zheng Z, Bakris GL. Clinical trial designs of emerging therapies for diabetic kidney disease (DKD). Postgrad Med 2024; 136 (06) 585-593
- 78 Neuen BL, Heerspink HJL, Vart P. et al. Estimated lifetime cardiovascular, kidney, and mortality benefits of combination treatment with SGLT2 inhibitors, GLP-1 receptor agonists, and nonsteroidal MRA compared with conventional care in patients with type 2 diabetes and albuminuria. Circulation 2024; 149 (06) 450-462
- 79 Sarafidis PA, Persu A, Agarwal R. et al. Hypertension in dialysis patients: A consensus document by the European Renal and Cardiovascular Medicine (EURECA-m) working group of the European Renal Association - European Dialysis and Transplant Association (ERA-EDTA) and the Hypertension and the Kidney working group of the European Society of Hypertension (ESH). J Hypertens 2017; 35 (04) 657-676
- 80 Zac-Varghese S, Mark P, Bain S. et al. Clinical practice guideline for the management of lipids in adults with diabetic kidney disease: Abbreviated summary of the Joint Association of British Clinical Diabetologists and UK Kidney Association (ABCD-UKKA) Guideline 2024. BMC Nephrol 2024; 25 (01) 216
- 81 Almahmeed W, Alabadla Z, Al Awadi F. et al. Improving therapeutic adherence and reducing therapeutic inertia in the management of people with cardiometabolic diseases: A call-to-action from the Middle East. Adv Ther 2025; 42 (03) 1340-1359
- 82 Faggiano A, Gualeni A, Barbieri L. et al. Therapeutic inertia in dyslipidemia management for secondary cardiovascular prevention: Results from the Italian ITACARE-P Network. J Clin Med 2025; 14 (02) 493 . Accessed October 20, 2025 at: https://www.mdpi.com/2077-0383/14/2/493
- 83 NICE. Type 2 diabetes in adults: Management. Accessed August 1, 2025 at: https://www.nice.org.uk/guidance/ng28/resources/type-2-diabetes-in-adults-management-pdf-1837338615493
- 84 Hirano T, Satoh N, Kodera R. et al. Dyslipidemia in diabetic kidney disease classified by proteinuria and renal dysfunction: A cross-sectional study from a regional diabetes cohort. J Diabetes Investig 2022; 13 (04) 657-667
- 85 KDIGO. KDIGO Clinical Practice Guideline for Lipid Management in Chronic Kidney Disease. Kidney International Supplements. 2013. Accessed December 10, 2024 at: https://kdigo.org/wp-content/uploads/2017/02/KDIGO-2013-Lipids-Guideline-English.pdf
- 86 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk | European Heart Journal | Oxford Academic [Internet]. Accessed December 10, 2024 at: https://academic.oup.com/eurheartj/article/41/1/111/5556353
- 87 Chu CD, Lamprea-Montealegre JA, Estrella MM. Too many for too few: Finding appropriate nephrology referrals for patients with CKD that optimize outcomes. Am J Kidney Dis 2022; 79 (03) 330-332 . Accessed December 10, 2024 at: https://www.ajkd.org/article/S0272-6386(21)00994-X/fulltext