

Subscribe to RSS
DOI: 10.1055/s-0045-1814460
Antimicrobial Efficacy of Silver-based Formulations against Fusobacterium nucleatum: A Mini-scoping Review
Authors

Abstract
Fusobacterium nucleatum is a critical periodontal pathogen implicated in biofilm maturation and inflammation in periodontitis. With growing concerns over antibiotic resistance, silver-based antimicrobial agents are emerging as promising alternatives. This minireview aims to evaluate the antimicrobial efficacy and biocompatibility of various silver formulations, including silver nitrate (AgNO3), silver diamine fluoride, silver nanoparticles (AgNPs), and glutathione-stabilized AgNPs (GSH-silver), specifically against F. nucleatum. A systematic literature search (1990–2024) across PubMed, EMBASE, EBSCOhost, and Google Scholar identified five in vitro studies. Key outcome measures included minimum inhibitory concentration (MIC), cytotoxicity, and proinflammatory responses. All formulations demonstrated significant antimicrobial efficacy, with 5 nm AgNPs showing the most potent effect (MIC = 25 µg/mL). Silver(I) carbohydrate complexes and GSH-silver showed enhanced efficacy and reduced cytotoxicity. However, elevated proinflammatory cytokine release was noted with some formulations. Silver-based formulations exhibit potent antimicrobial activity against F. nucleatum, but their inflammatory potential and cytotoxicity warrant further investigation. Future in vivo studies are needed to optimize dosing, assess tissue interactions, and validate the clinical safety of these silver-based formulations.
Keywords
Fusobacterium nucleatum - silver nanoparticles - antimicrobial efficacy - periodontal pathogens - cytotoxicity - glutathione-stabilized silverIntroduction
Biofilms are resilient and dynamic, substratum-attached microbial networks prevalent in nature, particularly in the oral cavity, where over 700 microbial species form multispecies communities on tooth surfaces and in supragingival and subgingival niches.[1] Upon maturation, biofilms develop a well-defined structure that protects resident microbes from antimicrobial agents and host immunity, enabling survival in fluctuating, challenging environments.[2] Early colonizers, such as streptococci and Actinomyces, initially adhere to host oral and dental surfaces, followed by co-adhesion and co-aggregation with other microbial species, leading to biofilm maturation.[1] [2] F. nucleatum, a Gram-negative anaerobe, plays a crucial role in this process and facilitates the formation of mature biofilms.[3] Fusobacterium species and subspecies impact the composition and architecture of supragingival and subgingival biofilms differently.[3] Residing in the anaerobic periodontal pocket, F. nucleatum promotes the adherence and integration of other periodontal microbes, such as Porphyromonas gingivalis, Treponema denticola, and red and orange complex bacteria and fungi, thereby contributing to the structural integrity of the subgingival polymicrobial biofilms.[3]
The periopathogen F. nucleatum has multiple virulence attributes, including adhesins that facilitate attachment to host tissues and other bacteria, hemolytic activity, and hydrogen sulfide production.[4] It also stimulates the production of matrix metalloproteinases (MMPs) by host cells, leading to tissue degradation and loss of periodontal attachment.[4] [5] These factors contribute to its ability to disrupt host immune responses and induce inflammation.[6]
Interactions between bacteria and immune cells are particularly noteworthy. Additionally, F. nucleatum exhibits several mechanisms to evade host immune defenses, which pose a significant challenge in combating this pathogen.[7] It modulates the immune response by inhibiting the activity of neutrophils and other phagocytic cells, reducing their ability to kill the bacteria.[7] [8] This immune evasion enables F. nucleatum to persist within periodontal pockets, contributing to chronic inflammation and tissue destruction.[9]
Thus, F. nucleatum plays a multifaceted role in periodontitis, involving intricate interactions within the subgingival biofilm, immune evasion, virulence attributes, and its function as a bridging organism that enhances the stability and pathogenicity of the biofilm. This makes it a formidable periodontal pathogen.[10] The management of periodontal disease typically involves mechanical debridement, such as scaling and root planning, often supplemented with local or systemic antibiotics.[11] However, the persistent nature of periodontal pathogens and the rise of antibiotic-resistant strains pose significant treatment challenges. These limitations highlight the need for alternative antimicrobial agents to enhance treatment outcomes and reduce disease recurrence.[11]
Silver, recognized for its broad-spectrum antimicrobial properties, has been used in various medical applications, including wound dressings and coatings for medical devices.[12] Its antimicrobial effects are attributed to its ability to disrupt microbial cell membranes, interfere with enzyme functions, and induce oxidative stress within microbial cells.[12]
Silver-based formulations, including silver diamine fluoride (SDF), silver nanoparticles (AgNPs), and silver nitrate (AgNO3), are used to manage dental conditions such as caries and dentine hypersensitivity.[13] Additionally, SDF has been used successfully to reduce gingival inflammation and manage hyperplastic gingivitis.[14] [15] Several studies have demonstrated the antibacterial activity of silver-based compounds against various oral pathogens, including F. nucleatum, as adjunct treatments in periodontal therapy.[16] [17] Recent advances in nanomaterials have refined silver's clinical potential beyond its traditional antibacterial scope. Newer nanoscale composites and silver–organic hybrids demonstrate not only enhanced antimicrobial efficacy but also improved biocompatibility. For instance, reviewed controlled-release silver dressings minimize cytotoxicity, while sustaining antimicrobial ion flux.[18] [19] [20] [21]
However, a gap exists in reviews specifically addressing silver formulations and F. nucleatum. In this systematic review, we aimed to collate studies detailing silver formulations tested as antimicrobials against F. nucleatum, including their potential and limitations.
Methods
Data Sources
A scoping systematic review was conducted using the PubMed, Google Scholar, EMBASE, and EBSCOhost databases to identify relevant English-language RCTs, in vitro and ex vivo studies from peer-reviewed journals.
Search Terms
The following search terms were used to select qualifying studies from the databases, covering articles published between January 1, 1990 and January 31, 2024: (“In Vitro Techniques”[MeSH] AND “Periodontitis/microbiology”[MeSH]) AND (“Silver”[MeSH] OR “Silver Nitrate”[MeSH] OR “Silver Nanoparticles”[MeSH] OR “Silver Diamine Fluoride”[MeSH]) AND (“Microbial Sensitivity Tests”[MeSH] OR “Colony Count, Microbial”[MeSH] OR “Minimum Inhibitory Concentration”[MeSH])
“Antimicrobial activity of silver against periodontal pathogens” AND “Silver nitrate” AND “Periodontitis”
(“in vitro study” AND “Periodontal pathogen”) AND (“Silver nitrate” OR “Silver nanoparticle” OR “Silver diamine fluoride”) AND (“Minimum inhibitory concentration” OR “Bacterial colony count” OR “Antibacterial efficacy”)
(“In vitro assay” AND “Periodontal pathogens”) AND (“Silver compounds” OR “Silver nitrate antimicrobial” OR “Silver nanoparticles antibacterial” OR “Silver diamine fluoride periodontitis”) AND (“Microbial sensitivity” OR “Minimum inhibitory concentration” OR “Antibacterial activity” OR “Cytotoxicity and inflammation assays”).
Focused Question
What is the antimicrobial efficacy of various silver-based formulations against Fusobacterium nucleatum, and what are their potential advantages and limitations in periodontal therapy?
Outcome Measure
To evaluate and summarize the antimicrobial efficacy of different silver-based formulations (e.g., silver nitrate, silver diamine fluoride, silver nanoparticles, and silver(I) carbohydrate complexes) against Fusobacterium nucleatum.
Study Selection
Inclusion Criteria
Studies were included if they met the following criteria:
-
Clinical trials, in vitro, in vivo, and ex vivo studies assessing the antimicrobial efficacy of silver-based compounds against periodontal pathogens, specifically F. nucleatum.
-
Detailed interventions specifying concentrations and methods of application.
-
Quantitative data on antimicrobial efficacy (e.g., minimum inhibitory concentration [MIC] values, CFU reduction).
-
Qualitative data on cytotoxicity and inflammatory responses, if available.
-
Peer-reviewed journal articles.
-
Articles published in English.
Exclusion Criteria
Studies were excluded if they met any of the following criteria:
-
Studies assessing the antimicrobial efficacy of silver-based compounds against periodontal pathogens other than F. nucleatum.
-
Studies that did not align with the predetermined study objectives or were limited to abstracts, reviews, or commentaries.
-
Studies with unspecified or unclear intervention methods or concentrations.
-
Studies lacking quantitative measures of antimicrobial efficacy.
Data Search and Data Analysis
We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews (PRISMA-ScR) guidelines to ensure a systematic approach.[22] [Fig. 1] illustrates the search strategy and the outcomes. A meta-analysis was not feasible due to the heterogeneity in silver compound formulations and concentrations, complicating data pooling for quantitative analysis.

During the initial phase of our three-step electronic data search and analysis, we (N.B., K.S.F., A.K., and I.K.) assessed the titles and abstracts of relevant studies to identify those meeting the predefined inclusion criteria. In the second phase, a detailed examination of the full texts of the identified articles was conducted by the reviewers (A.K. and I.K.) to gain a comprehensive understanding of the data. This rigorous analysis ensured that the selected studies met the eligibility criteria and that the reported outcomes aligned with our objectives. Additionally, a backward search was performed by K.S.F. and N.B., scrutinizing the references of the included studies to identify any other relevant research.
In the final phase, the reviewers (N.B. and A.K.) extracted and evaluated data from the selected studies. The specific characteristics of each included study, such as study setting, samples, intervention, and country, were recorded using the Cochrane model. Other factors, such as sample size, evaluation time, assessment methods, and study conclusions, were systematically examined to effectively synthesize the findings.
For managing the identified manuscripts, bibliographic software EndNote version 12 (Clarivate Analytics, USA) was used. [Table 1] summarizes the characteristics of the included in vitro trials and their findings regarding the antimicrobial efficacy of silver-based formulations against F. nucleatum. This table provides a concise overview of the key findings of each study. [Table 2] presents a quantitative cross-study comparison, consolidating numerical data and threshold values to illustrate the heterogeneity observed in MIC ranges, nanoparticle dimensions, and cytotoxicity outcomes.
Abbreviations: HGF, human gingival fibroblast; NA, not available.
Quality and Overall Risk of Bias Assessment of the Included Reports
Two researchers (A.K. and I.K.) independently assessed the quality of the reports included and the overall risk of bias. In case of discrepancies, the third and fourth reviewers (N.B. and K.S.F., respectively) were consulted to reach a consensus. The quality of the selected studies was evaluated individually using the Quality Assessment Tool for In Vitro Studies (QUIN Tool).[23] This evaluation considered 12 criteria: clearly stated aims/objectives, detailed sample size calculation, comprehensive explanation of sampling techniques, information on comparison groups, detailed methodology, operator details, randomization, outcome measurement methods, outcome assessor details, blinding, statistical analysis, and result presentation. Each criterion was scored as follows: adequately specified (score = 2), not adequately specified (score = 1), not specified (score = 0), or not applicable (NA). The final score for each study was calculated by adding the scores of the applicable criteria. This score was then used to categorize studies as high (<50%), medium (50 to 70%), or low risk (>70%) of bias. The risk of bias was calculated using the formula: Final score = (Total score × 100)/(2 × number of applicable criteria) ([Table 3]). Studies receiving >70% of total possible points were classified as “low risk,” reflecting complete methodological reporting (for instance, Spacciapoli et al, Reise et al). Scores between 50 and 70% indicated “moderate risk,” often due to partial omission of operator randomization or blinding (for example, Zorraquín-Peña et al). None scored <50%, indicating generally acceptable methodological rigor.
Abbreviation: NA, not applicable.
Notes: Score: adequately specified: 2 points; inadequately specified: 1 point; not specified: 0 points. Bias: low risk (L) > 70%; medium risk (M) between 70 and 50%; high risk (H) < 50%.
Results
The reviewed studies[24] [25] [26] [27] [28] evaluated the antimicrobial efficacy of various silver-based compounds against periodontal pathogens. All studies employed an in vitro assay design to test the effectiveness of metallic silver salts[24] [26] [27] and silver nanoparticles[25] [28] against different strains of bacteria relevant to periodontal diseases.
Antimicrobial Efficacy of Metallic Silver Salts Against F. Nucleatum
In 2001, Spacciapoli et al tested metal ions such as silver nitrate, copper chloride, and zinc chloride, at concentrations ranging from 0.5 to 50 mg/mL.[24] These experiments, conducted in phosphate-buffered saline and human serum to mimic periodontal pocket conditions, revealed that silver nitrate exhibited strong antimicrobial activity against all tested periodontal pathogens, including F. nucleatum, at a concentration of 0.5 mg/mL, achieving at least a 3 log10 reduction in CFU/mL. The authors suggested that the antimicrobial activity of silver might be due to its ability to bind to essential enzyme sulfhydryl groups, thereby disrupting bacterial functions. Over a decade later, Reise et al (in 2016)[26] evaluated silver(I) carbohydrate complexes and silver nitrate using MIC and agar diffusion assays at concentrations of 10 and 20 mM. Their observations indicated that silver(I) carbohydrate complexes were more effective than AgNO3. The antimicrobial effects of silver were attributed to its interactions with bacterial DNA, cell membrane destruction, and inhibition of essential enzymes. Recently, Rams et al[27] tested SDF at concentrations of 38 and 19% on freshly isolated subgingival biofilm samples from adults with severe periodontitis. The results revealed that 87.5% of the subgingival samples were culture-negative for periodontal pathogens following exposure to either 38 or 19% SDF, with both concentrations significantly reducing total viable counts compared with the controls. Furthermore, the study by Rams et al was the only study to test multispecies biofilms, underscoring the need for future multispecies models.
Antimicrobial Efficacy of Silver Nano-particles Formulations Against F. Nucleatum
Zhong Lu et al[25] synthesized silver nanoparticles with mean sizes of approximately 5, 15, and 55 nm using reduction and hydrothermal methods. The antibacterial efficacy of these nanoparticles was assessed by colony counting and determination of the minimum inhibitory concentration, which revealed significant activity. Notably, the smallest particles (5 nm) exhibited the highest efficacy, with an MIC value of 25 µg/mL against F. nucleatum. The researchers suggested that Ag-NPs attach to bacterial cell membranes, disrupt membrane permeability, potentially penetrate inner membranes, and inactivate respiratory chain dehydrogenases. Additionally, the increased surface area of the smaller nanoparticles enhances their interaction with bacterial cells.
Another study by Zorraquín-Peña et al[28] investigated glutathione-stabilized silver nanoparticles (GSH-Ag-NPs) at Ag+ ion concentrations ranging from 3.08 to 98.50 µg/mL. The results demonstrated significant antibacterial activity of GSH-Ag-NPs against F. nucleatum. However, doses higher than 24.63 µg/mL were required to achieve a significant inhibition (p < 0.01) of F. nucleatum growth.
Cytotoxicity and Inflammatory Responses of the Silver Formulations on Periodontal Tissue
Zorraquín-Peña et al[28] investigated the cytotoxicity of glutathione-stabilized silver nanoparticles on a human gingival fibroblast cell line using MTT assay, at Ag concentrations of 6.16, 12.31, and 24.63 µg/mL after 30 minutes and 24 hours of exposure. At a concentration of 6.16 µg/mL, GSH-Ag-NPs did not exhibit significant cytotoxicity, maintaining cell viability above 90%. However, cell viability decreased substantially at concentrations of 12.31 and 24.63 µg/mL, with reductions of 25 and 40%, respectively, compared with control cells.
Similarly, Reise et al[26] evaluated the cytocompatibility of silver(I) carbohydrate complexes and AgNO3 on human gingival fibroblasts. AgNO3 demonstrated cytotoxic effects at concentrations exceeding 0.02 mM. In contrast, the silver complex tris[2-(β-D-thio-glucopyranosyl) ethyl]-amine-silver(I)-nitrate (complex 3) exhibited a significantly reduced cytotoxicity, being approximately 10 times less toxic to human gingival fibroblasts compared with AgNO3.
Inflammatory Response of Silver-based Formulations
Zorraquín-Peña et al exclusively studied the inflammatory response induced by glutathione-stabilized silver nanoparticles by measuring the production of proinflammatory cytokines IL-6, IL-8, and tumor necrosis factor-α (TNF-α) using ELISA after 30 minutes and 24 hours of exposure.[28] GSH-AgNPs caused upregulation of IL-6, IL-8, and TNF-α expression compared with control cells, with higher levels observed after 24 hours than after 30 minutes of exposure. Notably, IL-8 production was significantly higher than IL-6 and TNF-α. The highest IL-6 production occurred at a concentration of 6.16 µg/mL, while IL-8 and TNF-α release peaked at 3.08 µg/mL. At concentrations affecting cell viability (≥12.31 µg/mL), an inverse relationship was observed between cytokine production and cell viability.
Discussion
The results from the reviewed studies collectively demonstrate that silver-based formulations, both in nano- and non-nano sizes, exhibit significant antimicrobial activity against periodontal pathogens, including F. nucleatum. However, different formulations, including silver nitrate, silver nanoparticles, silver diamine fluoride, and silver(I) carbohydrate complexes, each present unique advantages and challenges in managing periodontal infections. To the best of our knowledge, this is the first comprehensive literature review examining the antimicrobial efficacy of silver formulations against F. nucleatum specifically.
Zhong Lu et al[25] investigated the antimicrobial efficacy of silver nanoparticles, with a particular emphasis on their size and concentration. Their findings underscored the significance of nanoparticle size in enhancing antibacterial activity. This increased potency is primarily attributed to the smaller nanoparticles' superior ability to penetrate bacterial cells more efficiently and their larger surface area for interaction.[29] These properties enable silver nanoparticles to disrupt bacterial cells more effectively, inhibiting critical metabolic and genetic functions and thereby reducing bacterial growth.[29]
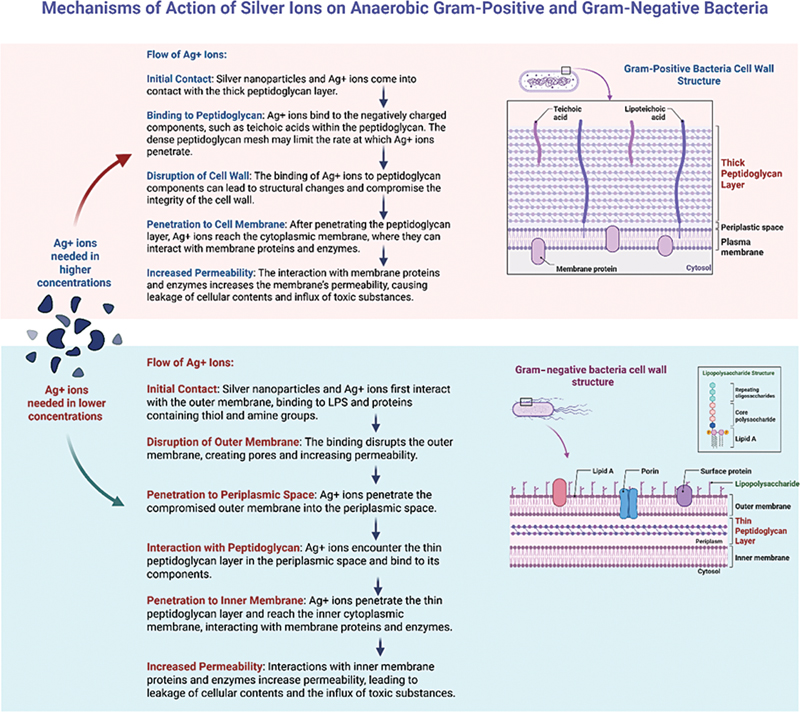
In the case of F. nucleatum and A. actinomycetemcomitans, both Gram-negative anaerobic bacteria, the observed MIC was 25 µg/mL. This is lower than the 50 µg/mL required for Gram-positive Streptococcus species. The difference in MICs can be attributed to variations in the cell wall structures. Gram-negative bacteria possess a thin peptidoglycan layer, an outer membrane containing proteins with thiol and amine groups and negatively charged lipopolysaccharides.[30] These structural components possibly enhance the permeability of the bacterial cell wall to silver ions, facilitating more effective antimicrobial action.[30] In contrast, Gram-positive bacteria have thicker peptidoglycan layers, which require higher doses of silver ions for effective penetration and binding.[30] Thus, the structural differences between Gram-negative and Gram-positive bacteria significantly influence their susceptibility to silver nanoparticle treatment. Gram-negative bacteria, with their thinner cell walls and accessible outer membranes, are more susceptible to the antimicrobial effects of nano-sized silver particles, possibly resulting in a lower MIC for these organisms ([Fig. 2]).
Our systematic review highlights the promising role of glutathione (GSH)-stabilized silver nanoparticles in periodontal therapy due to their multifaceted benefits. GSH, a potent antioxidant, plays a crucial role in mitigating the cytotoxic effects induced by nano-silver particles.[31] This protection occurs through the binding of silver components to the thiol (-SH) group present in GSH, which neutralizes the free silver ions released upon application. This interaction not only stabilizes silver nanoparticles at the nanoscale but also reduces their reactivity, minimizing potential cellular damage and inflammatory responses.[31]
Furthermore, the structural stabilization provided by GSH helps prevent silver from penetrating membranous surfaces, which could otherwise lead to weakened mitochondrial membranes, electron leakage, and increased production of reactive oxygen species (ROS).[31] [32] Additionally, GSH's antioxidant properties are beneficial for managing oxidative stress within periodontal tissues. By scavenging ROS, such as hydrogen peroxide (H2O2) and superoxide (O2 −), GSH helps counteract oxidative damage, thereby preserving cellular integrity.[31] [33] This mechanism is critical in protecting periodontal tissues from hyperreactivity-induced reactions caused by silver nanoparticles.[31] [32] [33]
Moreover, GSH has been implicated in regenerative processes essential for tissue repair,[34] a desirable outcome of bacterial removal facilitated by silver interactions.[33] One of the key regenerative functions of GSH is collagen synthesis,[34] which is crucial for the structural integrity of periodontal tissues. GSH reactivates vitamin C, a cofactor necessary for the hydroxylation of proline and lysine residues on collagen fibrils, leading to the formation of mature and strengthened collagen fibers.[34]
Despite the promising theoretical advantages, the practical applications of GSH-stabilized nano-silver have potential drawbacks. Reports indicate an elevation in inflammatory markers, such as interleukins (IL-6 and IL-8) and TNF-α, as observed by Zorraquín-Peña et al.[28] This cytokine response indicates a potential proinflammatory effect of the nanoparticles, which could undermine their therapeutic benefits.[32] Various confounding factors, such as nanoparticle size, duration of administration, and the ratio of GSH and nano-silver particles, may have influenced these outcomes.[33] Although the biochemical synergy between GSH and nano-silver is theoretically promising, its clinical efficacy and safety require extensive investigation. Addressing these factors will be essential for optimizing the therapeutic application of GSH-stabilized silver nanoparticles in the treatment of periodontitis. Therefore, further studies are necessary to comprehensively understand the interactions and effects of GSH-stabilized nano-silver on periodontal therapy.
Similarly, Reise et al[26] explored the potential for Ag+ stability with an alternate carbohydrate complement, where silver–carbohydrate complexes were created through thio-ether binding to silver nitrate. Cytotoxicity was significantly reduced in observed human gingival fibroblasts (HGF), possibly due to the stabilization of AgNO3 through a controlled release response via a weaker thio-ether bond.[35] This reduced cytotoxicity underscores the safety and feasibility of these complexes for potential clinical applications. Another intriguing characteristic of increased water solubility was noted in this study,[26] which appeared to promote more widespread distribution of AgNO3. Although not explicitly nano-size, these complexes exhibited relevant antimicrobial efficiency against peri-pathogens, including F. nucleatum. Although Reise et al's[26] in vitro study model demonstrated the significant antimicrobial efficacy and reduced cytotoxicity of silver(I) carbohydrate complexes, they did not assess their proinflammatory effects. Therefore, further studies are warranted to evaluate the potential proinflammatory responses associated with these compounds. Understanding the inflammatory impact is crucial to ensure their safe and effective application in clinical settings.
The reviewed metallic silver salts, including AgNO3, 38% SDF, and 19% SDF, also demonstrated significant antimicrobial efficacy, notably reducing the viable counts of F. nucleatum. The cytotoxic impact of SDF on HGFs is well-established.[32] However, the reviewed studies[24] [26] [27] did not investigate the safety of silver salts, particularly their cytotoxicity and inflammatory response in periodontal tissues, alongside their antimicrobial efficacy. Numerous studies support the cytotoxicity of HGFs. For instance, in 1998, Hidalgo et al[36] found that silver nitrate exhibited cytotoxicity to cultured fibroblasts at a concentration of 14 × 10−5%, with a contact time of 2 hours. In another in vitro study, Zhang et al[37] demonstrated that 0.01% SDF was cytotoxic to HGF, with this cytotoxic effect persisting even after 9 weeks of rinsing with artificial saliva. In support of these observations, Ho et al[38] recently reported that SDF toxicity to HGFs was instantaneous and severe. After applying 1 μL of 0.394% SDF, the HGF attachment process was disrupted immediately. Histological evaluations of the treated tissues revealed apoptotic cells in the epithelium and the upper half of the connective tissue. Given the complex structure of periodontal tissues, which include components such as gingival epithelium, connective tissue, and alveolar bone, it is crucial to understand how these tissues respond to cytotoxic agents.[39] Studying the cytotoxicity and inflammatory responses of these tissues is essential, as they play a significant role in the healing of periodontal destruction and supporting bone regeneration.[39] A comprehensive understanding of these responses will help develop safer and more effective treatments that combat microbial pathogens while promoting tissue regeneration and periodontal health.
Review limitations: We acknowledge that this review is limited by the relatively small number of studies included in the analysis. The limitation stems primarily from the scarcity of research specifically addressing the antimicrobial efficacy of silver against Fusobacterium nucleatum. The purpose of this mini-scoping review was not to provide an exhaustive synthesis but rather to map the existing evidence, identify research gaps, and encourage further investigation. We recognize that the limited scope of current research underscores the need for broader and more diverse investigations in this field, and we hope that our review aims to encourage such advancements.
MIC values ranged from 25 to 500 µg/mL (particle sizes 5–55 nm) ([Table 2]). Smaller nanoparticles produced stronger antimicrobial activity but also variable cytotoxic thresholds. This needs further research. Another limitation of the studies reviewed is that all were conducted in vitro, which may not fully replicate the complex environment of periodontal pockets. The physiological conditions, biofilm structure, and interactions with host tissues in vivo can differ significantly from those in laboratory settings. Additionally, the concentrations of silver formulations varied widely across studies, ranging from microgram to milligram levels. These variations could affect the comparability and generalizability of the results. Moreover, the duration of exposure to the silver formulations was not uniform, ranging from 30 minutes to 24 hours, which may have affected the consistency of the results and their applicability in clinical settings.
Fibroblasts were the only mammalian cell type evaluated; no studies included epithelial, osteoblastic, or immune models. Future work should assess these to capture tissue-specific cytotoxicity. Previous studies have also reported the cytotoxic effects of silver formulations on human gingival fibroblasts at specific concentrations. For instance, AgNO3 demonstrated cytotoxicity at concentrations exceeding 0.02 mM, and silver diamine fluoride shows cytotoxicity at concentrations as low as 0.01%. However, except for one study, none of the reviewed articles evaluated the inflammatory responses to silver formulations, a crucial factor for understanding their safety and efficacy in periodontal therapy.
Clinical Relevance
Scientific Rationale for the Study
F. nucleatum is a key periodontal pathogen contributing to biofilm maturation and chronic inflammation. Silver-based antimicrobials offer an alternative to conventional antibiotics, thereby helping overcome rising resistance.
Principal Findings
All reviewed silver formulations showed significant in vitro efficacy against F. nucleatum. Glutathione-stabilized silver nanoparticles and silver(I) carbohydrate complexes exhibited reduced cytotoxicity. Among all formulations, GSH-AgNPs and Ag(I) carbohydrate complexes exhibited the best efficacy–biocompatibility profile and hold promise for periodontal applications.
Practical Implications
Silver-based agents hold promise for adjunctive periodontal therapy. Yet, their safety profiles, especially regarding cytotoxicity and inflammation, require further in vivo validation to guide clinical applications.
Conclusion
The reviewed studies collectively highlight the significant antimicrobial potential of silver-based formulations against F. nucleatum, a key periodontal pathogen. Despite promising in vitro results, the cytotoxicity and inflammatory responses associated with various silver formulations underscore the necessity for more comprehensive in vivo studies. Further research should focus on standardizing the concentration and exposure times of silver formulations, as well as investigating their interactions with host tissues in vivo. Additionally, exploring combination therapies could help enhance the therapeutic potential of silver while mitigating its adverse effects. Addressing these challenges will be crucial for translating the antimicrobial properties of silver into effective and safe clinical applications against periodontal pathogens.
Conflict of Interest
None declared.
Data Availability Statement
The manuscript includes all the data analyzed in this study. The corresponding authors can be contacted for further inquiries.
-
References
- 1 Marsh PD. In sickness and in health—what does the oral microbiome mean to us? An ecological perspective. Adv Dent Res 2018; 29 (01) 60-65
- 2 Zhao A, Sun J, Liu Y. Understanding bacterial biofilms: from definition to treatment strategies. Front Cell Infect Microbiol 2023; 13: 1137947
- 3 Prucsi Z, Płonczyńska A, Potempa J, Sochalska M. Uncovering the oral dysbiotic microbiota as masters of neutrophil responses in the pathobiology of periodontitis. Front Microbiol 2021; 12: 729717
- 4 Groeger S, Zhou Y, Ruf S, Meyle J. Pathogenic mechanisms of Fusobacterium nucleatum on oral epithelial cells. Front Oral Health 2022; 3: 831607
- 5 Suzuki R, Kamio N, Sugimoto K. et al. Periodontopathic bacterium Fusobacterium nucleatum affects matrix metalloproteinase-9 expression in human alveolar epithelial cells and mouse lung. In Vivo 2022; 36 (02) 649-656
- 6 Llama-Palacios A, Potupa O, Sánchez MC, Figuero E, Herrera D, Sanz M. Proteomic analysis of Fusobacterium nucleatum growth in biofilm versus planktonic state. Mol Oral Microbiol 2020; 35 (04) 168-180
- 7 Chen Z, Huang L. Fusobacterium nucleatum carcinogenesis and drug delivery interventions. Adv Drug Deliv Rev 2024; 209: 115319
- 8 Muchova M, Kuehne SA, Grant MM. et al. Fusobacterium nucleatum elicits subspecies-specific responses in human neutrophils. Front Cell Infect Microbiol 2024; 14: 1449539
- 9 Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation. Nat Rev Immunol 2015; 15 (01) 30-44
- 10 Chen Y, Shi T, Li Y, Huang L, Yin D. Fusobacterium nucleatum: the opportunistic pathogen of periodontal and peri-implant diseases. Front Microbiol 2022; 13: 860149
- 11 Herrera D, van Winkelhoff AJ, Matesanz P, Lauwens K, Teughels W. Europe's contribution to the evaluation of the use of systemic antimicrobials in the treatment of periodontitis. Periodontol 2000 2023; . Epub ahead of print
- 12 Sim W, Barnard RT, Blaskovich MAT, Ziora ZM. Antimicrobial silver in medicinal and consumer applications: a patent review of the past decade (2007–2017). Antibiotics (Basel) 2018; 7 (04) 93
- 13 Fakhruddin KS, Egusa H, Ngo HC, Panduwawala C, Pesee S, Samaranayake LP. Clinical efficacy and the antimicrobial potential of silver formulations in arresting dental caries: a systematic review. BMC Oral Health 2020; 20 (01) 160
- 14 Lim GXD, Yang J. Effect of silver diamine fluoride on hyperplastic gingivitis in an adult with intellectual disability—a case report. Spec Care Dentist 2022; 42 (01) 73-79
- 15 Zheng FM, Yan IG, Duangthip D, Gao SS, Lo ECM, Chu CH. Silver diamine fluoride therapy for dental care. Jpn Dent Sci Rev 2022; 58: 249-257
- 16 Candotto V, Lauritano D, Carinci F. et al. Silver-based chemical device as an adjunct of domestic oral hygiene: a study on periodontal patients. Materials (Basel) 2018; 11 (08) 1483
- 17 Hernández-Venegas PA, Martínez-Martínez RE, Zaragoza-Contreras EA. et al. Bactericidal activity of silver nanoparticles on oral biofilms related to patients with and without periodontal disease. J Funct Biomater 2023; 14 (06) 311
- 18 Ramasubburayan R, Ramanathan G, Vijay SS. et al. Harnessing green nanoparticles: sustainable solutions for combating dental caries management. Mater Today Chem 2025; 45: 102631
- 19 Vishwanath N, Whitaker C, Allu S. et al. Silver as an antibiotic-independent antimicrobial: review of current formulations and clinical relevance. Surg Infect (Larchmt) 2022; 23 (09) 769-780
- 20 Ramya JR, Ali S. K TA, et al. Antimicrobial efficiency against fish pathogens on the green synthesized silver nanoparticles. Microb Pathog 2024; 193: 106725
- 21 Carvalho-Silva JM, Dos Reis AC. Systematic review of silver and vanadium-based antibiofilm agents: mechanisms and efficacy in oral biofilms. Future Microbiol 2025; 20 (10) 639-655
- 22 Tricco AC, Lillie E, Zarin W. et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018; 169 (07) 467-473
- 23 Sheth VH, Shah NP, Jain R, Bhanushali N, Bhatnagar V. Development and validation of a risk-of-bias tool for assessing in vitro studies conducted in dentistry: the QUIN. J Prosthet Dent 2024; 131 (06) 1038-1042
- 24 Spacciapoli P, Buxton D, Rothstein D, Friden P. Antimicrobial activity of silver nitrate against periodontal pathogens. J Periodontal Res 2001; 36 (02) 108-113
- 25 Lu Z, Rong K, Li J, Yang H, Chen R. Size-dependent antibacterial activities of silver nanoparticles against oral anaerobic pathogenic bacteria. J Mater Sci Mater Med 2013; 24 (06) 1465-1471
- 26 Reise M, Gottschaldt M, Matz C. et al. Antibacterial effect of silver (I) carbohydrate complexes on oral pathogenic key species in vitro. BMC Oral Health 2016; 16 (01) 42
- 27 Rams TE, Sautter JD, Ramírez-Martínez GJ, Whitaker EJ. Antimicrobial activity of silver diamine fluoride on human periodontitis microbiota. Gen Dent 2020; 68 (05) 24-28
- 28 Zorraquín-Peña I, Cueva C, González de Llano D, Bartolomé B, Moreno-Arribas MV. Glutathione-stabilized silver nanoparticles: antibacterial activity against periodontal bacteria, and cytotoxicity and inflammatory response in oral cells. Biomedicines 2020; 8 (10) 375
- 29 More PR, Pandit S, Filippis A, Franci G, Mijakovic I, Galdiero M. Silver nanoparticles: bactericidal and mechanistic approach against drug resistant pathogens. Microorganisms 2023; 11 (02) 369
- 30 Slavin YN, Asnis J, Häfeli UO, Bach H. Metal nanoparticles: understanding the mechanisms behind antibacterial activity. J Nanobiotechnology 2017; 15 (01) 65
- 31 Boltovets P, Kravchenko S, Manoilov E, Snopok B. Effect of glutathione on the destruction kinetics of silver nanoparticles in aqueous solutions: an optical study under neutral and alkaline conditions. Eng Proc 2023; 58 (01) 43
- 32 Mihailovic V, Katanic Stankovic JS, Selakovic D, Rosic G. An overview of the beneficial role of antioxidants in the treatment of nanoparticle-induced toxicities. Oxid Med Cell Longev 2021; 2021 (01) 7244677
- 33 Kravchenko S, Boltovets P, Snopok B. Chemical transformation of typical biological recognition elements in reactions with nanosized targets: a study of glutathione coated silver nanoparticles. Eng Proc 2023; 35 (01) 31
- 34 Lu SC. Glutathione synthesis. Biochim Biophys Acta 2013; 1830 (05) 3143-3153
- 35 Knerr PJ, Tzekou A, Ricklin D. et al. Synthesis and activity of thioether-containing analogues of the complement inhibitor compstatin. ACS Chem Biol 2011; 6 (07) 753-760
- 36 Hidalgo E, Bartolomé R, Barroso C, Moreno A, Domínguez C. Silver nitrate: antimicrobial activity related to cytotoxicity in cultured human fibroblasts. Skin Pharmacol Appl Skin Physiol 1998; 11 (03) 140-151
- 37 Zhang L, Li X, Yan H, Huang L. Salivary matrix metalloproteinase (MMP)-8 as a biomarker for periodontitis: a PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore) 2018; 97 (03) e9642
- 38 Ho Y, Gyurko R, Uzel NG. et al. An in vitro pilot study on the effects of silver diamine fluoride on periodontal pathogens and three-dimensional scaffolds of human fibroblasts and epithelial cells. Int J Dent 2022; 2022: 9439096
- 39 Usui M, Onizuka S, Sato T, Kokabu S, Ariyoshi W, Nakashima K. Mechanism of alveolar bone destruction in periodontitis—periodontal bacteria and inflammation. Jpn Dent Sci Rev 2021; 57: 201-208
Address for correspondence
Publication History
Article published online:
20 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Marsh PD. In sickness and in health—what does the oral microbiome mean to us? An ecological perspective. Adv Dent Res 2018; 29 (01) 60-65
- 2 Zhao A, Sun J, Liu Y. Understanding bacterial biofilms: from definition to treatment strategies. Front Cell Infect Microbiol 2023; 13: 1137947
- 3 Prucsi Z, Płonczyńska A, Potempa J, Sochalska M. Uncovering the oral dysbiotic microbiota as masters of neutrophil responses in the pathobiology of periodontitis. Front Microbiol 2021; 12: 729717
- 4 Groeger S, Zhou Y, Ruf S, Meyle J. Pathogenic mechanisms of Fusobacterium nucleatum on oral epithelial cells. Front Oral Health 2022; 3: 831607
- 5 Suzuki R, Kamio N, Sugimoto K. et al. Periodontopathic bacterium Fusobacterium nucleatum affects matrix metalloproteinase-9 expression in human alveolar epithelial cells and mouse lung. In Vivo 2022; 36 (02) 649-656
- 6 Llama-Palacios A, Potupa O, Sánchez MC, Figuero E, Herrera D, Sanz M. Proteomic analysis of Fusobacterium nucleatum growth in biofilm versus planktonic state. Mol Oral Microbiol 2020; 35 (04) 168-180
- 7 Chen Z, Huang L. Fusobacterium nucleatum carcinogenesis and drug delivery interventions. Adv Drug Deliv Rev 2024; 209: 115319
- 8 Muchova M, Kuehne SA, Grant MM. et al. Fusobacterium nucleatum elicits subspecies-specific responses in human neutrophils. Front Cell Infect Microbiol 2024; 14: 1449539
- 9 Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation. Nat Rev Immunol 2015; 15 (01) 30-44
- 10 Chen Y, Shi T, Li Y, Huang L, Yin D. Fusobacterium nucleatum: the opportunistic pathogen of periodontal and peri-implant diseases. Front Microbiol 2022; 13: 860149
- 11 Herrera D, van Winkelhoff AJ, Matesanz P, Lauwens K, Teughels W. Europe's contribution to the evaluation of the use of systemic antimicrobials in the treatment of periodontitis. Periodontol 2000 2023; . Epub ahead of print
- 12 Sim W, Barnard RT, Blaskovich MAT, Ziora ZM. Antimicrobial silver in medicinal and consumer applications: a patent review of the past decade (2007–2017). Antibiotics (Basel) 2018; 7 (04) 93
- 13 Fakhruddin KS, Egusa H, Ngo HC, Panduwawala C, Pesee S, Samaranayake LP. Clinical efficacy and the antimicrobial potential of silver formulations in arresting dental caries: a systematic review. BMC Oral Health 2020; 20 (01) 160
- 14 Lim GXD, Yang J. Effect of silver diamine fluoride on hyperplastic gingivitis in an adult with intellectual disability—a case report. Spec Care Dentist 2022; 42 (01) 73-79
- 15 Zheng FM, Yan IG, Duangthip D, Gao SS, Lo ECM, Chu CH. Silver diamine fluoride therapy for dental care. Jpn Dent Sci Rev 2022; 58: 249-257
- 16 Candotto V, Lauritano D, Carinci F. et al. Silver-based chemical device as an adjunct of domestic oral hygiene: a study on periodontal patients. Materials (Basel) 2018; 11 (08) 1483
- 17 Hernández-Venegas PA, Martínez-Martínez RE, Zaragoza-Contreras EA. et al. Bactericidal activity of silver nanoparticles on oral biofilms related to patients with and without periodontal disease. J Funct Biomater 2023; 14 (06) 311
- 18 Ramasubburayan R, Ramanathan G, Vijay SS. et al. Harnessing green nanoparticles: sustainable solutions for combating dental caries management. Mater Today Chem 2025; 45: 102631
- 19 Vishwanath N, Whitaker C, Allu S. et al. Silver as an antibiotic-independent antimicrobial: review of current formulations and clinical relevance. Surg Infect (Larchmt) 2022; 23 (09) 769-780
- 20 Ramya JR, Ali S. K TA, et al. Antimicrobial efficiency against fish pathogens on the green synthesized silver nanoparticles. Microb Pathog 2024; 193: 106725
- 21 Carvalho-Silva JM, Dos Reis AC. Systematic review of silver and vanadium-based antibiofilm agents: mechanisms and efficacy in oral biofilms. Future Microbiol 2025; 20 (10) 639-655
- 22 Tricco AC, Lillie E, Zarin W. et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018; 169 (07) 467-473
- 23 Sheth VH, Shah NP, Jain R, Bhanushali N, Bhatnagar V. Development and validation of a risk-of-bias tool for assessing in vitro studies conducted in dentistry: the QUIN. J Prosthet Dent 2024; 131 (06) 1038-1042
- 24 Spacciapoli P, Buxton D, Rothstein D, Friden P. Antimicrobial activity of silver nitrate against periodontal pathogens. J Periodontal Res 2001; 36 (02) 108-113
- 25 Lu Z, Rong K, Li J, Yang H, Chen R. Size-dependent antibacterial activities of silver nanoparticles against oral anaerobic pathogenic bacteria. J Mater Sci Mater Med 2013; 24 (06) 1465-1471
- 26 Reise M, Gottschaldt M, Matz C. et al. Antibacterial effect of silver (I) carbohydrate complexes on oral pathogenic key species in vitro. BMC Oral Health 2016; 16 (01) 42
- 27 Rams TE, Sautter JD, Ramírez-Martínez GJ, Whitaker EJ. Antimicrobial activity of silver diamine fluoride on human periodontitis microbiota. Gen Dent 2020; 68 (05) 24-28
- 28 Zorraquín-Peña I, Cueva C, González de Llano D, Bartolomé B, Moreno-Arribas MV. Glutathione-stabilized silver nanoparticles: antibacterial activity against periodontal bacteria, and cytotoxicity and inflammatory response in oral cells. Biomedicines 2020; 8 (10) 375
- 29 More PR, Pandit S, Filippis A, Franci G, Mijakovic I, Galdiero M. Silver nanoparticles: bactericidal and mechanistic approach against drug resistant pathogens. Microorganisms 2023; 11 (02) 369
- 30 Slavin YN, Asnis J, Häfeli UO, Bach H. Metal nanoparticles: understanding the mechanisms behind antibacterial activity. J Nanobiotechnology 2017; 15 (01) 65
- 31 Boltovets P, Kravchenko S, Manoilov E, Snopok B. Effect of glutathione on the destruction kinetics of silver nanoparticles in aqueous solutions: an optical study under neutral and alkaline conditions. Eng Proc 2023; 58 (01) 43
- 32 Mihailovic V, Katanic Stankovic JS, Selakovic D, Rosic G. An overview of the beneficial role of antioxidants in the treatment of nanoparticle-induced toxicities. Oxid Med Cell Longev 2021; 2021 (01) 7244677
- 33 Kravchenko S, Boltovets P, Snopok B. Chemical transformation of typical biological recognition elements in reactions with nanosized targets: a study of glutathione coated silver nanoparticles. Eng Proc 2023; 35 (01) 31
- 34 Lu SC. Glutathione synthesis. Biochim Biophys Acta 2013; 1830 (05) 3143-3153
- 35 Knerr PJ, Tzekou A, Ricklin D. et al. Synthesis and activity of thioether-containing analogues of the complement inhibitor compstatin. ACS Chem Biol 2011; 6 (07) 753-760
- 36 Hidalgo E, Bartolomé R, Barroso C, Moreno A, Domínguez C. Silver nitrate: antimicrobial activity related to cytotoxicity in cultured human fibroblasts. Skin Pharmacol Appl Skin Physiol 1998; 11 (03) 140-151
- 37 Zhang L, Li X, Yan H, Huang L. Salivary matrix metalloproteinase (MMP)-8 as a biomarker for periodontitis: a PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore) 2018; 97 (03) e9642
- 38 Ho Y, Gyurko R, Uzel NG. et al. An in vitro pilot study on the effects of silver diamine fluoride on periodontal pathogens and three-dimensional scaffolds of human fibroblasts and epithelial cells. Int J Dent 2022; 2022: 9439096
- 39 Usui M, Onizuka S, Sato T, Kokabu S, Ariyoshi W, Nakashima K. Mechanism of alveolar bone destruction in periodontitis—periodontal bacteria and inflammation. Jpn Dent Sci Rev 2021; 57: 201-208