

Subscribe to RSS
DOI: 10.1055/s-0045-1814464
Randomized Clinical Trial Assessing Patient-reported Outcomes with Bar–Locator versus Bar–Clip Attachments in Mandibular Two-implant Overdentures
Authors

Abstract
Objective
This randomized clinical trial compared patient satisfaction and oral health-related quality of life (OHRQoL) in edentulous individuals rehabilitated with mandibular two-implant overdentures retained by bar–locator or bar–clip attachments.
Material and Methods
A total of 16 edentulous participants received two implants in the mandibular canine regions and were randomly assigned to receive overdentures with either bar–locator or bar–clip attachments. Patient satisfaction was assessed using a 100-mm visual analog scale (VAS), and OHRQoL was measured using the Oral Health Impact Profile (OHIP-14) after 3 months of functional use. Independent samples t-tests were applied with a significance level of p < 0.05.
Statistical Analysis
Comparisons between the two attachment groups were performed using the independent samples t-test, and statistical significance was set at p < 0.05. In addition to p-values, effect sizes (Cohen's d) were calculated to assess the magnitude and clinical relevance of intergroup differences.
Results
The bar–locator group reported significantly higher satisfaction regarding denture stability, retention, and masticatory efficiency, whereas the bar–clip group demonstrated greater overall comfort and lower psychological discomfort scores. No statistically significant differences were found in other domains of satisfaction or OHRQoL.
Conclusion
Both attachment systems improved patient satisfaction and OHRQoL, with each demonstrating distinct advantages. The bar–locator system provided superior functional performance, while the bar–clip system enhanced comfort and psychosocial adaptation. Clinical selection should be based on patient priorities and anatomical conditions.
Introduction
Conventional complete dentures are often associated with clinical limitations, including inadequate stability and retention, mucosal irritation, and reduced comfort during mastication.[1] These shortcomings have been substantially mitigated by the advent of implant-supported overdentures, which provide superior functional performance, enhanced aesthetics, and greater patient-reported satisfaction.[2]
Implant overdentures may employ stud attachments for unsplinted implants or bar attachments for splinted configurations.[3] [4] According to the McGill Consensus Statement, regardless of the attachment design (ball, magnet, or bar), the two-implant overdenture represents the recommended standard treatment for the edentulous mandible.[5]
Bar attachments are available in various designs that splint implants, enhance load distribution across the attachment interfaces, and resist dislodging forces in both vertical and oblique directions, thereby improving prosthesis stability.[6] Their structural characteristics, such as diameter, material composition, cross-sectional configuration, and the distance from the mucosa, may vary considerably. These design variations influence the biomechanical response of the supporting implants as well as the adjacent peri-implant tissues.[7] [8]
Attachment systems, particularly bar designs, have been shown to substantially improve patient-reported outcomes with overdentures by enhancing prosthesis stability and retention, which in turn leads to superior masticatory performance.[9]
Several techniques are available for securing a locator attachment to a bar, including drill-and-tap procedures, laser welding, and gold bar casting, each differing in how the metal patrix is integrated with the bar. The drill-and-tap technique offers practical advantages, as it facilitates both the initial connection of the attachment to the bar and its subsequent replacement in cases of retention loss.[10] [11]
Bar–clip attachments are a well-established modality in implant-supported overdenture treatment, effectively mitigating issues of prosthetic retention and stability while significantly enhancing patient satisfaction. The bar framework is fabricated by adapting prefabricated plastic patterns onto a master cast, followed by casting in a suitable metal alloy. A distinguishing characteristic of this system is the incorporation of a plastic retentive sleeve, which contrasts with the predominantly metallic components used in alternative attachment systems. These plastic sleeves facilitate straightforward chairside replacement when retention diminishes, thereby maintaining optimal prosthetic performance with minimal clinical intervention.[12]
The visual analog scale (VAS) is a simple, reliable, and standard tool for measuring subjective experiences such as patient satisfaction and comfort in implant overdenture therapy. Its continuous scale is more sensitive to subtle changes than categorical scales, making it highly effective for clinical practice and research.[13] [14]
Oral Health-Related Quality of Life (OHRQoL) reflects the impact of oral health on functional, psychological, and social well-being. Implant-supported overdentures have been shown to significantly enhance OHRQoL by improving mastication, comfort, and self-esteem. Validated tools such as the Oral Health Impact Profile (OHIP-14) and VAS are commonly used to quantify these improvements.[15] [16]
This study aimed to record and analyze patient satisfaction and quality of life with mandibular implant overdentures using a bar–locator and bar–clip attachments. The null hypothesis stated that there would be no significant difference between the attachments examined.
Material and Methods
Study Design
A total of 16 completely edentulous patients were recruited from the outpatient clinic of the Department of Removable Prosthodontics, Faculty of Dentistry, Mansoura University. The required sample size was calculated using G*Power software (version 3.1.5, Kiel, Germany) based on the primary outcome of patient satisfaction, as reported by Mahanna et al.[17] The analysis assumed an effect size (f) of 0.40, an α error probability of 0.05, and a power (1–β) of 0.80 to detect intergroup differences using the independent-samples t-test. The minimum total sample size required was 16 participants (8 per group). This sample size was considered adequate to detect clinically meaningful differences between attachment systems while maintaining acceptable statistical power for a parallel-group design. The present study was conducted following the CONSORT statement. The study's patient flow diagram and allocation are illustrated in [Fig. 1]. Ethical approval for the study protocol was obtained from the Faculty of Dentistry, Mansoura University, with approval no. M21011122, and the trial was prospectively registered at ClinicalTrials.gov (Identifier: NCT06673186). Written informed consent was obtained from all participants before enrollment. Patient eligibility and stratification were based on predefined criteria, including age, sex, and bone quality ([Table 1]).
Abbreviations: SD, standard deviation; X, mean.

Participants were randomly assigned to two groups using a computer-generated randomization sequence. Group allocation was concealed in sequentially numbered, opaque, sealed envelopes prepared by an independent researcher not involved in participant recruitment, clinical procedures, or data analysis, ensuring adequate allocation concealment.
Due to the nature of the interventions, complete blinding of the participants and the treating prosthodontist was not possible. However, to minimize assessment bias, the research assistant who administered the postoperative VAS and OHIP-14 questionnaires was blinded to the group allocation of the participants. Furthermore, the statistician performing the final data analysis was also kept blinded to the group identities, which were coded neutrally during the analytical phase.
Inclusion and Exclusion Criteria
All patients demonstrated adequate residual alveolar ridge dimensions in both the maxilla and mandible to permit implant placement in the mandibular canine region, with a minimum bone height of 11 mm and a width of 3.7 mm confirmed by cone-beam computed tomography. In addition, all participants exhibited a class I maxillomandibular relationship and a vertical restorative space ranging between 12 and 15 mm, corresponding primarily to class II to class I restorative space according to the classification of Ahuja and Cagna.[18] This range provides adequate clearance for bar-retained mandibular overdentures. All participants also presented with healthy, well-keratinized mucosa and favorable soft-tissue conditions.[19]
Individuals were excluded from participation if they exhibited physical, psychological, or social impairments or systemic conditions that contraindicate minor oral surgical procedures, such as severe cardiovascular disease or poorly controlled type 2 diabetes. Additional exclusion criteria included a diagnosis of osteoporosis, a history of radiation therapy to the head and neck region, high-risk behavioral patterns (e.g., chronic alcohol use or heavy tobacco consumption), as well as clinical signs of parafunctional activity or temporomandibular disorders.[20] [21]
Pre-prosthetic Preparation
To promote soft tissue adaptation before implant placement, all participants were rehabilitated with newly constructed maxillary and mandibular complete dentures, which they were instructed to wear continuously. For accurate implant positioning and angulation, a mucosa-supported surgical guide was fabricated for each patient.
Surgical Procedure
In the mandibular interforaminal region, two implants were inserted for each patient using a static computer-guided approach with a stereolithographic mucosa-supported surgical guide stent to ensure accurate implant positioning and angulation. During surgery, participants were instructed to bite lightly on the surgical stent to stabilize the guide and facilitate accurate placement of fixation pins. Following sequential osteotomy preparation, the guide was removed, the implants were inserted, and cover screws were placed. Verification of implant positioning was performed immediately postoperatively using panoramic radiography.
After a healing period of 3 months to allow for osseointegration, the implants were surgically exposed to establish a gingival collar. Healing abutments were connected and maintained for 2 weeks to allow peri-implant soft tissue maturation ([Fig. 2]).

Group Allocation and Prosthetic Procedures
After soft tissue healing and fabrication of the definitive impression, participants were randomly assigned to two equal groups (n = 8) using a balanced allocation method to ensure comparability. Randomization was performed after completion of the surgical phase and before prosthetic fabrication, ensuring that all participants underwent identical surgical procedures. Consequently, the grouping influenced only the type of attachment system used during prosthetic construction.
Definitive impressions were made using the open-tray technique. Impression copings were connected to the implants and splinted intraorally to minimize displacement during impression removal. Once the impression was withdrawn, implant analogs were attached to the transfer copings before pouring, and a definitive mandibular master cast was fabricated for each participant.
In Group I (bar–locator attachment, [Fig. 3A]), participants were rehabilitated with mandibular overdentures retained by a bar–locator system. The bar framework was initially sculpted in wax and subsequently cast in cobalt–chromium alloy to achieve a passive fit on the master cast. Following casting, two threaded channels were created on the occlusal surface of the definitive bar using sequential instrumentation with a 1.7-mm drill, followed by a 2.0-mm tap to receive the locator female components. These components were secured within the threaded channels by means of a customized rider to ensure mechanical stability.

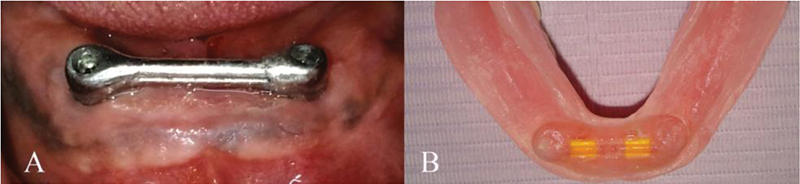
In Group II (bar–clip attachment, [Fig. 4A]), participants received mandibular overdentures retained by a conventional bar–clip system. A prefabricated plastic bar pattern was adapted to the master cast and then cast in cobalt–chromium alloy to fabricate the definitive bar framework.
In both experimental groups, trial insertion of the bar frameworks was performed to verify passive fit before denture fabrication. Artificial teeth were arranged following the principles of bilateral balanced occlusion to optimize masticatory efficiency and prosthetic stability. The overdentures were then processed, finished, polished, and delivered.
Attachment Pick-up Procedures
The pick-up of attachment systems was performed following standardized protocols. In the bar–locator group, two locator nylon inserts with metal housings were positioned on the bar and processed into the intaglio surface of the mandibular overdenture using auto-polymerizing acrylic resin ([Fig. 3B]). In the bar–clip group, two yellow plastic clips were similarly positioned and picked up using self-curing acrylic resin ([Fig. 4B]). For both groups, undercuts beneath the bar were blocked out, and lingual vents were created to permit the escape of excess resin. Patients maintained centric occlusion during polymerization to ensure accurate seating and vertical dimension. Excess resin was then removed, and the denture base was finished and polished.
Post-insertion adjustments were performed as required, and all participants received standardized oral-hygiene instructions to promote long-term prosthesis maintenance and peri-implant tissue health.
Study Outcomes
Participant satisfaction was assessed through a questionnaire based on a VAS. The questionnaire encompassed several domains, including overall comfort, denture stability and retention, speech difficulties, challenges associated with biting and masticating various food textures, oral hygiene maintenance, ease of denture handling, and social impact. Responses were recorded on a 100-mm scale, where 0 represented complete dissatisfaction and 100 denoted maximum satisfaction.[22] To ensure linguistic and cultural validity, the questionnaire was administered in Arabic.
Oral health-related quality of life was assessed using the Arabic version of the OHIP-14 ([Table 2]). This instrument comprises 14 items grouped into seven domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap.[23] Each item was scored on a five-point Likert scale: “never” (1), “hardly ever” (2), “occasionally” (3), “fairly often” (4), and “very often” (5). Higher cumulative scores reflected poorer oral health–related quality of life, whereas lower scores indicated better outcomes.
Both the VAS and OHIP-14 questionnaires were administered 3 months after delivery of the overdentures, a period considered sufficient for neuromuscular adaptation to the prosthetic appliances.[24]
Statistical Analysis
Data analysis was conducted using SPSS software (version 25.0; IBM Corp., Armonk, NY, USA). Comparisons between the two attachment groups were performed using the independent-samples t-test, and statistical significance was set at p < 0.05. In addition to p-values, effect sizes (Cohen's d) were calculated to assess the magnitude and clinical relevance of intergroup differences.
Results
The results of patient-reported satisfaction as measured by the VAS are summarized in [Table 3] and [Fig. 5]. Overall, both attachment systems provided high satisfaction scores across all measured domains, though some differences were statistically and clinically significant.

Abbreviations: max, maximum; min, minimum; SD, standard deviation; X, mean.
Note: a P value is significant at 5% level. Cohen's d values: 0.2 = small, 0.5 = medium, 0.8 = large effect. size.
Patients rehabilitated with bar–locator attachments (Group I) demonstrated significantly higher satisfaction with denture stability and retention (p = 0.019, d = 1.16) and biting and chewing ability (p = 0.034, d = 1.04), indicating large effect sizes. These findings suggest that the bar–locator design provided superior functional performance and enhanced prosthesis stability.
Conversely, the bar–clip group (Group II) reported significantly greater comfort with dentures (p = 0.014, d = 1.22), also reflecting a large effect size, highlighting its advantage in overall comfort. No statistically significant differences were observed between the two groups regarding speech, ease of denture handling, or social interactions, although the bar–locator group tended to report slightly higher satisfaction in handling ease.
Effect size interpretation further emphasizes that most significant differences between groups were not only statistically meaningful but also clinically substantial, with d values exceeding 0.8.
The results of the OHIP-14 are presented in [Table 4] and [Fig. 6]. No significant differences were observed between the two attachment systems across most domains, including functional limitation, physical pain, physical disability, psychological disability, social disability, and handicap (p > 0.05 for all).

Abbreviations: OHIP-14, Oral Health Impact Profile; SD, standard deviation; X, mean.
Notes: a P value is significant at 5% level.
Cohen's d values: 0.2 = small, 0.5 = medium, 0.8 = large effect size.
However, a statistically significant difference was detected in psychological discomfort, with the bar–clip group showing a lower mean score (1.63 ± 0.52) than the bar–locator group (2.38 ± 0.52) (p = 0.014, d = 1.18), representing a large effect size and indicating enhanced psychological well-being among bar–clip users.
Overall, both attachment systems produced favorable outcomes in oral health-related quality of life, though their benefits appeared to differ functionally and psychologically. The bar–locator system offered greater mechanical stability and masticatory efficiency, whereas the bar–clip system provided superior comfort and psychological adaptation during the early post-insertion phase.
Discussion
The findings of the present study demonstrate that implant-supported overdentures enhance patient satisfaction and oral health-related quality of life (OHRQoL), regardless of the attachment system used. This is consistent with previous reports indicating that even a single implant can positively influence patient satisfaction and perceived oral health outcomes, while two implants are often considered sufficient to provide satisfactory retention and function for mandibular overdentures.[25] [26] VAS has been widely validated as a reliable instrument for assessing patient satisfaction in prosthodontic research, providing a simple yet precise metric along a 0 to 100 continuum.[27] [28]
The bar–locator system was associated with significantly higher satisfaction in terms of denture stability, retention, and masticatory performance. This may be attributed to its dual-retention mechanism, which provides both internal and external frictional engagement, enhancing resistance to both vertical and rotational displacement.[29] The degree of retention is largely dependent on the type and material of the attachment system.[30] In addition, the low vertical profile and self-aligning design of the locator system improve prosthesis seating, load distribution, and functional efficiency during mastication. These characteristics directly contribute to enhanced oral functional capacity and explain the higher satisfaction observed during biting and chewing. Previous studies have similarly reported that improved overdenture retention enhances muscular activity and chewing efficiency.[24] Shady et al[31] found that locator-based bar attachments achieved higher retention values and better patient satisfaction due to their mechanical design and resilience, while Elsyad et al[32] confirmed their reduced maintenance requirements and improved masticatory performance in patients with atrophied ridges. These findings are consistent with other studies demonstrating that bar–locator attachments offer superior retention and long-term stability compared with bar–clip and ball systems.[31]
In contrast, the bar–clip system demonstrated superior overall comfort. The improved comfort can be explained by the flexible nature of the plastic clip inserts, which allow minor rotational and vertical resilience of the overdenture around the bar during function. This micro-mobility helps to dissipate occlusal loads, thereby reducing the stress transmitted to the peri-implant bone and mucosa.[11] Moreover, the lower vertical height of the bar–clip framework minimizes denture base bulk, improving tongue space and speech adaptation. These characteristics are consistent with the results of Mahanna et al,[17] who reported that attachments with reduced vertical dimensions enhance comfort and minimize tongue interference.
No significant differences were found between groups regarding ease of denture handling, specifically insertion and removal. Nevertheless, participants using bar–locator attachments expressed higher satisfaction in this domain, possibly due to the self-aligning properties of the locator design. These features facilitate accurate seating of the prosthesis and may be further enhanced by incorporating guide planes on a milled bar to create a common path of insertion. This observation corroborates the findings of Al-Harbi,[29] who emphasized the clinical advantage of the self-aligning mechanism inherent in locator attachments.
Regarding OHRQoL, as assessed by OHIP-14, no significant intergroup differences were observed across most domains, except for psychological discomfort. Participants rehabilitated with bar–clip overdentures reported lower levels of psychological discomfort compared with those with bar–locator systems. This may be attributed to the increased vertical profile of bar–locator attachments, which can produce a perceptible bulkiness. Prior studies have suggested that the relatively high vertical dimension of bar attachments may stimulate periosteal mechanoreceptors surrounding implants, potentially contributing to heightened self-awareness of the prosthesis and a diminished sense of natural integration.[33]
From a biomechanical standpoint, the different patient responses observed between the two systems can be explained by their distinct load transfer patterns. Bar–locator systems are characterized by more rigid fixation, transferring masticatory forces axially along the implants, which improves retention but may increase the load concentration on individual fixtures. Conversely, bar–clip systems permit a small degree of rotational movement around the bar, which helps distribute stress across both implants and the residual ridges.[10] [11] This controlled resilience can enhance long-term comfort and reduce stress-related complications. Therefore, the choice between attachment systems represents a fundamental clinical trade-off between mechanical stability and biological adaptability.
Clinically, these findings have important implications for prosthesis selection and long-term maintenance. The bar–locator system may be preferable for patients prioritizing functional efficiency, stability, and strong retention, such as those with high masticatory demands or reduced neuromuscular control. However, the clinician should anticipate periodic replacement of nylon inserts due to wear and potential retention.[30] In contrast, the bar–clip system may be more suitable for patients emphasizing comfort, ease of adaptation, or limited vestibular depth. The clip inserts are also inexpensive and easily replaceable chairside, facilitating straightforward long-term maintenance.
All patients received new conventional dentures before implant placement to standardize occlusion and adaptation. The study focused on comparing two bar attachment systems; therefore, assessment of satisfaction with conventional dentures was not included. Previous studies have already confirmed the superior outcomes of implant overdentures over conventional dentures, so including a control group was unnecessary.
Despite the encouraging findings, this study has certain limitations that warrant consideration. The relatively small sample size may limit the generalizability of the outcomes; however, inclusion of effect size calculations allows a more meaningful interpretation of the magnitude and clinical relevance of the observed differences. The 3-month follow-up period reflects early patient adaptation rather than long-term prosthetic stability, maintenance requirements, or peri-implant tissue responses. Future investigations with extended observation periods (≥12 months) are recommended to evaluate neuromuscular adaptation, attachment wear resistance, and peri-implant tissue health over time.
Variations in participants' educational background may have influenced their comprehension of the assessment tools; however, the Arabic versions of the VAS and OHIP-14 employed in this study have been previously validated and demonstrated acceptable reliability among Arabic-speaking populations. These instruments provided dependable measures of patient-reported outcomes. Based on the obtained results, the null hypothesis was rejected, as significant differences were observed between the bar–locator and bar–clip attachment systems in multiple domains of satisfaction and oral health-related quality of life.
Conclusion
Within the limitations of this clinical trial, both attachment systems significantly enhanced patient satisfaction and oral health-related quality of life in mandibular overdenture rehabilitation. The bar–locator system demonstrated superior stability, retention, and masticatory efficiency due to its dual-retentive and self-aligning features, whereas the bar–clip system provided greater overall comfort owing to its resilient design and reduced vertical profile. These findings underscore the importance of balancing mechanical retention with biological adaptability when selecting attachment systems. Individual patient priorities, anatomical conditions, and maintenance considerations should guide clinical choice.
Conflict of Interest
None declared.
Acknowledgement
This study is supported via funding from Prince Sattam bin Abdulaziz University project number (PSAU/2025/R/ 1447).
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
-
References
- 1 Heckmann SM, Heussinger S, Linke JJ, Graef F, Pröschel P. Improvement and long-term stability of neuromuscular adaptation in implant-supported overdentures. Clin Oral Implants Res 2009; 20 (11) 1200-1205
- 2 Borges GA, Barbin T, Dini C. et al. Patient-reported outcome measures and clinical assessment of implant-supported overdentures and fixed prostheses in mandibular edentulous patients: a systematic review and meta-analysis. J Prosthet Dent 2022; 127 (04) 565-577
- 3 Yilmaz B, Ozkir E, Johnston WM, McGlumphy E. Dislodgement force analysis of an overdenture attachment system. J Prosthet Dent 2020; 123 (02) 291-298
- 4 Salehi R, Shayegh SS, Johnston WM, Hakimaneh SMR. Effects of interimplant distance and cyclic dislodgement on retention of LOCATOR and ball attachments: an in vitro study. J Prosthet Dent 2019; 122 (06) 550-556
- 5 Feine JS, Carlsson GE, Awad MA. et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Montreal, Quebec, May 24-25, 2002. Int J Oral Maxillofac Implants 2002; 17 (04) 601-602
- 6 Naert I, Gizani S, Vuylsteke M, van Steenberghe D. A 5-year randomized clinical trial on the influence of splinted and unsplinted oral implants in the mandibular overdenture therapy. Part I: Peri-implant outcome. Clin Oral Implants Res 1998; 9 (03) 170-177
- 7 ELsyad MA, Emera RMK, Ashmawy TM. Effect of different bar designs on axial and nonaxial retention forces of implant-retained maxillary overdentures: an in vitro study. Int J Oral Maxillofac Implants 2019; 34 (01) 31-38
- 8 de la Rosa Castolo G, Guevara Perez SV, Arnoux PJ, Badih L, Bonnet F, Behr M. Implant-supported overdentures with different clinical configurations: mechanical resistance using a numerical approach. J Prosthet Dent 2019; 121 (03) 546.e1-546.e10
- 9 Shafie HR. Clinical and Laboratory Manual of Implant Overdentures. John Wiley & Sons; 2013
- 10 Seo YH, Bae EB, Kim JW. et al. Clinical evaluation of mandibular implant overdentures via Locator implant attachment and Locator bar attachment. J Adv Prosthodont 2016; 8 (04) 313-320
- 11 Kim MS, Yoon MJ, Huh JB, Jeon YC, Jeong CM. Implant overdenture using a locator bar system by drill and tapping technique in a mandible edentulous patient: a case report. J Adv Prosthodont 2012; 4 (02) 116-120
- 12 Wei L, Ma Q, Qin X, Pan S. In vitro cyclic dislodging test on retentive force of two types of female parts of SFI-Bar. Int J Prosthodont 2016; 29 (03) 293-295
- 13 Matarasso S, Iorio Siciliano V, Aglietta M, Andreuccetti G, Salvi GE. Clinical and radiographic outcomes of a combined resective and regenerative approach in the treatment of peri-implantitis: a prospective case series. Clin Oral Implants Res 2014; 25 (07) 761-767
- 14 Tosun B, Uysal N. Examination of oral health quality of life and patient satisfaction in removable denture wearers with OHIP-14 scale and visual analog scale: a cross-sectional study. BMC Oral Health 2024; 24 (01) 1353
- 15 Revilla-León M, Yilmaz B, Kois JC, Att W. Prevention of peri-implant disease in edentulous patients with fixed implant rehabilitations. Clin Implant Dent Relat Res 2023; 25 (04) 743-751
- 16 Chai HH, Gao SS, Chen KJ, Lo ECM, Duangthip D, Chu CH. Tools evaluating child oral health–related quality of life. Int Dent J 2024; 74 (01) 15-24
- 17 Mahanna FF, Elsyad MA, Mourad SI, Abozaed HW. Satisfaction and oral health-related quality of life of different attachments used for implant-retained overdentures in subjects with resorbed mandibles: a crossover trial. Int J Oral Maxillofac Implants 2020; 35 (02) 423-431
- 18 Ahuja S, Cagna DR. Classification and management of restorative space in edentulous implant overdenture patients. J Prosthet Dent 2011; 105 (05) 332-337
- 19 Abozaed HW. Patient satisfaction and oral health-related quality of life of quadrilateral bar versus bilateral linear bar for mandibular implant overdenture: randomized controlled clinical trial. Eur J Dent 2025; Epub ahead of print.
- 20 Mourad KE, Emera RMK, Habib A. Effect of different implant positions for two implant-retained mandibular overdenture: a retrospective 5-years radiographic evaluation of the circumferential peri-implant bone loss and posterior ridge resorptive changes. BMC Oral Health 2024; 24 (01) 1161
- 21 de Souza RF, Bedos C, Esfandiari S. et al. Single-implant overdentures retained by the Novaloc attachment system: study protocol for a mixed-methods randomized cross-over trial. Trials 2018; 19 (01) 243
- 22 Elsyad MA. Patient satisfaction and prosthetic aspects with mini-implants retained mandibular overdentures. A 5-year prospective study. Clin Oral Implants Res 2016; 27 (07) 926-933
- 23 Elsyad MA, Mostafa AZ. Effect of telescopic distal extension removable partial dentures on oral health related quality of life and maximum bite force: a preliminary cross over study. J Esthet Restor Dent 2018; 30 (01) 14-21
- 24 Elsyad MA, Khairallah AS. Chewing efficiency and maximum bite force with different attachment systems of implant overdentures: a crossover study. Clin Oral Implants Res 2017; 28 (06) 677-682
- 25 El-Waseef FA, Abozaed HW. Patient satisfaction and oral health–related quality of life for single-implant mandibular overdentures reinforced by cobalt chromium or PEEK framework versus conventional complete denture: a crossover trial. Alex Dent J 2024; 49 (01) 116-123
- 26 Al-Magaleh WR, Swelem AA, Radi IAW. The effect of 2 versus 4 implants on implant stability in mandibular overdentures: a randomized controlled trial. J Prosthet Dent 2017; 118 (06) 725-731
- 27 Heydecke G, Thomason JM, Awad MA, Lund JP, Feine JS. Do mandibular implant overdentures and conventional complete dentures meet the expectations of edentulous patients?. Quintessence Int 2008; 39 (10) 803-809
- 28 Cune M, van Kampen F, van der Bilt A, Bosman F. Patient satisfaction and preference with magnet, bar-clip, and ball-socket retained mandibular implant overdentures: a cross-over clinical trial. Int J Prosthodont 2005; 18 (02) 99-105
- 29 Al-Harbi S. Implant-supported milled bar mandibular overdenture with locator attachments: clinical considerations and laboratory techniques. Int Dent 2006; 8: 54-64
- 30 Pan YH, Ramp LC, Liu PR. Patient responses to dental implant-retained mandibular overdenture therapy: a 6-year clinical study. Chang Gung Med J 2007; 30 (04) 363-369
- 31 Shady M, Emera R, Hegazy SA, Kenawy M. Bar locator versus bar clip attachment for implant-assisted mandibular overdenture. Dentistry 2014; 6: 1122-2161
- 32 ELsyad MA, Abdraboh AE, Denewar MM, Mohamed SS. Prosthetic complications and maintenance of different attachments used to stabilize mandibular 2-implant overdentures in patients with atrophied ridges. A 5-year randomized controlled clinical trial. Clin Implant Dent Relat Res 2022; 24 (04) 497-509
- 33 Elsyad MA, Khairallah AS, Shawky AF. Changes in the edentulous maxilla with ball and telescopic attachments of implant-retained mandibular overdentures: a 4-year retrospective study. Quintessence Int 2013; 44 (07) 487-495
Address for correspondence
Publication History
Article published online:
20 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Heckmann SM, Heussinger S, Linke JJ, Graef F, Pröschel P. Improvement and long-term stability of neuromuscular adaptation in implant-supported overdentures. Clin Oral Implants Res 2009; 20 (11) 1200-1205
- 2 Borges GA, Barbin T, Dini C. et al. Patient-reported outcome measures and clinical assessment of implant-supported overdentures and fixed prostheses in mandibular edentulous patients: a systematic review and meta-analysis. J Prosthet Dent 2022; 127 (04) 565-577
- 3 Yilmaz B, Ozkir E, Johnston WM, McGlumphy E. Dislodgement force analysis of an overdenture attachment system. J Prosthet Dent 2020; 123 (02) 291-298
- 4 Salehi R, Shayegh SS, Johnston WM, Hakimaneh SMR. Effects of interimplant distance and cyclic dislodgement on retention of LOCATOR and ball attachments: an in vitro study. J Prosthet Dent 2019; 122 (06) 550-556
- 5 Feine JS, Carlsson GE, Awad MA. et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Montreal, Quebec, May 24-25, 2002. Int J Oral Maxillofac Implants 2002; 17 (04) 601-602
- 6 Naert I, Gizani S, Vuylsteke M, van Steenberghe D. A 5-year randomized clinical trial on the influence of splinted and unsplinted oral implants in the mandibular overdenture therapy. Part I: Peri-implant outcome. Clin Oral Implants Res 1998; 9 (03) 170-177
- 7 ELsyad MA, Emera RMK, Ashmawy TM. Effect of different bar designs on axial and nonaxial retention forces of implant-retained maxillary overdentures: an in vitro study. Int J Oral Maxillofac Implants 2019; 34 (01) 31-38
- 8 de la Rosa Castolo G, Guevara Perez SV, Arnoux PJ, Badih L, Bonnet F, Behr M. Implant-supported overdentures with different clinical configurations: mechanical resistance using a numerical approach. J Prosthet Dent 2019; 121 (03) 546.e1-546.e10
- 9 Shafie HR. Clinical and Laboratory Manual of Implant Overdentures. John Wiley & Sons; 2013
- 10 Seo YH, Bae EB, Kim JW. et al. Clinical evaluation of mandibular implant overdentures via Locator implant attachment and Locator bar attachment. J Adv Prosthodont 2016; 8 (04) 313-320
- 11 Kim MS, Yoon MJ, Huh JB, Jeon YC, Jeong CM. Implant overdenture using a locator bar system by drill and tapping technique in a mandible edentulous patient: a case report. J Adv Prosthodont 2012; 4 (02) 116-120
- 12 Wei L, Ma Q, Qin X, Pan S. In vitro cyclic dislodging test on retentive force of two types of female parts of SFI-Bar. Int J Prosthodont 2016; 29 (03) 293-295
- 13 Matarasso S, Iorio Siciliano V, Aglietta M, Andreuccetti G, Salvi GE. Clinical and radiographic outcomes of a combined resective and regenerative approach in the treatment of peri-implantitis: a prospective case series. Clin Oral Implants Res 2014; 25 (07) 761-767
- 14 Tosun B, Uysal N. Examination of oral health quality of life and patient satisfaction in removable denture wearers with OHIP-14 scale and visual analog scale: a cross-sectional study. BMC Oral Health 2024; 24 (01) 1353
- 15 Revilla-León M, Yilmaz B, Kois JC, Att W. Prevention of peri-implant disease in edentulous patients with fixed implant rehabilitations. Clin Implant Dent Relat Res 2023; 25 (04) 743-751
- 16 Chai HH, Gao SS, Chen KJ, Lo ECM, Duangthip D, Chu CH. Tools evaluating child oral health–related quality of life. Int Dent J 2024; 74 (01) 15-24
- 17 Mahanna FF, Elsyad MA, Mourad SI, Abozaed HW. Satisfaction and oral health-related quality of life of different attachments used for implant-retained overdentures in subjects with resorbed mandibles: a crossover trial. Int J Oral Maxillofac Implants 2020; 35 (02) 423-431
- 18 Ahuja S, Cagna DR. Classification and management of restorative space in edentulous implant overdenture patients. J Prosthet Dent 2011; 105 (05) 332-337
- 19 Abozaed HW. Patient satisfaction and oral health-related quality of life of quadrilateral bar versus bilateral linear bar for mandibular implant overdenture: randomized controlled clinical trial. Eur J Dent 2025; Epub ahead of print.
- 20 Mourad KE, Emera RMK, Habib A. Effect of different implant positions for two implant-retained mandibular overdenture: a retrospective 5-years radiographic evaluation of the circumferential peri-implant bone loss and posterior ridge resorptive changes. BMC Oral Health 2024; 24 (01) 1161
- 21 de Souza RF, Bedos C, Esfandiari S. et al. Single-implant overdentures retained by the Novaloc attachment system: study protocol for a mixed-methods randomized cross-over trial. Trials 2018; 19 (01) 243
- 22 Elsyad MA. Patient satisfaction and prosthetic aspects with mini-implants retained mandibular overdentures. A 5-year prospective study. Clin Oral Implants Res 2016; 27 (07) 926-933
- 23 Elsyad MA, Mostafa AZ. Effect of telescopic distal extension removable partial dentures on oral health related quality of life and maximum bite force: a preliminary cross over study. J Esthet Restor Dent 2018; 30 (01) 14-21
- 24 Elsyad MA, Khairallah AS. Chewing efficiency and maximum bite force with different attachment systems of implant overdentures: a crossover study. Clin Oral Implants Res 2017; 28 (06) 677-682
- 25 El-Waseef FA, Abozaed HW. Patient satisfaction and oral health–related quality of life for single-implant mandibular overdentures reinforced by cobalt chromium or PEEK framework versus conventional complete denture: a crossover trial. Alex Dent J 2024; 49 (01) 116-123
- 26 Al-Magaleh WR, Swelem AA, Radi IAW. The effect of 2 versus 4 implants on implant stability in mandibular overdentures: a randomized controlled trial. J Prosthet Dent 2017; 118 (06) 725-731
- 27 Heydecke G, Thomason JM, Awad MA, Lund JP, Feine JS. Do mandibular implant overdentures and conventional complete dentures meet the expectations of edentulous patients?. Quintessence Int 2008; 39 (10) 803-809
- 28 Cune M, van Kampen F, van der Bilt A, Bosman F. Patient satisfaction and preference with magnet, bar-clip, and ball-socket retained mandibular implant overdentures: a cross-over clinical trial. Int J Prosthodont 2005; 18 (02) 99-105
- 29 Al-Harbi S. Implant-supported milled bar mandibular overdenture with locator attachments: clinical considerations and laboratory techniques. Int Dent 2006; 8: 54-64
- 30 Pan YH, Ramp LC, Liu PR. Patient responses to dental implant-retained mandibular overdenture therapy: a 6-year clinical study. Chang Gung Med J 2007; 30 (04) 363-369
- 31 Shady M, Emera R, Hegazy SA, Kenawy M. Bar locator versus bar clip attachment for implant-assisted mandibular overdenture. Dentistry 2014; 6: 1122-2161
- 32 ELsyad MA, Abdraboh AE, Denewar MM, Mohamed SS. Prosthetic complications and maintenance of different attachments used to stabilize mandibular 2-implant overdentures in patients with atrophied ridges. A 5-year randomized controlled clinical trial. Clin Implant Dent Relat Res 2022; 24 (04) 497-509
- 33 Elsyad MA, Khairallah AS, Shawky AF. Changes in the edentulous maxilla with ball and telescopic attachments of implant-retained mandibular overdentures: a 4-year retrospective study. Quintessence Int 2013; 44 (07) 487-495