

Subscribe to RSS
DOI: 10.1055/s-0045-1814757
One-Stage Posterior Open Fixation with SpineJack Expansion Kyphoplasty for Unstable A4 Complete Thoracolumbar Burst Fracture with Neurological Deficit: A Proof-of-Concept Case Series
Authors

Abstract
Objectives
Usually, complete burst fractures of the thoracolumbar spine responsible for neurological deficit are managed with posterior open long-segment fixation, laminectomy, and second-stage anterior corpectomy. Although SpineJack expansion kyphoplasty allows for one-stage posterior-only restoration of the anterior and middle columns of the spine, to date, it has not been employed for complete burst fracture with neurological deficit.
Materials and Methods
Review of all cases of AO Spine A4 thoracolumbar complete burst fractures with neurological deficit treated by a single senior spine surgeon at Sainte-Anne Military Teaching Hospital using the same surgical procedure—SpineJack expansion kyphoplasty, posterior pedicle screw fixation, and posterior decompression—between November 2023 and October 2025.
Results
There were five patients with a mean age of 42.6 ± 16.8 years. Levels involved were T12, L1, L2, and L3 (patients 1–4), and combined L2L3 in a last severe trauma case (patient 5). Neurological deficit was classified as American Spinal Injury Association (ASIA) C in four cases, and ASIA B in patient 5. Mean preoperative loss of vertebral body height was 54 ± 10.3% and regional kyphosis 22.8 ± 4.4 degrees. Mean postoperative length of stay was 16.2 ± 24.6 days, and 5.3 ± 2.5 days excluding patient 5. Patients 1 to 4 returned to work after a mean delay of 3.3 ± 0.5 months. At the 1-year follow-up, the mean visual analog scale score was 2.8 ± 0.5, the mean Oswestry Disability Index was 7.6 ± 5.2, the mean segmental kyphosis was 4.2 ± 6.9 degrees, and the mean loss of vertebral body height was 11.2 ± 8.9%.
Conclusion
SpineJack expansion kyphoplasty combined with short-segment monoaxial pedicle screw fixation and laminectomy is a possible one-stage surgical treatment option for complete burst fracture of the thoracolumbar spine with neurological deficit.
Keywords
spine trauma - complete burst - spinal compression fracture - ASIA scale - SpineJack - expansion kyphoplastyIntroduction
Compression burst fractures of the thoracolumbar spine are frequent lesions that occur in up to 7% of high-energy blunt trauma.[1] Such injuries induce the mechanical failure of the anterior and middle columns of Denis,[2] responsible for particularly strong lever arms on the surgical construct, all the more at the thoracolumbar junction. Traditionally, patients suffering from AO Spine A4[3] complete burst fractures of the thoracolumbar spine were treated with open long-segment posterior fixation and decompression, followed by second-staged corpectomy.[4] [5] This surgical strategy greatly reduced the lower back's flexibility and induced surgical morbidity owing to the anterior retroperitoneal approach.[6]
The advent of expansion kyphoplasty using SpineJack titanium implants, combined with short-segment posterior fixation, allowed for one-stage posterior-only surgical treatment of most spinal burst fractures.[7] [8] To date, this well-known spinal surgical procedure has not been employed for complete burst fractures with neurological deficit, aside from cases with complete paraplegia,[9] probably because of the technical difficulty of placing the implants in the comminuted vertebral body and the concern about cement leakage into the spinal canal.
Hence, we present our initial experience of performing open SpineJack expansion kyphoplasty for patients suffering from a complete burst fracture of the thoracolumbar spine responsible for neurological deficit.
Materials and Methods
Inclusion Criteria
We retrospectively reviewed all patients who were admitted to the neurosurgery department of Sainte-Anne Military Teaching Hospital during a 2-year recruitment period, between November 2023 and October 2025, for complete burst fracture of the thoracolumbar spine with an important recess of the posterior wall responsible for neurological deficit. These fractures had to be classified A4 according to the AO Spine system.[3]
All these fractures displayed a posterior vertical “lamina greenstick fracture,”[10] [11] [12] a pathognomonic pattern of “burst” fractures according to the AO Spine classification system.[3] The patients had to be treated by the senior author using SpineJack titanium implants placed in the fractured vertebral body.
Exclusion Criteria
We voluntarily excluded from this patient series all the operated cases of incomplete burst fractures classified A3 on the AO Spine system, but also the operated cases of A4 complete burst fractures without neurological deficit.
Indeed, the aim of the present study was to demonstrate the feasibility, the safety, and the long-term efficacy of single-stage posterior fixation with SpineJack implant for complete burst fractures with neurological deficit, owing to the fact that it has never been reported before for this precise trauma indication.
Surgical Procedure
All patients were operated on by a single senior spine surgeon, in the prone position, with curare administration to relax erector spinae muscles. First, the thoracolumbar burst fracture was reduced using ligamentotaxis by placing thick surgical pads under the thorax and the upper thighs, thus providing hyperlordosis.
An open posterior approach was performed. Thanks to proper patient positioning, the collapsed vertebral body displayed sufficient re-expansion to introduce appropriate reamers, and then large titanium SpineJack implants (Stryker) with a total implant length of 28 mm and a diameter of 5.8 mm, allowing deployment of the 20-mm plates up to a 20-mm height. The implants were voluntarily placed close to the anterior wall, thus optimizing vertebral body expansion. SpineJack implants were completely expanded, regardless of whether their upper plates extended into the disc above the broken superior vertebral endplate ([Fig. 1]).

Under biplane fluoroscopy control, 4 to 6 mL of high-viscosity radiopaque VertaPlex cement was injected very slowly through one working channel, at least until the double cross sign appeared,[13] making sure the other working channel was opened, thus reducing injection pressure and consequently the odds for cement leakage into the spinal canal. Placing jack implants close to the anterior wall also reduced the odds of posterior cement leak. Then, 2mL of cement was injected very slowly inside the other working channel ([Fig. 1]). Exceptionally, in patients with large anatomy, up to 11mL of cement has been injected in a single vertebra in order to obtain “armed concrete” reconstruction of the anterior column of the spine.
Second, monoaxial pedicle screws were placed one level above and below the involved spine level. Slightly too long curved rods and bolts were placed, and bilateral distraction maneuvers were performed using the specific tool under lateral fluoroscopy guidance, allowing restoration of the native sagittal balance of the spine ([Fig. 1]).
Finally, posterior decompression including laminectomy and bilateral arthrectomy was performed. Thanks to such wide posterior bone decompression, slight cement leakage into the spinal canal was never an issue.
The surgical technique described earlier has already been detailed previously.[14] [15]
Data Extraction
Clinical data, including back pain according to the visual analog scale (VAS) and patient-reported functional impairment according to the Oswestry Disability Index (ODI), as well as radiologic parameters, including the loss of vertebral body height and the posttraumatic kyphosis, were assessed before surgery, at 6 months, and finally, after 1 year. Vertebral body fusion was assessed at the 1-year follow-up using computed tomography scan and standing radiographs of the spine.
Results
Five patients were included with a mean age of 42.6 ± 16.8 years ([Table 1]). The levels involved were T12, L1, L2, and L3 one time each ([Table 1], patients 1–4), and L2L3 in a severe trauma patient ([Table 1], patient 5). All patients presented with neurological deficit, which was classified C on the American Spinal Injury Association (ASIA) scale in four cases ([Table 1], patients 1–4), and B in 1 case ([Table 1], patient 5).[16] All the patients were operated on using SpineJack expansion kyphoplasty of the affected spine level(s), and short segment monoaxial pedicle screw fixation, that is, one level above and one level below the fractured level, whenever possible. Distraction on the pedicle screws provided supplementary gain of vertebral body height. Eventually, a laminectomy and arthrectomy provided spinal canal decompression ([Fig. 2]).
|
Patient no. |
Age (y) sex |
Fracture level |
Preoperative ASIA |
Preoperative VAS |
Preoperative ODI |
Preoperative vertebral loss of height (%)/kyphosis (deg) |
Index surgery |
Posttraumatic dural tear |
Revision surgery |
Length of stay (d) |
6-month /1-year ODI (/100) |
6-month VAS (/10) |
1-year ASIA |
1-year vertebral loss of height (%)/kyphosis (deg) |
Return to work (mo) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
1 |
39 ♂ |
L1 |
C |
10 |
100 |
50/20 |
SJ L1, PSF +2–2, L |
No |
– |
4 |
6/12 |
2 |
E |
11/0 |
3 |
|
2 |
22 ♀ |
L3 |
C |
10 |
100 |
56/30 |
SJ L3, PSF +1–1, L |
Yes |
Pseudomeningocele closure postoperative day 7 |
9 |
2/2 |
3 |
E |
0/0 |
4 |
|
3 |
33 ♀ |
L2 |
C |
10 |
100 |
52/24 |
SJ L2, PSF +1–1, L |
No |
– |
4 |
14/12 |
3 |
E |
10/5 |
3 |
|
4 |
56 ♂ |
T12 |
C |
10 |
100 |
70/20 |
SJ T12, PSF +1–1, L |
No |
– |
4 |
10/10 |
3 |
E |
25/16 |
3 |
|
5 |
63 ♀ |
L2L3 |
B |
10 |
100 |
42/20 |
SJ L2L3, PSF +1–1, L |
Yes |
– |
60 |
– |
2[a] |
C[a] |
– |
Abbreviations: L, laminectomy; ODI, Oswestry Disability Index; PSF, pedicle screw fixation; SJ, SpineJack; VAS, visual analog scale.
a Only 3-month follow-up available for patient number 5.

It is to note that, in two cases, a greenstick lamina fracture recessed within the spinal canal was responsible for a posttraumatic dural tear with trapped rootlets ([Table 1], patients 2 and 5).[10] [12] Cautious reintegration of nerve roots using neurosurgical patties, and then watertight microsurgical continuous dural closure using 5.0 Prolene was performed. Despite this, patient 2 required revision surgery for another round of microsurgical closure of dural tear owing to symptomatic pseudomeningocele causing intracranial hypotension, which resolved immediately after the revision procedure ([Fig. 3]).

Surgical procedure lasted an average of 150 minutes, and 210 minutes in case of posttraumatic dural tear requiring microsurgical closure. Intraoperative blood loss was below 400 mL in all cases, and none of the patients required blood transfusion.
On postoperative computed tomography scan, there was minimal cement leakage into the paravertebral area and the spinal canal in every case, without any clinical consequences, though. Mean hospital stay was 5.3 ± 2.5 days, considering patients 1 to 4, and 16.2 ± 24.6 days, taking into account patient 5 who suffered from severe trauma. The three patients with intact dura mater were discharged home on postoperative day 4. Patient 2 was discharged on postoperative day 9, that is, 2 days after revision surgery for closure of posttraumatic pseudomeningocele. All these patients were discharged home free of neurological deficit. Finally, patient 5 was discharged to rehabilitation 60 days after hospital admission.
Patients 1 to 4 were followed up for 12 months, whereas patient 5 recently attended her 3-month follow-up visit. Clinically speaking, all patients steadily improved after surgical fixation compared with preoperative status, notably according to the 6-month back pain according to VAS (2.6 ± 0.5 vs. 10/10 upon admission), and also to the ODI (8.0 ± 5.2 at 6 months, and 7.6 ± 5.2 at 1 year, vs. 100/100 upon admission). Patients 1 to 4 returned to work after a mean delay of 3.3 ± 0.5 months.
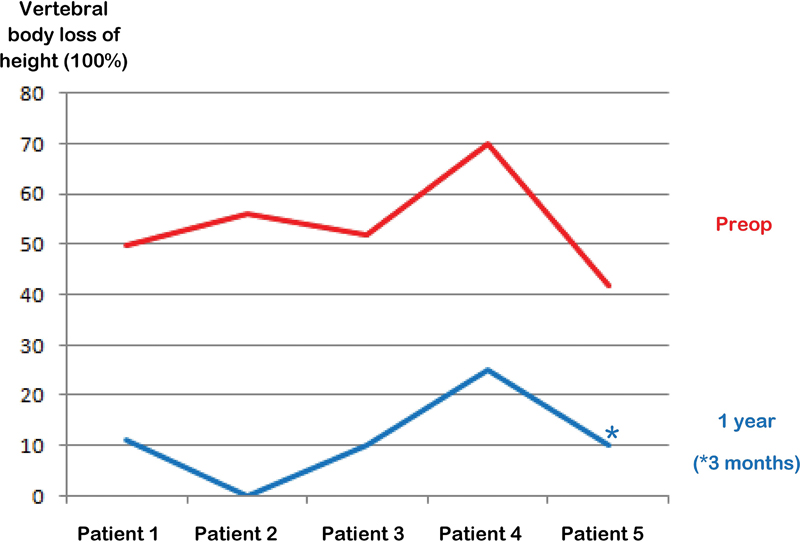
Sagittal parameters, including loss of vertebral body height (11.2 ± 8.9% vs. 54 ± 10.3%, [Fig. 4]) and segmental kyphosis (4.2 ± 6.9 vs. 22.8 ± 4.4 degrees, [Fig. 5]) also steadily improved on standing lateral X-ray until the 1-year follow-up visit compared with the preoperative period. All comminuted vertebral bodies showed proper fusion.

Discussion
Biomechanical Context of Thoracolumbar Burst Fractures
During surgical treatment of AO Spine A4 complete fractures of the thoracolumbar spine, spine surgeons should be aware of the greater risk of neurological compromise compared with A3 incomplete burst fractures, owing notably to improper reduction of the bone fragments recessed into the spinal canal, insufficient posterior surgical decompression of the spinal canal, and the risk of cement leakage through the posterior wall in case of associated kyphoplasty.
Besides, one should take into account the higher odds for vertebral body symptomatic pseudarthrosis because of the comminuted character of a complete burst fracture.
We believe that all these issues can be properly addressed with the above-mentioned surgical technique.
Biomechanical Advantages of SpineJack Expansive Implants
First, a SpineJack implant properly placed, that is, right behind the anterior wall and right below the upper endplate, usually allows for the regain of native vertebral body height. For this purpose, we use the largest SpineJack implants developed by Stryker, that is, with a diameter of 5.8 mm and a total length of 28 mm, whenever possible. Patient positioning with hyperlordosis generally provides sufficient vertebral body expansion, thus enabling jack implant insertion. If not, a complementary distraction maneuver on monoaxial pedicle screws allows gaining sufficient vertebral body height to place the kyphoplasty implants.[14]
The restoration of native vertebral body shape participates in reducing the rate of pseudoarthrosis. Monoaxial pedicle screw fixation provides the supplementary stability to achieve this goal. This way, jack implant combined with monoaxial pedicle screw fixation allows for posterior-only reconstruction of the damaged anterior and middle columns of Denis.[2]
Surgical Tips Allowing an Optimal Functional Result
In thoracolumbar complete burst fractures, the posterior longitudinal ligament may be partially disrupted. This being said, the present technique uses ligamentotaxis with hyperlordosis, expansion kyphoplasty, and even distraction on monoaxial screws to make the bone fragments recessed in the spinal canal reintegrate into the vertebral body, thus providing indirect neurological decompression.
Very slow unilateral cement injection under repeated fluoroscopy guidance, while keeping the contralateral working channel open, reduces the odds for clinically significant cement leakage.
Wide posterior bone decompression with laminectomy and arthrectomy is performed, freeing the spinal canal and the lateral recess regardless of the remaining presence of anterior recessed bone fragments or even cement leakage.[14] Finally, short segment posterior fixation allows for the patient to keep nearly physiological lower back flexibility, without the need for implant removal.
Pros and Cons of Posterior Open SpineJack versus Anterolateral Corporectomy
One-stage posterior three columns reconstruction using SpineJack implants, as described earlier, allows us to avoid the need for anterolateral lumbar corpectomy ([Fig. 6]). Indeed, lumbar corpectomy carries rare though severe complications, including notably vascular injury, bowel or urogenital perforation, and retrograde ejaculation caused by injury to the lumbar sympathetic chain,[6] even in experienced hands.[5] [17]

Very recently, a few authors have proposed single-stage posterior-only pedicle screw fixation combined with transpedicular nerve root sparing corpectomy. Nevertheless, such a technique requires extensive muscle dissection and long-segment fixation,[18] [19] [20] both being major drawbacks that we aim to avoid with the use of SpineJack implants.
Limitations
First, thoracolumbar burst fractures generally involve the thoracolumbar junction and the lumbar spine. Hence, even “complete burst” cases of thoracolumbar compression fractures, displaying important posterior wall recess and greenstick fracture of the lamina, are rarely responsible for complete neurological deficit of the lower limbs, thanks to the compliance of the rootlets of the cauda equina.[3] [10] [11] This may explain why the patients included here only displayed incomplete neurological deficit, classified B to C on the ASIA scale.[16]
Second, the decision to place SpineJack implants inside the comminuted fractured vertebral body of a complete burst with neurological compromise remains a matter of debate. Hence, “neurological compromise” stands as a contraindication for the use of SpineJack implants according to the manufacturer (Stryker). As such, many spine surgeons still fear, justly, for cement leakage into the spinal canal when treating a case of burst fracture with kyphoplasty. Besides, from a biomechanical point of view, I do not believe that all spine surgeons would trust SpineJack implants to provide sufficient vertebral body expansion, and the cement to provide sufficient biomechanical rigidity, to allow for keeping proper fracture realignment in the long term, even with complementary short-segment fixation.
This may explain why, to our knowledge, this innovative and demanding technique has only been reported by the senior author for the surgical treatment of complete burst fractures of the thoracolumbar spine with incomplete neurological deficit. This accounts for the small size of this patient series.
Even though past evidence still supports posterior fixation followed by anterior corpectomy as the gold standard for surgical treatment of thoracolumbar complete burst fractures,[5] [17] we hope that this patient series can lay the foundations for a promising and less invasive surgical alternative.[14] [15]
Conclusion
One-stage posterior-only open SpineJack expansion kyphoplasty combined with short-segment monoaxial screw fixation and laminoarthrectomy is a technically demanding, but feasible, safe, and efficient surgical option for complete burst fracture of the thoracolumbar spine with neurological deficit. The favorable long-term functional and radiologic results of this small patient series indicate that it could become a valuable surgical option for these heavily injured patients. More powerful studies and the reproducibility of this technique by other spine surgeons are mandatory before generalization, though.
Conflict of Interest
None declared.
Ethical Approval
This study was approved by the National Committee of the French College of Neurosurgeons on June 17, 2025, under the reference number IRB00011687. This work was conducted according to the Declaration of Helsinki of 1964 and any of its further amendments.
-
References
- 1 Katsuura Y, Osborn JM, Cason GW. The epidemiology of thoracolumbar trauma: A meta-analysis. J Orthop 2016; 13 (04) 383-388
- 2 Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 1983; 8 (08) 817-831
- 3 Vaccaro AR, Oner C, Kepler CK. et al; AOSpine Spinal Cord Injury & Trauma Knowledge Forum. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine 2013; 38 (23) 2028-2037
- 4 Greiner-Perth A-K, Wilke H-J, Liebsch C. Which spinal fixation technique achieves which degree of stability after thoracolumbar trauma? A systematic quantitative review. Spine J 2024
- 5 Graillon T, Rakotozanany P, Blondel B, Adetchessi T, Dufour H, Fuentes S. Circumferential management of unstable thoracolumbar fractures using an anterior expandable cage, as an alternative to an iliac crest graft, combined with a posterior screw fixation: results of a series of 85 patients. Neurosurg Focus 2014; 37 (01) E10
- 6 Piche JD, Butt B, Ahmady A. et al. Lateral lumbar corpectomy: indications and surgical technique with review of the literature. Semin Spine Surg 2022; 34: 100949
- 7 Venier A, Roccatagliata L, Isalberti M. et al. Armed kyphoplasty: an indirect central canal decompression technique in burst fractures. AJNR Am J Neuroradiol 2019; 40 (11) 1965-1972
- 8 Fuentes S, Blondel B, Metellus P, Gaudart J, Adetchessi T, Dufour H. Percutaneous kyphoplasty and pedicle screw fixation for the management of thoraco-lumbar burst fractures. Eur Spine J 2010; 19 (08) 1281-1287
- 9 Woodruff R, Marco RAW. Use of kyphoplasty versus 360-degree fusion for unstable thoracolumbar burst fractures: using minimally invasive techniques in trauma. Semin Spine Surg 2013; 25: 176-181
- 10 Shi X, Xiang S, Dai B, He Z. Association of the presence and its types of lamina fractures with posterior dural tear and neurological deficits in traumatic thoracic and lumbar burst fractures. BMC Musculoskelet Disord 2021; 22 (01) 300
- 11 Yan L, Liu Y, He B, Liu J, Luo Z, Hao D. Clinical case-series report of traumatic cauda equina herniation: a pathological phenomena occurring with thoracolumbar and lumbar burst fractures. Medicine (Baltimore) 2017; 96 (14) e6446
- 12 Aydinli U, Karaeminoğullari O, Tişkaya K, Oztürk C. Dural tears in lumbar burst fractures with greenstick lamina fractures. Spine 2001; 26 (18) E410-E415
- 13 Chang C-J, Hong C-K, Hsu C-C. “Double Cross Sign” could be an indicator of an adequate amount of bone cement in kyphoplasty with the SpineJack system: a retrospective study. Diagnostics (Basel) 2022; 12 (12) 3068
- 14 Beucler N. How I do it: SpineJack expansion kyphoplasty for AO spine A4 complete burst fracture with neurological deficit. Acta Neurochir (Wien) 2024; 166 (01) 457
- 15 Beucler N. Single-staged three columns reconstruction of thoracolumbar AO Spine A4 burst fracture with traumatic canal stenosis causing neurological deficit using posterior open monoaxial pedicle screw distraction fixation, laminectomy, and titanium jack implant expansion kyphoplasty to avoid the need for corpectomy: an elegant proof-of-concept case. Neurosurg Rev 2024; 47 (01) 267
- 16 American Spinal Injury Association (ASIA). Ninth annual scientific meeting April 11th-13th, 1983, Denver, Colorado, U.S.A. Abstracts. Paraplegia 1984; 22 (01) 45-54
- 17 Meyer M, Noudel R, Farah K. et al. Isolated unstable burst fractures of the fifth lumbar vertebra: functional and radiological outcome after posterior stabilization with reconstruction of the anterior column: About 6 cases and literature review. Orthop Traumatol Surg Res 2020; 106 (06) 1215-1220
- 18 Chen C, Wu C, Wang W, Wang X. Single-stage posterior unilateral transpedicular corpectomy with circumferential reconstructive stabilization for the treatment of severe thoracic and lumbar complete burst fractures. Global Spine J 2025;16(1):21925682251338789
- 19 Haddadi K, Hosseini SM, Khadem A, Hashemian MB. One-stage posterior only corpectomy and fusion in the treatment of a unique acute low lumbar L4 burst fracture without neurologic deficit: a case presentation. Asian J Neurosurg 2020; 15 (03) 691-694
- 20 Graillon T, Rakotozanany P, Blondel B, Adetchessi T, Dufour H, Fuentes S. Circumferential management of unstable thoracolumbar fractures using an anterior expandable cage, as an alternative to an iliac crest graft, combined with a posterior screw fixation: results of a series of 85 patients. Neurosurg Focus 2014; 37 (01) E10
Address for correspondence
Publication History
Article published online:
22 January 2026
© 2026. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Katsuura Y, Osborn JM, Cason GW. The epidemiology of thoracolumbar trauma: A meta-analysis. J Orthop 2016; 13 (04) 383-388
- 2 Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 1983; 8 (08) 817-831
- 3 Vaccaro AR, Oner C, Kepler CK. et al; AOSpine Spinal Cord Injury & Trauma Knowledge Forum. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine 2013; 38 (23) 2028-2037
- 4 Greiner-Perth A-K, Wilke H-J, Liebsch C. Which spinal fixation technique achieves which degree of stability after thoracolumbar trauma? A systematic quantitative review. Spine J 2024
- 5 Graillon T, Rakotozanany P, Blondel B, Adetchessi T, Dufour H, Fuentes S. Circumferential management of unstable thoracolumbar fractures using an anterior expandable cage, as an alternative to an iliac crest graft, combined with a posterior screw fixation: results of a series of 85 patients. Neurosurg Focus 2014; 37 (01) E10
- 6 Piche JD, Butt B, Ahmady A. et al. Lateral lumbar corpectomy: indications and surgical technique with review of the literature. Semin Spine Surg 2022; 34: 100949
- 7 Venier A, Roccatagliata L, Isalberti M. et al. Armed kyphoplasty: an indirect central canal decompression technique in burst fractures. AJNR Am J Neuroradiol 2019; 40 (11) 1965-1972
- 8 Fuentes S, Blondel B, Metellus P, Gaudart J, Adetchessi T, Dufour H. Percutaneous kyphoplasty and pedicle screw fixation for the management of thoraco-lumbar burst fractures. Eur Spine J 2010; 19 (08) 1281-1287
- 9 Woodruff R, Marco RAW. Use of kyphoplasty versus 360-degree fusion for unstable thoracolumbar burst fractures: using minimally invasive techniques in trauma. Semin Spine Surg 2013; 25: 176-181
- 10 Shi X, Xiang S, Dai B, He Z. Association of the presence and its types of lamina fractures with posterior dural tear and neurological deficits in traumatic thoracic and lumbar burst fractures. BMC Musculoskelet Disord 2021; 22 (01) 300
- 11 Yan L, Liu Y, He B, Liu J, Luo Z, Hao D. Clinical case-series report of traumatic cauda equina herniation: a pathological phenomena occurring with thoracolumbar and lumbar burst fractures. Medicine (Baltimore) 2017; 96 (14) e6446
- 12 Aydinli U, Karaeminoğullari O, Tişkaya K, Oztürk C. Dural tears in lumbar burst fractures with greenstick lamina fractures. Spine 2001; 26 (18) E410-E415
- 13 Chang C-J, Hong C-K, Hsu C-C. “Double Cross Sign” could be an indicator of an adequate amount of bone cement in kyphoplasty with the SpineJack system: a retrospective study. Diagnostics (Basel) 2022; 12 (12) 3068
- 14 Beucler N. How I do it: SpineJack expansion kyphoplasty for AO spine A4 complete burst fracture with neurological deficit. Acta Neurochir (Wien) 2024; 166 (01) 457
- 15 Beucler N. Single-staged three columns reconstruction of thoracolumbar AO Spine A4 burst fracture with traumatic canal stenosis causing neurological deficit using posterior open monoaxial pedicle screw distraction fixation, laminectomy, and titanium jack implant expansion kyphoplasty to avoid the need for corpectomy: an elegant proof-of-concept case. Neurosurg Rev 2024; 47 (01) 267
- 16 American Spinal Injury Association (ASIA). Ninth annual scientific meeting April 11th-13th, 1983, Denver, Colorado, U.S.A. Abstracts. Paraplegia 1984; 22 (01) 45-54
- 17 Meyer M, Noudel R, Farah K. et al. Isolated unstable burst fractures of the fifth lumbar vertebra: functional and radiological outcome after posterior stabilization with reconstruction of the anterior column: About 6 cases and literature review. Orthop Traumatol Surg Res 2020; 106 (06) 1215-1220
- 18 Chen C, Wu C, Wang W, Wang X. Single-stage posterior unilateral transpedicular corpectomy with circumferential reconstructive stabilization for the treatment of severe thoracic and lumbar complete burst fractures. Global Spine J 2025;16(1):21925682251338789
- 19 Haddadi K, Hosseini SM, Khadem A, Hashemian MB. One-stage posterior only corpectomy and fusion in the treatment of a unique acute low lumbar L4 burst fracture without neurologic deficit: a case presentation. Asian J Neurosurg 2020; 15 (03) 691-694
- 20 Graillon T, Rakotozanany P, Blondel B, Adetchessi T, Dufour H, Fuentes S. Circumferential management of unstable thoracolumbar fractures using an anterior expandable cage, as an alternative to an iliac crest graft, combined with a posterior screw fixation: results of a series of 85 patients. Neurosurg Focus 2014; 37 (01) E10