

Subscribe to RSS
DOI: 10.1055/s-0045-1815733
Exploring the Outcomes of Hodgkin Lymphoma in Pediatric Patients: A Systematic Review from India
Authors
Funding None.

Abstract
Hodgkin lymphoma (HL) has emerged as one of the most curable pediatric cancers globally. However, in low- and middle-income countries like India, the treatment landscape is shaped by various biological, social, and resource-related factors, leading to variability in management approaches and outcomes. This systematic review aims to bring together the available data to provide an integrated overview of current management practices and outcome of childhood HL in India. Thirteen studies were reviewed, including 3 multicenter studies, with a total cohort of 1,766 children. The median age at diagnosis ranged from 7 to 10 years, with male-to-female ratios between 2.8:1 and 10.5:1. A significant proportion (70–80%) of children presented with advanced stages of the disease. Utilization of positron emission tomography-computed tomography for assessment was inconsistent across centers, and the use of radiotherapy (RT) varied widely. Most centers have reported 5-year overall survival and 5-year event-free survival of approximately 90% and above and 75 to 85%, respectively. Adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD) was the most widely used regimen; however, recent studies have used vincristine, etoposide, prednisolone, doxorubicin (OEPA)/cyclophosphamide, vincristine, prednisolone, dacarbazine (COPDAC) with the intent to reduce long-term side effects associated with radiation exposure. Treatment-related mortality of around 5% was noted with OEPA/COPDAC in Indian setting in contrast to ABVD, which is close to 1%. Feasibility and long-term benefits of the former chemotherapy need further follow-up. Challenges such as treatment abandonment and toxic deaths remain significant, and there is a notable lack of data on long-term outcomes and late effects, necessitating further research in these areas.
Introduction
The evolution of treatment over the past 4 to 5 decades has altered the outcome of pediatric Hodgkin lymphoma (HL) such that the majority of patients are cured. The inclusion of HL as one of the six index cancers in the World Health Organization-Global Initiative for Childhood Cancer initiative launched in 2018,[1] emphasizes the need to discuss and increase the awareness about it, especially in low- and middle-income countries (LMICs). Multiple collaborative trials in the West have come up with various treatment regimens based on risk-stratified and response-based approach with the aim of prevention of long-term side effects while maintaining the excellent cure rates.[2] [3] [4] Although LMICs, like India, have kept pace with changes in management of HL globally, there are significant variables that might affect outcome. The biologic and demographic differences observed in pediatric HL between the West and India include a higher male preponderance, poor nutritional status, younger age at presentation, and increased incidence of a mixed cellularity pathologic subtype in India.[5] With heterogeneity in the treatment approach and variable resource availability in India,[6] a systematic review is needed to understand the current management and outcome of childhood HL in India. The purpose of this review was to summarize and integrate the published literature on reported current management practices and outcome of pediatric HL from India. Recent collaborative efforts with prospective multicenter studies under the aegis of the Indian Pediatric Oncology Group (InPOG, which has recently been renamed the Indian Pediatric Hematology Oncology Group) has proven a crucial step toward a more streamlined approach in pediatric oncology in our country where resource limitation is a major determinant of outcomes.[7] [8] This review is an effort which will provide useful baseline information and overview of treatment strategies for HL across the country.
Materials and Methods
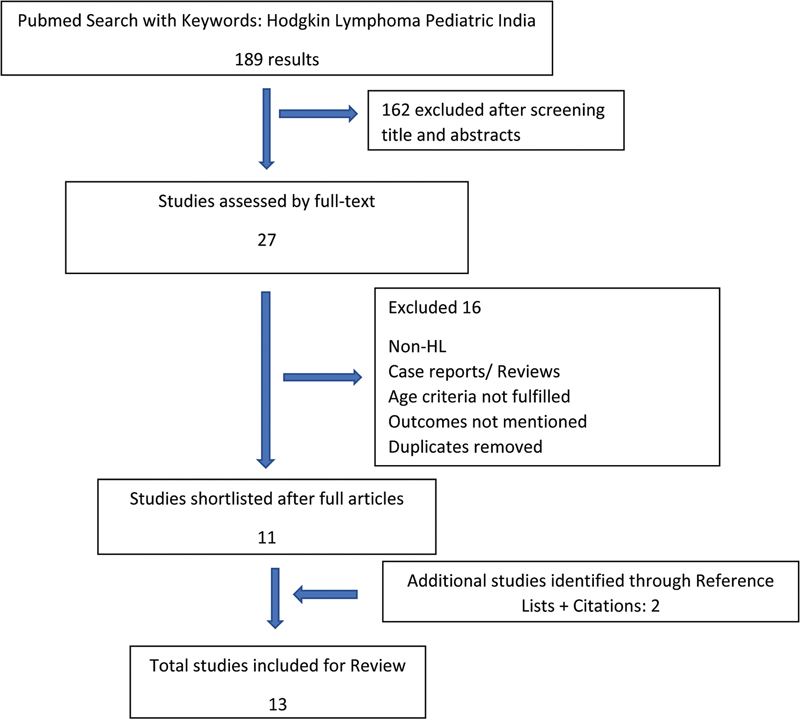
A search of Medline (via PubMed) using keywords “Hodgkin lymphoma,” “pediatric,” and “India” was done in January 2023. The search was limited to studies published from the year 2000 onward. Studies which reported outcomes on survival, related to pediatric HL (age < 18 years) were included. Title and abstracts of the search results were independently screened by two investigators (K.T. and R.S.A.) to identify potentially eligible studies. Full text of these was then screened to make the final decision. Analysis of the articles was done by two independent reviewers (C.V. and R.S.A.). Retrospective case–control studies, randomized control trials, and retrospective cohort studies were included in the review. Manual examination of reference lists as well as of citations (through Google Scholar) of included studies were done to identify any additional studies which may not have been identified in Medline. [Fig. 1] depicts the flow diagram for study selection approach.
The results of the searches were compared and merged. Any single or multicenter study from India was eligible for inclusion. If there were more than one study from the same institute, only the most recent was included. Case reports and studies reporting less than 20 cases were excluded. Where available, data for early stage (stage 1 and 2A) and advanced stage (stage 2B, 3, and 4) was also examined separately. Demographic and clinical variables were collected from the shortlisted studies. Chemotherapeutic and radiotherapy (RT) strategies used were also included. Key outcomes of the review included survival rates, mortality, relapse rates, disease progression, and treatment abandonment. The key features and outcomes of the selected studies were summarized in tabular form, and an overall narrative presentation synthesized the findings to provide insights into the current landscape of pediatric HL management in India.
Results
The studies included[5] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] [20] for this review along with their clinical and demographic details have been summarized in [Table 1]. Thirteen studies were included, which covered variable time periods (range 1988–2019). While most were single-center studies, three recent studies were multicenter studies including two InPOG collaborative studies with 27 participating centers across the country.[13] [19] [20] Together, they constituted 1,766 children with HL with the median age of children ranging from 7 to 10 years. There was male preponderance (majority of centers reported ratio of > 4:1) in all studies with male-to-female ratio ranging from 2.8:1 to 10.5:1. Most common histology noted was mixed cellularity followed by nodular sclerosis. A significant proportion of patients, approximately 70 to 80%, presented with advanced-stage disease, a finding that showed little variation between earlier and more recent studies, highlighting the persistent burden of advanced presentations. B symptoms were present in approximately half of the patients while bulky disease was present in a quarter of children. Most centers utilized contrast-enhanced computed tomography (CECT) for staging and response assessment; however, the increasing availability and affordability of positron emission tomography-CT (PET-CT) in recent times have led to its use for this purpose.
|
Study details |
Study period |
No. of patients |
Age group (y) |
M:F |
Advanced stage (≥ 2b) |
B symptoms |
Bulky disease |
Histology |
Chemotherapy[a] |
Staging and response assessment modality |
Indication and dose (in parenthesis) of radiotherapy |
Radiotherapy |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Chandra et al, 2008[9] |
1988–2004 |
35 |
< 18 |
10.5:1 |
83% |
NM |
NM |
MC 50.5%, NS 23.7%, LP 20% |
COPP X 6: 83%, COPP X 3 + ABVD X 3: 11.4%, ABVD X 6: 2.9% |
CT |
Bulky disease; (NM) |
11% |
|
Trehan et al, 2013[10] |
1990–2006 |
206 |
3–16 |
10.5:1 |
52% (≥ 3) |
54% |
NM |
MC 69.6% |
ABVD/ ABVD-COPP/ MOPP-COPP/OEPA |
CT |
No routine RT, Individualized decision; (NM) |
1.44% |
|
Verma and Kumar, 2015[11] |
1994–2012 |
184 |
< 15 |
7.4:1 |
82% |
79% |
19.10% |
MC 38%, NS 32%, LP 13.7% |
ABVD, COPP, COPP/ABV |
CT |
Incomplete or no response; (NM) |
6.5% |
|
Jain et al, 2016[12] |
1996–2013 |
167 |
< 18 |
9.4:1 |
31.80% |
43% |
16.70% |
MC 49.8%, NS 25.8%, LR 10.8% |
ABVD |
CT (PET in few) |
Bulky disease/PR; (20–36 Gy) |
30.50% |
|
Radhakrishnan et al, 2016[5] |
2001–2010 |
172 |
< 18 |
2.8:1 |
40% |
32% |
27% |
MC 45%, NS 35%, LP 2%, LD 1% |
ABVD (70%), ABV/COPP hybrid |
CT |
Bulky disease or PR; (bulky 20–30 Gy; PR 30–36 Gy) |
19% |
|
Bhethanabhotla et al, 2017[13] |
2003–2013 |
186 |
< 18 |
4.6:1 |
100% |
74.20% |
44.6% |
MC 44.1%, NS 32.2%, LR 2.7% |
ABVD |
CT/PET |
Bulky disease/PR/ extranodal disease; (25 Gy) |
40.30% |
|
Seth et al, 2015[14] |
2005–2010 |
35 |
< 13 |
7.7:1 |
65.70% |
60% |
25.70% |
MC 25.7%, NS 28.6%, LP 25.7% |
ABVD, BEACOPP in progression (2 cases) |
CT (PET in 10) |
PR; (20–30Gy) |
11.40% |
|
Gupta et al, 2019[15] |
2005–2014 |
90 |
< 15 |
7.2:1 |
87.80% |
87.80% |
15.60% |
MC 44.4%, NS 26.7% |
ABVD, COPP/ABVD, COPP |
CT |
Bony involvement; (NM) |
2.20% |
|
Jayabose et al, 2016[16] |
2010–2014 |
26 |
4–18 |
4.2:1 |
100% |
NM |
NM |
NM |
HR: mBEACOPP + ABVD, IR: ABVE-PC/ ABVE-PC + ABVD |
CT (PET in 7) |
PR; (NM) |
7.60% |
|
Palayullakandi et al, 2022[17] |
2010–2019 |
143 |
< 13 |
5.8:1 |
74% (TG2 and 3) |
46.2% |
58.9% |
NM |
OEPA/COPADAC |
PET-CT |
Inadequate PET response; (NM) |
21% |
|
Parambil et al, 2020[18] |
2013–2016 |
126 |
< 15 |
4.7:1 |
90.40% |
65.80% |
86.80% |
MC 27.2%, NS 19.3%, LR 7%, NS 46.5% |
LR: ABVD IR + HR: OEPA + COPDAC |
PET |
Bulky sites and ERA < CR; (19.8 Gy in bulky and 30.6 Gy in ERA < CR) |
76% |
|
Mahajan et al, 2021[19] |
2015–2018 |
134 |
< 18 |
5.7:1 |
0% |
NM |
39.50% |
NM |
ABVD X 4 cycles |
PET (49.2%) Rest CT |
Bulky sites, suboptimal ERA; (21Gy) |
39% |
|
Jain et al, 2022[20] |
2015–2018 |
262 |
< 18 |
5.2:1 |
100.00% |
75.50% |
50.30% |
NM |
ABVD X 6 cycles |
PET (44.6%) Rest CT |
Bulky sites, suboptimal ERA; (21Gy) |
42.30% |
Abbreviations: CR, complete response; CT, computed tomography; ERA, early response assessment; HR, high risk; IR, intermediate risk; LD, lymphocyte depleted; LP, lymphocytic predominance; LR, low risk; LR, lymphocyte rich; MC, mixed cellularity; NA, not applicable; NM, not mentioned; NS, nodular sclerosis; NS, not specified; PET, positron emission tomography; PR, partial response; TG: treatment groups as per Euronet-PHL-C1-protocol.
a Chemotherapy abbreviations: COPP, Cyclophosphamide, Oncovin [Vincristine], Procarbazine, Prednisolone; ABVD, Adriamycin [Doxorubicin], Bleomycin, Vinblastine, Dacarbazine; MOPP, nitrogen mustard, vincristine, procarbazine, prednisolone; ABV, Adriamycin, bleomycin, vinblastine; BEACOPP, bleomycin, etoposide, adriamycin, COPP; mBEACOPP, modified BEACOPP; ABVE-PC, Adriamycin, bleomycin, vincristine, etoposide, prednisone, cyclophosphamide; OEPA, vincristine, etoposide, prednisolone, doxorubicin; COPDAC, cyclophosphamide, vincristine, prednisolone, dacarbazine.
Chemotherapy
The most frequently employed chemotherapy regimen was Adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD), either alone or in combination with cyclophosphamide, Oncovin [vincristine], procarbazine, prednisolone (COPP), used by most centers. The same backbone was also used for the InPOG studies.[19] [20] Palayullakandi et al[17] and Parambil et al[18] have reported outcomes with Euronet-PHL-C1-protocol using OEPA-COPDAC-based chemotherapy.
Number of cycles and intensification by addition of other drugs was based on stage at presentation and early response assessment by CECT/PET. Number of ABVD cycles varied from 4 to 8 depending upon the stage of disease and individual institutional protocols. Early-stage disease received 4 to 6 cycles and advanced stage disease received 6 to 8 cycles. The treatment details have been described in [Table 1].
Radiotherapy
RT was incorporated in nearly all centers, with involved field radiation therapy being the preferred modality. The most common indications had been bulky disease and partial or no response on reassessment. Study by Bhethanabhotla et al involving patients from three centers have additionally given radiation to extranodal disease.[13] Two centers were not using radiation routinely and given radiation to occasional patients on individualized basis.[10] [15] In three studies[13] [16] [20] involving only advanced stage cases, indications were bulky disease/partial response/extranodal disease. Regardless of indication, in several studies, the proportion of children receiving radiation was around 10% or lower. On the other end of the spectrum, in one study, three out of four children with HL received RT.[18] Six studies have mentioned the dose of radiation given, which were 20 to 30 Gy in bulky disease and ranged from 25 to 36 Gy for partial response as shown in [Table 1].
Survival Outcomes
The survival outcomes as well as the events occurred have been outlined in [Table 2]. The median follow-up period ranged from 17 months to 5 years. For HL all stages combined, most of the centers have reported 5-year overall survival (OS) of around 90% and above except one center which has reported approximately 80% survival. Five-year event-free survival (EFS) reported by five studies has ranged from 75 to 85% with one outlier at the lower end of 53%.[11] Seven studies have also reported OS and EFS separately in early and advanced-stage disease. OS ranged from 90 to 100% in early stage and 70 to 95% in advanced-stage disease. Likewise, EFS ranged from 70 to 100% and 50 to 94% in early and advanced stage, respectively.
|
Study |
Progression on treatment/relapse/both (%) |
TRM |
Abandonment |
Overall OS |
Overall EFS |
Early stage OS |
Early stage EFS |
Late stage OS |
Late stage EFS |
|---|---|---|---|---|---|---|---|---|---|
|
Chandra et al, 2008[9] |
2.8/11.4/14.2 |
8.50% |
5.7% |
NM |
80% (5 y) |
NM |
NM |
NM |
NM |
|
Trehan et al, 2013[10] |
2.8/11.1/13.9 |
NM |
7.7% |
92.7% (5 y) |
77.5% (5 y) |
97.7% |
90.2% |
88.2% |
73.2% |
|
Verma and Kumar, 2015[11] |
4.8/9.7/14.5 |
6.5% |
20% |
79.4% (5 y) |
53.1% (5 y) |
90.1% |
70.7% |
77% |
49.6% |
|
Jain et al, 2016[12] |
2.4/11.3/13.7 |
NM |
1.1% |
95.9% (5 y) |
79.1% (5 y) |
97.2%, |
93.9% |
94.3% |
63.7% |
|
Radhakrishnan et al, 2016[5] |
1.7/16/17.7 |
1.16% |
2.90% |
92.9% (5 y) |
83.1% (5 y) |
96% (stage I), 94.7% (stage II) |
91.7% (stage I), 86.6% (stage II) |
84% (stage III), 69.8% (stage IV) |
78.3% (stage III), 57.1% (stage IV) |
|
Bhethanabhotla et al, 2017[13] |
4.8/8/12.8 |
1% |
4.2% |
95.3% (5 y) |
84.4% (5 y) |
NM |
NM |
95.30% |
84.40% |
|
Seth et al, 2015[14] |
5.7/11.4/17.1 |
None |
0 |
100% (5 y) |
76.7% (5 y) |
NM |
NM |
NM |
NM |
|
Gupta et al, 2019[15] |
1.1/12.2/13.3 |
None |
5.50% |
88.80% |
84.50% |
90.0% |
90.0% |
89.0% |
83.8% |
|
Jayabose et al, 2016[16] |
3.8/0/3.8 |
None |
None |
NM |
100% |
NM |
NM |
NM |
NM |
|
Palayullakandi et al, 2022[17] |
0/6.3/6.3 |
5.3% |
9.1% |
93.5 ± 2.2% (4 y) |
86.2 ± 3.4% (4 y) |
100% (4 y; TG1) |
93.2 ± 4.6% (4 y; TG1) |
92.1 ± 4.5% (4 y; TG2) 88.1 ± 4.6% (4 y; TG3) |
84.7 ± 6.5% (4 y; TG2) 82 ± 6% (4 y; TG3) |
|
Parambil et al, 2020[18] |
1.5/2.6/4.1 |
3.9% |
NM |
NM |
NM |
100% (LR, 3 y) |
100% (LR, 3 y) |
94.4% (IR), 92.6% (HR) |
94.4% (IR), 90.3% (HR) |
|
Mahajan et al, 2021[19] |
1.5/2.2/3.7 |
0.75% |
0.75% |
NM |
NM |
97.7% (5 y) |
95.5% (5 y) |
NM |
NM |
|
Jain et al, 2021[20] |
4.2/10.7/14.9 |
1.14% |
3.43% |
NM |
NM |
NM |
NM |
90.8% (5 y) |
81.1% (5 y) |
Abbreviations: EFS, event-free survival; NM, not mentioned; OS, overall survival; TG, treatment groups as per Euronet-PHL-C1-protocol; TRM, treatment-related mortality.
Causes of treatment failure included progression/relapse, toxic deaths, and abandonment. The largest proportion of treatment failure was due to progression/relapse, which was around 15% in most studies, but has been close to 5% in the most recent studies.[17] [18] [19] Toxicity-related mortality (TRM) was generally 0 to 1%, except for two of the earliest studies (8.5 and 6.5% by Chandra et al[9] and Verma and Kumar,[11] respectively) and more recently around 5% in two studies, which used the more intensive OEPA/COPDAC chemotherapy backbone.[17] [18] Abandonment data has been provided in seven studies, which ranged from 0 to 8% in six studies with one study reporting exceptionally high abandonment rate of 20%.[11]
Discussion
The findings of this systematic review highlight the evolving landscape of pediatric HL management in India, reflecting both progress and persistent challenges characteristic of LMICs. While factors such as the simplicity of treatment protocols, favorable tumor biology, and lower toxicity from less myelosuppressive chemotherapy will contribute to better outcomes, issues like high rates of treatment abandonment, advanced disease at presentation, and resource limitations hinder outcomes. Analyzing the data of 13 included studies across the nation published over a period of last three decades and comparing these studies in two cohorts of recent era (group 1) and earlier era (group 2) as shown in [Table 3] highlights some noteworthy details. To facilitate comparison, the year 2010 was chosen as a convenient cutoff for commencement point of studies to categorize them into earlier and recent era phase.
Abbreviations: ABVD, Adriamycin [Doxorubicin], Bleomycin, Vinblastine, Dacarbazine; COPDAC, cyclophosphamide, vincristine, prednisolone, dacarbazine; COPP, Cyclophosphamide, Oncovin [Vincristine], Procarbazine, Prednisolone; CT, computed tomography; OEPA, ; PET, positron emission tomography.
The epidemiologic patterns seen across the included studies—particularly younger age at presentation, male predominance, and a higher frequency of mixed cellularity histology—are consistent with previously published LMIC data sets, including the Indian Council of Medical Research (ICMR) 2017 Pediatric Lymphoma Guidelines and recent global LMIC-focused reviews.[21] [22] [23] [24] These patterns contrast with high-income countries (HICs), where nodular sclerosis is more common and peak age is slightly older.[25] The contrasting biology in LMIC suggests that environmental, socioeconomic, and infection-related exposures may contribute.
Delayed diagnosis and high rates of advanced-stage presentation continue to be major concern in LMICs contributing to treatment complexity. Nearly 70 to 80% of Indian children were diagnosed at stage IIB to IV, markedly higher than in HIC cohorts.[25] System-level delays including referral lag, limited awareness at primary care level, and constrained access to pediatric oncology services remain important barriers.
The transition in chemotherapy protocols from predominantly ABVD-based regimens to risk- and response-adapted strategies such as OEPA/COPDAC in contemporary study cohorts mirrors global trends but requires judicious adaptation in our setting. While OEPA/COPDAC has been associated with lower relapse rates internationally, Indian centers reported higher TRM (up to 5%), likely reflecting limited supportive care capacity. Adoption of such intensive protocols should be in alignment of supportive care infrastructure. In the era of adapted treatment regimens,[26] this observation provides a guidance to achieve a balance between reducing progression/relapse rates and the need for strengthening supportive care to bring down TRM rates to reach the ultimate goal of improved survival rates.
Another interesting observation is PET-CT–based response assessment, which is currently the backbone of modern HL management internationally, remains inconsistently accessible across India. However, uniform use of PET-CT in recent studies is a notable advancement.[27] [28] Limited availability, cost, and uneven infrastructure remain barriers. Both ICMR[24] and recent LMIC reviews[25] recommend PET-CT where feasible, but also call for validated CT-based early response criteria for resource-limited settings.
RT practices, an integral treatment modality in HL, remain heterogeneous, with some centers using RT in < 10% and others in > 70% of cases as tabulated in [Table 1]. Variation arises from inconsistent access to RT facilities, differing oncologist preferences, lack of standardized national protocols, and differing levels of PET integration. Recent InPHOG trials aim to harmonize RT decision-making.[20]
Comparing the survival outcomes from past epidemiological data, there has been constant improvement in survival rates in LMICs in current time.[29] [30] However, the obstacles still persisting common to LMICs are treatment abandonment, socioeconomic disparity for treatment access, and compromised nutrition. Abandonment rates have improved over time (from 20% in older studies to < 10% in recent cohorts) ([Table 3]), reflecting expansion of government and nongovernmental supporting funds, public insurance schemes, increased awareness, and increasing participation of centers in prospective collaborative trial in India.
This systematic review summarizes the ongoing practices in pediatric HL in the country; however, this study is limited by the lack of access to individual patient data. There has been paucity of data on long-term outcomes as well as late effects.
Conclusion
Although high abandonment, advanced disease at presentation, and a significant TRM are roadblocks in the stride of optimal outcomes of pediatric HL, consistent and fairly good outcomes have paved the way to focus on reducing long-term effects also. Higher male predisposition in HL is a unique biological feature noted in all studies. Conventional approach of chemotherapy with ABVD backbone seems to yield reasonable outcomes with acceptable TRM. There is heterogeneity for RT use with variable indications and individualized approaches across various centers. As we transition toward approaches that further reduce long-term treatment-related toxicities including alternative intensive chemotherapy protocols, more focused radiation techniques, and attention to robust supportive care, the collaborative trials seem the way forward in near future. As of now, there is limited data on late effects but this is now being increasingly considered an important area to focus on. By far, we seem to be doing well in terms of favorable outcomes. The gap between treatment and overtreatment has the answer to avoid long-term side effects, which reinforces the strong need of working together, which can mitigate not only treatment-related factors but various social impacts also. Need to monitor late effects cannot be overemphasized.
Conflict of Interest
None declared.
Authors' Contributions
R.S.A. conceptualized the study, supervised the work, and critically reviewed the manuscript. K.T. collected the data, searched literature, and analyzed the data. Analysis of the articles was done by two independent reviewers (C.V. and R.S.A.). K.T. and C.V. integrated and interpreted the data and cowrote the manuscript. All authors discussed the results and approved the final draft.
Patient Consent
Patient consent is not required.
-
References
- 1 WHO Global Initiative for Childhood Cancer. An overview. World Health Organization; 2020. Accessed November 2022 at: https://www.who.int/docs/default-source/documents/health-topics/cancer/who-childhood-cancer-overview-booklet.pdf?sfvrsn=83cf45S52_1&download=true
- 2 Schellong G, Pötter R, Brämswig J. et al; The German-Austrian Pediatric Hodgkin's Disease Study Group. High cure rates and reduced long-term toxicity in pediatric Hodgkin's disease: the German-Austrian multicenter trial DAL-HD-90. J Clin Oncol 1999; 17 (12) 3736-3744
- 3 Mauz-Körholz C, Hasenclever D, Dörffel W. et al. Procarbazine-free OEPA-COPDAC chemotherapy in boys and standard OPPA-COPP in girls have comparable effectiveness in pediatric Hodgkin's lymphoma: the GPOH-HD-2002 study. J Clin Oncol 2010; 28 (23) 3680-3686
- 4 Dörffel W, Rühl U, Lüders H. et al. Treatment of children and adolescents with Hodgkin lymphoma without radiotherapy for patients in complete remission after chemotherapy: final results of the multinational trial GPOH-HD95. J Clin Oncol 2013; 31 (12) 1562-1568
- 5 Radhakrishnan V, Dhanushkodi M, Ganesan TS. et al. Pediatric Hodgkin lymphoma treated at cancer institute, Chennai, India: long-term outcome. J Glob Oncol 2016; 3 (05) 545-554
- 6 Arora RS, Mahajan A, Dinand V. et al. InPOG-HL-15–01 - challenges and lessons learnt in setting up the first collaborative multicentre prospective clinical trial in childhood cancer in India. Pediatric Hematology Oncology J 2020; 5 (04) 166-170
- 7 Arora RS, Bakhshi S. Indian Pediatric Oncology Group. (InPOG) – collaborative research in India comes of age. Pediatr Hematol Oncol J 2016; 1 (01) 13-17
- 8 Arora RS, Raj R, Mahajan A, Radhakrishnan N, Chinnaswamy G, Banavali S. Collaborative cancer research: progress report from the Indian Pediatric Oncology Group. Lancet Child Adolesc Health 2021; 5 (04) 239-240
- 9 Chandra J, Naithani R, Singh V, Saxena YK, Sharma M, Pemde H. Developing anticancer chemotherapy services in a developing country: Hodgkin lymphoma experience. Pediatr Blood Cancer 2008; 51 (04) 485-488
- 10 Trehan A, Singla S, Marwaha RK, Bansal D, Srinivasan R. Hodgkin lymphoma in children: experience in a tertiary care centre in India. J Pediatr Hematol Oncol 2013; 35 (03) 174-179
- 11 Verma N, Kumar A. Treating Hodgkin's lymphoma in a resource poor setting: challenges and outcome. Cancer and Onc Res. 2015; 3 (02) 11-16
- 12 Jain S, Kapoor G, Bajpai R. ABVD-based therapy for Hodgkin lymphoma in children and adolescents: lessons learnt in a tertiary care oncology center in a developing country. Pediatr Blood Cancer 2016; 63 (06) 1024-1030
- 13 Bhethanabhotla S, Jain S, Kapoor G. et al. Outcome of pediatric advanced Hodgkin lymphoma treated with ABVD and predictors of inferior survival: a multicenter study of 186 patients. Leuk Lymphoma 2017; 58 (07) 1617-1623
- 14 Seth R, Das RR, Puri K, Singh P. Clinical profile and chemotherapy response in children with Hodgkin lymphoma at a tertiary care centre. J Clin Diagn Res 2015; 9 (11) SC25-SC30
- 15 Gupta V, Singh TB, Gupta SK. Response and relapses in pediatric Hodgkin's lymphoma treated with chemotherapy alone. Indian J Med Paediatr Oncol 2019; 40: 341-346
- 16 Jayabose S, Viswanathan K, Kumar V. et al. ABVE-PC and modified BEACOPP regimen in Indian children with Hodgkin lymphoma: feasibility and efficacy. Indian J Med Paediatr Oncol 2016; 37 (02) 106-111
- 17 Palayullakandi A, Trehan A, Jain R. et al. Retrospective single-center experience with OEPA/COPDAC and PET-CT based strategy for pediatric Hodgkin lymphoma in a LMIC setting. Pediatr Hematol Oncol 2022; 39 (07) 587-599
- 18 Parambil BC, Narula G, Prasad M. et al. Clinical profile and outcome of classical Hodgkin lymphoma treated with a risk-adapted approach in a tertiary cancer center in India. Pediatr Blood Cancer 2020; 67 (02) e28058
- 19 Mahajan A, Singh M, Bakhshi S. et al. Treating early-stage Hodgkin lymphoma in resource-limited settings: InPOG-HL-15-01 experience. Pediatr Blood Cancer 2021; 68 (10) e29219
- 20 Jain S, Bakhshi S, Seth R. et al. Risk based and response adapted radiation therapy for children and adolescents with newly diagnosed advanced stage Hodgkin lymphoma treated with ABVD chemotherapy: a report from the Indian pediatric oncology group study InPOG-HL-15-01. Leuk Lymphoma 2022; 63 (05) 1111-1118
- 21 Lo AC, Dieckmann K, Pelz T. et al. Pediatric classical Hodgkin lymphoma. Pediatr Blood Cancer 2021; 68 (Suppl. 02) e28562
- 22 Bhopal SS, Mann KD, Pearce MS. Registration of cancer in girls remains lower than expected in countries with low/middle incomes and low female education rates. Br J Cancer 2012; 107 (01) 183-188
- 23 Mahajan A, Bakhshi S, Seth R. et al. Hodgkin lymphoma in children under 5 years: do they behave differently?. J Pediatr Hematol Oncol 2022; 44 (04) 186-190
- 24 Indian Council of Medical Research. Consensus Document for Management of Pediatric Lymphomas & Solid Tumors. New Delhi: ICMR; 2017. . Accessed October 11, 2025 at: https://www.icmr.gov.in/icmrobject/custom_data/pdf/resource-guidelines/PEDIATRIC_LYMPHOMAS_AND_SOLID_TUMORS_0.pdf
- 25 Moleti ML, Testi AM, Al-Hadad S, Al-Jadiry MF, Foà R. Pediatric Hodgkin lymphoma in low- and middle-income countries (LMICs). A narrative review. Mediterr J Hematol Infect Dis 2024; 16 (01) e2024078
- 26 Howard SC, Davidson A, Luna-Fineman S. et al. A framework to develop adapted treatment regimens to manage pediatric cancer in low- and middle-income countries: the Pediatric Oncology in Developing Countries (PODC) Committee of the International Pediatric Oncology Society (SIOP). Pediatr Blood Cancer 2017; 64 (Suppl. 05) 64
- 27 Mauz-Körholz C, Landman-Parker J, Balwierz W. et al. Response-adapted omission of radiotherapy and comparison of consolidation chemotherapy in children and adolescents with intermediate-stage and advanced-stage classical Hodgkin lymphoma (EuroNet-PHL-C1): a titration study with an open-label, embedded, multinational, non-inferiority, randomised controlled trial. Lancet Oncol 2022; 23 (01) 125-137
- 28 Kalra M, Bakhshi S, Singh M. et al. Response assessment by positron emission tomography-computed tomography as compared with contrast-enhanced computed tomography in childhood Hodgkin lymphoma can reduce the need for radiotherapy in low- and middle-income countries. Pediatr Blood Cancer 2023; 70 (02) e30091
- 29 Nandakumar A, Anantha N, Appaji L. et al. Descriptive epidemiology of childhood cancers in Bangalore, India. Cancer Causes Control 1996; 7 (04) 405-410
- 30 Swaminathan R, Rama R, Shanta V. Childhood cancers in Chennai, India, 1990-2001: incidence and survival. Int J Cancer 2008; 122 (11) 2607-2611
Address for correspondence
Publication History
Article published online:
20 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 WHO Global Initiative for Childhood Cancer. An overview. World Health Organization; 2020. Accessed November 2022 at: https://www.who.int/docs/default-source/documents/health-topics/cancer/who-childhood-cancer-overview-booklet.pdf?sfvrsn=83cf45S52_1&download=true
- 2 Schellong G, Pötter R, Brämswig J. et al; The German-Austrian Pediatric Hodgkin's Disease Study Group. High cure rates and reduced long-term toxicity in pediatric Hodgkin's disease: the German-Austrian multicenter trial DAL-HD-90. J Clin Oncol 1999; 17 (12) 3736-3744
- 3 Mauz-Körholz C, Hasenclever D, Dörffel W. et al. Procarbazine-free OEPA-COPDAC chemotherapy in boys and standard OPPA-COPP in girls have comparable effectiveness in pediatric Hodgkin's lymphoma: the GPOH-HD-2002 study. J Clin Oncol 2010; 28 (23) 3680-3686
- 4 Dörffel W, Rühl U, Lüders H. et al. Treatment of children and adolescents with Hodgkin lymphoma without radiotherapy for patients in complete remission after chemotherapy: final results of the multinational trial GPOH-HD95. J Clin Oncol 2013; 31 (12) 1562-1568
- 5 Radhakrishnan V, Dhanushkodi M, Ganesan TS. et al. Pediatric Hodgkin lymphoma treated at cancer institute, Chennai, India: long-term outcome. J Glob Oncol 2016; 3 (05) 545-554
- 6 Arora RS, Mahajan A, Dinand V. et al. InPOG-HL-15–01 - challenges and lessons learnt in setting up the first collaborative multicentre prospective clinical trial in childhood cancer in India. Pediatric Hematology Oncology J 2020; 5 (04) 166-170
- 7 Arora RS, Bakhshi S. Indian Pediatric Oncology Group. (InPOG) – collaborative research in India comes of age. Pediatr Hematol Oncol J 2016; 1 (01) 13-17
- 8 Arora RS, Raj R, Mahajan A, Radhakrishnan N, Chinnaswamy G, Banavali S. Collaborative cancer research: progress report from the Indian Pediatric Oncology Group. Lancet Child Adolesc Health 2021; 5 (04) 239-240
- 9 Chandra J, Naithani R, Singh V, Saxena YK, Sharma M, Pemde H. Developing anticancer chemotherapy services in a developing country: Hodgkin lymphoma experience. Pediatr Blood Cancer 2008; 51 (04) 485-488
- 10 Trehan A, Singla S, Marwaha RK, Bansal D, Srinivasan R. Hodgkin lymphoma in children: experience in a tertiary care centre in India. J Pediatr Hematol Oncol 2013; 35 (03) 174-179
- 11 Verma N, Kumar A. Treating Hodgkin's lymphoma in a resource poor setting: challenges and outcome. Cancer and Onc Res. 2015; 3 (02) 11-16
- 12 Jain S, Kapoor G, Bajpai R. ABVD-based therapy for Hodgkin lymphoma in children and adolescents: lessons learnt in a tertiary care oncology center in a developing country. Pediatr Blood Cancer 2016; 63 (06) 1024-1030
- 13 Bhethanabhotla S, Jain S, Kapoor G. et al. Outcome of pediatric advanced Hodgkin lymphoma treated with ABVD and predictors of inferior survival: a multicenter study of 186 patients. Leuk Lymphoma 2017; 58 (07) 1617-1623
- 14 Seth R, Das RR, Puri K, Singh P. Clinical profile and chemotherapy response in children with Hodgkin lymphoma at a tertiary care centre. J Clin Diagn Res 2015; 9 (11) SC25-SC30
- 15 Gupta V, Singh TB, Gupta SK. Response and relapses in pediatric Hodgkin's lymphoma treated with chemotherapy alone. Indian J Med Paediatr Oncol 2019; 40: 341-346
- 16 Jayabose S, Viswanathan K, Kumar V. et al. ABVE-PC and modified BEACOPP regimen in Indian children with Hodgkin lymphoma: feasibility and efficacy. Indian J Med Paediatr Oncol 2016; 37 (02) 106-111
- 17 Palayullakandi A, Trehan A, Jain R. et al. Retrospective single-center experience with OEPA/COPDAC and PET-CT based strategy for pediatric Hodgkin lymphoma in a LMIC setting. Pediatr Hematol Oncol 2022; 39 (07) 587-599
- 18 Parambil BC, Narula G, Prasad M. et al. Clinical profile and outcome of classical Hodgkin lymphoma treated with a risk-adapted approach in a tertiary cancer center in India. Pediatr Blood Cancer 2020; 67 (02) e28058
- 19 Mahajan A, Singh M, Bakhshi S. et al. Treating early-stage Hodgkin lymphoma in resource-limited settings: InPOG-HL-15-01 experience. Pediatr Blood Cancer 2021; 68 (10) e29219
- 20 Jain S, Bakhshi S, Seth R. et al. Risk based and response adapted radiation therapy for children and adolescents with newly diagnosed advanced stage Hodgkin lymphoma treated with ABVD chemotherapy: a report from the Indian pediatric oncology group study InPOG-HL-15-01. Leuk Lymphoma 2022; 63 (05) 1111-1118
- 21 Lo AC, Dieckmann K, Pelz T. et al. Pediatric classical Hodgkin lymphoma. Pediatr Blood Cancer 2021; 68 (Suppl. 02) e28562
- 22 Bhopal SS, Mann KD, Pearce MS. Registration of cancer in girls remains lower than expected in countries with low/middle incomes and low female education rates. Br J Cancer 2012; 107 (01) 183-188
- 23 Mahajan A, Bakhshi S, Seth R. et al. Hodgkin lymphoma in children under 5 years: do they behave differently?. J Pediatr Hematol Oncol 2022; 44 (04) 186-190
- 24 Indian Council of Medical Research. Consensus Document for Management of Pediatric Lymphomas & Solid Tumors. New Delhi: ICMR; 2017. . Accessed October 11, 2025 at: https://www.icmr.gov.in/icmrobject/custom_data/pdf/resource-guidelines/PEDIATRIC_LYMPHOMAS_AND_SOLID_TUMORS_0.pdf
- 25 Moleti ML, Testi AM, Al-Hadad S, Al-Jadiry MF, Foà R. Pediatric Hodgkin lymphoma in low- and middle-income countries (LMICs). A narrative review. Mediterr J Hematol Infect Dis 2024; 16 (01) e2024078
- 26 Howard SC, Davidson A, Luna-Fineman S. et al. A framework to develop adapted treatment regimens to manage pediatric cancer in low- and middle-income countries: the Pediatric Oncology in Developing Countries (PODC) Committee of the International Pediatric Oncology Society (SIOP). Pediatr Blood Cancer 2017; 64 (Suppl. 05) 64
- 27 Mauz-Körholz C, Landman-Parker J, Balwierz W. et al. Response-adapted omission of radiotherapy and comparison of consolidation chemotherapy in children and adolescents with intermediate-stage and advanced-stage classical Hodgkin lymphoma (EuroNet-PHL-C1): a titration study with an open-label, embedded, multinational, non-inferiority, randomised controlled trial. Lancet Oncol 2022; 23 (01) 125-137
- 28 Kalra M, Bakhshi S, Singh M. et al. Response assessment by positron emission tomography-computed tomography as compared with contrast-enhanced computed tomography in childhood Hodgkin lymphoma can reduce the need for radiotherapy in low- and middle-income countries. Pediatr Blood Cancer 2023; 70 (02) e30091
- 29 Nandakumar A, Anantha N, Appaji L. et al. Descriptive epidemiology of childhood cancers in Bangalore, India. Cancer Causes Control 1996; 7 (04) 405-410
- 30 Swaminathan R, Rama R, Shanta V. Childhood cancers in Chennai, India, 1990-2001: incidence and survival. Int J Cancer 2008; 122 (11) 2607-2611