

RSS-Feed abonnieren
DOI: 10.1055/s-0045-1815746
Adverse Glycemic Outcomes in Patients with Diabetic Neuropathy and Diabetic Foot Who Fast during Ramadan: Subanalysis of the Diabetes and Ramadan (DaR) Global Survey 2020–2022
Autor*innen
Funding and Sponsorship None.

Abstract
Background
Individuals with type 2 diabetes mellitus (T2DM) with diabetic peripheral neuropathy (DPN) or diabetic foot (DF) disease may be at increased risk of adverse glycemic events during Ramadan. This study evaluated fasting behavior and glycemic outcomes in participants with T2DM, categorized as without DPN/DF, with DPN, and with DPN + DF.
Methods
Data from 12,530 participants in the Diabetes and Ramadan Global Survey (2020–2022) were analyzed. Outcomes included the prevalence of those who fasted and episodes of hypo- and hyperglycemia.
Results
DPN and DPN + DF were present in 18.8 and 3.5% of participants, respectively. The rate of fasting declined with increasing complication burden (no DPN/DF 88.1%, DPN 78.2%, DPN + DF b%, p ≤ 0.0001). The odds of hyperglycemia, breaking the fast due to hyperglycemia, and severe hyperglycemia were higher in those with DPN (adjusted odds ratio [AOR]: 1.59, 2.14, and 3.17, respectively, all p < 0.0001), and DPN + DF (AOR: 1.63, 2.36, and 3.47, respectively, all p = < 0.05– < 0.0001) compared with T2DM without DPN/DF. Patients with DPN had the highest odds of daytime hypoglycemia (AOR: 1.71 vs. 1.54, p < 0.0001) and breaking fast due to hypoglycemia (AOR: 1.59 vs. 1.38, p < 0.0001) compared with T2DM without DPN/DF. The rate of severe hypoglycemia did not differ between groups (1.7 vs. 2.2 vs. 3.4%, p = 0.06). Participants with DPN monitored glucose more frequently when fasting but were less likely to receive Ramadan-focused education (both p ≤ 0.0001).
Conclusion
Although the majority of patients with T2DM fasted, those with DPN and DF were least likely to fast during Ramadan. However, among those who fasted, the presence of DPN and especially DPN + DF was associated with a higher risk of hyperglycemia and hypoglycemia. Pre-Ramadan assessment and targeted education are key in enabling safer fasting in patients with T2DM and DPN, especially those with DPN + DF.
Keywords
diabetic complications - diabetic foot disease - diabetic neuropathy - glycemic control - Ramadan fastingIntroduction
Ramadan fasting is observed by more than 1 billion Muslims globally.[1] During this period, fasting from dawn to sunset is obligatory for healthy adults but exempted for those with medical conditions such as diabetes. Despite these exemptions, most people with type 2 diabetes mellitus (T2DM) fast.[1] [2] This introduces unique metabolic and behavioral challenges, including changes in meal timing and composition, altered sleep and activity patterns, and modifications in medication schedules, which impact glucose variability and increase the risk of both hypoglycemia and hyperglycemia.[3] [4] [5]
Individuals with diabetic peripheral neuropathy (DPN) or diabetic foot (DF) disease may be especially vulnerable during Ramadan due to autonomic neuropathy and impaired response to hypoglycemia or reduced mobility with consequent hyperglycemia.[6] [7] Additionally, most patients with DPN/DF will be treated with a greater number and more complex medication regimens, which may make glucose management more difficult during fasting. Current risk stratification models for Ramadan fasting such as those developed by the International Diabetes Federation Diabetes and Ramadan (IDF-DaR) Alliance do not adjust for the presence of DPN or DF.[1] [2] Indeed, research on the impact of neuropathy and foot disease on fasting practices and glycemic outcomes is very limited.[6] [7] [8] [9]
Large-scale Ramadan studies such as EPIDIAR and CREED have provided valuable insights into fasting behaviors and risks among individuals with T2DM.[3] [4] Both demonstrated increased rates of hypoglycemia and hyperglycemia among fasting participants and identified persistent gaps in pre-Ramadan education.[3] [4] [5] However, neither stratified outcomes in relation to the presence of DPN nor DPN and DF. The Diabetes and Ramadan (DaR) Global Survey (2020–2022), a large multicountry initiative encompassing diverse Muslim populations, provides a unique opportunity to explore these gaps. In this analysis, we have evaluated fasting behavior and glycemic outcomes in individuals with DPN, DPN + DF to those without DPN or DF to enable evidence-based risk stratification and recommendations for individuals with DPN and DF who wish to fast during Ramadan.
Methods
Study Design and Setting
This study is a retrospective observational cohort analysis of data from the DaR Global Survey (2020–2022). The survey included Muslim individuals withT2DM from seven geographic regions: the Gulf, the Middle East, Türkiye, the United Kingdom, Africa, the Indian subcontinent, and Southeast Asia. Data were collected during routine outpatient clinic visits within 10 weeks of Ramadan finishing. This analysis specifically compares glycemic outcomes during Ramadan among patients with T2DM and DPN, DPN and DF, and patients with T2DM without DPN or DF.
Participants
All patients were regular attendees of outpatient clinics during the study period. As this was a retrospective analysis of preexisting data, no formal sample size calculation was performed.
Variables and Outcomes
Participants were categorized into three groups: those with DPN, both DPN and DF, and those without DPN or DF. The primary outcomes were whether patients fasted during Ramadan, the occurrence of daytime hypoglycemia, hyperglycemia, severe hypoglycemia or hyperglycemia requiring assistance or medical attention, and breaking the fast due to either hypoglycemia or hyperglycemia.
Secondary variables included age, sex, duration of diabetes, glycated hemoglobin (HbA1c), body mass index (BMI), systolic blood pressure, and lipid profile, including low-density lipoprotein (LDL) levels, presence of hypertension, diabetic retinopathy, microalbuminuria, nephropathy, and hyperlipidemia. The use of diabetes medications was documented, including insulin, metformin, sulfonylureas, GLP-1 receptor agonists, DPP-4 inhibitors, SGLT2 inhibitors, and thiazolidinediones. Data were collected on the frequency of self-monitoring of blood glucose (SMBG) during Ramadan and the receipt of Ramadan-focused diabetes education, either through routine clinic consultations or the distribution of educational leaflets.
Data Collection
Data were obtained via structured questionnaires administered by trained health care professionals during routine clinic visits. Information collected included demographic details, duration of diabetes, HbA1c levels, and current treatment regimens.
Statistical Analysis
Survey data from Ramadan 2020 and 2022 were combined for analysis. Descriptive statistics were used to summarize the clinical and demographic characteristics of participants across the three groups: DPN, DPN + DF, and no DPN/DF. Continuous variables were presented as means with standard deviations and compared using one-way analysis of variance. Categorical variables were expressed as frequencies and percentages and compared using the chi-square (χ2) test. When global tests were significant, pairwise comparisons were conducted with Bonferroni adjustment for multiple comparisons where applicable.
Multivariable logistic regression models were used to evaluate the association between complication group (DPN only, or both DPN and DF) and each Ramadan-related outcome: fasting status, daytime hypoglycemia, hyperglycemia, severe hypoglycemia, severe hyperglycemia, breaking the fast due to hypoglycemia, and breaking the fast due to hyperglycemia. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were calculated after adjusting for the presence of nephropathy, retinopathy, macrovascular complications and age, sex, duration of diabetes, HbA1c, hypertension, hyperlipidemia, and insulin use.
All analyses were conducted using IBM SPSS Statistics version 30, and a two-tailed p-value ≤ 0.05 was considered statistically significant.
Results
Patient Clinical Characteristics
Of the 12,530 participants with T2DM, 2,357 (18.8%) had DPN, and 442 (3.5%) had DPN + DF, while the remaining 9,731 (77.7%) had no DPN/DF ([Table 1]).
Abbreviations: DF, diabetic foot; DPN, diabetic peripheral neuropathy; T2DM, type 2 diabetes mellitus.
Notes: Values are presented as mean ± standard deviation or n (%). Group comparisons were performed using one-way analysis of variance for continuous variables and χ2 test for categorical variables. Significant differences between controls (no DPN or DF) and groups with either or both complications are denoted as ‡ p ≤ 0.05, † p ≤ 0.01, †† p ≤ 0.001, ††† p ≤ 0.0001. Superscript letters indicate post hoc pairwise comparisons. Values sharing the same superscript letter are not significantly different, whereas values with different superscript letters differ significantly (p < 0.05). The p-value reflects the comparison between DPN and both DPN and DF.
Compared with patients without DPN/DF, those with DPN and DPN + DF were significantly older (p ≤ 0.0001), had longer diabetes duration (p ≤ 0.0001), higher systolic blood pressure (p ≤ 0.0001), and higher LDL levels (p ≤ 0.0001), but comparable BMI (p > 0.05). Participants with DPN + DF had a longer duration of T2DM (14.1 ± 8.7 vs. 9.2 ± 7.1, and 11.9 ± 7.6 years, p ≤ 0.0001), higher HbA1c (9.1 ± 2.2 vs. 8.2 ± 1.9, and 8.9 ± 2.1, p ≤ 0.0001), and there was a higher proportion of males (57.5 vs. 48.4 and 42.6%, p ≤ 0.0001) compared with DPN and no DPN/DF groups.
Medications
Insulin use was higher in those with DPN + DF (72.9%) and DPN (59.4%) compared with those without DPN/DF (38.4%) (p ≤ 0.0001). A higher proportion of participants with DPN (1.7 and 6.5%), DPN + DF (2.0 and 6.8%) compared with those without DPN/DF (0.6 and 3.8%) (p ≤ 0.0001) were treated with a GLP-1 receptor agonist and thiazolidinedione. Participants with DPN had higher sulfonylurea and metformin use compared with those with DPN + DF (p ≤ 0.0001), and higher sulfonylurea but lower metformin use (p ≤ 0.0001) compared with those without DPN/DF. DPP-4 and SGLT2 inhibitor use did not differ between groups (p = 0.09 and 0.41, respectively) ([Table 2]).
Abbreviations: DF, diabetic foot; DPN, diabetic peripheral neuropathy.
Notes: Group comparisons were performed using the χ2 test. Data are shown as n (%). Superscript letters indicate post hoc pairwise comparisons. Values sharing the same superscript letter are not significantly different, whereas values with different superscript letters differ significantly (p < 0.05). The p-values indicate overall group differences.
Complications
There was a stepwise increase in the prevalence of retinopathy, nephropathy, and macrovascular complications in those without DPN/DF, DPN, and DPN + DF (p ≤ 0.0001). Patients with DPN and DPN + DF had a higher prevalence of hypertension, hyperlipidemia, and microalbuminuria compared with those without DPN/DF (p ≤ 0.0001) ([Table 2]).
Self-Monitoring of Blood Glucose and Ramadan Focused Education
Patients with DPN more frequently performed SMBG during Ramadan compared with patients without DPN/DF (p ≤ 0.0001). Patients with DPN and DPN + DF received less education during routine clinic consultations and educational leaflets compared with patients without DPN/DF (p ≤ 0.0001) ([Table 3]).
Abbreviations: DF, diabetic foot; DPN, diabetic peripheral neuropathy; SMBG, self-monitoring of blood glucose.
Notes: Values are presented as n (%). Group comparisons were performed using the χ2 test. Superscript letters indicate post hoc pairwise comparisons. Values sharing the same superscript letter are not significantly different, whereas values with different superscript letters differ significantly (p < 0.05). The p-values indicate overall group differences.
Fasting Rates and Glycemic Outcomes during Ramadan
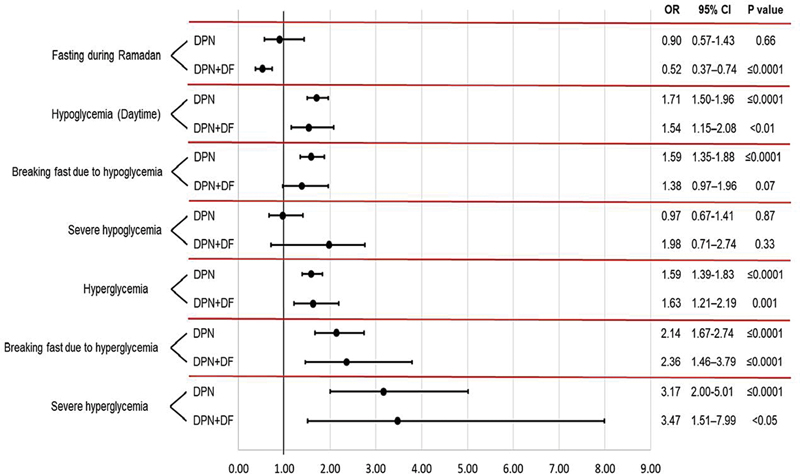
Fasting during Ramadan was less frequent in those with DPN + DF and DPN compared with those without DPN/DF (b vs. 78.2 vs 88.1%, all p ≤ 0.0001). The prevalence of daytime hypoglycemia, hyperglycemia, breaking the fast due to hypoglycemia or hyperglycemia, and severe hyperglycemia was significantly higher in patients with DPN and DPN + DF compared with patients without DPN/DF (p ≤ 0.0001), while the frequency of severe hypoglycemia was comparable between groups (p = 0.06) ([Table 4] and [Fig. 1]).
Abbreviations: DF, diabetic foot; DPN, diabetic peripheral neuropathy.
Notes: Group comparisons were performed using the χ2 test. Superscript letters indicate post hoc pairwise comparisons. Values sharing the same superscript letter are not significantly different, whereas values with different superscript letters differ significantly (p < 0.05). The p-values indicate overall group differences.
After adjustment for nephropathy, retinopathy, macrovascular complications, age, sex, duration of diabetes, HbA1c, hypertension, hyperlipidemia, and insulin therapy, the odds of fasting during Ramadan were lower in participants with DPN + DF (AOR: 0.52, 95% CI: 0.37–0.74, p ≤ 0.0001), but not in those with DPN (p = 0.66). The odds of hypoglycemia were higher in those with DPN + DF (AOR: 1.54, 95% CI: 1.15–2.08, p < 0.01) and DPN (AOR: 1.71, 95% CI: 1.50–1.95, p ≤ 0.0001) compared with those without DPN/DF. The odds of breaking the fast due to hypoglycemia were higher in those with DPN (AOR: 1.59, 95% CI: 1.35–1.88, p < 0.0001), but not DPN + DF (p = 0.07) compared with those without DPN/DF. The odds of hyperglycemia (AOR: 1.59, 95% CI: 1.39–1.83, p < 0.0001), breaking the fast due to hyperglycemia (AOR: 2.14, 95% CI: 1.67–2.74, p < 0.0001), and severe hyperglycemia (AOR: 3.17, 95% CI: 2.00–5.01, p < 0.0001) were higher in those with DPN and were further increased in those with DPN + DF (AORs 1.63, 2.36, and 3.47, respectively, p = < 0.05– < 0.0001).
Discussion
This study shows that individuals with DPN and DF were less likely to fast during Ramadan compared with those without DPN or DF. The odds of hyperglycemia, breaking the fast due to hyperglycemia, and severe hyperglycemia were higher in those with DPN, and even higher in those with DPN and DF. However, individuals with DPN had the highest risk of daytime hypoglycemia and breaking the fast due to hypoglycemia. Severe hypoglycemia rates were similar across groups. Patients with DPN and DF had a higher prevalence of hypertension, hyperlipidemia, retinopathy, microalbuminuria, nephropathy, and macrovascular complications. Patients with DPN and DF performed SMBG more frequently during Ramadan, but were less likely to receive Ramadan-focused education, underscoring a gap between awareness and structured support. These findings highlight the need for targeted risk assessment and tailored education for individuals with DPN and DF to enable safer fasting during Ramadan.
Large-scale Ramadan studies, such as EPIDIAR[3] and the multicountry CREED cohorts,[4] [10] have reported high levels of fasting in individuals with T2DM during Ramadan, despite the presence of complications. EPIDIAR reported a fivefold increase in severe hyperglycemia,[3] and in CREED, those with complications were more likely to experience hypoglycemia.[10] In both studies, fewer than half the participants received Ramadan-focused education. However, neither study stratified outcomes in relation to the presence of DPN or both DPN and DF. Our study shows that patients with DPN and DF have the lowest fasting rate, the highest risk of hyperglycemia-related events, despite more frequent insulin use, and a lower likelihood of receiving Ramadan-focused education.
Our findings provide important empirical support for the IDF-DAR Practical Guidelines, which had relied on consensus to classify patients with DPN and history of DF ulcer or active foot disease as high or very high risk for fasting, with recommendations for individualized counseling, careful medication adjustment, and frequent glucose monitoring before and during Ramadan.[1] [11] Notably, despite this guidance, patients with DPN and DF were less likely to receive Ramadan-focused education, particularly through leaflets, compared with those without DPN or DF, suggesting that they were simply advised not to fast. Nevertheless, these patients fasted, and despite more frequent SMBG during Ramadan, their rates of hyperglycemia and fasting interruption were higher, suggesting that monitoring alone, without effective education, is not sufficient. This is consistent with a study showing that frequent glucose monitoring is associated with fewer acute glycemic events, but only when combined with education and management plans.[12] Tourkmani et al showed that a pre-Ramadan education program including individualized risk assessment, dietary advice, medication adjustment, and training in self-monitoring significantly reduced the incidence of hypoglycemia, improved glycemic stability, and enhanced safety during fasting, even in those with diabetes complications.[13] The educational gap identified in our cohort should be prioritized to improve outcomes in high-risk groups.
The higher prevalence of vascular risk factors, including hypertension and dyslipidemia, together with retinopathy, nephropathy, and greater insulin use in patients with DPN and DF likely contributes to their increased risk of adverse glycemic events during Ramadan. Jabbar et al showed that insulin therapy and the presence of chronic complications were independently associated with a higher likelihood of hypoglycemia and hyperglycemia during fasting.[4] In a cohort of patients with T2DM from Qatar, Kingdom of Saudi Arabia, and Kuwait, we previously reported that individuals with DPN and DF had poorer glycemic control and higher insulin use, which may increase their risk of acute glycemic events during Ramadan.[14] Collectively, these findings reinforce the importance of targeted risk assessment with structured Ramadan-focused education, individualized medication adjustment, and increased SMBG in patients with DPN and DF who choose to fast during Ramadan.
We acknowledge that this study relied on self-reported data for complications and glycemic events, which may have resulted in recall bias and misclassification. Furthermore, the severity of adverse glycemic events was assessed indirectly through questions on event frequency, fasting interruption, and need for medical assistance. Nevertheless, this study is large with a geographically diverse sample, addressing Ramadan-specific outcomes, including both severe and nonsevere glycemic events, with adjustment for key confounders such as insulin and sulfonylurea use. By stratifying participants into those with DPN and DPN + DF, this study enabled assessment of the cumulative impact of these complications on fasting practices and glycemic risk.
Conclusion
In conclusion, individuals with DPN and DF were less likely to fast during Ramadan, but in those who fasted, the occurrence of adverse glycemic events was increased. This highlights the importance of structured risk assessment and Ramadan-focused education with individualized therapy to enhance the safety of fasting in patients with DPN and DF.
Conflict of Interest
None declared.
Authors' Contribution
All authors contributed to the conception, data collection/analysis, drafting of the manuscript, and approved its final version.
Compliance with Ethical Principles
The original DAR Surveys were approved by the Dubai Health Authority, and all patients provided informed consent for anonymous participation.
* These authors are the joint first authors.
-
References
- 1 Hassanein M, Afandi B, Yakoob Ahmedani M. et al. Diabetes and Ramadan: practical guidelines 2021. Diabetes Res Clin Pract 2022; 185: 109185
- 2 Al Arouj M. et al. Risk-stratification of individuals with diabetes before Ramadan. In: IDF-DAR Diabetes and Ramadan Practical Guidelines 2021. Brussels: International Diabetes Federation; 2021
- 3 Salti I, Bénard E, Detournay B. et al; EPIDIAR study group. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care 2004; 27 (10) 2306-2311
- 4 Babineaux SM, Toaima D, Boye KS. et al. Multi-country retrospective observational study of the management and outcomes of patients with type 2 diabetes during Ramadan in 2010 (CREED). Diabet Med 2015; 32 (06) 819-828
- 5 Hassanein M, Binte Zainudin S, Shaikh S. et al. An update on the current characteristics and status of care for Muslims with type 2 diabetes fasting during Ramadan: the DAR global survey 2022. Curr Med Res Opin 2024; 40 (09) 1515-1523
- 6 Hicks CW, Selvin E. Epidemiology of peripheral neuropathy and lower extremity disease in diabetes. Curr Diab Rep 2019; 19 (10) 86
- 7 Savelieff MG, Elafros MA, Viswanathan V, Jensen TS, Bennett DL, Feldman EL. The global and regional burden of diabetic peripheral neuropathy. Nat Rev Neurol 2025; 21 (01) 17-31
- 8 Tavakoli M, Klingelhöfer D, Fadavi H, Groneberg DA. The landscape of global research on diabetic neuropathy. Front Endocrinol (Lausanne) 2023; 14: 1220896
- 9 Ismail CAN. Issues and challenges in diabetic neuropathy management: a narrative review. World J Diabetes 2023; 14 (06) 741-757
- 10 Jabbar A, Hassanein M, Beshyah SA, Boye KS, Yu M, Babineaux SM. CREED study: hypoglycaemia during Ramadan in individuals with type 2 diabetes mellitus from three continents. Diabetes Res Clin Pract 2017; 132: 19-26
- 11 Shaltout I, Abdelwahab AM, El Meligi A. et al. Risk stratification in people with diabetes for fasting during Ramadan: consensus from Arabic Association for the Study of Diabetes and Metabolism. Curr Diabetes Rev 2024; 20 (07) e201023222409
- 12 Al Hayek AA, Robert AA, Al Dawish MA, Zamzami MM, Sam AE, Alzaid AA. Impact of an education program on patient anxiety, depression, glycemic control, and adherence to self-care and medication in type 2 diabetes. J Family Community Med 2013; 20 (02) 77-82
- 13 Tourkmani AM, Hassali MA, Alharbi TJ. et al. Impact of Ramadan focused education program on hypoglycemic risk and metabolic control for patients with type 2 diabetes. Patient Prefer Adherence 2016; 10: 1709-1717
- 14 Ponirakis G, Elhadd T, Al Ozairi E. et al. Prevalence and risk factors for diabetic peripheral neuropathy, neuropathic pain and foot ulceration in the Arabian Gulf region. J Diabetes Investig 2022; 13 (09) 1551-1559
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
22. Januar 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Hassanein M, Afandi B, Yakoob Ahmedani M. et al. Diabetes and Ramadan: practical guidelines 2021. Diabetes Res Clin Pract 2022; 185: 109185
- 2 Al Arouj M. et al. Risk-stratification of individuals with diabetes before Ramadan. In: IDF-DAR Diabetes and Ramadan Practical Guidelines 2021. Brussels: International Diabetes Federation; 2021
- 3 Salti I, Bénard E, Detournay B. et al; EPIDIAR study group. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care 2004; 27 (10) 2306-2311
- 4 Babineaux SM, Toaima D, Boye KS. et al. Multi-country retrospective observational study of the management and outcomes of patients with type 2 diabetes during Ramadan in 2010 (CREED). Diabet Med 2015; 32 (06) 819-828
- 5 Hassanein M, Binte Zainudin S, Shaikh S. et al. An update on the current characteristics and status of care for Muslims with type 2 diabetes fasting during Ramadan: the DAR global survey 2022. Curr Med Res Opin 2024; 40 (09) 1515-1523
- 6 Hicks CW, Selvin E. Epidemiology of peripheral neuropathy and lower extremity disease in diabetes. Curr Diab Rep 2019; 19 (10) 86
- 7 Savelieff MG, Elafros MA, Viswanathan V, Jensen TS, Bennett DL, Feldman EL. The global and regional burden of diabetic peripheral neuropathy. Nat Rev Neurol 2025; 21 (01) 17-31
- 8 Tavakoli M, Klingelhöfer D, Fadavi H, Groneberg DA. The landscape of global research on diabetic neuropathy. Front Endocrinol (Lausanne) 2023; 14: 1220896
- 9 Ismail CAN. Issues and challenges in diabetic neuropathy management: a narrative review. World J Diabetes 2023; 14 (06) 741-757
- 10 Jabbar A, Hassanein M, Beshyah SA, Boye KS, Yu M, Babineaux SM. CREED study: hypoglycaemia during Ramadan in individuals with type 2 diabetes mellitus from three continents. Diabetes Res Clin Pract 2017; 132: 19-26
- 11 Shaltout I, Abdelwahab AM, El Meligi A. et al. Risk stratification in people with diabetes for fasting during Ramadan: consensus from Arabic Association for the Study of Diabetes and Metabolism. Curr Diabetes Rev 2024; 20 (07) e201023222409
- 12 Al Hayek AA, Robert AA, Al Dawish MA, Zamzami MM, Sam AE, Alzaid AA. Impact of an education program on patient anxiety, depression, glycemic control, and adherence to self-care and medication in type 2 diabetes. J Family Community Med 2013; 20 (02) 77-82
- 13 Tourkmani AM, Hassali MA, Alharbi TJ. et al. Impact of Ramadan focused education program on hypoglycemic risk and metabolic control for patients with type 2 diabetes. Patient Prefer Adherence 2016; 10: 1709-1717
- 14 Ponirakis G, Elhadd T, Al Ozairi E. et al. Prevalence and risk factors for diabetic peripheral neuropathy, neuropathic pain and foot ulceration in the Arabian Gulf region. J Diabetes Investig 2022; 13 (09) 1551-1559