

Subscribe to RSS
DOI: 10.1055/s-0046-1815924
Endoscopic Full-Thickness Resection of Gastric Subepithelial Lesion from Peritoneal Side
Authors

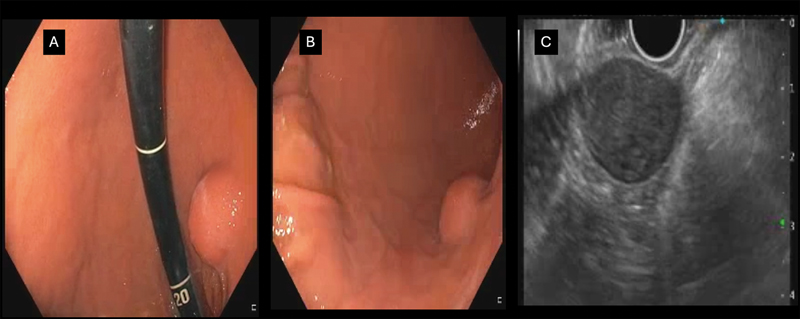
A 52-year-old woman with a history of tongue carcinoma was detected to have a 3-cm submucosal lesion in mid-gastric body. Endoscopic ultrasound examination revealed a 3.5-cm lesion arising from the fourth layer of the gastric wall, and fine-needle biopsy was suggestive of a mesenchymal tumor ([Fig. 1]). After discussion with the patient, the decision to perform excavating endoscopic submucosal dissection or endoscopic full-thickness resection (EFTR) was taken, as guided by the depth of the tumor.
After marking at a 5-mm distance from margins, submucosal dissection (forced coagulation mode, Effect 3.5, 55 W) of the lesion was done initially on the proximal side, followed by the distal and lateral sides. Loop-and-clip–assisted traction was applied to the proximal side of the mucosal flap. Intramuscular dissection revealed tumor extension up to the serosal wall. Full-thickness incision on the muscle and serosal layer was given on the oral side of the lesion, and the peritoneal cavity could be visualized. No pneumoperitoneum was created, but previously applied traction aided in adequate exposure of the serosal side by partly drawing the lesion into the gastric cavity and better visualization of large vessels on the serosal side, avoiding inadvertent injury. Further dissection was performed from the serosal side with pre-emptive vessel coagulation ([Fig. 2]). After en bloc resection, the full-thickness defect closure was done by the loop-and-clip method ([Video 1]). Noncontrast computed tomography of the abdomen on the next day revealed no peritoneal collection with clips in situ. Patient was kept nil by mouth for the next 48 hours, followed by nasojejunal feed at 48 hours. Oral diet was resumed on day 7. Follow-up endoscopy after 3 months revealed complete healing at the resection site with no residual tumor ([Fig. 3]). Histopathology with immunohistochemistry revealed schwannoma with tumor-free horizontal margins ([Fig. 4]).



Practical Implications for Endoscopists
-
Proper evaluation of gastric subepithelial lesion (SEL) is essential.[1] Lesions with a deeper layer of origin may require full-thickness resection or conversion to surgery if expertise is not available.[2]
-
EFTR can be performed for gastric lesions arising from the deeper part of the muscularis propria and with extramural extension.[3]
-
Exposed and nonexposed EFTR are options for gastric SEL removal. Lesion size, location, and depth may guide the choice of technique.[4]
-
During EFTR, exposure of the serosal side with properly applied traction can avoid inadvertent injury to large vessels.
-
Internal traction using widely available clips and a loop is a feasible option.
-
Gastric defects after EFTR can be closed with the loop-and-clip technique[5] or endoscopic suturing with the OverStitch device.
Conflict of Interest
None declared.
-
References
- 1 Vasilakis T, Ziogas D, Tziatzios G. et al. EUS-guided diagnosis of gastric subepithelial lesions, what is new?. Diagnostics (Basel) 2023; 13 (13) 2176
- 2 Zhao SQ, Wang SY, Ge N. et al. Endoscopic full-thickness resection vs surgical resection for gastric stromal tumors: efficacy and safety using propensity score matching. World J Gastrointest Surg 2025; 17 (03) 101002
- 3 Deprez PH, Moons LMG, OʼToole D. et al. Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2022; 54 (04) 412-429
- 4 Chiu PWY, Yip HC, Chan SM, Ng SKK, Teoh AYB, Ng EKW. Endoscopic full-thickness resection (EFTR) compared to submucosal tunnel endoscopic resection (STER) for treatment of gastric gastrointestinal stromal tumors. Endosc Int Open 2023; 11 (02) E179-E186
- 5 Fukuda H, Uedo N, Shichijo S. Traction-assisted endoscopic full-thickness resection for extraluminal type gastrointestinal stromal tumor. Endosc Int Open 2021; 9 (08) E1243-E1245
Address for correspondence
Publication History
Article published online:
27 January 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Vasilakis T, Ziogas D, Tziatzios G. et al. EUS-guided diagnosis of gastric subepithelial lesions, what is new?. Diagnostics (Basel) 2023; 13 (13) 2176
- 2 Zhao SQ, Wang SY, Ge N. et al. Endoscopic full-thickness resection vs surgical resection for gastric stromal tumors: efficacy and safety using propensity score matching. World J Gastrointest Surg 2025; 17 (03) 101002
- 3 Deprez PH, Moons LMG, OʼToole D. et al. Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2022; 54 (04) 412-429
- 4 Chiu PWY, Yip HC, Chan SM, Ng SKK, Teoh AYB, Ng EKW. Endoscopic full-thickness resection (EFTR) compared to submucosal tunnel endoscopic resection (STER) for treatment of gastric gastrointestinal stromal tumors. Endosc Int Open 2023; 11 (02) E179-E186
- 5 Fukuda H, Uedo N, Shichijo S. Traction-assisted endoscopic full-thickness resection for extraluminal type gastrointestinal stromal tumor. Endosc Int Open 2021; 9 (08) E1243-E1245