

Subscribe to RSS
DOI: 10.4103/LIUJ.LIUJ_17_19
Evolving a national preventive protocol for vertical transmission of group B streptococcus in a low-resource country: The culture-based approach
Authors

Abstract
Objective: The study objective was to determine the role and applicability of the culture-based approach to Group B Streptococcus(GBS) screening and the effect on pregnancy outcome. Materials and Methods: This is a prospective cross-sectional study involving 166 consenting antenatal clinic attendees at 35–37 weeks' gestation using purposive sampling. All participants had vaginal and rectal swabs collected and cultured with the availability of culture results at the time of presentation in labor. All GBS-colonized mothers received intrapartum prophylaxis with parenteral antibiotics based on antibiotic sensitivity from the onset of labor or the rupture of membrane until delivery. Statistical analysis was conducted using SPSS software version 21.0, while P < 0.05 was considered statistically significant. Results: The GBS maternal prevalence was 7.8%, and culture-positive women had both vaginal and rectal colonization. Marital status (P = 0.002), multiple sexual partners (P =0.001), previous sexually transmitted infections (P = 0.013), and low socioeconomic status (P = 0.012) were significantly associated with GBS colonization. GBS isolates were 100% sensitive to ampicillin, all participants had a minimum of two doses of intrapartum prophylaxis with parenteral ampicillin, there was no maternal morbidity, and the vertical transmission of GBS was 0%. Conclusions: The culture-based approach and the culture-based maternal intrapartum prophylaxis prevented both maternal and neonatal complications from GBS. Establishing regional- and national-level preventive protocols will be a central strategy for the prevention.
Key-words:
Group B Streptococcus - maternal sepsis - national protocol - neonatal sepsis - screening protocol - vertical transmission of infectionsIntroduction
Group B Streptococcus(GBS) is a vertical transmissible infection and a cause of puerperal infection and neonatal sepsis.[[1]] Its prevalence in humans varies depending on the geographical location, race, socioeconomic status, and a history of previously affected infants and previous preterm delivery.[[2]] GBS infection was initially thought to be a disease of developed countries; however, studies showed a similar prevalence in low-resource countries.[[3]] Reports across the African continent have also revealed that GBS is emerging as an important cause of neonatal sepsis, especially in low-income countries.[[4]],[[5]]
Globally, GBS carriage among parturient ranges between 10.0% and 40.0%.[[1]],[[3]],[[6]] In Nigeria, it ranges from 6.6% to 32.0%.[[7]],[[8]],[[9]],[[10]] GBS is associated with significant maternal peripartum disease including bacteremia, endocarditis, chorioamnionitis, and endometritis.[[2]] Asymptomatic GBS infection is equally deleterious with associated adverse pregnancy outcomes including low birth weight, preterm delivery, and premature rupture of membrane (PROM).[[5]] In addition, neonatal GBS disease affects 0.1–0.5/1000 live births, resulting in up to 50.0% neonatal mortality and significant long-term morbidity.[[11]]
There are two main approaches, namely the culture- and risk-based approaches, to screening for GBS infection in pregnancy. The culture-based approach is based on the universal antenatal maternal screening at 35–37 weeks' gestation using culture of low vaginal and/or rectal swab. This is the gold standard and standard of care in developed countries, especially in the USA.[[5]],[[11]] The risk-based approach is based on clinical risk factor evaluation in parturient; thus, it is limited only to symptomatic women although it is cost-effective and time saving and targets women without prior contact with health personnel.[[5]] Therefore, it is preferred in some countries, especially in low-resource settings. Neonatal GBS infection can be prevented by the administration of prophylactic intravenous antibiotics based on the sensitivity pattern of the GBS strain isolated from the colonized pregnant woman.[[12]] Although oral administration may cause a transient decrease in the GBS load, bacterial eradication is not achieved except in GBS urinary tract infection; thus, it is not recommended.[[12]]
Despite the documented maternal morbidity and neonatal morbidity and mortality from GBS disease, many institutions in low-resource countries lack a standardized protocol to prevent its vertical transmission.[[13]] This study, therefore, aimed to add to the available evidence to stimulate the formation of institutional protocols for GBS management in low-resource countries.
Materials and Methods
This was a cross-sectional study involving 166 antenatal clinic attendees at a tertiary hospital in North-Central Nigeria. The sample size was calculated; purposive sampling was employed while the inclusion criteria were booked status, gestational age of 35–37 weeks, and willingness to participate. Unbooked women, those outside the specified gestational age, and those unwilling to participate were excluded from the study. After obtaining consent, all participants had low vaginal and rectal swabs collected and analyzed with the availability of culture result at the time of presentation in labor. The samples were collected using separate swab sticks for the vagina and rectum; the swab sticks were transferred in Todd Hewitt medium to the laboratory for analysis using an earlier described guideline.[[14]] The samples were inoculated onto blood and chocolate agars and incubated for 18–24 h at 35°C–37°C in ambient air (blood agar) and carbon dioxide-enriched atmosphere (a candle extinction jar). The culture plates were inspected to identify organisms suggestive of GBS (i.e., narrow zone of β-hemolysin). The isolates were further characterized using a combination of Gram stain and biochemical tests, i.e., catalase test; bacitracin susceptibility test; and Christie–Atkins–Munch–Peterson tests, to distinguish between Staphylococcus and Streptococcus. Antibiotic sensitivity was done by disc diffusion method. All GBS isolates were first inoculated into sterile normal saline, and the suspension was adjusted to 0.5% McFarland standard. The suspension was used to inoculate Mueller–Hinton agar into which single antibiotic discs were applied and incubated at 37°C aerobically for 18–24 h inside the candle extension jar. Staphylococcus aureus(ATCC® 25923) strain was used as the control, and the results were read and interpreted by comparing inhibition zone diameter of test with the control according to laboratory (Clinical and Laboratory Standards Institute) guidelines.
Participants thereafter had routine antenatal follow-ups and were required to present early in labor. All GBS-positive parturient had prophylaxis with intravenous ampicillin 2 g stat, and then 1 g 4 hourly till delivery starting from the time of presentation in labor. Puerperal follow-up was with telephone calls and counseling to re-present if there were fever, foul-smelling lochia, or abnormal vaginal discharge. All neonates were monitored for the first 48 h for the symptoms and signs of early-onset neonatal sepsis which included grunting, poor feeding, lethargy, fever(temperature ≥38°C), tachycardia (heart rate >160/min), or tachypnea (respiratory rate >60 cycles/minute). Neonates without the clinical features of GBS were discharged home at 48 h after educating the mother on the signs of neonatal GBS disease such as grunting, poor feeding, fever, irritability, lethargy (limpness), and immediate presentation, if such was noticed. In addition, the mothers were phoned daily during the 1st week of life to find out the clinical conditions of the neonates. Babies with feature of neonatal infection were admitted at the neonatal intensive care unit and managed appropriately including a GBS culture to ascertain the source of infection. While awaiting the results of investigations, empirical treatment using parenteral penicillin and intramuscular gentamycin was commenced for the babies.
Ethical approval was obtained from the ethical review committee of the tertiary institution before the commencement of the study. Statistical analysis was conducted using SPSS software version 21.0 (IBM, Armonk, NY, USA), and P < 0.05 was considered statistically significant.
Results
The age range of the 166 participants was 18–39 years (mean ± standard deviation = 30.3 ± 4.9). Thirteen participants were culture positive for GBS, with a prevalence of 7.8% (78.0/1000). All colonized women had both vaginal and rectal colonization. The maternal biosocial factors that significantly related to GBS carriage included marital status (P = 0.002), multiple sexual partners (P = 0.001), previous sexually transmitted infection (P = 0.013), and low socioeconomic status (P = 0.012) [[Table 1]].

[[Table 2]] shows that the only statistically significant risk factor for GBS carriage was preterm PROM(P = 0.001). In addition, GBS carriage was statistically significantly (P = 0.001) related to gestational age at delivery as more than half of the GBS carriers (53.8%) had preterm delivery, whereas two (15.4%) had babies with low birth weight. At the end of 24 h, nine (69.2%) neonates were healthy, whereas four (30.8%) had perinatal asphyxia; on the 7th day of life, all neonates of GBS carrier mothers were healthy with no neonatal sepsis recorded. All GBS carrier mothers received intrapartum intravenous ampicillin; 15.4% received two doses while 53.8% received five doses; there was no maternal puerperal complication.

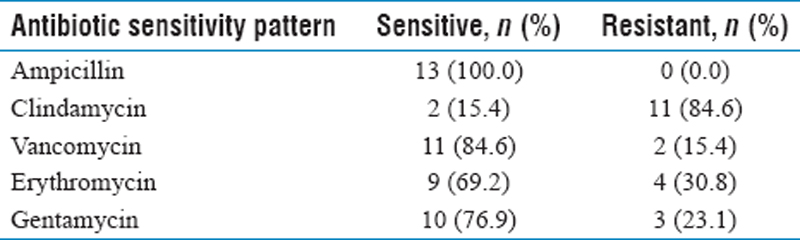
[[Table 3]] shows that all the 13(100%) GBS carriers isolated were sensitive to ampicillin, 11 (84.6%) to vancomycin, 9 (69.2%) to erythromycin, and 10(76.9%) to gentamycin. On logistic regression [[Table 4]], the significant predictor of GBS carriage was found to be multiple sexual partners, which was an independent predictor of GBS carriage (P = 0.024) with an odd that is eight times higher than that of a parturient with a single sexual partner.

Discussion
The incidence of GBS among pregnant women in this study was 7.8%, which is comparable to 6.6%–11.3% in parts of Nigeria,[[7]],[[8]],[[9]] 4.0% in Togo,[[15]] and 9.5% in Korea.[[16]] Other studies from different regions of Africa reported a prevalence of 16.5%–19.0%,[[15]],[[17]],[[18]] while an international study[[1]] reported the prevalence to be 29.0% for Africans, 13.0% for Asians, and 21.0% for Europeans. The wide variation in the reported prevalence may be attributed to differences in the geographical location and other demographic variables such as maternal age, gestational age, obstetric history, study population, as well as the culture and the isolation techniques. Studies have also shown that racial and genetic factors are known contributing factors to variations in GBS carriage.[[1]]
Although a majority of participants in this study were aged 26–35 years, the highest GBS colonization was among single mothers aged 18–30 years. The young women were more sexually active; this corroborates a previously reported association of GBS with sexually active young women having multiple sexual partners and poor socioeconomic status.[[18]] The observed association of GBS colonization with primiparity appears similar to other reports from Nigeria,[[17]] which may be linked to the expected higher sexual activity among them. The effect of GBS colonization in preterm delivery was documented in this study to corroborate earlier reports.[[4]],[[18]] In this study, there was culture-based screening, adequate intrapartum parenteral prophylaxis, and no vertical transmission of GBS infection. In a study on risk-based approach to GBS management among women with risk factors for GBS conducted in the same city as the index study, 20.8% of the participants had risk factors for vertical transmission of GBS and despite parenteral intrapartum prophylaxis, the incidence of early-onset neonatal GBS disease among women with risk factors was 12.9/1000.[[4]] This finding contrasts with the index study which reported no vertical transmission, thereby suggesting better outcome with the culture-based approach. Another challenge with the risk-based approach is the cases of inadequate prophylaxis due to late presentation. In Ilorin, Nigeria, a risk-based evaluation for GBS transmission reported that neonatal GBS disease occurred in babies of mothers who had inadequate antibiotics (less than two doses) due to late presentation in labor.[[4]] This remains a major challenge on the effectiveness of the risk-based approach as some parturient are unable to attain adequate prophylaxis unlike the culture-based approach. However, proponents of the risk-based approach have emphasized their particular benefit for unbooked patients, which is common in low-resource settings and also because it is less expensive.[[5]] In addition, this study reported no maternal complication unlike 17.5% in another study using the risk-based approach.[[5]] Therefore, the culture-based approach for GBS prevention is shown to be superior to the risk-based approach.
This study reported no resistance to ampicillin, thereby supporting ampicillin as the drug of choice for intrapartum antibiotics prophylaxis for GBS colonization in pregnant women.[[18]] However, the observed resistance to erythromycin compares to reports by other researchers.[[19]] This further supports the recommendation that antibiotic susceptibility testing for erythromycin therapy is desirable to prevent neonatal GBS infection.[[20]] However, erythromycin remains the drug of choice for women with serious penicillin allergy although Tazi et al. reported GBS susceptibility to all other antimicrobial and low-level resistance against aminoglycosides.[[21]] The opinion is that differences in antimicrobial use, prophylaxis protocol, and serotype frequency may account for these differences.[[22]]
While antibiotic resistance is global, physicians have been encouraged to join public health authorities, the infection-control community, and the pharmaceutical industry to curb the inappropriate use of antibiotics and promote responsible prescribing.[[23]]
Conclusions
Nigeria requires effective institutional as well as national policies on the prevention of neonatal GBS as the disease is not uncommon in our country as well as in other low-income countries. The culture-based approach offers better maternal and neonatal outcome which in effect may eradicate vertical GBS transmission. Parturient in Nigeria also deserve the maximal effort to treat the infection and prevent the eventual complications.

Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Valkenburg-van den Berg AW, Sprij AJ, Oostvogel PM, Mutsaers JA, Renes WB, Rosendaal FR, et al. Prevalence of colonisation with group B streptococci in pregnant women of a multi-ethnic population in the Netherlands. Eur J Obstet Gynecol Reprod Biol 2006;124:178-83.
- 2 Donbraye-Emmanuel OO, Okonko ID, Donbraye E, Ojezele MO, Ali JA, Fashina NA, et al. Isolation and characterization of group B streptococci and other pathogens among pregnant women in Ibadan Southwest Nigeria. J Appl Biosci 2010;29:1781-92.
- 3 Yancey MK, Schuchat A, Brown LK, Ventura VL, Markenson GR. The accuracy of late antenatal screening cultures in predicting genital group B streptococcal colonization at delivery. Obstet Gynecol 1996;88:811-5.
- 4 Berkley JA, Lowe BS, Mwangi I, Williams T, Bauni E, Mwarumba S. Bacteremia among children admitted to a rural hospital in Kenya. N Engl J Med 2005;352:39-47.
- 5 Adeniran AS, Aboyeji AP, Fawole AA, Adesiyun OO, Saidu R. Role of risk-based approach in the prevention of vertical transmission of neonatal sepsis. Niger Postgrad Med J 2015;22:88-92.
- 6 Costa AL, Lamy Filho F, Chein MB, Brito LM, Lamy ZC, Andrade KL. Prevalence of colonization by group B Streptococcus in pregnant women from a public maternity of northwest region of Brazil. Rev Bras Ginecol Obstet 2008;30:274-80.
- 7 Nsagha DS, Bello CS, Kahdakai-Olukemi VT. Maternal carriage in pregnancy of Group B Streptococcus in jos: Relation of endocervical-anorectal colonization. Nig Q J Hosp Med 1997;7:53-6.
- 8 Nwachukwu N, Utsalo S, Kanu I, Anyawu E. Genital colonization of group B Streptococcus at term pregnancy in Calabar, Nigeria. Int J Paediatr Neonatol 2006;7:2-6.
- 9 Onipede A, Adefusi O, Adeyemi A, Adejuyigbe E, Oyelese A, Ogunniyi T. Group B streptococcal carriage during late pregnancy in Ile-Ife, Nigeria. Afr J Clin Exp Microbiol 2012;13:135-43.
- 10 Banjo TO, Rotimi VO, Abdu OO. Colonization of pregnant women and their babies by group B streptococci. West Afr J Med 1988;7:91-6.
- 11 Adriaanse AH, Lagendijk I, Muytjens HL, Nijhuis JG, Kollée LA. Neonatal early onset group B streptococcal infection. A nine-year retrospective study in a tertiary care hospital. J Perinat Med 1996;24:531-8.
- 12 Fairlie T, Zell ER, Schrag S. Effectiveness of intrapartum antibiotic prophylaxis for prevention of early-onset group B streptococcal disease. Obstet Gynecol 2013;121:570-7.
- 13 Carvalho FJ, Almelda A, Cubal A, Torres S, Terra I, Oliveira C, et al. Assessing missed opportunities for the prevention of early onset neonatal infection by group B Streptococcus. Inter Res J Basis Clin Stud 2013;1:67-70.
- 14 Grimwood K, Stone PR, Gosling IA, Green R, Darlow BA, Lennon DR, et al. Late antenatal carriage of group B Streptococcus by New Zealand women. Aust N Z J Obstet Gynaecol 2002;42:182-6.
- 15 Stoll BJ, Schuchat A. Maternal carriage of group B streptococci in developing countries. Pediatr Infect Dis J 1998;17:499-503.
- 16 Uh Y, Jang IH, Yoon KJ, Lee CH, Kwon JY, Kim MC, et al. Colonization rates and serotypes of group B streptococci isolated from pregnant women in a Korean tertiary hospital. Eur J Clin Microbiol Infect Dis 1997;16:753-6.
- 17 Ezeonu IM, Agbo MC. Incidence and antimicrobial resistance profile of group B Streptococcus infection in pregnant women in Nsukka, Enugu State, Nigeria. Afr J Microbiol Res 2014;8:91-5.
- 18 Dzowela T, Komolafe OO, Igbigbi A. Prevalence of group B Streptococcus colonization in antenatal women at the Queen Elizabeth central hospital, Blantyre – A preliminary study. Malawi J Med 2005;17:97-9.
- 19 Mollerach A, Méndez E, Massa R, Di Conza J. Streptococcus agalactiae isolated in Santa Fe, Argentina: Antibiotic susceptibility and erythromycin-clindamycin resistance mechanisms. Enferm Infecc Microbiol Clin 2007;25:67-8.
- 20 Heelan JS, Hasenbein ME, McAdam AJ. Resistance of group B Streptococcus to selected antibiotics, including erythromycin and clindamycin. J Clin Microbiol 2004;42:1263-4.
- 21 Tazi A, Gueudet T, Varon E, Gilly L, Trieu-Cuot P, Poyart C. Fluoroquinolone-resistant group B streptococci in acute exacerbation of chronic bronchitis. Emerg Infect Dis 2008;14:349-50.
- 22 Uh Y, Jang IH, Hwang GY, Yoon KJ, Song W. Emerging erythromycin resistance among group B streptococci in Korea. Eur J Clin Microbiol Infect Dis 2001;20:52-4.
- 23 Hsu LY, Tan TY, Jureen R, Koh TH, Krishnan P, Tzer-Pin Lin R, et al. Antimicrobial drug resistance in Singapore hospitals. Emerg Infect Dis 2007;13:1944.-7.
Corresponding author
Publication History
Received: 21 June 2019
Accepted: 21 July 2019
Article published online:
10 June 2022
© 2019. Libyan International Medical University. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Valkenburg-van den Berg AW, Sprij AJ, Oostvogel PM, Mutsaers JA, Renes WB, Rosendaal FR, et al. Prevalence of colonisation with group B streptococci in pregnant women of a multi-ethnic population in the Netherlands. Eur J Obstet Gynecol Reprod Biol 2006;124:178-83.
- 2 Donbraye-Emmanuel OO, Okonko ID, Donbraye E, Ojezele MO, Ali JA, Fashina NA, et al. Isolation and characterization of group B streptococci and other pathogens among pregnant women in Ibadan Southwest Nigeria. J Appl Biosci 2010;29:1781-92.
- 3 Yancey MK, Schuchat A, Brown LK, Ventura VL, Markenson GR. The accuracy of late antenatal screening cultures in predicting genital group B streptococcal colonization at delivery. Obstet Gynecol 1996;88:811-5.
- 4 Berkley JA, Lowe BS, Mwangi I, Williams T, Bauni E, Mwarumba S. Bacteremia among children admitted to a rural hospital in Kenya. N Engl J Med 2005;352:39-47.
- 5 Adeniran AS, Aboyeji AP, Fawole AA, Adesiyun OO, Saidu R. Role of risk-based approach in the prevention of vertical transmission of neonatal sepsis. Niger Postgrad Med J 2015;22:88-92.
- 6 Costa AL, Lamy Filho F, Chein MB, Brito LM, Lamy ZC, Andrade KL. Prevalence of colonization by group B Streptococcus in pregnant women from a public maternity of northwest region of Brazil. Rev Bras Ginecol Obstet 2008;30:274-80.
- 7 Nsagha DS, Bello CS, Kahdakai-Olukemi VT. Maternal carriage in pregnancy of Group B Streptococcus in jos: Relation of endocervical-anorectal colonization. Nig Q J Hosp Med 1997;7:53-6.
- 8 Nwachukwu N, Utsalo S, Kanu I, Anyawu E. Genital colonization of group B Streptococcus at term pregnancy in Calabar, Nigeria. Int J Paediatr Neonatol 2006;7:2-6.
- 9 Onipede A, Adefusi O, Adeyemi A, Adejuyigbe E, Oyelese A, Ogunniyi T. Group B streptococcal carriage during late pregnancy in Ile-Ife, Nigeria. Afr J Clin Exp Microbiol 2012;13:135-43.
- 10 Banjo TO, Rotimi VO, Abdu OO. Colonization of pregnant women and their babies by group B streptococci. West Afr J Med 1988;7:91-6.
- 11 Adriaanse AH, Lagendijk I, Muytjens HL, Nijhuis JG, Kollée LA. Neonatal early onset group B streptococcal infection. A nine-year retrospective study in a tertiary care hospital. J Perinat Med 1996;24:531-8.
- 12 Fairlie T, Zell ER, Schrag S. Effectiveness of intrapartum antibiotic prophylaxis for prevention of early-onset group B streptococcal disease. Obstet Gynecol 2013;121:570-7.
- 13 Carvalho FJ, Almelda A, Cubal A, Torres S, Terra I, Oliveira C, et al. Assessing missed opportunities for the prevention of early onset neonatal infection by group B Streptococcus. Inter Res J Basis Clin Stud 2013;1:67-70.
- 14 Grimwood K, Stone PR, Gosling IA, Green R, Darlow BA, Lennon DR, et al. Late antenatal carriage of group B Streptococcus by New Zealand women. Aust N Z J Obstet Gynaecol 2002;42:182-6.
- 15 Stoll BJ, Schuchat A. Maternal carriage of group B streptococci in developing countries. Pediatr Infect Dis J 1998;17:499-503.
- 16 Uh Y, Jang IH, Yoon KJ, Lee CH, Kwon JY, Kim MC, et al. Colonization rates and serotypes of group B streptococci isolated from pregnant women in a Korean tertiary hospital. Eur J Clin Microbiol Infect Dis 1997;16:753-6.
- 17 Ezeonu IM, Agbo MC. Incidence and antimicrobial resistance profile of group B Streptococcus infection in pregnant women in Nsukka, Enugu State, Nigeria. Afr J Microbiol Res 2014;8:91-5.
- 18 Dzowela T, Komolafe OO, Igbigbi A. Prevalence of group B Streptococcus colonization in antenatal women at the Queen Elizabeth central hospital, Blantyre – A preliminary study. Malawi J Med 2005;17:97-9.
- 19 Mollerach A, Méndez E, Massa R, Di Conza J. Streptococcus agalactiae isolated in Santa Fe, Argentina: Antibiotic susceptibility and erythromycin-clindamycin resistance mechanisms. Enferm Infecc Microbiol Clin 2007;25:67-8.
- 20 Heelan JS, Hasenbein ME, McAdam AJ. Resistance of group B Streptococcus to selected antibiotics, including erythromycin and clindamycin. J Clin Microbiol 2004;42:1263-4.
- 21 Tazi A, Gueudet T, Varon E, Gilly L, Trieu-Cuot P, Poyart C. Fluoroquinolone-resistant group B streptococci in acute exacerbation of chronic bronchitis. Emerg Infect Dis 2008;14:349-50.
- 22 Uh Y, Jang IH, Hwang GY, Yoon KJ, Song W. Emerging erythromycin resistance among group B streptococci in Korea. Eur J Clin Microbiol Infect Dis 2001;20:52-4.
- 23 Hsu LY, Tan TY, Jureen R, Koh TH, Krishnan P, Tzer-Pin Lin R, et al. Antimicrobial drug resistance in Singapore hospitals. Emerg Infect Dis 2007;13:1944.-7.