

Subscribe to RSS
DOI: 10.4103/ajm.AJM_81_17
Submandibular lipoblastoma: Case report of a rare tumor in childhood
Authors
Financial support and sponsorship Nil.

Abstract
Lipoblastoma is a rare, benign tumor usually occurring in childhood. It is essentially localized in the extremities and trunk, with few cases reported in the neck. We report the case of a 2-year-old girl with a rapidly enlarging, painless neck mass. Magnetic resonance imaging (MRI) revealed a 3-cm mass in the right submandibular region. Review of literature, diagnostic methods, and genetics of lipomatous tumors are discussed. Complete surgical excision via a lateral cervical approach demonstrated a white soft tissue with an adherent ganglion. Histology and immunohistochemistry confirmed the diagnosis of lipoblastoma. Cervical lipoblastoma is rare, and typically asymptomatic, rarely causing nerve compression or airway obstruction. MRI can help identifying the lipomatous nature of the mass, but the findings can be inconsistent due to variable maturity of fat cells and the mesenchymal content of the tumor. Diagnosis is always based on pathological examination. Further chromosomal analysis is useful in differentiating lipoblastoma from liposarcoma. Complete surgical excision is the recommended treatment.
Introduction
Lipoblastoma is a benign tumor; it arises from embryonal fat cells and occurs in infants and children. It is mostly localized in the trunk and extremities.[1] Several cases of lipoblastoma of the neck have been reported in the literature.[2] It typically presents as a progressively enlarging, painless neck mass. However, symptoms such as respiratory compromise, Horner's syndrome, and hemiparesis can occur from compression of cervical structures.[3],[4]
Diagnosis is often suggested by magnetic resonance imaging (MRI), but can only be confirmed by pathological examination. In this report, we present an exceptional case of submandibular lipoblastoma.
Case Report
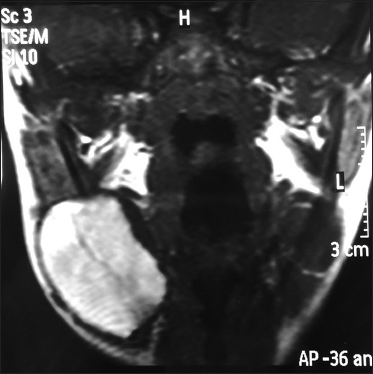
A 26-month-old full-term girl presented a palpable mass in the right submandibular region for about 9 months. There was no history of trauma, infection, dysphagia, dyspnea, stridor, or fever. She had no other discomfort or any associated symptoms such as irritable crying, vomiting, fever, or body weight loss. The physical examination revealed that the mass was soft, mobile, and measured about 4 cm without skin infiltration. The biological examinations were unremarkable. Sonography of the neck showed a well-demarcated echoic mass (with respect to the subcutaneous fat) in the right submandibular region measuring 35 mm × 20 mm. There were no color flow signals within this lesion. Otherwise, we noticed multiple bilateral lymphadenopathy. MRI demonstrated a well-defined mass of 36 mm × 23 mm × 39 mm in the right submaxillary angle showing hyperintense signals on both T1–T2, but many areas disappeared with fat suppression sequences [Figure 1].
Tumor excision through a laterocervical approach was performed and a 3.5 cm well-encapsulated, soft, yellowish-white tissue was noted in the right submandibular area. An adherent ganglion measuring 1 cm in diameter, was also resected. One year after surgical treatment, the patient did not show any recurrence.
Macroscopic examination revealed multilobular appearance with a glistening cut surface. Histopathologically, the tumor was composed of lobular aggregation of regular mature adipocytes and immature myxoid mesenchymal tissue [Figure 2] and the adherent ganglion had a normal histological aspect. All the margins were negative. Tumoral cells showed diffuse expression of PS 100 [Figure 3]. The pathological diagnosis was then circumscribed lipoblastoma.


Discussion
Lipoblastoma is a rare benign tumor of immature white fat usually found in extremities and the truck but also can be observed in the axilla, mediastinum, retroperitoneum, and prevertebral areas.[2] In the head and neck region, it accounts for about 30% of adipocytic tumors in children and typically presents as a progressively enlarging, painless mass. Although generally asymptomatic, 2 cases of respiratory compromise,[5] 2 cases of Horner's syndrome,[4] and a case of hemiparesis [4] have been reported. A case of upper extremity weakness caused by compression of the spinal cord was also reported by O'Donnell et al.[4]
Concerning diagnostic imaging studies, computed tomography can be used to demonstrate the presence of mass, but MRI is particularly helpful to suggest the histologic components of the tumor, as well as its more accurate estimation of the extent of disease, particularly in lipoblastomatosis.[6] Lipoblastoma typically appears hyperintense on both T1-and T2-weighted images, though it is consistently less intense than mature fat on T1-weighted images, likely due to its fibrous septae and the variable degree of lipomatous differentiation. Lipocytes, or mature fat cells, exhibit relatively high signal intensity on T1-weighted images, while lipoblasts show lower intensity. Therefore, despite the usefulness of MRI in assessment of lipoblastoma, it is not diagnostic, due to the presence of similar findings in other benign and malignant fatty tumors.
The differential diagnosis of lipomatous tumors should include lipoma, lipoblastoma, hibernoma, and liposarcoma. Lipomas are adipose tumors that are composed of only mature fat and do not show lobulation. The presence of lipoblasts is helpful in distinguishing lipoblastoma from other benign adipose tumors.[7]
Lipoblastoma is categorized into two types: the circumscribed lipoblastoma (~70% of cases), a superficial and encapsulated lesion, and diffuse lipoblastomatosis (about 30% of cases), a deeply located, poorly circumscribed lesion with an infiltrative growth pattern that may affect surrounding muscle structures.[2] It is important to recognize that both tumors may contain mitotic figures, as lipoblastoma is a mass of embryonic fat cells in varying degrees of differentiation. Although both tumors may contain a plexiform capillary network, this feature tends to be more prominent in liposarcoma. It is particularly important to differentiate myxoid liposarcoma from lipoblastoma, as both tumors have myxoid background. The characteristic lobulation of lipoblastoma is typically absent in liposarcoma but can be seen in the myxoid variant.
Hyperchromasia and nuclear atypia are present in liposarcoma, but are absent in lipoblastoma, and may be the most important distinguishing feature.[8]
Hibernoma, which is a tumor of embryonic brown fat, should also be considered in the differential diagnosis of lipoblastoma.[9] It also displays a lobular pattern, but it is composed entirely of brown fat with a characteristic eosinophilic, granular cytoplasm that is not present in the white fat of lipoblastoma.[7]
The present case demonstrated variable maturity of adipocytes, as well as a distinct myxoid component, without a significant degree of vascularity.
Different lipomatous tumors, such as lipoma, lipoblastoma, and liposarcoma, tend to have characteristic chromosomal abnormalities.[6],[7],[8],[9],[10] Such genetic anomalies can be used as a diagnostic supplement to histology in differentiating lipoblastoma from liposarcoma. Indeed, it has been proposed that abnormalities of chromosome 8q may be associated with upregulation of the production of the PLAG1 gene, which is considered to be the likely oncogenic target in lipoblastoma formation.[10]
Histological analysis is still mandatory. The technique of fat suppression sequencing is particularly valuable in the assessment of lipoblastoma in its ability to demonstrate the presence of fatty tissue even when standard T1 and T2 images fail to demonstrate sufficient hyperintensity of the tumor to indicate such content.
Despite the well-localized, nonmalignant nature of lipoblastomas, they are most of the time rapidly growing tumors and may eventually cause compressive symptoms. This was not the case in the patient presented in this report, the tumor was asymptomatic, and there were no compressive symptoms. Lipoblastoma does not recur when completely resected, but lipoblastomatosis has a distinct propensity for recurrence.[6] Therefore, the standard therapy for cervical lipoblastoma is complete surgical excision.
Conclusion
This case demonstrates the need to consider lipoblastoma, along with other lipomatous tumors, in the differential diagnosis of all pediatric neck masses.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
-
References
- 1 Chung EB, Enzinger FM. Benign lipoblastomatosis. An analysis of 35 cases. Cancer 1973; 32: 482-92
- 2 Basaran UN, Inan M, Bilgi S, Pul M. Lipoblastoma: A rare cervical mass in childhood. Int J Pediatr Otorhinolaryngol 2001; 61: 265-8
- 3 Rasmussen IS, Kirkegaard J, Kaasbøl M. Intermittent airway obstruction in a child caused by a cervical lipoblastoma. Acta Anaesthesiol Scand 1997; 41: 945-6
- 4 O'Donnell KA, Caty MG, Allen JE, Fisher JE. Lipoblastoma: Better termed infantile lipoma?. Pediatr Surg Int 2000; 16: 458-61
- 5 Farrugia MK, Fearne C. Benign lipoblastoma arising in the neck. Pediatr Surg Int 1998; 13: 213-4
- 6 Dilley AV, Patel DL, Hicks MJ, Brandt ML. Lipoblastoma: Pathophysiology and surgical management. J Pediatr Surg 2001; 36: 229-31
- 7 Bruyeer E, Lemmerling M, Poorten VV, Sciot R, Hermans R. Paediatric lipoblastoma in the head and neck: Three cases and review of literature. Cancer Imaging 2012; 12: 484-7
- 8 Fletcher C, editor. Diagnostic Histopathology of Tumors. Vol. 2. New York: Churchill
Livingstone; 1995. p. 1045.
- 9 Hicks J, Dilley A, Patel D, Barrish J, Zhu SH, Brandt M. et al. Lipoblastoma and lipoblastomatosis in infancy and childhood: Histopathologic, ultrastructural, and cytogenetic features. Ultrastruct Pathol 2001; 25: 321-33
- 10 Miller GG, Yanchar NL, Magee JF, Blair GK. Lipoblastoma and liposarcoma in children: An analysis of 9 cases and a review of the literature. Can J Surg 1998; 41: 455-8
Address for correspondence
Publication History
Article published online:
12 August 2021
© 2018. Syrian American Medical Society. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Private Ltd.
A-12, Second Floor, Sector -2, NOIDA -201301, India
-
References
- 1 Chung EB, Enzinger FM. Benign lipoblastomatosis. An analysis of 35 cases. Cancer 1973; 32: 482-92
- 2 Basaran UN, Inan M, Bilgi S, Pul M. Lipoblastoma: A rare cervical mass in childhood. Int J Pediatr Otorhinolaryngol 2001; 61: 265-8
- 3 Rasmussen IS, Kirkegaard J, Kaasbøl M. Intermittent airway obstruction in a child caused by a cervical lipoblastoma. Acta Anaesthesiol Scand 1997; 41: 945-6
- 4 O'Donnell KA, Caty MG, Allen JE, Fisher JE. Lipoblastoma: Better termed infantile lipoma?. Pediatr Surg Int 2000; 16: 458-61
- 5 Farrugia MK, Fearne C. Benign lipoblastoma arising in the neck. Pediatr Surg Int 1998; 13: 213-4
- 6 Dilley AV, Patel DL, Hicks MJ, Brandt ML. Lipoblastoma: Pathophysiology and surgical management. J Pediatr Surg 2001; 36: 229-31
- 7 Bruyeer E, Lemmerling M, Poorten VV, Sciot R, Hermans R. Paediatric lipoblastoma in the head and neck: Three cases and review of literature. Cancer Imaging 2012; 12: 484-7
- 8 Fletcher C, editor. Diagnostic Histopathology of Tumors. Vol. 2. New York: Churchill
Livingstone; 1995. p. 1045.
- 9 Hicks J, Dilley A, Patel D, Barrish J, Zhu SH, Brandt M. et al. Lipoblastoma and lipoblastomatosis in infancy and childhood: Histopathologic, ultrastructural, and cytogenetic features. Ultrastruct Pathol 2001; 25: 321-33
- 10 Miller GG, Yanchar NL, Magee JF, Blair GK. Lipoblastoma and liposarcoma in children: An analysis of 9 cases and a review of the literature. Can J Surg 1998; 41: 455-8