

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_148_20
Primary intracranial squamous cell carcinoma with a fatal course
Authors

Intracranial squamous cell carcinomas (SCCs) are extremely rare. They can be primary or represent a degeneration of an epidermoid cyst (EC). We report the case of a patient operated, with an endoscopic transnasal approach, for a primary intracranial SCC. The optimal management for patients with primary intracranial SCC or ECs which have undergone malignant degeneration has yet to be identified.
Introduction
Intracranial squamous cell carcinomas (SCCs) are extremely rare lesions.[[1]] Epidermoid cysts (ECs), from which they can derive, constitute 0.2%–1.8% of all intracranial tumors. It was described for the first time in 1807 by an artist in a French medical school and later (1829) documented by the pathologist Cruveilhier who referred to them as “tumours perlees” (pearly tumors).[[2]] They consist of aberrated ectodermal cells which develop into epithelium-like cells between the 3rd and 5th weeks of gestation, when the neural tube forms.[[1]] ECs have an anatomical predilection for intracranial, extra-axial, and paramedian cisternal space; the cerebellopontine angle (CPA) cistern is the most common site of presentation (50%–60%), followed by the parasellar region (30%),[[1]] in an intradural and paramedian position.[[2]] Histopathologically, they are lined by keratinized stratified squamous epithelium and grow as a consequence of continuous desquamation and degradation of cell membranes. ECs are typically benign with favorable prognosis, and they rarely degenerate into malignant SCC.[[1]] We report our experience dealing with the endoscopic transnasal approach for a primary SCC of the left CPA.
Case Report
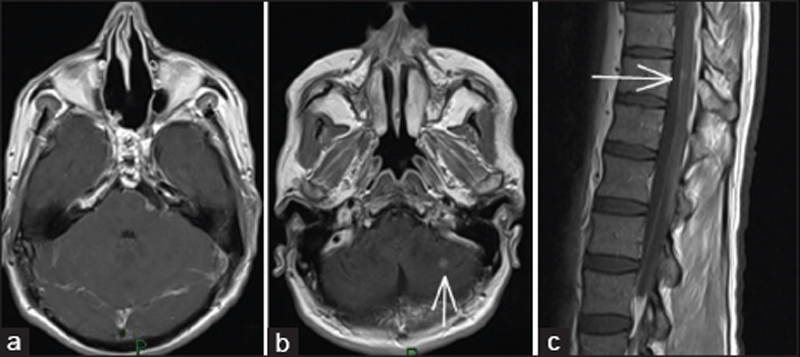
A 35-year-old male was admitted with left trigeminal (V1–V2) palsy, dizziness, and left ear hearing loss. Magnetic resonance imaging (MRI) revealed a large cystic lesion of the left cerebellopontine cistern with a possible small postcontrast impregnation of a portion of the medial wall [[Figure 1]]. The lesion displaced the fifth left cranial nerve posteriorly. An endoscopic transsphenoidal/transclival surgical removal of the lesion was scheduled. While awaiting surgery, the patient experienced rapid deterioration with vomiting, drowsiness, and headache. The day before the surgery, the patient had an episode of opisthotonus and unconsciousness preceded by intense lower back pain. An emergency head computed tomography (CT) scan revealed minimum ventricular dilatation. Surgery revealed a large cyst with a thin layer of white capsule containing soft white tissue that was macroscopically completely removed; a dural plastic with autologous fat, an intradural layer of fascia lata, hemostatic material, and a septal flap, was performed. Following surgery, the trigeminal palsy resolved, but the patient remained drowsy and reported referred frontal pain and had fever without, however, humoral signs of infection. Head CT scans showed the surgical result [[Figure 2]] and a gradual increase of ventricular system dimensions. The patient was treated with external drainage; frontal pain resolved, but the conscious state did not improve. In the meantime, the results of the histological tests came through and reported “…severe cytologic and architectural atypia with hyperchromatic nuclei, atypical mitosis and marked replicative activity (Ki67 proliferative index: About 40%). The aspects described are indicative of a malignant transformation.” Despite the postoperative cerebrospinal fluid (CSF) study and culture being normal and negative for infection, the patient continued to have fever, and cytological examination reported malignant cells in the CSF. Cerebral and spinal MRI, carried out 1 month after the surgery, confirmed leptomeningeal carcinomatosis (LC) [[Figure 3]]. The patient was transferred with ventriculoperitoneal shunt to the oncology unit where he was unable to start chemotherapy or radiotherapy due to poor neurological and clinical status. He died 1 month later. There are no reports in literature of cases with such a severe course.


Discussion
Intracranial SCC can be secondary to chronic inflammation of an EC, due to either repeated irritation and cyst rupture,[[2]],[[3]],[[4]],[[5]],[[6]],[[7]] subtotal resection of the cyst wall, recurrent meningitis,[[1]],[[2]],[[8]] introduction of a foreign material intraoperatively [[9]] or, like in our case, arise de novo. This last possibility is extremely rare, and only eight cases, other than this, are reported in literature.[[10]],[[11]],[[12]],[[13]],[[14]],[[15]],[[16]],[[17]] The clinical characteristics of these cases are summarized in [[Table 1]]. Hamlat et al. classified primary intracranial carcinomas into five categories based on clinicopathological presentation:[[8]] (1) initial malignant transformation of EC; (2) malignant transformation of remnant EC; (3) malignant transformation with LC; (4) SCC arising from another benign cyst; and (5) other malignancies arising from benign cysts including melanoma, adenocarcinoma, sarcomatoid carcinoma, and osteosarcoma. In a 2013 review, Nagasawa et al. identified 58 cases of epidermoid tumor with malignant transformation in literature published between 1912 and 2010.[[1]] ECs, radiologically, are typically hypodense on CT scan, hypointense on T1 MRI, and hyperintense on T2 imaging and diffusion weighted imaging (DWI). They have smooth margins and lack contrast enhancement. Lack of diffusion restriction, irregular margins, and presence of contrast enhancement suggest malignant changes.[[1]],[[2]],[[8]],[[18]] Radiological evidence of histological malignancy are the presence of enhancement (88% of tumors) and presence of foreign body giant cell reaction, which has focal enhancement next to EC. The presence of calcification is usually a hallmark of long-standing disease and is more often observed in benign EC. There is no specific location with a predilection for malignant degeneration. LC following malignant transformation has also been reported and tends to have a worse prognosis. Wide dissemination can occur through direct spread from an intradural primary tumor or through seeding of malignant cells in the CSF. Of the twenty reported cases of LC following malignant transformation in the literature, nine were associated with surgery.[[2]],[[19]] This indicates that intraoperative seeding is possibly a potential risk factor for tumor cells' spread.[[9]] The clinical presentation of EC could be dysfunction or irritation of cranial nerve (V–VII–VIII and X), cerebellar and brain stem dysfunction, as well as hydrocephalus and meningeal irritation.[[2]] It has been reported that hearing loss is the most common symptom in patients with epidermoid (37.6%), followed by trigeminal neuralgia (29.7%), dizziness or vertigo, facial palsy (19.4%), headache (17.9%), and diplopia (16.7%). The pathogenetic mechanism of trigeminal neuropathy in patients with CPA epidermoid remains uncertain. Direct compression of the nerve at the root entry zone, displacement of the trigeminal nerve, and compression against a blood vessel at the root entry zone, or combination of the two have been suggested as possible causes. The irritant, inflammatory nature of the epidermoid tumor could also be implied as a possible cause of pain, in cases where the nerve is completely wrapped by tumor. The keratin content may directly cause irritation and hyperactivity of the nerve without an intervening vascular loop. Tumor removal itself may relieve symptoms, but it is reported that persistent distortion of the trigeminal nerve can also often be the cause of persistent pain after satisfactory resection. Although the management for de novo primary intracranial SCC is still controversial,[[20]] the treatment of choice for ECs is surgical resection.[[1]],[[2]],[[8]] It is important also to remove the capsule in order to reduce the recurrence of the tumor,[[2]],[[8]] although it is not always possible (literature reports total removal to be between 18% and 97%). One operative complication of this type of lesion is aseptic meningitis, which is related to the spilling of cholesterol crystals into the cerebrospinal pathway.[[19]] Irrigation of the surgical field with idrocortisone solution during surgery and delayed withdrawal of steroids in the postoperative period have been advocated as possible measures for preventing chemical meningitis.[[21]] Retrospectively, we cannot exclude that, in our case, surgery was the cause of tumor cells' dissemination that leads to aseptic meningitis, which worsened the patient's neurological status, and prevented any improvement until death. However, the rapid progression of the patient's symptoms, the presence of a postcontrast enhancing of a portion of the medial wall at the preoperative MRI, and the severe lower back pain and hopistono occurred the day before surgery ( first sings of leptomeningeal dissemination?) suggest the malignancy of the lesion ab initio.

Conclusions
The optimal management for patients with primary intracranial SCC or ECs which have undergone malignant degeneration has yet to be identified. As no single treatment regimen (chemotherapy, radiotherapy, and surgery) has been proven to be dominantly effective, the most likely benefit may stem from multiple adjuvant therapies. Gamma-knife radiosurgery inhibits tumor growth for a short period of time, but any beneficial long-term effect is unlikely.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Nagasawa DT, Choy W, Spasic M, Yew A, Trang A, Garcia HM, et al. An analysis of intracranial epidermoid tumors with malignant transformation: Treatment and outcomes. Clin Neurol Neurosurg 2013;115:1071-8.
- 2 Raheja A, Eli IM, Bowers CA, Palmer CA, Couldwell WT. Primary intracranial epidermoid carcinoma with diffuse leptomeningeal carcinomatosis: Report of two cases. World Neurosurg 2016;88:692.e9-6.92E+18.
- 3 Knorr JR, Ragland RL, Smith TW, Davidson RI, Keller JD. Squamous carcinoma arising in a cerebellopontine angle epidermoid: CT and MR findings. AJNR Am J Neuroradiol 1991;12:1182-4.
- 4 Roh TH, Park YS, Park YG, Kim SH, Chang JH. Intracranial squamous cell carcinoma arising in a cerebellopontine angle epidermoid cyst: A case report and literature review. Medicine (Baltimore) 2017;96:e9423.
- 5 Cuoco JA, Rogers CM, Busch CM, Apfel LS, Entwistle JJ, Marvin EA. Intracranial squamous cell carcinoma arising from a cerebellopontine angle epidermoid cyst remnant four decades after partial resection. Front Oncol 2019;9:694.
- 6 Shaikh MY, Sharif S, Rafay M. Primary intracranial squamous cell carcinoma arising in dermoid cyst. Asian J Neurosurg 2019;14:904-6.
- 7 Agarwal S, Rishi A, Suri V, Sharma MC, Satyarthi GD, Garg A, et al. Primary intracranial squamous cell carcinoma arising in an epidermoid cyst – A case report and review of literature. Clin Neurol Neurosurg. 2007;109:888-91.
- 8 Hamlat A, Hua ZF, Saikali S, Egreteau J, Guegan Y. Malignant transformation of intracranial epidermoid cyst with leptomeningeal carcinomatosis: Case report. Acta Neurol Belg 2003;103:221-4.
- 9 Shah A, Goel A, Goel N. A case of cerebellopontine angle epidermoid tumor and brainstem squamous cell carcinoma presenting as collision tumor. Acta Neurochir (Wien) 2010;152:1087-8.
- 10 Wong SW, Ducker TB, Powers JM. Fulminatin parapontine epidermoid carcinoma in a 4-year-old. Cancer 1976;37:1521-31.
- 11 Nosaka Y, Nagao S, Tabuchi K, Nishimoto A. Primary intracranial epidermoid carcinoma. Case report. J Neurosurg 1979;50:830-3.
- 12 Garcia CA, McGarry PA, Rodriguez F. Primary intracranial squamous cell carcinoma of the right cerebellopontine angle. J Neurosurg 1981;54:824-8.
- 13 Ebisudani D, Hamazaki F, Oka H, Okada J, Ohshima T, Matsumoto K, et al. [An autopsy case of primary intracranial squamous cell carcinoma]. No Shinkei Geka 1990;18:193-8.
- 14 Jain R, Gujar S, McKeever P, Robertson P, Mukherji S. Imaging findings associated with childhood primary intracranial squamous cell carcinoma. AJNR Am J Neuroradiol 2003;24:109-11.
- 15 Mallick S, Biswas A, Kumar N, Chand Sharma M, Kumar R, Mohan Reddy R, et al. Primary intracranial basaloid squamous cell carcinoma: An enigma. Neurol Neurochir Pol 2012;46:489-95.
- 16 O'Neill BT, Segkos K, Kasper EM, Pallotta JA. Non-metastatic squamous cell carcinoma within a Rathke's cleft cyst. Pituitary 2016;19:105-9.
- 17 Liu X, Chen Z, Dong Y, He X, Pan X, Tong D. Primary intracranial squamous cell carcinoma arising de novo: A case report and review of the literature. World Neurosurg 2018;120:372-81.
- 18 Link MJ, Cohen PL, Breneman JC, Tew JM Jr. Malignant squamous degeneration of a cerebellopontine angle epidermoid tumor. Case report. J Neurosurg 2002;97:1237-43.
- 19 Lunardi P, Missori P, Rizzo A, Gagliardi FM. Chemical meningitis in ruptured intracranial dermoid. Case report and review of the literature. Surg Neurol 1989;32:449-52.
- 20 Kwon SM, Kim JH, Kim YH, Hong SH, Kim CJ. Treatment and survival outcomes of primary intracranial squamous cell carcinoma. World Neurosurg 2019;125:e1-e9.
- 21 Kapoor JR, Kapoor R, Buzea C, Gropper MR. Spinal epidermoid tumors: Novel approach to aseptic meningitis. J Spinal Disord Tech 2003;16:193-4.
Address for correspondence
Publication History
Received: 08 April 2020
Accepted: 21 May 2020
Article published online:
16 August 2022
© 2020. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Nagasawa DT, Choy W, Spasic M, Yew A, Trang A, Garcia HM, et al. An analysis of intracranial epidermoid tumors with malignant transformation: Treatment and outcomes. Clin Neurol Neurosurg 2013;115:1071-8.
- 2 Raheja A, Eli IM, Bowers CA, Palmer CA, Couldwell WT. Primary intracranial epidermoid carcinoma with diffuse leptomeningeal carcinomatosis: Report of two cases. World Neurosurg 2016;88:692.e9-6.92E+18.
- 3 Knorr JR, Ragland RL, Smith TW, Davidson RI, Keller JD. Squamous carcinoma arising in a cerebellopontine angle epidermoid: CT and MR findings. AJNR Am J Neuroradiol 1991;12:1182-4.
- 4 Roh TH, Park YS, Park YG, Kim SH, Chang JH. Intracranial squamous cell carcinoma arising in a cerebellopontine angle epidermoid cyst: A case report and literature review. Medicine (Baltimore) 2017;96:e9423.
- 5 Cuoco JA, Rogers CM, Busch CM, Apfel LS, Entwistle JJ, Marvin EA. Intracranial squamous cell carcinoma arising from a cerebellopontine angle epidermoid cyst remnant four decades after partial resection. Front Oncol 2019;9:694.
- 6 Shaikh MY, Sharif S, Rafay M. Primary intracranial squamous cell carcinoma arising in dermoid cyst. Asian J Neurosurg 2019;14:904-6.
- 7 Agarwal S, Rishi A, Suri V, Sharma MC, Satyarthi GD, Garg A, et al. Primary intracranial squamous cell carcinoma arising in an epidermoid cyst – A case report and review of literature. Clin Neurol Neurosurg. 2007;109:888-91.
- 8 Hamlat A, Hua ZF, Saikali S, Egreteau J, Guegan Y. Malignant transformation of intracranial epidermoid cyst with leptomeningeal carcinomatosis: Case report. Acta Neurol Belg 2003;103:221-4.
- 9 Shah A, Goel A, Goel N. A case of cerebellopontine angle epidermoid tumor and brainstem squamous cell carcinoma presenting as collision tumor. Acta Neurochir (Wien) 2010;152:1087-8.
- 10 Wong SW, Ducker TB, Powers JM. Fulminatin parapontine epidermoid carcinoma in a 4-year-old. Cancer 1976;37:1521-31.
- 11 Nosaka Y, Nagao S, Tabuchi K, Nishimoto A. Primary intracranial epidermoid carcinoma. Case report. J Neurosurg 1979;50:830-3.
- 12 Garcia CA, McGarry PA, Rodriguez F. Primary intracranial squamous cell carcinoma of the right cerebellopontine angle. J Neurosurg 1981;54:824-8.
- 13 Ebisudani D, Hamazaki F, Oka H, Okada J, Ohshima T, Matsumoto K, et al. [An autopsy case of primary intracranial squamous cell carcinoma]. No Shinkei Geka 1990;18:193-8.
- 14 Jain R, Gujar S, McKeever P, Robertson P, Mukherji S. Imaging findings associated with childhood primary intracranial squamous cell carcinoma. AJNR Am J Neuroradiol 2003;24:109-11.
- 15 Mallick S, Biswas A, Kumar N, Chand Sharma M, Kumar R, Mohan Reddy R, et al. Primary intracranial basaloid squamous cell carcinoma: An enigma. Neurol Neurochir Pol 2012;46:489-95.
- 16 O'Neill BT, Segkos K, Kasper EM, Pallotta JA. Non-metastatic squamous cell carcinoma within a Rathke's cleft cyst. Pituitary 2016;19:105-9.
- 17 Liu X, Chen Z, Dong Y, He X, Pan X, Tong D. Primary intracranial squamous cell carcinoma arising de novo: A case report and review of the literature. World Neurosurg 2018;120:372-81.
- 18 Link MJ, Cohen PL, Breneman JC, Tew JM Jr. Malignant squamous degeneration of a cerebellopontine angle epidermoid tumor. Case report. J Neurosurg 2002;97:1237-43.
- 19 Lunardi P, Missori P, Rizzo A, Gagliardi FM. Chemical meningitis in ruptured intracranial dermoid. Case report and review of the literature. Surg Neurol 1989;32:449-52.
- 20 Kwon SM, Kim JH, Kim YH, Hong SH, Kim CJ. Treatment and survival outcomes of primary intracranial squamous cell carcinoma. World Neurosurg 2019;125:e1-e9.
- 21 Kapoor JR, Kapoor R, Buzea C, Gropper MR. Spinal epidermoid tumors: Novel approach to aseptic meningitis. J Spinal Disord Tech 2003;16:193-4.