

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_17_20
Endoscopic third ventriculostomy for hydrocephalus in infants: A single-center experience
Authors

Introduction: Hydrocephalus remains one of the more common pathologies managed in pediatric neurosurgery. Endoscopic third ventriculostomy (ETV) has become the procedure of choice for the treatment of hydrocephalus due to aqueductal stenosis with high success rate. It has an advantage over ventriculoperitoneal (VP) shunting, as it enables patients to remain device free. Objective: The purpose of this study is to assess the role of ETV in the treatment of hydrocephalus in children under 1 year of age, including preterm low birth weight infants. Materials and Methods: A prospective study of 30 infants undergoing ETV in our institution between January 2014 and December 2018 was carried out. There were 25 cases of congenital hydrocephalus with aqueductal stenosis, two cases of Dandy–Walker cyst, two cases of cerebellopontine angle arachnoid cyst, and one case of posttubercular meningitis. ETV success score was calculated preoperatively to evaluate the percentage of success of ETV. Results: The overall success rate was 76.66% (23), with highest success rate of 84% in aqueductal stenosis. The mean age was 6.75 months (range: 1.5–12 months). Five infants were born preterm, four of them required a permanent VP shunt. There were two cases of intraoperative bleeding, four cases of cerebrospinal fluid leak from the wound, and one case of meningitis. Conclusion: ETV can be considered a safe and effective modality for the initial treatment of hydrocephalus in full-term normal birth weight infants, while the success of ETV in preterm low birth weight infants need further study of maturity at birth and birth weight as the determinant factors for the success of ETV in this special group.
Introduction
Endoscopic third ventriculostomy (ETV) has become the procedure of choice for the treatment of occlusive hydrocephalus with reported high success rate mainly for aqueduct stenosis.[[1]] ETV has an advantage over ventriculoperitoneal (VP) shunt insertion, as it enables the patient to remain device free. However, its efficacy, even now, is widely discussed in the literature.[[2]] Some reports have shown poor success rates in infants as compared to older infants.[[3]]
The aim of this study is to analyze and report our experience with ETV for the treatment of hydrocephalus in 30 children under 1 year of age, including preterm low birth weight infants.
Materials and Methods
This is a prospective study of 30 infants under the age of 1 year who underwent ETV in our institution during the period of January 2014 to December 2018. A detailed history, physical examination, and computed tomography scan was done in all the cases. Of total 30 infants, there were 25 cases of congenital hydrocephalus with aqueductal stenosis, two cases of Dandy–Walker cyst, two cases of cerebellopontine angle arachnoid cyst both infants had low Glasgow Coma Scale, so we performed ETV first as emergency basis and one case of posttubercular meningitis. ETV success score was calculated preoperatively to evaluate the percentage success of ETV as advised by Kulkarni et al. [[Table 1]].

ETV success score was 40% for one infant, 50% for 19 infants, 60.5% for two infants, 70% for four infants, and 80% for four infants.
ETV was performed using a rigid pediatric endoscope (Karl Storz, Tuttlingen, Germany), size 17F. The scope was introduced through the anterior fontanels, or a burr hole was placed just anterior to the coronal suture in the mid pupillary line in the patients with small fontanel.
The floor of the third ventricle was punctured using a Fogarty catheter, and the fenestration was enlarged using a Fogarty catheter balloon. Successful creation of stoma was confirmed by appreciating clap sign as the indicator of establishing cerebrospinal fluid (CSF) flow as well as visualization of basilar artery complex intraoperatively.
Complications of ETV such as intraoperative bleeding, postoperative infections, CSF leak, and failure of procedure were evaluated.
ETV success was defined clinically by the criteria of improvement in the patient neurological status (e.g., alertness, feeding, status of anterior fontanel, and head circumference), and surgically, as no further CSF diversion procedure required during the follow-up period of 1 year. We did not use any radiological parameter to assess the success of ETV as a very low socioeconomic status and affordability of our patients.
The follow-up period was ranged from 12 to 48 months.
Results
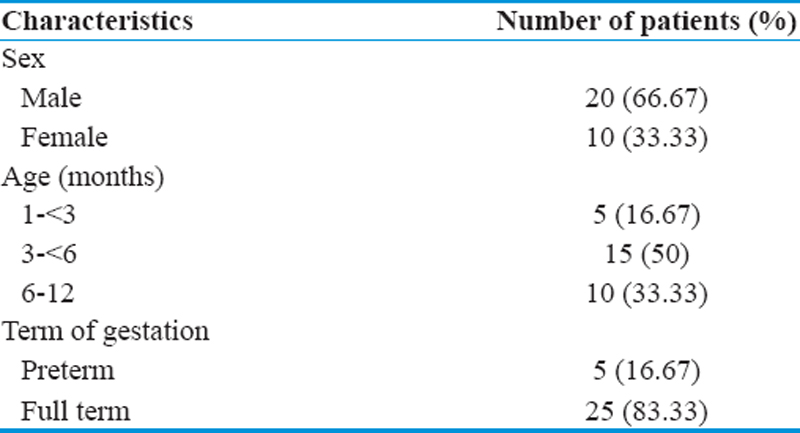
A total of 30 infants under the age of 1 year were studied. Male:female ratio was 2:1. The mean age was 6.75 months (ranged from 1.5 to 12 months). Twenty of them were <6 months, and ten infants aged between 6 and 11 months. Five infants born preterm have low birth weight [[Table 2]].
Clinical improvement in infants <6 months and infants aged 6 months to 1 year was 15 (60%) and 8 (80%), respectively. Of five prematures, low birth weight infants, one has improved (20%), while 22 (88%) out of 25 full-term normal birth weight infants showed clinical improvement, which was sustained during the follow-up period, and this was statistically significant (P < 0.001) [[Table 3]].

The overall success rate of ETV was 76.66% (23/30). In patients with obstructive hydrocephalus secondary to aqueduct stenosis, the success rate was 21 out of 25 (84%), the success rate in CP angle arachnoid cyst was 1 out of 2 (50%), and Dandy–Walker cyst was 1 out of 2 (50%) [[Table 4]].

Four of the five preterm infants required a permanent VP shunt. There were two cases of intraoperative bleeding which stopped after continuous irrigation in one case, while the procedure had to be abandoned in another patient due to continuous bleeding. Four cases developed CSF leak from the burr hole site, which may be associated with very thin cortex. Leak stopped in three cases on postoperative days 3–5 with conservative management, and one case required resuturing of pericranium graft. One case developed meningitis who recovered with proper antibiotic treatment [[Table 5]].

Discussion
The overall clinical success rate of ETV in our study was 76.66%. These results are comparable to other studies which show the success rate of 64%–85% in infants.[[4]],[[5]],[[6]]
Under the age of 1 year, ETV also has a higher success rate in case of aqueduct stenosis than in case of other etiology although significantly less than in older children.[[7]],[[8]]
The failure rate of ETV was 23.33% (7/30) in the present study, including six cases of persistence of clinical signs and symptoms of hydrocephalus in the follow-up period, which may be due to the reclosure of stoma with the formation of the arachnoid membrane. Apart from the age, etiology as the determinant factors for the success of ETV in full-term infants for preterm low birth weight infants maturity at birth and their birth weight should be addressed further for the high failure of ETV in this particular subset of patients, and one case in which procedure was abandoned due to persistent intraoperative bleeding.
The failure rate of ETV in low birth weight premature infants (n = 5) was higher (80%) as compared to full-term normal birth weight infants (16%).[[9]],[[10]] Reasons for the low efficacy of ETV in preterm low birth weight infants are still debatable but distensible head with its immature skull may be real culprit, which would prevent an adequate flow through the ETV, and it may be responsible for insufficient pressure gradient between the cortical subarachnoid spaces and the venous sinuses as advised by Zucchelli and Galassi.[[11]]
In the present study, the overall complication rate was 23.33%. The most common complications included CSF leak (13.33%), intraoperative bleeding (6.66%), and infection (3.33%) results were comparable to other studies.[[12]],[[13]],[[14]]
The overall shunt rate post-ETV was 23.33% (7/30), of this, 71.4% (5/7) of shunt required in 0–6-month age group infants, and 28.6% of shunt placement done in 6–12-month age group infants.[[15]]
Conclusion
ETV can be considered a safe and effective modality for the initial treatment of hydrocephalus in full-term normal birth weight infants, while the success of ETV in preterm low birth weight infants need further study of maturity at birth and birth weight as the determinant factors for the success of ETV in this special group.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Elbaba S, Steinmetz M, Ross J, Moon D, Luciano M. Endoscopic third ventriculostomy for objective hydrocephalus in the pediatric population: Evaluation of outcome. Eur J Pediatr Surg 2001;11 Supp 1:S52-4.
- 2 Saute JAM, Jardim LB. Riluzole in patients with hereditary cerebellar ataxia. Lancet Neurol 2016;15:788-9.
- 3 Koch D, Wagner W. Endoscopic third ventriculostomy in infants of less than 1 year of age: Which factors influence the outcome? Childs Nerv Syst 2004;20:405-11.
- 4 Gorayeb RP, Cavalheiro S, Zymberg ST. Endoscopic third ventriculostomy in children younger than 1 year of age. J Neurosurg 2004;100:427-9.
- 5 Yadav YR, Jaiswal S, Adam N. Endoscopic third ventriculostomy in infants. Neurology (India) 2006;54:161-3.
- 6 Etus V, Ceylan S. Success of endoscopic third ventriculostomy in children less than 2 years of age. Neurosurg Rev 2005;28:284-8.
- 7 Kulkarni AV, Drake JM, Mallucci CL, Sgouros S, Roth J, Constantini S, et al. Endoscopic third ventriculostomy in the treatment of childhood hydrocephalus. J Pediatr 2009;155:254-90.
- 8 Grunert P, Charalampaki P, Hopf N, Filippi R. The role of third ventriculostomy in the management of obstructive hydrocephalus. Minim Invasive Neurosurg 2003;46:16-21.
- 9 Ogiwara H, Dipatri AJ Jr., Alden TD, Bowman RM, Tomita T. Endoscopic third ventriculostomy for obstructive hydrocephalus in children younger than 6 months of age. Childs Nerve Syst 2010;26:343-7.
- 10 Jung TY, Chong S, Kim IY, Lee JY, Phi JH, Kim SK, et al. Prevention of complications in endoscopic third ventriculostomy. J Korean Neurosurg Soc 2017;60:282-8.
- 11 Zucchelli M, Galassi E. Higher failure of endoscopic third ventriculostomy in infants: The “distensible” skull is the culprit. Pediatr Neurosurg 2018;53:163-6.
- 12 Vulcu S, Eickele L, Cinalli G, Wagner W, Oertel J. Long-term results of endoscopic third ventriculostomy: An outcome analysis. J Neurosurg 2015;123:1456-62.
- 13 Elgamal EA, El-Dawlatly AA, Murshid WR, El-Watidy SM, Jamjoom ZA. Endoscopic third ventriculostomy for hydrocephalus in children younger than 1 year of age. Childs Nerv Syst 2011;27:111-6.
- 14 Furlanetti LL, Santos MV, Oliveira RS. Neuroendoscopic surgery in children: An analysis of 200 consecutive procedures. Arq Neuropsiquiatr 2013;71:165-70.
- 15 Jernigan SC, Berry JG, Graham DA, Goumnerova L. The comparative effectiveness of ventricular shunt placement versus endoscopic third ventriculostomy for initial treatment of hydrocephalus in infants. J Neurosurg Pediatr 2014;13:295-300.
Address for correspondence
Publication History
Received: 15 January 2020
Accepted: 20 April 2020
Article published online:
16 August 2022
© 2020. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Elbaba S, Steinmetz M, Ross J, Moon D, Luciano M. Endoscopic third ventriculostomy for objective hydrocephalus in the pediatric population: Evaluation of outcome. Eur J Pediatr Surg 2001;11 Supp 1:S52-4.
- 2 Saute JAM, Jardim LB. Riluzole in patients with hereditary cerebellar ataxia. Lancet Neurol 2016;15:788-9.
- 3 Koch D, Wagner W. Endoscopic third ventriculostomy in infants of less than 1 year of age: Which factors influence the outcome? Childs Nerv Syst 2004;20:405-11.
- 4 Gorayeb RP, Cavalheiro S, Zymberg ST. Endoscopic third ventriculostomy in children younger than 1 year of age. J Neurosurg 2004;100:427-9.
- 5 Yadav YR, Jaiswal S, Adam N. Endoscopic third ventriculostomy in infants. Neurology (India) 2006;54:161-3.
- 6 Etus V, Ceylan S. Success of endoscopic third ventriculostomy in children less than 2 years of age. Neurosurg Rev 2005;28:284-8.
- 7 Kulkarni AV, Drake JM, Mallucci CL, Sgouros S, Roth J, Constantini S, et al. Endoscopic third ventriculostomy in the treatment of childhood hydrocephalus. J Pediatr 2009;155:254-90.
- 8 Grunert P, Charalampaki P, Hopf N, Filippi R. The role of third ventriculostomy in the management of obstructive hydrocephalus. Minim Invasive Neurosurg 2003;46:16-21.
- 9 Ogiwara H, Dipatri AJ Jr., Alden TD, Bowman RM, Tomita T. Endoscopic third ventriculostomy for obstructive hydrocephalus in children younger than 6 months of age. Childs Nerve Syst 2010;26:343-7.
- 10 Jung TY, Chong S, Kim IY, Lee JY, Phi JH, Kim SK, et al. Prevention of complications in endoscopic third ventriculostomy. J Korean Neurosurg Soc 2017;60:282-8.
- 11 Zucchelli M, Galassi E. Higher failure of endoscopic third ventriculostomy in infants: The “distensible” skull is the culprit. Pediatr Neurosurg 2018;53:163-6.
- 12 Vulcu S, Eickele L, Cinalli G, Wagner W, Oertel J. Long-term results of endoscopic third ventriculostomy: An outcome analysis. J Neurosurg 2015;123:1456-62.
- 13 Elgamal EA, El-Dawlatly AA, Murshid WR, El-Watidy SM, Jamjoom ZA. Endoscopic third ventriculostomy for hydrocephalus in children younger than 1 year of age. Childs Nerv Syst 2011;27:111-6.
- 14 Furlanetti LL, Santos MV, Oliveira RS. Neuroendoscopic surgery in children: An analysis of 200 consecutive procedures. Arq Neuropsiquiatr 2013;71:165-70.
- 15 Jernigan SC, Berry JG, Graham DA, Goumnerova L. The comparative effectiveness of ventricular shunt placement versus endoscopic third ventriculostomy for initial treatment of hydrocephalus in infants. J Neurosurg Pediatr 2014;13:295-300.