
Subscribe to RSS
DOI: 10.4103/ajns.AJNS_206_19
Modification of periosteal flap as management of cerebrospinal fluid leakage after frontal sinus fracture surgery in moderate traumatic brain injury patients

Main management for the frontal sinus fracture is using the pericranial flap. Pericranial flaps based on the supraorbital and supratrochlear vasculature have previously been used with significant success for the separation of intracranial and extracranial spaces after major trauma. Defect closure was modified due to lack of the frontal periosteum; the graft was made from the temporal side of periosteum to make primary periosteal flap longer. Defect closure could be optimum. Evaluation for 6 months showed a significant improvement without major complications. In this article, we propose a new modification technique as one of promising alternatives.
#
Introduction
Management of extensive frontal sinus fractures in case of traumatic brain injury (TBI) has been a concern for 100 years.[[1]] The surgical techniques for management frontal sinus were derived from the treatment of frontal sinusitis and had many complications. Because of the complications, it remains controversial. In this patient, extensive disruption of the posterior table of the frontal sinus has a reasonable prognosis for recovery, ablation of the frontal sinus by cranialization has been recommended.[[2]]
Cerebrospinal fluid (CSF) leakage development has been a major concern. Patients would require a craniotomy to access the injured site of the brain to allow better visualization of any tears of the dura.[[3]] In this case, the frontal sinus has been closed by periosteal flap and nasofrontal duct has been obliterated by muscular patch. This maneuver is advocated and practiced by many surgeons to separate the paranasal sinuses from the brain. To decrease the incidence of a CSF leak following a dural repair, several techniques, including the use of allogenic and autogenous materials, have been recommended.
Pericranial flaps based on the supraorbital and supratrochlear vasculature have previously been used with significant success for the separation of intracranial and extracranial spaces after major trauma and reconstructive effort in the head, especially anterior skull base. Although frontal sinus obliteration also requires the removal of sinus mucosa and separation from the nasal vault, protection of the exposed intracranial contents is a critical issue encountered only during cranialization.[[2]]
#
Case Report
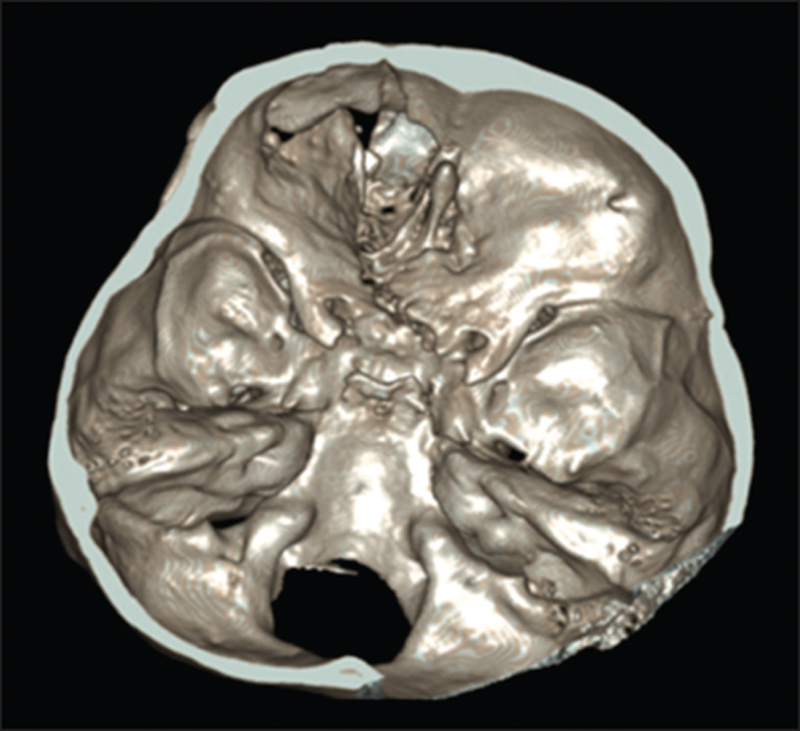
A 19-year-old female with a history of decreased consciousness after a traffic accident in 2016, fell from a motorcycle. Primary survey was performed; there was an open wound with fractured skull based on the left frontal region. The patient came with Glasgow Coma Scale (GCS) E3V3M5 with pupil round, equal 3 mm on both eyes, and light reflex was normal on both eyes. Laboratory tests were performed, there was no abnormality on laboratory results. Noncontrast head computed tomography (CT) scan was performed. Depressed fracture and biconvex-shaped hematoma were found on the left frontal region. The patient was diagnosed with moderate TBI, epidural hematoma (EDH) on the left frontal region, and open frontal sinus fracture. Craniotomy evacuation of EDH, cranialization, decortication, and debridement was performed [[Figure 1]].

After the surgery, the patient's condition was gradually improved, was put under postoperative care for a few days, and was subsequently discharged. However, the head CT scan on postoperative day 30, a pneumatocele was present at the frontal region [[Figure 2]]. Despite of radiologic findings, the patient did not have any major complaints.

The patient was returned to the hospital 22 months after the surgery with a chief complaint of rhinorrhea and severe headache for 3 months. The patient was prescribed pain-killer drugs, but the complaint did not significantly improve. The headache worsened without a decrease of consciousness. Head magnetic resonance imaging was performed to investigate the underlying causes. T2 sequence was suggestive of arachnoid cyst filled with CSF on the left frontal area. Differential diagnosis included a frontal defect at the previous surgical site [[Figure 3]].

General examination and vital signs were normal. On neurological examination, the GCS was E4V5M6 with round and equal pupil and bilaterally positive light reflex. There was no lateralization or sensoric deficit. Thin-sliced head CT scan was performed to observe any presence of skull base defect [[Figure 4]].
The patient underwent second craniotomy with supine position, and bicoronal incision uses old scars as mark. After doing skin flap, periosteal, and bone flap, the defect of frontal sinus can be exposed. The main problem of this procedure is shortness of the periosteal flap because the patient had been underwent surgical periosteal flap before in EDH and first decranialization. For this procedure, we prepare for redecortication of the frontal sinus, defect exploration, defect closure with modification periosteal graft and temporal muscle, and external ventricular drainage (EVD) on the right Kocher point. Defect closure was modified due to the short nature of the frontal periosteum, some periosteal from temporal muscle grafted to make primary periosteal flap longer. Defect closure could be optimum. The primary suture was done to stitch it with temporal muscle using standard bicoronal incision and skin flap [[Figure 5]].

Postoperative general and neurological statuses were good, headache had receded, and rhinorrhea had stopped. On postoperative 3rd day, patient's consciousness improved and headache decreased. On evaluative CT scan, the pneumocephalus had gotten smaller. The second and third evaluations on 9th and 13th revealed that pneumocephalus appeared even smaller. After 8 days of surgery, the patient has done a dependent test for the shunt, and CSF analysis was sterile. In this patient we performed ventriculo-peritoneal Shunt due to shunt dependent. The last CT performed on 1 month after surgery showed that the pneumocephalus had improved further. There was a slight hyperdense appearance which was suspected for a minute bleeding [[Figure 6]].

Improvement of the clinical appearance of the patient after undergo this procedure is followed until 6 months. There are no major complaints, and then, the patient followed by an evaluation of CT scan and pneumocephalus of the left frontal side has been decreased.
Surgical technique
The patient's entire scalp is shaved. After administration of a local anesthetic with a vasoconstrictor, a standard bi-temporal incision is made, and the bi-temporal flap elevation is performed in a subgaleal plane up to the nasofrontal area. The first three layers of the scalp (skin, subcutaneous tissue, and galea aponeurotica) are elevated, whereas the pericranium and loose areolar connective tissue are left attached to the skull. The pericranial flap is then outlined. The length of the flap cannot be as long as the initial scalp incision, so it can be extended by performing a subgaleal dissection further posteriorly beyond the initial scalp incision. The lateral extents of the flap correspond to the temporal fusion lines, where the superficial and deep layers of the deep temporal fascia fuse with the pericranium. The pericranial flap anteriorly and based on the deep branches of the supraorbital and supratrochlear arteries. A subperiosteal dissection is then performed to elevate the pericranial flap from the skull to the level of the supraorbital rims. The fractured frontal sinus and anterior cranial fossa are exposed. Necrotic brain is removed, and any dural tears are closed primarily with nonresorbable sutures. Fibrin sealant is applied over the repair. The mucosa is removed from the sinus walls as well as from the nasofrontal ducts, and a peripheral ostectomy is performed. If a formal craniotomy has been performed, the pericranial flap is adapted to line the anterior cranial fossa. In this case, there is defect at dura mater that makes leakage of the CSF. The modification of pericranial flap is the addition of the periosteal graft from temporal. It can be sutured to the dura or can be placed passively. The anterior wall is replaced and secured using plates and screws. All bony impingements on the vascular supply of the flap must be relieved. The bitemporal flap is then closed in a layered fashion, and a pressure dressing is applied and maintained for 48 h.
#
#
Discussion
Separation of the brain tissue from the paranasal sinus space is a consideration in many surgical procedures. Cranial base tumor resection and trauma with a significant injury to the frontal sinus and skull base may lead to communication between the brain tissue and paranasal sinuses and may be complicated by a dural tear and CSF leak. A communication between these environments should be surgically repaired to prevent future complications such as retrograde spread of infection from the paranasal region into the brain resulting in meningitis or subdural and brain abscesses. Many techniques are described in the literature regarding frontal sinus obliteration (Fattahi, 2009). Actually in this case, the management of the fracture of frontal sinus had been done. Complication acquired is CSF leakage, it could be inadequate of decranialization. In the other hand, intraoperative decision of closing, the dural defect could be very difficult and tricky. In this presented case, we found shortening of the pericranial flap.
Many uses for the pericranial flap can be found in the literature. It has been used for the reconstruction of nasal septal defects, coverage of cochlear implants,[[7]] and reconstruction of external auditory canal following mastoidectomy, periorbital soft-tissue reconstruction, coverage of soft-tissue defects with bone exposure such as in full-thickness avulsion of scalp defects due to trauma and reconstruction.[[8]] The pericranial flap has also been extensively used in craniofacial reconstruction to provide soft-tissue bulk. In trauma surgery, this flap gives the surgeon the opportunity to seal a CSF leak and provides viable tissue for the obliteration of the frontal sinus and the isolation of the intracranial from the paranasal environment. Since it is locally available during the bitemporal flap elevation, it obviates the need for other autogenous or allogeneic materials, such as abdominal fat, tensor fascia lata, or synthetic bone cements.[[4]],[[5]],[[6]] Consideration of the main vasculature of this case should be as the first. We decided to use periosteal graft.
The anteriorly based pericranial flap, as used in this report, has a reliable vascular supply that has been extensively studied. This axial flap is based on the deep branches of the supraorbital and supratrochlear arteries. Anatomical studies performed by Yoshioka and colleagues recommend that dissection in the subgaleal plane does not extend past 1 cm cephalad to the supraorbital ridge, to avoid compromising the blood supply to the flap secondary to the variation in the anatomy of the bifurcation of the superficial and deep branches of the supraorbital and supratrochlear arteries.[[7]] Venous drainage of the flap is by means of the transverse supraorbital vein, which also courses within 1 cm cephalad to the supraorbital rim.[[9]] The entire flap can be elevated and used to obliterate the frontal sinus or line the anterior cranial fossa, or it can be sectioned in the midline while maintaining the blood supply to each half of the flap.
Based on the research of Yoshioka, 2005, about the vascular anatomy of anterior based on the pericranial flap, the frontal pericranial flap has to focused on the deep arteries and veins supplying the pericranium [[Figure 7]]. The deep branches of the supraorbital and supratrochlear arteries that supply the frontal pericranial flap divided from the supraorbital and supratrochlear arteries at the level of the supraorbital rim or below in approximately 70% of cases. In the remainder, the deep pericranial branches of the supraorbital or supratrochlear artery were separated from the superficial branch 5.5–15 mm (mean: 8.6 mm) above the orbital rim. If the separation of pericranium from the galea-frontalis layer begins near the coronal suture and extends downward to the orbital rim, the major deep branches to the pericranium will be transected in nearly 30% of cases. Actually, in this case, we still preserve for the vascularization of the flap from supraorbital and supratrochlear and gives a modification, adding a rich vascularization graft from the temporal region at the same side.[[10]]

The study of the Yoshioka and Rhoton, 2005, the supraorbital nerve courses along the orbital roof and divide into superficial and deep branches near the orbital rim. The superficial branch enters the galea-frontalis layer, and the deep branch ascends on the pericranium. The supratrochlear nerve had only a superficial branch that disappeared into the corrugator muscle at the level of the supraorbital rim. Supraorbital artery, the main or superficial trunk of the supraorbital artery, the major supply of a frontal pericranial flap that is based on the supraorbital rim gave rise to an average of 2.4 (range: 2–4 mm), deep pericranial branches having an average diameter of 0.59 mm (range, 0.2–1.2 mm). Supratrochlear artery, a smaller and more medially coursing vessel than the supraorbital artery, entered the corrugator muscle at the level of the supraorbital rim and divided into a superficial branch to the superficial layers of the scalp and a deep branch to the pericranium. The supratrochlear arteries give rise to an average of 1.5 (range: 1–3 mm), deep branches having an average diameter of 0.39 mm (range: 0.2–0.8 mm).The venous drainage of the frontal scalp is divided into a group of larger veins that drain the superficial layers of the scalp, including the galea-frontalis layer, and a group of smaller veins that drain the pericranium. Supraorbital and supratrochlear nerve, the supraorbital nerve coursed along the orbital roof and turned upward at the orbital rim. It had superficial and deep branches. The superficial branch passed around the orbital rim, entered the galea-frontalis layer near the supraorbital rim, and ascended in the frontal scalp. In assumption that kind of anatomical structure, this modification of standard procedure adding a periosteal graft for pericranial flap could have satisfaction results.[[10]]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
#
#
#
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Ravindra VM, Neil JA, Shah LM, Schmidt RH, Bisson EF. Surgical management of traumatic frontal sinus fractures: Case series from a single institution and literature review. Surg Neurol Int 2015;6:141.
- 2 Donath A, Sindwani R. Frontal sinus cranialization using the pericranial flap: An added layer of protection. Laryngoscope 2006;116:1585-8.
- 3 Fattahi T, Dipasquale J. Utility of the pericranial flap in frontal sinus and anterior cranial fossa trauma. Int J Oral Maxillofac Surg 2009;38:1263-7.
- 4 Ilankovan V, Adcock SD. The galeo pericranial flap in oropharyngeal reconstruction. Br J Oral Maxillofac Surg 1996;34:47-50.
- 5 Jensen R, McCutcheon IE, DeMonte F. Postoperative swelling of pericranial pedicle graft producing intracranial mass effect. report of two cases. J Neurosurg 1999;91:124-7.
- 6 Leatherbarrow B, Watson A, Wilcsek G. Use of the pericranial flap in medial canthal reconstruction: Another application for this versatile flap. Ophthalmic Plast Reconstr Surg 2006;22:414-9.
- 7 Paloma V, Samper A, Cervera-Paz FJ. Surgical technique for reconstruction of the nasal septum: the pericranial flap. Head Neck 2000;22:90-4.
- 8 Wang RC, Parisier SC, Weiss MH, Chute PM, Hellman SA, Sauris E. Cochlear implant flap complications. Ann Otol Rhinol Laryngol 1990;99:791-5.
- 9 Yoshioka N, Kishimoto S. Anteriorly based pericranial flap: an anatomic study of feeding arteries. Skull Base Surg 1991;1:161-4.
- 10 Yoshioka N, Rhoton AL Jr. Vascular anatomy of the anteriorly based pericranial flap. Neurosurgery 2005;57:11-6.
Address for correspondence
Publication History
Received: 01 July 2019
Accepted: 19 November 2019
Article published online:
16 August 2022
© 2020. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Ravindra VM, Neil JA, Shah LM, Schmidt RH, Bisson EF. Surgical management of traumatic frontal sinus fractures: Case series from a single institution and literature review. Surg Neurol Int 2015;6:141.
- 2 Donath A, Sindwani R. Frontal sinus cranialization using the pericranial flap: An added layer of protection. Laryngoscope 2006;116:1585-8.
- 3 Fattahi T, Dipasquale J. Utility of the pericranial flap in frontal sinus and anterior cranial fossa trauma. Int J Oral Maxillofac Surg 2009;38:1263-7.
- 4 Ilankovan V, Adcock SD. The galeo pericranial flap in oropharyngeal reconstruction. Br J Oral Maxillofac Surg 1996;34:47-50.
- 5 Jensen R, McCutcheon IE, DeMonte F. Postoperative swelling of pericranial pedicle graft producing intracranial mass effect. report of two cases. J Neurosurg 1999;91:124-7.
- 6 Leatherbarrow B, Watson A, Wilcsek G. Use of the pericranial flap in medial canthal reconstruction: Another application for this versatile flap. Ophthalmic Plast Reconstr Surg 2006;22:414-9.
- 7 Paloma V, Samper A, Cervera-Paz FJ. Surgical technique for reconstruction of the nasal septum: the pericranial flap. Head Neck 2000;22:90-4.
- 8 Wang RC, Parisier SC, Weiss MH, Chute PM, Hellman SA, Sauris E. Cochlear implant flap complications. Ann Otol Rhinol Laryngol 1990;99:791-5.
- 9 Yoshioka N, Kishimoto S. Anteriorly based pericranial flap: an anatomic study of feeding arteries. Skull Base Surg 1991;1:161-4.
- 10 Yoshioka N, Rhoton AL Jr. Vascular anatomy of the anteriorly based pericranial flap. Neurosurgery 2005;57:11-6.