

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_218_17
Endoscopic approach to thalamic and intraventricular hemorrhage
Authors

Objective: To highlight the basic points of brain endoscopic procedure for Thalamic and Intraventricular Hemorrhage to achieve repeatability and reproducibility in the results among the new brain endoscopic surgeons. Method: Sharing the experience of 10 years as an endoscopic surgeon to bring out the basic insight into the method, challenges, points which need special attention during the surgery and discussion of recent advancements in the endoscopic equipment for safe surgery. Conclusion: Procedure of endoscopic evacuation of brain hematoma is simple with learning curve. In the beginning new endoscopic surgeons should operate in the presence of experience surgeon. They should follow standard technique to achieve the good surgical outcome and uniformity in the result every time they perform the surgery.
Introduction
Basic endoscopic skills have already been discussed previous three papers on putaminal, subcortical, and cerebellar hemorrhage. Thalamic hemorrhage is deep, so it is very invasive to approach by craniotomy. The authors have experience of about 50 cases of endoscopic evacuation of the thalamic hematoma through intraventricular route. Once we introduce the lucent sheath in the hematoma cavity, the process is same like another hematoma evacuation. We can control intracranial pressure and hydrocephalus by evacuating hematoma from the 3rd ventricle and can wait for sometime without intervention.
Before Operation
Indication
All kinds of intraventricular hemorrhage (IVH) and thalamic hemorrhage (TH) can be evacuated through the endoscope. If there is very small thalamic hematoma or hematoma on one side only, may not be operated. External ventricular drainage (EVD) should be placed in case of worsening of the hydrocephalus in these cases.
Preoperative examination
Magnetic resonance angiography or computed tomography angiography (CTA) should be done. The authors prefer digital subtraction angiography to CTA as this can exclude arteriovenous malformation (AVM), arteriovenous fistula (AVF), moyamoya, aneurysmal hemorrhage, high or low flow AVM/AVF, and venous angiomas. Venous malformations are contraindication for surgery. It is difficult to coagulate bleeding from big vessel. Marking on the skull for entry point should be done with CT scan (axial, coronal, and sagittal image). MRI T2 STIR image can show the bleeding point.
Instrumentation
We need both the rigid and flexible endoscope along with the translucent sheath of both the large and smaller diameter. Bigger one needed in case of expected bleeding or to coagulate the larger vessel. It is better if we have a suction tube with irrigation. Otherwise, we can use angiographic sheath or catheter for irrigation which can be placed in the suction or endoscope. We need a special tool for hemostasis in case of using flexible endoscope [[Figure 1]].

Approach
We need to investigate the position, extension, and wideness of the hematoma. There can be three approaches for the hematoma evacuation from thalamic and intraventricular bleed.
-
Anterior horn
-
Posterior horn
-
Direct puncture to the hematoma
In some cases, we can combine all three of them:
-
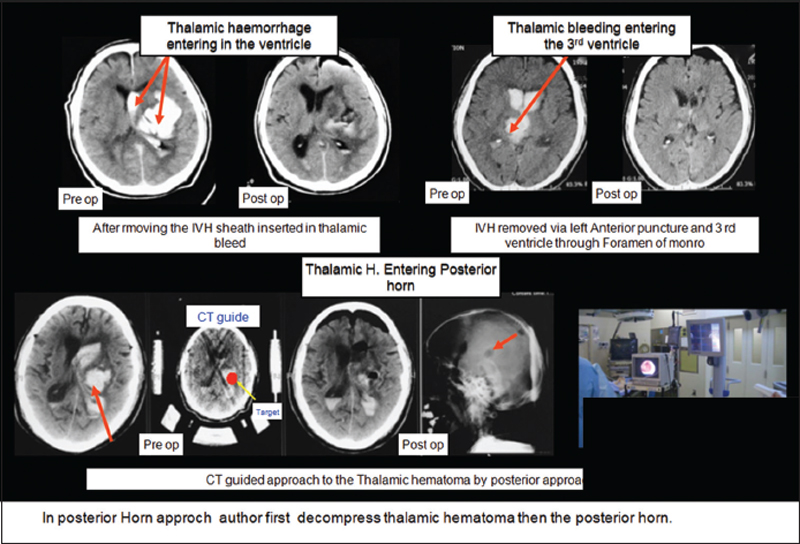
Anterior horn puncture – This approach is used for IVH in the lateral horns, body, and 3rd ventricular hematoma. This approach is not used for hematoma in the posterior horn. This can also be used in ventricular hemorrhage with TH in medial upper direction. In this approach, TH can be evacuated after evacuating the intraventricular part. Sheath is advanced in the thalamic hematoma after evacuating the ventricular part
-
Posterior horn puncture – This is better approach for thalamic hematoma which extends to posterior horn and brainstem in posteroinferior direction. We need navigation system or CT-guided system for the evacuation as there is no landmark for orientation as in case of anterior horn approach
-
Direct puncture – If the hemorrhage is in the anterolateral direction close to the putaminal/temporal region, we can use the direct puncture as in case of putaminal or subcortical hemorrhage [[Figure 2]].
Anesthesia and Positioning
The authors prefer to evacuate under general anesthesia as it may take longer time to evacuate the hematoma. Position is decided by the approach and wideness of the hematoma [[Figure 3]].

Approach: Evacuation of Thalamic Hematoma
For puncture through the anterior horn, translucent sheath is inserted and flexible endoscope is introduced. Anatomical landmarks, for example, foramen of monro and choroid plexus confirmed. When sheath is placed in hematoma cavity, we change from flexible to rigid endoscope. Hematoma cavity is observed with the help of irrigation and suction.
In case of puncture through the posterior horn, it is better to use navigation system or CT-guided system to decide the puncture point. Once sheath is inserted in the hematoma cavity, irrigation is stopped and evacuation of the thalamic hematoma is started. In thalamic hematoma, we push the sheath lightly in the hematoma, and it is evacuated inside out because if CSF start coming in the sheath, initially, it is difficult to perform the procedure. If the thalamic hematoma is removed directly, it is removed in the same way as described before, inside-to-outside technique [[Figure 4]].

Technique
There can be four-hand technique which is commonly practiced in which surgeon holds rigid scope with the right hand and keep irrigation suction in the left hand. Assistant holds the sheath and helps with irrigation and coagulation. In two-hand technique, surgeon holds scope in the right hand and irrigation, suction, and sheath with the left hand. Although the two-hand technique is faster, it needs much more expertise [[[Figure 5]] and Video].

Evacuation of intraventricular hemorrhage
In case of IVH, when we use rigid endoscope, we can suction out all the hematomas very fast. Due to this sudden collapse of ventricle some time brain shrinks and can cause acute subdural hematoma. The authors advocate the use of flexible endoscope for the evacuation of IVH. We can do slow evacuation and continuous irrigation with the flexible endoscope and keep the ventricle expanded to avoid sudden collapse and its complications. In flexible endoscope, we remove hematoma from the hole in the endoscope. We must know the position of hole so that we can suction with one hole and use other instruments, for example, monopolar and forceps with another hole. We put the hole toward the hematoma and suction with 5-10 ml syringe. When the hematoma amount is large, it can block the suction. If the endoscope gets blocked, hematoma is flushed off outside the brain. This procedure is repeated several times until the ventricles get cleared. If the aqueduct is dilated, we can negotiate flexible endoscope in the 4th ventricle for evacuation of hematoma, but the authors do not recommend this due to high risk. To prevent the hydrocephalus, we either can do the 3rd ventriculostomy or EVD can be left after the operation. Sheathless technique can also be used if there is a route for the egress of the fluid; bilateral EVD or one side EVD has been done and we proceed from the other side. Scope can be moved more freely without the sheath, but we should be careful for the vital structure around the ventricle. Endoscope is negotiated by irrigation and pushing technique into the ventricle in sheathless procedure. This procedure is not recommended as standard, but sometimes, it is very effective and better to know this technique [[Figure 6]].

Checking hemostasis
There are small perforators in thalamic bleed so hemostasis can be easily achieved. Monopolar is used for coagulation like in other bleeding. In IVH, new bleeding is unlikely to occur unless we injure the ventricular structure. We should take care of the veins on the ventricular wall, bleeding from the choroid plexus, tract, and the puncture point. Mostly bleeding is stopped with water pressure by taking endoscope close to the bleeding point. Vital tissue can be damaged if we use coagulation tool. Bleeding should be stopped, every time we find them. If there is large intraventricular bleeding, it must be stopped by irrigation, pressure, or drainage. New bleeding hematoma is sometimes hard to evacuate. It needs bigger sheath and suction tube and may need to change from flexible to rigid endoscope. If there is small hematoma on the bleeding point, it should not be pulled out.
Closure
If the 3rd ventricle is clear, no hematoma in aqueduct and 3rd ventriculostomy has been done, and then, there is no need for the ventricular drainage. After the endoscopic procedure, tract is bigger than the normal drainage, so there may be postoperative subdural hygroma or CSF leak. The authors use hemostatic material, for example, fibrin glue for the closure of the tract, dural closure with suture, and application of fibrin glue on the suture line. The authors prefer to close the burr hole with ceramic cap. Skin and muscles are closed like normal durotomy.
Conclusion
We can remove the hematoma less invasively with neuroendoscope, and we can get good result in cases of thalamic hematoma with IVH.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India