

RSS-Feed abonnieren
DOI: 10.4103/ajns.AJNS_245_18
Neurosurgical management of parasagittal and falcine meningiomas: Judicious modern optimization of the results in a 100-case study
Autoren

Context: The management of parasagittal and falcine meningiomas centers around the relationship between the tumor and the venous anatomy of the superior sagittal sinus (SSS) and the bridging veins. Aims: The present study aims to address neurosurgical outcomes in a cohort of patients with parasagittal and falcine meningiomas >2.0 cm in the largest diameter, in which a neurosurgical/multidisciplinary treatment was considered. Settings and Design: The clinical outcomes of patients undergoing neurosurgical management for parasagittal and falcine meningiomas at the authors' institution over a 15-year period were analyzed. Analysis was limited to those tumors (primary, residual, or recurrences) >2.0 cm in the largest diameter. Subjects and Methods: The authors identified 100 patients with parasagittal/falcine meningiomas >2.0 cm in their largest diameter, who underwent neurosurgical treatment at their institution between 1999 and 2013. Statistical Analysis Used: Tumor control was assessed using Kaplan–Meier analysis, and specific attention was paid to the relationship between the tumor and the SSS and its impact on tumor control and outcome. Results: There was no difference in rates of tumor control in patients who received subtotal resection for a WHO Grade I tumor, followed by close observation, compared with those undergoing gross-total resection, primarily because no cases were observed in which the tumor remnant in the SSS demonstrated interval growth on serial imaging studies. Of patients in this series, 13% experienced at least one neurological, medical, surgical, or radiosurgical complication, and the mortality was 0%. Conclusions: These data provide a more judicious optimization of the expected outcome that can be obtained with treatment of these tumors, in which a combination of image guidance, advanced microsurgical techniques, and conformal radiation treatments is used.
Introduction
As the second most common region of origin for intracranial meningiomas, the basic pathological, anatomical, and surgical features of parasagittal and falcine meningiomas are familiar to most neurosurgeons.[[1]],[[2]],[[3]],[[4]],[[5]],[[6]],[[7]] More specifically, the management of these tumors centers around the relationship between the tumor and venous anatomy of the superior sagittal sinus (SSS), and the large cerebral veins that enter the sinus in proximity of them.[[1]],[[5]],[[7]],[[8]],[[9]],[[10]] The propensity for these tumors to encase or adhere to cerebral veins, or to invade the venous sinus, can greatly complicate our efforts to achieve the safe, complete removal of the tumor and its involved dural base.[[1]],[[5]],[[7]],[[8]],[[9]],[[10]]
Over recent decades, stereotactic radiosurgery (SRS) and conformal radiotherapy (CRT) have been established as safe and effective methods for limiting the growth of appropriately sized meningiomas.[[7]],[[11]],[[12]] Some investigators have proposed the use of radiosurgery as the sole treatment for most small parasagittal and falcine meningiomas, due to the lack of any markedly radiosensitive structures in the vicinity of these tumors.[[7]],[[8]] In cases of small, minimally symptomatic tumors without imaging features that are of concern or a known history of rapid growth on serial imaging studies, SRS or CRT should be given serious consideration, even though we still consider surgery or a “wait and see” strategy. In the last option, we perform magnetic resonance imaging (MRI) contrast-enhanced examination every 6 months for the 1st year and then every 12 months.
In the present study, our aim was to address neurosurgical outcomes in a focused cohort of patients with parasagittal and falcine meningiomas for which both SRS and transcranial resection were considered for a state-of-the-art management. Our study series include too patients from the era of radiosurgery in full, started in our Department in 1996, whom outcomes data for neurosurgical treatment are most relevant for the present neurosurgical practice.
Subjects and Methods
Patient population
These patients were adults (age ≥18 years) who underwent neurosurgical multidisciplinary treatment at the authors' Neurosurgical Department between 1999 and 2013, had preoperative MRI and postoperative computed tomography scan (CT-scan) imaging (<24 h), and had at least 1 year of clinical and neuroradiological (MRI) follow-up. Patients with hemangiopericytomas were excluded from the study. For each patient, MRI studies were reviewed to confirm diagnosis of a parasagittal or falcine meningioma, which were defined as those that primarily arose either from the falx or from the dura mater at the lateral edge of the SSS. In general, surgical cases involved tumors >2.0 cm in largest diameter, tumors with imaging features raising concerns for higher histological grade (that is, irregular borders, an indistinct interface with the cortical surface), tumors growing rapidly on serial imaging, and tumors with significant symptoms referable to mass effect.
Outcome assessment
Central pathological review was performed on the basis of the WHO guidelines.[[13]] Clinical data were collected from patient records and telephone interviews. All clinical assessments were performed by a neurosurgeon. In each case, the extent of resection and Simpson grade [[7]],[[14]],[[15]] were determined using a combination of the surgeon's assessment and MRI.
Neurosurgical strategy and perioperative management
Intraoperative neuronavigation was routinely used to minimize the skin incision and craniotomy size while attempting a Simpson Grade 1 resection. Preoperative embolization was not considered even for the large tumors because often, the vascular supply for these larger tumors included pial supply. In general, en bloc resection was not attempted for large tumors, due to tumor size, and instead the tumor was debulked from within using an ultrasonic aspirator. Careful attention was paid to identifying and respecting the arachnoid plane at the tumor–brain interface, which facilitates complete resection and minimizes pial vessel injury. Whenever possible, involved dura was resected with a 2-cm circumferential margin, and the dura was closed with either a pericranial graft or the artificial dura substitute. For lesions with bone invasion, the craniectomy site was repaired using methyl methacrylate. For larger cranial defects, a preoperative custom-made cranioplasty was used.
Although the goal of the operation from the outset was total tumor removal, the discovery of significant involvement of the SSS or the bridging cortical veins often limited these attempts and was managed as follows. We generally do not resect patent cortical bridging veins involved with tumor, and we leave tumor remnants that are densely adherent to these vessels. Completely occluded venous sinuses were resected, taking care to spare any patent cortical bridging veins on the edges of the occluded portion of the sinus. Complete sinus occlusion was generally confirmed using the venous phases obtained during the digital subtraction angiography (DSA) studies or a technically adequate MR venogram as evidence of complete sinus occlusion. More commonly, we noted invasion of tumor into a patent sinus. In case of small invasion of the SSS, tumor can be removed using patient microsurgical dissection of the dura layers, with hemostasis obtained with bipolar coagulation, or hemostatic agents combined with fibrin glues or reconstructions techniques when necessary. We do not attempt removal of larger degrees of tumor invasion of a patent sinus and instead leave this portion of the tumor, which is observed using serial imaging, and treated with radiosurgery immediately postoperatively, or the time of progression or with surgery if the sinus is completely occluded by the tumor. For falcine meningiomas, that portion of the falx below the SSS is resected after the bulky tumor is removed. This then qualifies the removal as Simpson Grade 1.
Intraoperatively, all patients received Decadron (8 mg), mannitol (1 g/kg), and ceftriaxone (2 gr) at the time of incision. On postoperative day 1, a prophylactic dose of enoxaparin (4000 UI subcutaneously each day) was initiated in all patients and continued for 2 weeks. Routine use of venous thrombosis prophylaxis was not started until after 1999.[[7]],[[16]] The incidence of postoperative intracranial hemorrhage was no different in the patient groups before or after prophylaxis was begun.[[7]],[[17]] Irrespective of preoperative seizure history, all patients had also received loading doses of an antiepileptic agent at the time of surgery (Dintoin initially, Keppra most recently), which was continued for 2 weeks postoperatively and then discontinued.
In the immediate postoperative period (<24 h), a CT-scan imaging was performed to all patients. MRI was performed at 6-month intervals for all patients for a period of 2 years. For those patients with known residual tumor after surgery, and those with WHO Grade II or III tumors, MRI was continued at 1-year interval. Patients with gross totally resected WHO Grade I tumors were followed clinically and with MRI at 2-year interval. In case of new or worsened symptoms, urgent MRI was performed. Recurrence was defined as any unequivocal, new enhancement in the resection cavity. Tumor progression was defined as any unequivocal increase in the size of the residual tumor seen on the immediate postoperative imaging. For purposes of comparing rates of tumor control, recurrence and progression were treated as a similar event.
Statistical analysis
Statistical analysis was performed using the Kaplan–Meier method. Binary variables were compared using the Pearson Chi-square test. Continuous variables were compared using an independent samples t-test or ANOVA, after statistical confirmation of data normality. Continuous variables are presented as the mean ± standard error. Statistical tests were considered significant when P < 0.05 after correcting for multiple comparisons using the Bonferroni method. All odds ratios reflect the risk of having new or worse neurological dysfunction after surgery.
Results
Demographics and presenting symptoms
We identified 100 patients with symptomatic, and/or growing, >2.0 cm in the largest diameter parasagittal/falcine meningiomas who underwent multidisciplinary neurosurgical treatment of their lesion at our department between 1999 and 2013. The median length of follow-up was 6.9 years (range 1–15 years). The basic demographics are summarized in [[Table 1]]. Significant invasion of SSS was noted in 46 (46%) of 100 cases. The age and sex distribution of these patients did not differ significantly from that in patients without sinus invasion. Tumors invading the sinus were more commonly WHO Grade II or III (58% vs. 32%, P < 0.01), commonly larger, but there was no difference in histopathological type between tumors associated with the anterior, middle and posterior thirds of the sinus. There was no WHO Grade III meningiomas in patients referred to the group without sinus invasion.

The presenting symptoms for patients in this series are summarized in [[Table 2]]. Approximately one-third of all patients, many of whom had tumors more than 4 cm in largest diameter, presented without referable symptoms or deficits (35 of 100). Headaches (in 25 of 100) and seizures (in 16 of 100) occurred commonly. Ataxia/gait disturbance, unilateral weakness occurred as frequently as lower extremity weakness. Notable was the interesting occurrence of new-onset psychotic symptoms in 5 patients, 3 of whom demonstrated invasion of the SSS.

Management of superior sagittal sinus invasion and the impact on tumor control
Four of 46 patients with sinus occlusion were found to have complete sinus occlusion on preoperative studies, and the involved portion of the sinus was fully resected in all 4 patients. None of these patients experienced recurrence of their tumor over a median follow-up period of 9.9 years (range 2.6–13.4 years). In 30 of 42 cases, the sinus invasion was minor and could be removed using careful microsurgical dissection, with hemostasis obtained using gel foam, fibrin glue, and occasionally suturing the sinus wall. In the other 12 cases, more significantly sinus invasion was noted, and the tumor was subtotally resected, the exposed attachments coagulated, and the remnant tumor left in the sinus. Nine of the 12 patients undergoing subtotal resection (STR) received SRS within 3–5 months after surgery to treat the residual tumor in the sinus (60 Gy in 20 fractions). One (WHO Grade III) of the patients who received upfront radiosurgery, demonstrated subsequent tumor growth during follow-up (5.2 years postoperatively), and was treated with repeat surgery. None of the other seven patients who received upfront radiosurgery demonstrated any evidence of subsequent tumor growth over a follow-up period of 9.3 years (range 2.1–14 years). One of the 30 patients receiving complete tumoral removal and one of the three receiving STR experienced tumor recurrence or progression over a follow-up period of 7.7 years (range 1.7–15 years). All 2 patients with recurrence had WHO Grade II tumors, which were treated with repeat surgery at the time of recurrence. Of the 54 patients in which no sinus invasion was found at surgery, gross total resection (GTR) was obtained in 51 of them. In the cases in which STR was performed, the tumor was adherent to bridging veins, which forced an STR to spare venous anatomy. All 3 patients undergoing STR, underwent radiosurgery within 3 months of surgery (60 Gy in 20 fractions). For all of them (WHO Grade II tumors) there was no evidence of subsequent tumor recurrence or progression during follow-up. There were 2 recurrences in the patients who underwent GTR, involving WHO Grade II tumors, which recurred at 3.45 and 5.75 years postoperatively, and were treated with repeat surgery at the time of recurrence. In this series, there were no patients who had WHO Grade I GTR, which recurred at the overall period of follow-up.
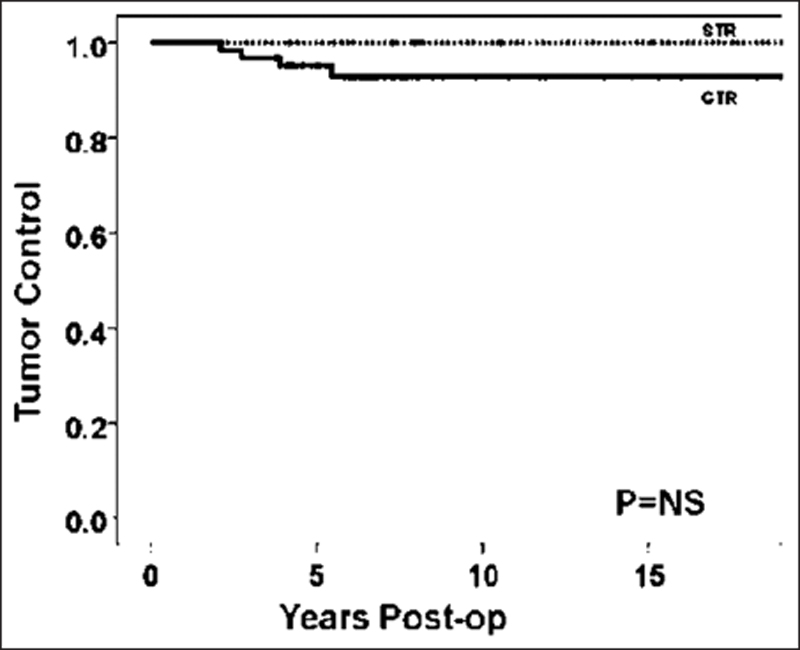
We performed Kaplan–Meier analysis for patients with WHO Grade I tumors to compare recurrence/progression-free survival for patients GTR versus STR. Patients who underwent upfront radiosurgery to the remnant lesion following STR were excluded from this analysis, to study the natural history of small tumor remnants that remained in the SSS or were attached to the veins. As seen in [[Figure 1]], there was no difference in rates of tumor control for patients who received STR for a Grade I tumor, followed by close observation, compared with those undergoing GTR, primarily because we did not observe any cases in which the tumor remnant in the SSS demonstrated interval growth on serial imaging studies.
Morbidity
In this series, 87% of patients did not experience any complications as a result of neurosurgical treatment [[Table 3]]. Three of 100 patients experienced new or worsened neurological deficits after surgery, referable to surgical manipulation around the motor strip. Medical complications were relatively uncommon (5 of 100 patients). Neurosurgical/radiosurgical complications constituted the majority of complications in this series (8 of 100 patients). Brain edema was the most common complication (including 2 patients underwent SRS for residual tumor within 3 months of surgery). None of the four patients with brain edema required surgical treatment. There was 1 episode of venous infarction noted. The cause of venous infarction in this case was not determined; however, it did not occur in a patient with a known vein sacrifice, or with documented venous sinus thrombosis.

Discussion
In this study, we reported our experience with neurosurgical management of parasagittal and falcine meningiomas in a focus of patients, who author believes best represent the volume of patients treated in contemporary neurosurgery, namely those with meningiomas >2.0 cm in the largest diameter. These tumors are frequently symptomatic, often higher grade, and in some cases are massive. More than one-third of the tumors in this series exceeded 4 cm in diameter, and 7 tumors in this series exceeded 8 cm in diameter. Despite these challenges, we have found that complete resection or good tumor control with acceptable low rates of morbidity can be achieved with advanced microneurosurgical techniques and thoughtful consideration of the venous anatomy and its relationship to the tumor.
A principal goal of our analysis was to provide data in addition to the outcomes for patients with these tumors, regarding the surgical and clinical significance of invasion of the SSS. Whereas tumors causing complete sinus occlusion can usually be removed in their entirety, and tumors that do not invade the sinus can usually be resected without great difficulty, the management of tumors invading the SSS and causing incomplete sinus occlusion has always posed the greatest surgical dilemma.[[1]],[[2]],[[3]],[[18]] The continuous evolution of microneurosurgical techniques led to an increasingly aggressive attempts at complete surgical removal of parasagittal meningiomas.[[5]],[[9]],[[19]],[[20]],[[21]] In this treatment paradigm, complete resection is the goal of all surgeries, with direct surgical removal of tumor from the sinus performed if necessary. Maintenance of central venous outflow in this approach is achieved using surgical patching of the sinus, or a bypass procedure if necessary.
This study presents our results with the alternate approach of removing as much tumor as possible while preserving major cortical veins and leaving tumor remnants that significantly involve the sinus.[[7]],[[8]]
In this approach, as previously reported by Sughrue et al.,[[7]] the residual tumor can be followed closely with serial imaging and treated with radiosurgery or repeat surgery in the event of subsequent growth. We have found that even with minor degrees of sinus invasion, we were able to remove all of the tumor without heroic efforts. The tumor control rates we have observed are excellent, with the majority of the recurrences that we observed resulting from higher grade tumor histopathological features. These data suggest that small residual portions of WHO Grade I tumors left in and around the SSS do not grow appreciably for several years after surgery, even without adjuvant radiation-based treatments.
The results do not obviate the need for many years of close imaging follow-up, but they suggest that radiosurgical management of residual disease might be delayed or even avoided in some patients. We support that in general these data suggest a move toward less aggressive resection in cases of tumor invasion of a patent sinus. In cases of minor invasion, we will continue to attempt to address these fragments surgically. However, given our good results by simply leaving tumor in the sinus, following the remnant with serial imaging, and managing recurrences with radiosurgery or repeat surgery, it seems less necessary to be surgically heroic in these cases.
In cases involving the anterior one-third of the SSS in which the MR venogram or four vessel DSA shows at least 2 other draining veins on the opposite side, remote from the region of involved sinus, we believe it is safe to consider limited or even complete sinus resection. In cases of complete occlusion of the SSS, total excision is safe. However, in cases with incomplete occlusion, or when there are fewer than 2 veins on the opposite side, separation of the leaves of the dura matter preserving the inner layer of the lateral wall of the SSS is acceptable.
Close observation and radiosurgery as needed are important in the management of WHO Grade I tumors that invade a patent sinus, especially for remnants in the middle and posterior one-third of the sinus. The data of our study suggest that in many cases, radiosurgery can be delayed because many tumor remnants in the sinus do not grow on serial imaging. Planning resection and grafting of the sinus, given the great rates of tumor control seen in radiosurgery, seems of no role in the neurosurgical management of these tumors. As previously reported by Smith et al.,[[22]] we treat WHO Grade II tumors with selective use of radiotherapy. We treat all WHO Grade III tumors with external beam radiotherapy.[[23]]
Conclusions
Authors present their experience with neurosurgical management of parasagittal/falcine meningiomas >2.0 cm in the largest diameter. The fact the median follow-up period is of 9.9 years in our analysis can be considered as a limitation of our study. However, these data provide a judicious modern estimate of the expected outcomes that can be obtained after treating patients with these tumors, using a combination of advanced microneurosurgical techniques and tools, image guidance, and treatment with CRT.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Chung SB, Kim CY, Park CK, Kim DG, Jung HW. Falx meningiomas: Surgical results and lessons learned from 68 cases. J Korean Neurosurg Soc 2007;42:276-80.
- 2 Colli BO, Carlotti CG Jr., Assirati JA Jr., Dos Santos MB, Neder L, Dos Santos AC. Parasagittal meningiomas: Follow-up review. Surg Neurol 2006;66 Suppl 3:S20-7.
- 3 Giombini S, Solero CL, Lasio G, Morello G. Immediate and late outcome of operations for parasagittal and falx meningiomas. Report of 342 cases. Surg Neurol 1984;21:427-35.
- 4 Korshunov AG, Timirgaz VV, Kalinina EE, Kozlov AV. The characteristics of the histological structure of parasagittal meningiomas and their effect on postoperative recurrence. Zh Vopr Neirokhir Im N N Burdenko 1996;10-5.
- 5 Kozlov AV, Gabibov GA, Konovalov AN, Korshunov AG, Timigraz VV, Kalinina EE. Optimization of surgical strategy in parasagittal meningiomas. A 1605-case study. Clin Neurol Neurosurg 1997;99 Suppl 1:S6.
- 6 Nishimoto A. Parasagittal and falx meningiomas – Surgical technique (author's transl). No Shinkei Geka 1974;2:17-22.
- 7 Sughrue ME, Rutkowski MJ, Shangari G, Parsa AT, Berger MS, McDermott MW. Results with judicious modern neurosurgical management of parasagittal and falcine meningiomas. Clinical article. J Neurosurg 2011;114:731-7.
- 8 Kondziolka D, Flickinger JC, Perez B. Judicious resection and/or radiosurgery for parasagittal meningiomas: Outcomes from a multicenter review. Gamma knife meningioma study group. Neurosurgery 1998;43:405-13.
- 9 Sindou M. Meningiomas invading the sagittal or transverse sinuses, resection with venous reconstruction. J Clin Neurosci 2001;8 Suppl 1:8-11.
- 10 Sindou M, Hallacq P, Ojemann RG, Laws ER Jr. Aggressive vs. conservative treatment of parasagittal meningiomas involving the superior sagittal sinus. In: Al-Mefty O, Origitano TC, Harkey HL, editors. Controversies in Neurosurgery. New York: Thieme Medical Publishers; 1996. p. 80-9.
- 11 Kondziolka D, Levy EI, Niranjan A, Flickinger JC, Lunsford LD. Long-term outcomes after meningioma radiosurgery: Physician and patient perspectives. J Neurosurg 1999;91:44-50.
- 12 Kondziolka D, Mathieu D, Lunsford LD, Martin JJ, Madhok R, Niranjan A, et al. Radiosurgery as definitive management of intracranial meningiomas. Neurosurgery 2008;62:53-8.
- 13 Kleihues P, Sobin LH. World Health Organization classification of tumors. Cancer 2000;88:2887.
- 14 Kinjo T, al-Mefty O, Kanaan I. Grade zero removal of supratentorial convexity meningiomas. Neurosurgery 1993;33:394-9.
- 15 Simpson D. The recurrence of intracranial meningiomas after surgical treatment. J Neurol Neurosurg Psychiatry 1957;20:22-39.
- 16 Agnelli G, Piovella F, Buoncristiani P, Severi P, Pini M, D'Angelo A, et al. Enoxaparin plus compression stockings compared with compression stockings alone in the prevention of venous thromboembolism after elective neurosurgery. N Engl J Med 1998;339:80-5.
- 17 Cage TA, Lamborn KR, Ware ML, Frankfurt A, Chakalian L, Berger MS, et al. Adjuvant enoxaparin therapy may decrease the incidence of postoperative thrombotic events though does not increase the incidence of postoperative intracranial hemorrhage in patients with meningiomas. J Neurooncol 2009;93:151-6.
- 18 Nowak A, Marchel A. Surgical treatment of parasagittal and falx meningiomas. Neurol Neurochir Pol 2007;41:306-14.
- 19 Sindou M, Hallacq P. Venous reconstruction in surgery of meningiomas invading the sagittal and transverse sinuses. Skull Base Surg 1998;8:57-64.
- 20 Sindou M, Wydh E, Jouanneau E, Nebbal M, Lieutaud T. Long-term follow-up of meningiomas of the cavernous sinus after surgical treatment alone. J Neurosurg 2007;107:937-44.
- 21 Sindou MP, Alvernia JE. Results of attempted radical tumor removal and venous repair in 100 consecutive meningiomas involving the major dural sinuses. J Neurosurg 2006;105:514-25.
- 22 Smith JS, Lal A, Harmon-Smith M, Bollen AW, McDermott MW. Association between absence of epidermal growth factor receptor immunoreactivity and poor prognosis in patients with atypical meningioma. J Neurosurg 2007;106:1034-40.
- 23 Sughrue ME, Sanai N, Shangari G, Parsa AT, Berger MS, McDermott MW, et al. Outcome and survival following primary and repeat surgery for World Health Organization grade III meningiomas. J Neurosurg 2010;113:202-9.
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
09. September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Chung SB, Kim CY, Park CK, Kim DG, Jung HW. Falx meningiomas: Surgical results and lessons learned from 68 cases. J Korean Neurosurg Soc 2007;42:276-80.
- 2 Colli BO, Carlotti CG Jr., Assirati JA Jr., Dos Santos MB, Neder L, Dos Santos AC. Parasagittal meningiomas: Follow-up review. Surg Neurol 2006;66 Suppl 3:S20-7.
- 3 Giombini S, Solero CL, Lasio G, Morello G. Immediate and late outcome of operations for parasagittal and falx meningiomas. Report of 342 cases. Surg Neurol 1984;21:427-35.
- 4 Korshunov AG, Timirgaz VV, Kalinina EE, Kozlov AV. The characteristics of the histological structure of parasagittal meningiomas and their effect on postoperative recurrence. Zh Vopr Neirokhir Im N N Burdenko 1996;10-5.
- 5 Kozlov AV, Gabibov GA, Konovalov AN, Korshunov AG, Timigraz VV, Kalinina EE. Optimization of surgical strategy in parasagittal meningiomas. A 1605-case study. Clin Neurol Neurosurg 1997;99 Suppl 1:S6.
- 6 Nishimoto A. Parasagittal and falx meningiomas – Surgical technique (author's transl). No Shinkei Geka 1974;2:17-22.
- 7 Sughrue ME, Rutkowski MJ, Shangari G, Parsa AT, Berger MS, McDermott MW. Results with judicious modern neurosurgical management of parasagittal and falcine meningiomas. Clinical article. J Neurosurg 2011;114:731-7.
- 8 Kondziolka D, Flickinger JC, Perez B. Judicious resection and/or radiosurgery for parasagittal meningiomas: Outcomes from a multicenter review. Gamma knife meningioma study group. Neurosurgery 1998;43:405-13.
- 9 Sindou M. Meningiomas invading the sagittal or transverse sinuses, resection with venous reconstruction. J Clin Neurosci 2001;8 Suppl 1:8-11.
- 10 Sindou M, Hallacq P, Ojemann RG, Laws ER Jr. Aggressive vs. conservative treatment of parasagittal meningiomas involving the superior sagittal sinus. In: Al-Mefty O, Origitano TC, Harkey HL, editors. Controversies in Neurosurgery. New York: Thieme Medical Publishers; 1996. p. 80-9.
- 11 Kondziolka D, Levy EI, Niranjan A, Flickinger JC, Lunsford LD. Long-term outcomes after meningioma radiosurgery: Physician and patient perspectives. J Neurosurg 1999;91:44-50.
- 12 Kondziolka D, Mathieu D, Lunsford LD, Martin JJ, Madhok R, Niranjan A, et al. Radiosurgery as definitive management of intracranial meningiomas. Neurosurgery 2008;62:53-8.
- 13 Kleihues P, Sobin LH. World Health Organization classification of tumors. Cancer 2000;88:2887.
- 14 Kinjo T, al-Mefty O, Kanaan I. Grade zero removal of supratentorial convexity meningiomas. Neurosurgery 1993;33:394-9.
- 15 Simpson D. The recurrence of intracranial meningiomas after surgical treatment. J Neurol Neurosurg Psychiatry 1957;20:22-39.
- 16 Agnelli G, Piovella F, Buoncristiani P, Severi P, Pini M, D'Angelo A, et al. Enoxaparin plus compression stockings compared with compression stockings alone in the prevention of venous thromboembolism after elective neurosurgery. N Engl J Med 1998;339:80-5.
- 17 Cage TA, Lamborn KR, Ware ML, Frankfurt A, Chakalian L, Berger MS, et al. Adjuvant enoxaparin therapy may decrease the incidence of postoperative thrombotic events though does not increase the incidence of postoperative intracranial hemorrhage in patients with meningiomas. J Neurooncol 2009;93:151-6.
- 18 Nowak A, Marchel A. Surgical treatment of parasagittal and falx meningiomas. Neurol Neurochir Pol 2007;41:306-14.
- 19 Sindou M, Hallacq P. Venous reconstruction in surgery of meningiomas invading the sagittal and transverse sinuses. Skull Base Surg 1998;8:57-64.
- 20 Sindou M, Wydh E, Jouanneau E, Nebbal M, Lieutaud T. Long-term follow-up of meningiomas of the cavernous sinus after surgical treatment alone. J Neurosurg 2007;107:937-44.
- 21 Sindou MP, Alvernia JE. Results of attempted radical tumor removal and venous repair in 100 consecutive meningiomas involving the major dural sinuses. J Neurosurg 2006;105:514-25.
- 22 Smith JS, Lal A, Harmon-Smith M, Bollen AW, McDermott MW. Association between absence of epidermal growth factor receptor immunoreactivity and poor prognosis in patients with atypical meningioma. J Neurosurg 2007;106:1034-40.
- 23 Sughrue ME, Sanai N, Shangari G, Parsa AT, Berger MS, McDermott MW, et al. Outcome and survival following primary and repeat surgery for World Health Organization grade III meningiomas. J Neurosurg 2010;113:202-9.