

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_252_20
Endoscopic transcortical transventricular management of cystic craniopharyngioma: Outcome analysis of 32 cases at a tertiary care center
Authors

Background: Microsurgical resection has been considered the gold standard treatment of craniopharyngioma, but lately, it has found less favor due to its morbidity and is being replaced by minimally invasive cyst drainage procedures. We present our experience of transventricular endoscopy and cyst drainage along with its technique and have analyzed its results. Materials and Methods: Clinical and radiological data of all cystic craniopharyngioma patients treated by transventricular endoscopic cyst drainage and Ommaya placement were retrieved and analyzed Results: Thirty-two patients underwent endoscopic cyst drainage during the study period. All patients had immediate clinical and radiological improvement. No significant complications were seen. All patients underwent adjuvant radiotherapy and six patients (18.7%) showed recurrence. Three patients died in the follow-up period. Conclusions: Endoscopic transcortical transventricular cyst drainage with Ommaya reservoir along with adjuvant radiotherapy is a simple, safe, and effective treatment modality.
Key-words:
Cystic craniopharyngioma - cystocisternostomy - endoscopic transcortical transventricular - Ommaya - radiotherapyIntroduction
Craniopharyngiomas are benign neoplasm with malignant behavior and account for nearly 3% of all intracranial tumors.[[1]],[[2]],[[3]],[[4]],[[5]] About 60%–90% of all craniopharyngiomas have a cystic component and propensity to extend into the anterior third ventricle, interpeduncular cistern, and retro and parasellar region.[[1]],[[3]],[[6]] Gross total resection of this tumor is the gold standard surgical treatment, but the preservation of neurological and hypothalamopituitary functions is also an important facet in the management of this complex tumor.[[5]]
Microscopic surgical resection and endoscopic cyst fenestration along with intracystic catheter placement of the Ommaya reservoir are the commonly performed surgical techniques.[[1]],[[7]],[[8]],[[9]],[[10]] Transcortical transventricular endoscopic surgery for cystic craniopharyngioma has gained acceptance as a safe minimally invasive alternative to resection.[[11]],[[12]]
In this retrospective study, an outcome analysis of transcortical transventricular endoscopically treated cystic craniopharyngioma over a period of 9 years was performed.
Materials and Methods
Records of 95 craniopharyngioma patients were retrieved from the departmental database, who were operated between January 2009 and October 2017 in the Department of Neurosurgery at King George's Medical University, Lucknow, India.
Thirty-two out of 95 patients had undergone endoscopic transcortical transventricular decompression and drainage along with cerebrospinal fluid (CSF) diversionary procedure, were included in this retrospective study. Ethical approval for conducting this study was taken from the institutional ethics committee.
Demographic details, clinical presentations, radiological features, intraoperative findings, details of CSF diversionary procedure, surgical complications, and follow-up details were noted.
Surgical technique
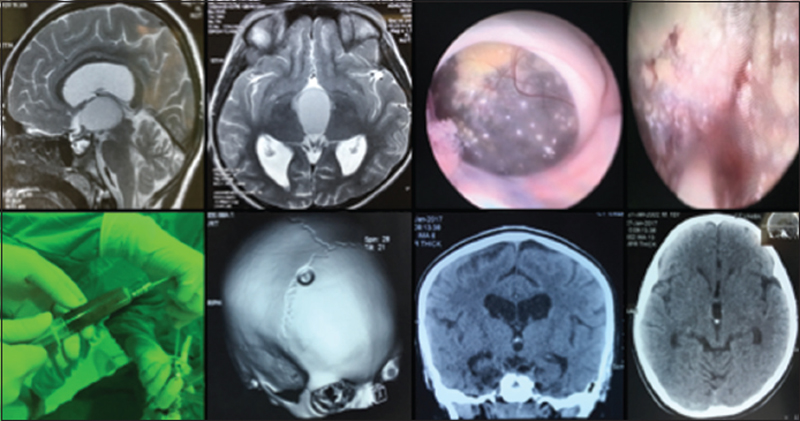
All cases in this study had undergone neuroendoscopy by Karl Storz Lotta system 6° ventriculoscope of diameter 6.1 mm with a working channel diameter of 2.9 mm (KARL STORZ SE and Co. Tuttlingen/Germany). Patients were positioned supine and a linear incision was given at coronal suture. A small precoronal burr hole 3 cm from the midline and 1 cm anterior to coronal suture was made. Dura was opened either in a linear fashion or a C-shaped flap. The lateral ventricle was entered with obturator and working sheath. A freehand technique was used in all cases. The endoscope was introduced inside ventricle and cystic craniopharyngioma was visualized at Foramen Monro. The cyst wall was coagulated, fenestrated, and biopsy was taken from the wall. Dark green or machine oil colored fluid was aspirated from the cyst. Irrigation and suction of the cyst was done and inside of the cyst was visualized by the endoscope. Multiple calcified spots along with friable, suckable contents were usually seen and taken out. In five cases, floor of the third ventricle and interpeduncular cistern were well visualized though the cyst for performing cystocisternostomy, this procedure was termed as double fenestration (ventriculocystostomy and cystocisternostomy) [[Figure 1]]. Patients with significant hydrocephalus would also undergo endoscopic septostomy, followed by a ventriculoperitoneal shunt performed through Keen's point in the same sitting. A catheter was positioned in the cyst cavity under direct vision through the scope and was connected to the Ommaya reservoir placed at burr hole [[Figure 2]]. The skin was closed in two layers.

Postoperative management
The patients were administered antibiotics according to our institute protocol. Postoperative computed tomography (CT) scan was done to rule out any bleed and confirm the placement of Ommaya catheter. Anti-epileptics (phenytoin 5 mg/kg in divided doses) was given for 6 months if the patient remained seizure-free. In four patients, we witnessed seizures in the postoperative period for which the dosage of anti-epileptic drug was increased and no further episodes of seizures were reported.
Results
The age of the patients ranged from 3 years to 68 years (mean 16.28 ± 15.70). Seventy-five percent of patients were below 16 years of age. There were 23 male and 9 female patients. Headache was the most common presenting complaint, followed by the visual disturbance. Presenting symptoms are enumerated in [[Table 1]].

Investigations
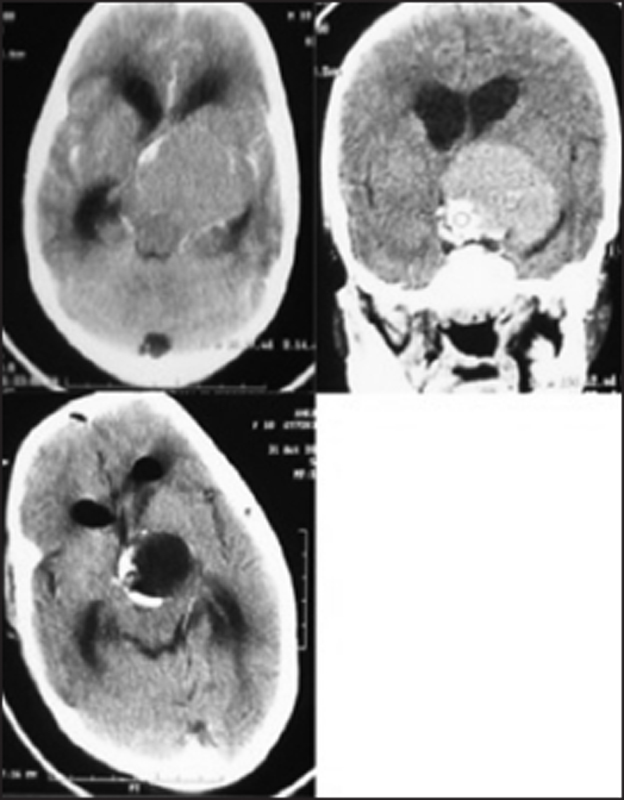
CT and magnetic resonance imaging scans were performed in all patients preoperatively. Fifty percent of the patients had hydrocephalus. All the patients had predominantly cystic craniopharyngioma with cyst diameter ranged from 3 cm to 8 cm (mean 4.5 cm). Calcification was seen in the wall of cyst in 70% of cases [[Table 2]].



Ophthalmological investigations showed papilledema in 53% (17/32) of patients which improved significantly after surgical intervention, whereas 40% (13/32) of patients had primary optic atrophy whose visual acuity status remained nearly same as preoperative or had only slight improvement.
Outcome
All 32 patients were treated by endoscopic fenestration of craniopharyngioma cyst along with a biopsy of cyst wall and complete drainage of cyst fluid. Ommaya reservoir was placed in all cases [[Figure 4]]. Twelve patients required a ventriculoperitoneal shunt and six patients among them also underwent septostomy who had significant hydrocephalus. In five patients, we were able to perform cystocisternostomy (double fenestration) [[Table 2]] and [[Figure 3]].

Headache improved in 92% (25/27) patients in whom headache was presenting symptom. Nausea, vomiting, and confusion improved in all patients.
External beam radiotherapy was given to all the patients. No patient developed any visual deterioration following radiotherapy. However, six patients showed clinical and radiological recurrence in the follow-up with requirement of multiple Ommaya aspirations, they were advised microsurgical intervention, but out of them, only two underwent transcranial surgical excision. The recurrence rate in the study was 18.75% (6/32). Remaining 26 patients (81%) had good tumor control on radiology, required no Ommaya aspirations and were doing well at follow-ups.
Complications
Burr-hole site skin infection was seen in one case which was treated successfully with antibiotics. Bacterial meningitis was seen in two cases (Case 1-Patient No. 9-both VP shunt and Ommaya reservoir with catheter were removed and intravenous antibiotics were given according to culture reports for 14 days, reinsertion of the shunt was done from a fresh site after CSF culture reports turned sterile). (Case 2-Patient No. 11-Ommaya reservoir with catheter was removed on the basis of positive culture reports and was treated with intravenous antibiotics). One case each of intraventricular hemorrhage and subdural collection was managed on conservative lines and fared well. Burr hole site extradural hemorrhage was seen in 1 case and was evacuated. CSF leak seen in two cases was due to shunt malfunction, which subsided on shunt revision. Shunt complications were treated by reinserting fresh shunts from the changed side [[Table 3]].

Mortality
Three patients expired in the follow-up. The exact cause of death could not be ascertained but telephonic conversation linked them to seizures due to poor compliance with anti-epileptics.
Follow-up
The patients were regularly followed up clinically and radiographically. CT scan was initially done at 3 months thereafter at 6 months and then at yearly interval. The mean follow-up was 22.7 ± 15.8 months (3–76 months) [[Table 2]].
Discussion
Craniopharyngiomas are commonly seen in two age groups (5–15 years) and (60–70 years).[[1]],[[5]],[[13]],[[14]] Similar observation was seen in our series. Majority of the patients were of pediatric age group.[[1]],[[5]],[[13]],[[14]] The mean age of the patients in this study was 16.28 ± 15.70 which is close to the reported mean age in other series.[[1]],[[5]],[[13]],[[14]] The clinical profile of patients in this series was similar to previously reported other series. Features of raised intracranial pressure and visual disturbance were commonly seen.[[5]],[[10]],[[13]],[[14]]
Gross total removal of cystic craniopharyngioma is considered as the gold standard treatment, but this procedure is plagued with significant morbidity and mortality following damage to the hypothalamus, optic apparatus, and stalk.[[1]],[[5]] To avoid the torrid postoperative course, surgical resection of cystic craniopharyngioma has largely been replaced by cyst fenestration and drainage, and it has become one of the commonly performed procedures for predominantly cystic craniopharyngioma.[[11]],[[12]],[[15]] Over the years, cyst fenestration along with Ommaya placement has evolved as a less invasive and more accurate surgical procedure, while it was initially performed percutaneously, or ultrasound-guided, but lately with endoscopy, it has led to better visualization of tumor cavity, accurate placement of catheter, as well as minimal damage to the hypothalamus or optic apparatus.[[3]],[[4]],[[9]],[[6]],[[16]],[[14]],[[17]] Rachinger et al. in their series concluded that cystic fenestration is as effective as microsurgery with less hypothalamic damage.[[18]] The present study further reiterates the above fact.
Lauretti et al. analyzed and stated the superiority of neuroendoscopy over stereotactic cyst aspiration as well as cyst CSF communication as a protective factor for recurrence.[[19]] In our series, patients had a collapse of cyst after cyst fenestration and widening of the cyst opening along with aspiration. Ommaya catheter holes had communication with both craniopharyngioma cyst and ventricle CSF. Patency of cyst and ventricle communication due to widening of fenestration and catheter holes both in cyst and ventricle is the probable reason which is believed to be the cause of no recollection in these patients. The same explanation was mooted by Al-Abyad and El-Sheikh and Moussa et al. in their series on cystic craniopharyngioma.[[13]],[[19]],[[20]],[[21]] In some series, chemical meningitis subsequent to spillage of cyst contents “machine oil” was reported.[[22]],[[23]] No complication pertaining to the cyst-ventricle communication or spillage and absorption was seen in this study and none were reported by the other series.[[7]],[[13]],[[20]],[[24]] The careful fenestration and aspiration of the cyst helps in avoiding the spillage of cyst contents into the ventricle thus minimizing chances of chemical meningitis. It was not seen in this study and has been rarely reported.[[13]],[[20]] No intracavitary treatment with bleomycin or interferon alpha was used in the present study. There are no conclusive results described in the literature supporting the use of intracavitary chemotherapy.[[2]],[[3]],[[23]],[[25]],[[26]],[[27]]
Complications noted in the series were similar to any series with procedures related to endoscopic transcranial procedures and all were managed effectively.[[9]],[[28]],[[29]],[[30]],[[31]] They were far less as compared to those encountered in the resection procedures and surely had lower morbidity.[[1]],[[29]],[[32]],[[33]],[[34]]
Transventricular endoscopic management begets superior results as compared to microsurgical techniques in terms of less postsurgical morbidity and complications along with drastically improved patient's symptomatology. It is also better than other techniques of cyst drainage as it gives real-time direct visualization of the procedure and the catheter placement in the cavity.
Radiotherapy's role in craniopharyngioma is controversial, and currently, adjuvant radiotherapy is given in cases of residual tumors after resection to prevent relapse.[[35]],[[36]],[[37]] Though concerns regarding damage to optic apparatus and endocrinopathies as well as inducing malignant transformation have been raised.[[38]],[[39]],[[40]] Rachinger et al. recommended to withhold or postpone radiotherapy in majority of cystic craniopharyngioma.[[18]] Lauretti et al. suggested that radiotherapy can be avoided after cyst drainage and should be given for recurrent or progressive cases[[41]] but several other series have conclusively prescribed radiotherapy for progression-free survival in cystic craniopharyngioma [[Table 4]].[[20]],[[36]],[[37]],[[41]],[[42]] In the present study, external beam radiotherapy was given in all 32 patients with good tumor control in follow-up with only 18.7% (6/32) patients showing recurrence. Post radiotherapy, no visual deterioration was noted in the follow-up. Therefore, we suggest radiotherapy to be given as adjuvant therapy following neuroendoscopic fenestration and drainage.

Limitation of the study
This study has few limitations. First, this is a retrospective single-institution series which stands low on the pyramid of the level of evidence. Second, the sample size is not large enough even though it is the largest series on the cystic craniopharyngioma treated by neuroendoscopy.
Conclusions
Neuroendoscopic transcortical transventricular drainage of cystic craniopharyngioma is a simple, safe, and effective treatment and lacks many risks associated with microsurgery. Cyst ventricle communication in this procedure effectively prevents reaccumulation and Ommaya reservoir catheter further reinforces this communication. Radiotherapy is to be given as adjuvant modality following neuroendoscopic decompression. Consensus on ideal management of craniopharyngioma is still far from over therefore multi-institutional collaborative study involving all treatment modalities should be formulated for obtaining more relevant statistical information to come to a definite conclusion.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Barajas MA, Ramírez-Guzmán G, Rodríguez-Vázquez C, Toledo-Buenrostro V, Velásquez-Santana H, del Robles RV, et al. Multimodal management of craniopharyngiomas: Neuroendoscopy, microsurgery, and radiosurgery. J Neurosurg 2002;97 (5 Suppl):607-9.
- 2 Lafay-Cousin L, Bartels U, Raybaud C, Kulkarni AV, Guger S, Huang A, et al. Neuroradiological findings of bleomycin leakage in cystic craniopharyngioma. Report of three cases. J Neurosurg 2007;107 (4 Suppl):318-23.
- 3 Cáceres A. Intracavitary therapeutic options in the management of cystic craniopharyngioma. Childs Nerv Syst 2005;21:705-18.
- 4 Lunsford LD, Pollock BE, Kondziolka DS, Levine G, Flickinger JC. Stereotactic options in the management of craniopharyngioma. Pediatr Neurosurg 1994;21:90-7.
- 5 Yasargil MG, Curcic M, Kis M, Siegenthaler G, Teddy PJ, Roth P. Total removal of craniopharyngiomas. Approaches and long-term results in 144 patients. J Neurosurg. 1990;73:3-11.
- 6 Cinalli G, Spennato P, Cianciulli E, Fiorillo A, Di Maio S, Maggi G. The role of transventricular neuroendoscopy in the management of craniopharyngiomas: Three patient reports and review of the literature. J Pediatr Endocrinol Metab 2006;19 Suppl 1:341-54.
- 7 Kuramoto T, Uchikado H, Tajima Y, Tokutomi T, Shigemori M. Neuroendoscopic placement of the reservoir in an elderly patient with recurrenced craniopharyngioma: Case report. No Shinkei Geka 2005;33:1207-12.
- 8 Cappabianca P, Cinalli G, Gangemi M, Brunori A, Cavallo LM, de Divitiis E, et al. Application of neuroendoscopy to intraventricular lesions. Neurosurgery 2008;62 Suppl 2:575-97.
- 9 Nakahara Y, Koga H, Maeda K, Takagi M, Tabuchi K. Neuroendoscopic transventricular surgery for suprasellar cystic mass lesions such as cystic craniopharyngioma and Rathke cleft cyst. Neurol Med Chir (Tokyo) 2004;44:408-13.
- 10 DiPatri AJ Jr., Prabhu V. A history of the treatment of craniopharyngiomas. Childs Nerv Syst 2005;21:606-21.
- 11 Joki T, Oi S, Babapour B, Kaito N, Ohashi K, Ebara M, et al. Neuroendoscopic placement of Ommaya reservoir into a cystic craniopharyngioma. Childs Nerv Syst 2002;18:629-33.
- 12 Nakamizo A, Inamura T, Nishio S, Inoha S, Ishibashi H, Fukui M. Neuroendoscopic treatment of cystic craniopharyngioma in the third ventricle. Minim Invasive Neurosurg 2001;44:85-7.
- 13 Moussa Moussa AH, Kerasha AA, Mahmoud ME. Surprising outcome of ommaya reservoir in treating cystic craniopharyngioma: A retrospective study. Br J Neurosurg 2013;27:370-3.
- 14 Nicolato A, Foroni R, Rosta L, Gerosa M, Bricolo A. Multimodality stereotactic approach to the treatment of cystic craniopharyngiomas. Minim Invasive Neurosurg 2004;47:32-40.
- 15 Hellwig D, Bauer BL, List-Hellwig E. Stereotactic endoscopic interventions in cystic brain lesions. Acta Neurochir Suppl 1995;64:59-63.
- 16 Frank F, Fabrizi AP, Frank G, Fioravanti A. Stereotactic management of craniopharyngiomas. Stereotact Funct Neurosurg 1995;65:176-83.
- 17 Gutin PH, Klemme WM, Lagger RL, MacKay AR, Pitts LH, Hosobuchi Y. Management of the unresectable cystic craniopharyngioma by aspiration through an Ommaya reservoir drainage system. J Neurosurg 1980;52:36-40.
- 18 Rachinger W, Oehlschlaegel F, Kunz M, Fuetsch M, Schichor C, Thurau S, et al. Cystic craniopharyngiomas: Microsurgical or stereotactic treatment? Neurosurgery 2017;80:733-43.
- 19 Lauretti L, Legninda Sop FY, Pallini R, Fernandez E, D'Alessandris QG. Neuroendoscopic treatment of cystic craniopharyngiomas: A case series with systematic review of the literature. World Neurosurg 2018;110:e367-73.
- 20 Al-Abyad A, El-Sheikh E. Management of grossly cystic craniopharyngioma by percutaneous aspiration and extermal beam irradiation. Egypt J Neurosurg 2006;21:123-37.
- 21 Shukla D. Transcortical Transventricular endoscopic approach and ommaya reservoir placement for cystic craniopharyngioma. Pediatr Neurosurg 2015;50:291-4.
- 22 Zanon N, Cavalheiro S, da Silva MC. Does the choice of surgical approach to insert an intratumoral catheter influence the results of intratumoral cystic treatment? Surg Neurol 2008;70:66-9.
- 23 Hader WJ, Steinbok P, Hukin J, Fryer C. Intratumoral therapy with bleomycin for cystic craniopharyngiomas in children. Pediatr Neurosurg 2000;33:211-8.
- 24 Fujimoto Y, Fujimoto Y, Kato A, Yoshimine T. Neuroendoscopic palliation for large cystic craniopharyngioma in an elderly patient. Br J Neurosurg 2007;21:618-21.
- 25 Mottolese C, Stan H, Hermier M, Berlier P, Convert J, Frappaz D, et al. Intracystic chemotherapy with bleomycin in the treatment of craniopharyngiomas. Childs Nerv Syst 2001;17:724-30.
- 26 Cavalheiro S, Dastoli PA, Silva NS, Toledo S, Lederman H, da Silva MC. Use of interferon alpha in intratumoral chemotherapy for cystic craniopharyngioma. Childs Nerv Syst 2005;21:719-24.
- 27 Savas A, Erdem A, Tun K, Kanpolat Y. Fatal toxic effect of bleomycin on brain tissue after intracystic chemotherapy for a craniopharyngioma: Case report. Neurosurgery 2000;46:213-6.
- 28 Delitala A, Brunori A, Chiappetta F. Purely neuroendoscopic transventricular management of cystic craniopharyngiomas. Childs Nerv Syst 2004;20:858-62.
- 29 Spaziante R, de Divitiis E, Irace C, Cappabianca P, Caputi F. Management of primary or recurring grossly cystic craniopharyngiomas by means of draining systems. Topic review and 6 case reports. Acta Neurochir (Wien) 1989;97:95-106.
- 30 Tamburrini G, D'Angelo L, Paternoster G, Massimi L, Cal-Darelli M, Di Rocco C. Endoscopic management of intra and paraventricular CSF cysts. Childs Nerv Syst 2007;23:645-52.
- 31 Gaab MR, Schroeder HW. Neuroendoscopic approach to intraventricular lesions. J Neurosurg 1998;88:496-505.
- 32 Tirakotai W, Hellwig D, Bertalanffy H, Riegel T. The role of neuroendoscopy in the management of solid or solid-cystic intra- and periventricular tumours. Childs Nerv Syst 2007;23:653-8.
- 33 Kirollos RW, Javadpour M, May P, Mallucci C. Endoscopic treatment of suprasellar and third ventricle-related arachnoid cysts. Childs Nerv Syst 2001;17:713-8.
- 34 Schubert T, Trippel M, Tacke U, van Velthoven V, Gumpp V, Bartelt S, et al. Neurosurgical treatment strategies in childhood craniopharyngiomas: is less more? Childs Nerv Syst 2009;25:1419-27.
- 35 Signorelli F, D'Alessandris QG, Maira G, Pallini R, Lauretti L. Letter: Malignant craniopharyngioma and radiotherapy: The missing link. Neurosurgery. 2015;76:E358-9.
- 36 Greenfield BJ, Okcu MF, Baxter PA, Chintagumpala M, Teh BS, Dauser RC, et al. Long-term disease control and toxicity outcomes following surgery and intensity modulated radiation therapy (IMRT) in pediatric craniopharyngioma. Radiother Oncol 2015;114:224-9.
- 37 Lee CC, Yang HC, Chen CJ, Hung YC, Wu HM, Shiau CY, et al. Gamma knife surgery for craniopharyngioma: Report on a 20-year experience. J Neurosurg 2014;121 Suppl: 167-78.
- 38 D'Alessandris QG, Signorelli F, Lauretti L. In reply: Radiation-induced malignant transformation of craniopharyngiomas. Neurosurgery 2016;79:E316.
- 39 Beer-Furlan A, Abi-Hachem R, Goksel B, Otero JJ, Carrau RL, Prevedello DM. Letter: radiation-induced malignant transformation of craniopharyngiomas. Neurosurgery 2016;79:E313-5.
- 40 Sofela AA, Hettige S, Curran O, Bassi S. Malignant transformation in craniopharyngiomas. Neurosurgery. 2014;705:306-14.
- 41 Schoenfeld A, Pekmezci M, Barnes MJ, Tihan T, Gupta N, Lamborn KR, et al. The superiority of conservative resection and adjuvant radiation for craniopharyngiomas. J Neurooncol 2012;108:133-9.
- 42 Takano S, Akutsu H, Mizumoto M, Yamamoto T, Tsuboi K, Matsumura A. Neuroendoscopy followed by radiotherapy in cystic craniopharyngiomas-a long-term follow-up. World Neurosurg 2015;84:1305-15.
Address for correspondence
Publication History
Received: 24 May 2020
Accepted: 26 August 2020
Article published online:
16 August 2022
© 2020. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Barajas MA, Ramírez-Guzmán G, Rodríguez-Vázquez C, Toledo-Buenrostro V, Velásquez-Santana H, del Robles RV, et al. Multimodal management of craniopharyngiomas: Neuroendoscopy, microsurgery, and radiosurgery. J Neurosurg 2002;97 (5 Suppl):607-9.
- 2 Lafay-Cousin L, Bartels U, Raybaud C, Kulkarni AV, Guger S, Huang A, et al. Neuroradiological findings of bleomycin leakage in cystic craniopharyngioma. Report of three cases. J Neurosurg 2007;107 (4 Suppl):318-23.
- 3 Cáceres A. Intracavitary therapeutic options in the management of cystic craniopharyngioma. Childs Nerv Syst 2005;21:705-18.
- 4 Lunsford LD, Pollock BE, Kondziolka DS, Levine G, Flickinger JC. Stereotactic options in the management of craniopharyngioma. Pediatr Neurosurg 1994;21:90-7.
- 5 Yasargil MG, Curcic M, Kis M, Siegenthaler G, Teddy PJ, Roth P. Total removal of craniopharyngiomas. Approaches and long-term results in 144 patients. J Neurosurg. 1990;73:3-11.
- 6 Cinalli G, Spennato P, Cianciulli E, Fiorillo A, Di Maio S, Maggi G. The role of transventricular neuroendoscopy in the management of craniopharyngiomas: Three patient reports and review of the literature. J Pediatr Endocrinol Metab 2006;19 Suppl 1:341-54.
- 7 Kuramoto T, Uchikado H, Tajima Y, Tokutomi T, Shigemori M. Neuroendoscopic placement of the reservoir in an elderly patient with recurrenced craniopharyngioma: Case report. No Shinkei Geka 2005;33:1207-12.
- 8 Cappabianca P, Cinalli G, Gangemi M, Brunori A, Cavallo LM, de Divitiis E, et al. Application of neuroendoscopy to intraventricular lesions. Neurosurgery 2008;62 Suppl 2:575-97.
- 9 Nakahara Y, Koga H, Maeda K, Takagi M, Tabuchi K. Neuroendoscopic transventricular surgery for suprasellar cystic mass lesions such as cystic craniopharyngioma and Rathke cleft cyst. Neurol Med Chir (Tokyo) 2004;44:408-13.
- 10 DiPatri AJ Jr., Prabhu V. A history of the treatment of craniopharyngiomas. Childs Nerv Syst 2005;21:606-21.
- 11 Joki T, Oi S, Babapour B, Kaito N, Ohashi K, Ebara M, et al. Neuroendoscopic placement of Ommaya reservoir into a cystic craniopharyngioma. Childs Nerv Syst 2002;18:629-33.
- 12 Nakamizo A, Inamura T, Nishio S, Inoha S, Ishibashi H, Fukui M. Neuroendoscopic treatment of cystic craniopharyngioma in the third ventricle. Minim Invasive Neurosurg 2001;44:85-7.
- 13 Moussa Moussa AH, Kerasha AA, Mahmoud ME. Surprising outcome of ommaya reservoir in treating cystic craniopharyngioma: A retrospective study. Br J Neurosurg 2013;27:370-3.
- 14 Nicolato A, Foroni R, Rosta L, Gerosa M, Bricolo A. Multimodality stereotactic approach to the treatment of cystic craniopharyngiomas. Minim Invasive Neurosurg 2004;47:32-40.
- 15 Hellwig D, Bauer BL, List-Hellwig E. Stereotactic endoscopic interventions in cystic brain lesions. Acta Neurochir Suppl 1995;64:59-63.
- 16 Frank F, Fabrizi AP, Frank G, Fioravanti A. Stereotactic management of craniopharyngiomas. Stereotact Funct Neurosurg 1995;65:176-83.
- 17 Gutin PH, Klemme WM, Lagger RL, MacKay AR, Pitts LH, Hosobuchi Y. Management of the unresectable cystic craniopharyngioma by aspiration through an Ommaya reservoir drainage system. J Neurosurg 1980;52:36-40.
- 18 Rachinger W, Oehlschlaegel F, Kunz M, Fuetsch M, Schichor C, Thurau S, et al. Cystic craniopharyngiomas: Microsurgical or stereotactic treatment? Neurosurgery 2017;80:733-43.
- 19 Lauretti L, Legninda Sop FY, Pallini R, Fernandez E, D'Alessandris QG. Neuroendoscopic treatment of cystic craniopharyngiomas: A case series with systematic review of the literature. World Neurosurg 2018;110:e367-73.
- 20 Al-Abyad A, El-Sheikh E. Management of grossly cystic craniopharyngioma by percutaneous aspiration and extermal beam irradiation. Egypt J Neurosurg 2006;21:123-37.
- 21 Shukla D. Transcortical Transventricular endoscopic approach and ommaya reservoir placement for cystic craniopharyngioma. Pediatr Neurosurg 2015;50:291-4.
- 22 Zanon N, Cavalheiro S, da Silva MC. Does the choice of surgical approach to insert an intratumoral catheter influence the results of intratumoral cystic treatment? Surg Neurol 2008;70:66-9.
- 23 Hader WJ, Steinbok P, Hukin J, Fryer C. Intratumoral therapy with bleomycin for cystic craniopharyngiomas in children. Pediatr Neurosurg 2000;33:211-8.
- 24 Fujimoto Y, Fujimoto Y, Kato A, Yoshimine T. Neuroendoscopic palliation for large cystic craniopharyngioma in an elderly patient. Br J Neurosurg 2007;21:618-21.
- 25 Mottolese C, Stan H, Hermier M, Berlier P, Convert J, Frappaz D, et al. Intracystic chemotherapy with bleomycin in the treatment of craniopharyngiomas. Childs Nerv Syst 2001;17:724-30.
- 26 Cavalheiro S, Dastoli PA, Silva NS, Toledo S, Lederman H, da Silva MC. Use of interferon alpha in intratumoral chemotherapy for cystic craniopharyngioma. Childs Nerv Syst 2005;21:719-24.
- 27 Savas A, Erdem A, Tun K, Kanpolat Y. Fatal toxic effect of bleomycin on brain tissue after intracystic chemotherapy for a craniopharyngioma: Case report. Neurosurgery 2000;46:213-6.
- 28 Delitala A, Brunori A, Chiappetta F. Purely neuroendoscopic transventricular management of cystic craniopharyngiomas. Childs Nerv Syst 2004;20:858-62.
- 29 Spaziante R, de Divitiis E, Irace C, Cappabianca P, Caputi F. Management of primary or recurring grossly cystic craniopharyngiomas by means of draining systems. Topic review and 6 case reports. Acta Neurochir (Wien) 1989;97:95-106.
- 30 Tamburrini G, D'Angelo L, Paternoster G, Massimi L, Cal-Darelli M, Di Rocco C. Endoscopic management of intra and paraventricular CSF cysts. Childs Nerv Syst 2007;23:645-52.
- 31 Gaab MR, Schroeder HW. Neuroendoscopic approach to intraventricular lesions. J Neurosurg 1998;88:496-505.
- 32 Tirakotai W, Hellwig D, Bertalanffy H, Riegel T. The role of neuroendoscopy in the management of solid or solid-cystic intra- and periventricular tumours. Childs Nerv Syst 2007;23:653-8.
- 33 Kirollos RW, Javadpour M, May P, Mallucci C. Endoscopic treatment of suprasellar and third ventricle-related arachnoid cysts. Childs Nerv Syst 2001;17:713-8.
- 34 Schubert T, Trippel M, Tacke U, van Velthoven V, Gumpp V, Bartelt S, et al. Neurosurgical treatment strategies in childhood craniopharyngiomas: is less more? Childs Nerv Syst 2009;25:1419-27.
- 35 Signorelli F, D'Alessandris QG, Maira G, Pallini R, Lauretti L. Letter: Malignant craniopharyngioma and radiotherapy: The missing link. Neurosurgery. 2015;76:E358-9.
- 36 Greenfield BJ, Okcu MF, Baxter PA, Chintagumpala M, Teh BS, Dauser RC, et al. Long-term disease control and toxicity outcomes following surgery and intensity modulated radiation therapy (IMRT) in pediatric craniopharyngioma. Radiother Oncol 2015;114:224-9.
- 37 Lee CC, Yang HC, Chen CJ, Hung YC, Wu HM, Shiau CY, et al. Gamma knife surgery for craniopharyngioma: Report on a 20-year experience. J Neurosurg 2014;121 Suppl: 167-78.
- 38 D'Alessandris QG, Signorelli F, Lauretti L. In reply: Radiation-induced malignant transformation of craniopharyngiomas. Neurosurgery 2016;79:E316.
- 39 Beer-Furlan A, Abi-Hachem R, Goksel B, Otero JJ, Carrau RL, Prevedello DM. Letter: radiation-induced malignant transformation of craniopharyngiomas. Neurosurgery 2016;79:E313-5.
- 40 Sofela AA, Hettige S, Curran O, Bassi S. Malignant transformation in craniopharyngiomas. Neurosurgery. 2014;705:306-14.
- 41 Schoenfeld A, Pekmezci M, Barnes MJ, Tihan T, Gupta N, Lamborn KR, et al. The superiority of conservative resection and adjuvant radiation for craniopharyngiomas. J Neurooncol 2012;108:133-9.
- 42 Takano S, Akutsu H, Mizumoto M, Yamamoto T, Tsuboi K, Matsumura A. Neuroendoscopy followed by radiotherapy in cystic craniopharyngiomas-a long-term follow-up. World Neurosurg 2015;84:1305-15.