

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_289_18
The role of decompressive craniectomy in traumatic brain injury: A systematic review and meta-analysis
Authors

The objective is to evaluate the efficacy of early decompressive craniectomy (DC) versus standard medical management ± late DC in improving clinical outcome in patients with traumatic brain injury (TBI). Electronic databases and gray literature (unpublished articles) were searched under different MeSH terms from 1990 to present. Randomized control trials, case–control studies, and prospective cohort studies on DC in moderate and severe TBI. Clinical outcome measures included Glasgow Coma Outcome Scale (GCOS) and extended GCOS, and mortality. Data were extracted to Review Manager software. A total of 45 articles and abstracts that met the inclusion criteria were retrieved and analyzed. Ultimately, seven studies were included in our meta-analysis, which revealed that patients who had early DC had no statistically significant likelihood of having a favorable outcome at 6 months than those who had a standard medical care alone or with late DC (OR of favorable clinical outcome at 6 months: 1.00; 95% confidence interval (CI): 0.75–1.34; P = 0.99). The relative risk (RR) of mortality in early DC versus the standard medical care ± late DC at discharge or 6 months is 0.62; 95% CI: 0.40–0.94; P = 0.03. Subgroup analysis based on RR of mortality shows that the rate of mortality is reduced significantly in the early DC group as compared to the late DC. RR of Mortality is 0.43; 95% CI: 0.26–0.71; P = 0.0009. However, good clinical outcome is the same. Early DC saves lives in patients with TBI. However, further clinical trials are required to prove if early DC improve clinical outcome and to define the best early time frame in performing early DC in TBI population.
Introduction
Cerebral edema remains one of the main complications of traumatic brain injury (TBI) that lead to increase in intracranial pressure (ICP) and reduction in the cerebral perfusion pressure (CPP).[[1]] This would successively cause detrimental effects on the cerebral oxygen metabolism and can lead to catastrophic events.[[2]],[[3]],[[4]],[[5]] In TBI, the cerebral contusion induces the life-threatening brain swelling within the first 2–3 h. The second peak of the brain swelling occurs within 2–5 days due to blood cell breakdown products and activated inflammatory cascades.[[6]],[[7]],[[8]]
As per the European Brain Injury Consortium and the American Brain Injury Consortium guidelines for severe TBI, decompressive craniectomy (DC) is one of the therapeutic options when conventional treatment fails to reduce the ICP, which involves; head elevation, sedation, analgesia, and neuromuscular paralysis.[[9]],[[10]],[[11]],[[12]],[[13]],[[14]],[[15]],[[16]],[[17]] Other treatment options for treating brain edema includes ventriculostomy (if an external ventricular drain had not already been inserted for ICP monitoring), pharmacologic blood-pressure augmentation, osmotherapy, moderate hypocapnia (PaCO2, 4.0–4.5 kPa [30–34 mmHg]), and therapeutic hypothermia (not <34°C).[[18]]
DC is a surgical technique designed to provide instantaneous and definitive relief of elevated ICP, especially when there is either unilateral or bilateral diffuse cerebral swelling, neurological deficit, dilated and unreactive pupils, failure of medical treatment with persistent ICP >30 mmHg and CPP <45 mmHg.[[9]],[[10]],[[18]],[[19]] Although some regard it as a last-ditch effort only to be used when more conservative ICP treatment measures have failed as mentioned above. Evidence suggests that early DC may play an optimal care of patients with elevated ICP.[[20]],[[21]],[[22]]
Based on that, an urgent DC can be a life-saving procedure by providing the room for the brain to swell, thus reducing the ICP and maintaining the CPP. However, wait-and-see approach is mostly adopted before the craniectomy or craniotomy of lesions evacuation, with evidence of neurological decline or ICP elevation with or without failure of medical management.[[23]]
Thus, the timing of DC could be very crucial regarding the surgical outcome despite being still debatable to intervene early or late as a second-tier therapy after the initial trial of medical management has failed.
In most of the cases, DC is performed following the protocol of medical treatment of refractory intracranial edema and hypertension as a secondary procedure (secondary DC).[[2]],[[8]] The timing of the DC (early vs. late) plays an important role as it may change the pathophysiological responses.[[7]],[[8]] It has been reported that the right time of DC can be determined by the clinical follow-up, repeated head computed tomography (CT) scans, and continuous ICP and CPP monitoring.[[9]],[[10]]
The safety and efficacy of DC as an early or late procedure, following the initial conservative management in TBI, has not been fully established due to limited randomized controlled trials (RCTs), looking at the timing of DC in predicting clinical outcome and the difficulty in performing these types of trials. Further studies are required to determine the timing of the DC surgery to improve the patient's clinical outcome.
Our meta-analysis is a further step to determine the efficacy of early DC versus the standard medical care ± late DC in improving the clinical outcome in TBI. Besides, to determine whether early DC versus late DC after failing the medical management of raised ICP has any role in improving the clinical outcome in TBI. Our a priori hypothesis was that early DC improves the clinical outcome of patients with moderate-to-severe TBI as compared to the standard medical care ± late DC.
Methods
Search strategy
We developed PICO question. Does the early DC versus the standard medical care ± late DC improves the clinical outcome in moderate-to-severe TBI? Based on that the following PICO question was obtained:
-
Population: Patients with moderate-to-severe TBI
-
Intervention: Early DC before the medical management
-
Control: Standard medical management ± late DC
-
Outcome: Extended Glasgow Coma Outcome Scale (GOS-E) at 6 months, GOS at 6 months.
Early or primary DC was defined as DC done at the time of mass lesion evacuation, and can be performed even without taking measures to reduce the ICP[[2]],[[8]] while late or secondary DC is defined as DC done to treat the refractory ICP, which according to some studies is >24–48 h.[[2]],[[8]]
The refractory ICP is defined as the raised ICP >25 mmHg that lasts for ≥15 min, which is not responding to the usual medical management.[[17]],[[24]] The intervention arm received early DC for the TBI. The control arm receives the standard medical care that involves; head elevation, sedation, analgesia, moderate hypothermia, osmotherapy (mannitol or hypertonic saline), and/or cerebrospinal fluid drainage alone or with the late DC.
We applied stringent inclusion criteria, selecting only RCTs, case–control studies (CCSs) or cohort studies (CS), and patients with moderate and severe with TBI who were candidates for DC and randomized to receive either early DC or standard medical care ± late DC. Case-series and retrospective studies were excluded.
We used the following MeSH headings: DC or ICP or TBI. We did not define any limitation in language. Articles published between 1990 and the present were searched. Two reviewers MS and NF completed all the review process.
The following databases were reviewed: the Cochrane Library, Medline, Embase, Web of Science, Google Scholar, Scopus, and PubMed. In addition, we reviewed the following gray literature: unpublished abstracts from the American and European Neurotrauma conferences over the past 10 years.
Data extraction and management
Demographic information, detailed methods, interventions, and outcomes were abstracted from the manuscripts chosen for the review and recorded on a special data form.
The data form included the following:
-
Methods: Design, method of randomization, setting of treatment, blindness of treatment or intervention (or not), withdrawals or patients lost to follow-up, type of analysis (intention to treat analysis), and primary and secondary outcomes
Population: Sample size, inclusion and exclusion criteria, age, gender, CT scan findings (based on the MARSHAL classification), time DC, time to medical management
-
Intervention: Early DC
-
Control: Standard medical management ± late DC
-
Outcome: Reported poor and good long- and short-term outcomes and mortality rate.
Outcome measures: several outcome measures were selected for our meta-analysis:
-
Functional outcomes: GOS-E 0–8: outcomes were dichotomized to favorable (5–8) or poor (1–4) from 6 months to 1 year
-
GOS at 6 months' favorable outcome (4–5) and unfavorable outcome (1–3)
-
Mortality defined as the number of deaths in a particular population per unit of time.
Assessment of risk of bias in included studies
To avoid publication bias, we reviewed the abstracts from the European and American TBI meetings, looking at unpublished trials.
Measures of treatment effect: Treatment efficacy was dichotomized as favorable or poor functional outcome
In order for the DC to be considered effective, we required the threshold between good and poor outcome to be clinically and statistically significant (P < 0.05).
Subgroup analysis and investigation of heterogeneity
The following subgroup analysis was performed:
-
Subgroup analysis based on the rate of mortality at discharge or at 6 months of early DC versus medical treatment ± followed by late DC
-
Subgroup analysis based on the rate of mortality at discharge or 6 months of early DC versus the late DC was carried out.
-
Subgroup analysis based on the early DC versus late DC leading to favorable and unfavorable outcome was carried out
-
The pooled meta-analysis was repeated with exclusion of the pediatric trial to measure the effect of early DC in the adult population with moderate-to-severe TBI.
Results
Description of studies
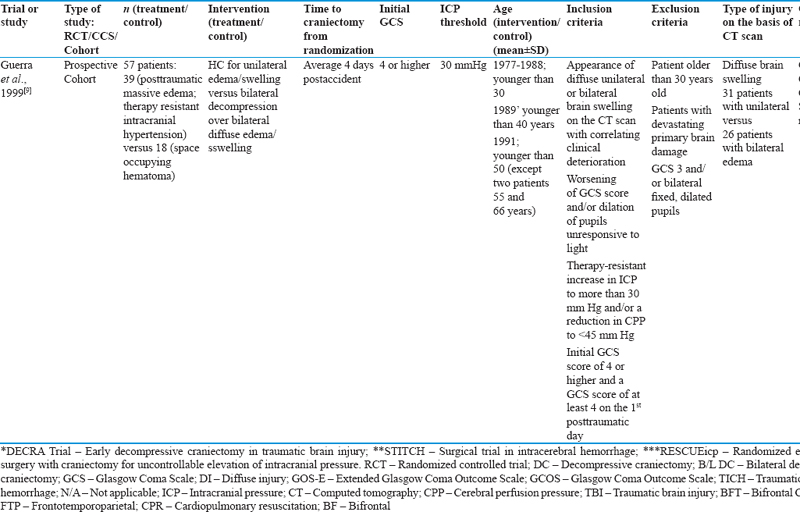
A total of 14,852 titles were reviewed from the above-mentioned electronic literature. Reviewing the gray literature did not add any abstracts. Forty-five studies were retrieved and analyzed. Seven studies (5 RCTs, 1 CCS, and 1 CS) met the inclusion criteria and included in our meta-analysis. The baseline characteristics and safety and efficacy of the RCTs, CCS, and prospective CS are summarized in [[Table 1]] and [[Table 2]].




Risk of bias in the randomized control trial studies
None of the RCT trials followed adequate sequence generation (computer generation), and few had the allocation of treatment concealed. Regarding blindness of the investigator and the patient outcome, none of the trials achieved double blindness; some of them achieved single investigator blindness. This is understandable in this type of RCT, in which the procedure is evaluated, and it could be difficult to blind the investigator or the patient to treatment allocation or immediate outcome measure.
Effects of interventions
The pooled meta-analysis of all seven studies (treatment arm 458 and control arm 406) revealed the following:
There is no statistically significant difference in the good clinical outcome at 6 months–1 year between early DC and medical treatment with or without late DC (Odds ratio [OR] of favorable clinical outcome at 6 months: 1.00; 95% confidence interval (CI): 0.75–1.34; P = 0.99). Hence, there does not exist any comparative difference in the clinical outcome between the intervention and the control arm as indicated in [[[Figure 1]] Panel A].

Six studies have reported the mortality rate in their results.[[17]],[[24]],[[25]],[[26]],[[27]],[[28]],[[29]] The RR of mortality at discharge or 6 months is 0.62; 95% CI: 0.40–0.94; P = 0.03. Hence, the mortality rate is reduced with the early DC as compared to the standard medical management ± late DC as showed in [[[Figure 1]] Panel B].
The outcome in the adult population after excluding the pediatric population in the first study[[28]] indicates that OR of favorable clinical outcome at 6 months: 0.94; 95% CI: 0.70–1.27; P = 0.70. The RR of mortality at discharge or 6 months is 0.59; 95% CI: 0.47–0.74; P < 0.00001.
Only three studies compared the early DC versus the late DC in TBI.[[9]],[[26]] There is no statistical significance difference in the good clinical outcome and unfavorable clinical outcome among those patients who had early DC versus late DC. The OR of good clinical outcome; 1.30; 95% CI: 0.75–2.27; P = 0.35 [[[Figure 2]] Panel A].

Regarding the mortality rate, it is reduced significantly in the early DC group as compared to the late DC group. RR of mortality rate in early DC versus late DC is 0.43; 95% CI: 0.26–0.71; P = 0.0009, [[[Figure 2]] Panel B].
Discussion
Our meta-analysis revealed that early DC and standard medical management whether alone or accompanied by late DC has almost the same effect on the functional clinical outcome of the patients with TBI. However, early DC reduces the mortality rate as compared to the patients who underwent late DC. However, because of several limitations in the studies mentioned above (lack of universal outcome scale, no double blindness in randomization, and clinical follow-up, and the small sample size in some studies), future double-blind, randomized control trial with large sample size is needed to prove the concept of early versus late DC. In addition, more evidence is required regarding the timing of the surgery in improving the clinical and functional outcome of patients with TBI.
The medical literature regarding early DC is very conflicting. There are several studies not in support of early DC. For example, Faleiro et al.[[30]] dichotomized 89 patients into <6 h, 6–24 h, and >24 h for DC and found that patients who were operated early had 59% mortality as compared to the 53% of patients who had the surgery later. Al-Jishi et al.[[31]] found that the primary DC had 45.5% good outcome and 40.9% mortality whereas, secondary DC had 73.1% good outcome and 15.4% mortality in his retrospective study. Albanèse et al.[[32]] found that patients who had primary decompression within 24 h had 20% good recovery and 50% died, while those who had secondary decompression (>24 h) had 38% good recovery and only 20% died. An early decompression was performed if the GCS was <6 with clinical signs of cerebral herniation (the absence of pupillary reflexes); ICP was not measured in these patients. The late decompression was performed if patients had intractable intracranial hypertension of >35 mmHg, unilateral or bilateral absence of pupillary reflex with abnormal CT head findings. However, he recommended performing early surgery in patients with intracranial hematoma and brain swelling, which eventually will improve the clinical outcome.
On the other hand, there are some literatures in support of early DC in improving outcome. For example, Honeybul et al.[[33]] carried out a cohort of 186 patients who required DC for severe TBI (2004–2010) indicated that none of the patients improved to achieve a level of independence or moderate disability, many did appear to have adapted to their disability and recalibrated their expectations for quality of life to a level of disability that they have previously thought unacceptable. Hartings et al.[[8]] compared the neurosurgical approaches in the treatment of TBI at two academic centers in the Cooperative Studies on Brain Injury Depolarizations at Kings College Hospital (KCH, n = 27) and Virginia Commonwealth University (VCU, n = 24) from July 2004 to March 2010. He found that patients treated at VCU underwent surgery earlier, had larger bone flaps, and more frequently underwent craniectomy than craniotomy. These differences were particularly accentuated in patients undergoing earlier lesion evacuation and corresponded to significantly lower postoperative ICP values, less spreading depolarizations, and better outcome (good outcome in 69% vs. 29% of cases). As by Seelig et al.,[[29]] if the surgery could be performed within 4 h, the mortality is only 30%, whereas if the surgery is performed over the 4 h, then the rate of mortality increases over 90%. Akyuz et al.[[34]] noted that the 40 patients who had early decompressive surgery as first tiers had much more portion of a better outcome than the other 36 patients operated as second tier (44.4% vs. 12.5%, P = 0.0018).
From the first glance at our meta-analysis result, one might conclude that there is no benefit from early DC in TBI patients. However, the intervention if carried out at an early stage is associated with decrease in the mortality rate. Our meta-analysis finding might be explained by being underpowered to show clinical benefit, and further trials are needed with larger sample size to evaluate the efficacy of early or primary DC versus the late or secondary DC in moderate-to-severe TBI.
Our study has several limitations. First, there is the possibility of selection and publication bias in our systematic review since only two reviewers carried out this part of the process. The reviewers might therefore be more influenced by the positive trial results than by the negative ones. However, we tried to limit such bias by doing the following steps: a gray literature review, in which, we reviewed the abstracts from several meetings to capture any RCT that was presented as an abstract but not published because of a negative result. Second, the lack of access to individual patient's data is one of the limitations. Third, there is a lack of same use of outcome scale among all the studies as some used GCOS while other used Extended Glasgow Coma Scale. Finally, our meta-analysis results cannot be generalized to all forms of decompressive craniectomies as there exists the difference between the thresholds of ICP as well as the timing of DC; thus, the intervention in the form of DC is dependent on it.
In conclusion, our data point that early DC saves life. However, there is no clinically significant relationship in the favorable and unfavorable clinical outcome between the two groups. Thus, our meta-analysis provides a basis to design the RCT with less bias, and determine the sample size of Phase-2 randomized trial of early versus late DC in patients with moderate-to-severe TBI.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Ghajar J. Traumatic brain injury. Lancet 2000;356:923-9.
- 2 Gong J, Wen L, Zhan R, Zhou HJ, Wang F, Liu G, et al. Early decompressing craniectomy in patients with traumatic brain injury and cerebral edema. Asian Biomed 2014;8:53-9.
- 3 Wardlaw JM, Easton VJ, Statham P. Which CT features help predict outcome after head injury? J Neurol Neurosurg Psychiatry 2002;72:188-92.
- 4 Treggiari MM, Schutz N, Yanez ND, Romand JA. Role of intracranial pressure values and patterns in predicting outcome in traumatic brain injury: A systematic review. Neurocrit Care 2007;6:104-12.
- 5 Huang SJ, Hong WC, Han YY, Chen YS, Wen CS, Tsan YS, et al. Clinical outcome of severe head injury in different protocol-driven therapies. J Clin Neurosci 2007;14:449-54.
- 6 Das S, Alam MJ, Islam KM, Elahi F, Mahmud E. Decompressive craniectomy in severe traumatic brain injury – A study of 20 cases. Bangladesh Med J 2014;43:2.
- 7 Timofeev I, Kirkpatrick PJ, Corteen E, Hiler M, Czosnyka M, Menon DK, et al. Decompressive craniectomy in traumatic brain injury: Outcome following protocol-driven therapy. Acta Neurochir Suppl 2006;96:11-6.
- 8 Hartings JA, Vidgeon S, Strong AJ, Zacko C, Vagal A, Andaluz N, et al. Surgical management of traumatic brain injury: A comparative-effectiveness study of 2 centers. J Neurosurg 2014;120:434-46.
- 9 Guerra WK, Gaab MR, Dietz H, Mueller JU, Piek J, Fritsch MJ, et al. Surgical decompression for traumatic brain swelling: Indications and results. J Neurosurg 1999;90:187-96.
- 10 Maas AI, Dearden M, Teasdale GM, Braakman R, Cohadon F, Iannotti F, et al. EBIC-guidelines for management of severe head injury in adults. European brain injury consortium. Acta Neurochir (Wien) 1997;139:286-94.
- 11 Marmarou A. Conduct of head injury trials in the United States: The American brain injury consortium (ABIC). Acta Neurochir Suppl 1996;66:118-21.
- 12 Diringer MN, Videen TO, Yundt K, Zazulia AR, Aiyagari V, Dacey RG Jr., et al. Regional cerebrovascular and metabolic effects of hyperventilation after severe traumatic brain injury. J Neurosurg 2002;96:103-8.
- 13 Doerfler A, Forsting M, Reith W, Staff C, Heiland S, Schäbitz WR, et al. Decompressive craniectomy in a rat model of “malignant” cerebral hemispheric stroke: Experimental support for an aggressive therapeutic approach. J Neurosurg 1996;85:853-9.
- 14 Marshall LF. Head injury: Recent past, present, and future. Neurosurgery 2000;47:546-61.
- 15 Oertel M, Kelly DF, Lee JH, McArthur DL, Glenn TC, Vespa P, et al. Efficacy of hyperventilation, blood pressure elevation, and metabolic suppression therapy in controlling intracranial pressure after head injury. J Neurosurg 2002;97:1045-53.
- 16 Piek J. Decompressive surgery in the treatment of traumatic brain injury. Curr Opin Crit Care 2002;8:134-8.
- 17 Hutchinson PJ, Kolias AG, Timofeev IS, Corteen EA, Czosnyka M, Timothy J, et al. Trial of decompressive craniectomy for traumatic intracranial hypertension. N Engl J Med 2016;375:1119-30.
- 18 Coplin WM, Cullen NK, Policherla PN, Vinas FC, Wilseck JM, Zafonte RD, et al. Safety and feasibility of craniectomy with duraplasty as the initial surgical intervention for severe traumatic brain injury. J Trauma 2001;50:1050-9.
- 19 Münch E, Horn P, Schürer L, Piepgras A, Paul T, Schmiedek P. Management of severe traumatic brain injury by decompressive craniectomy. Neurosurgery 2000;47:315-23.
- 20 Bor-Seng-Shu E, Figueiredo EG, Amorim RL, Teixeira MJ, Valbuza JS, de Oliveira MM, et al. Decompressive craniectomy: A meta-analysis of influences on intracranial pressure and cerebral perfusion pressure in the treatment of traumatic brain injury. J Neurosurg 2012;117:589-96.
- 21 Dennis MS, Burn JP, Sandercock PA, Bamford JM, Wade DT, Warlow CP, et al. Long-term survival after first-ever stroke: The oxfordshire community stroke project. Stroke 1993;24:796-800.
- 22 Göksu E, Uçar T, Akyüz M, Yılmaz M, Kazan S. Effects of decompressive surgery in patients with severe traumatic brain injury and bilateral non-reactive dilated pupils. Ulus Travma Acil Cerrahi Derg 2012;18:231-8.
- 23 Heuts SG, Bruce SS, Zacharia BE, Hickman ZL, Kellner CP, Sussman ES, et al. Decompressive hemicraniectomy without clot evacuation in dominant-sided intracerebral hemorrhage with ICP crisis. Neurosurg Focus 2013;34:E4.
- 24 Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, D'Urso P, et al. Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med 2011;364:1493-502.
- 25 Wettervik TS, Lenell S, Nyholm L, Howells T, Lewén A, Enblad P, et al. Decompressive craniectomy in traumatic brain injury: Usage and clinical outcome in a single centre. Acta Neurochir (Wien) 2018;160:229-37.
- 26 Mendelow AD, Gregson BA, Rowan EN, Francis R, McColl E, McNamee P, et al. Early surgery versus initial conservative treatment in patients with traumatic intracerebral hemorrhage (STITCH[Trauma]): The first randomized trial. J Neurotrauma 2015;32:1312-23.
- 27 Rubiano AM, Villarreal W, Hakim EJ, Aristizabal J, Hakim F, Dìez JC, et al. Early decompressive craniectomy for neurotrauma: An institutional experience. Ulus Travma Acil Cerrahi Derg 2009;15:28-38.
- 28 Taylor A, Butt W, Rosenfeld J, Shann F, Ditchfield M, Lewis E, et al. Arandomized trial of very early decompressive craniectomy in children with traumatic brain injury and sustained intracranial hypertension. Childs Nerv Syst 2001;17:154-62.
- 29 Seelig JM, Becker DP, Miller JD, Greenberg RP, Ward JD, Choi SC, et al. Traumatic acute subdural hematoma: Major mortality reduction in comatose patients treated within four hours. N Engl J Med 1981;304:1511-8.
- 30 Faleiro RM, Faleiro LC, Caetano E, Gomide I, Pita C, Coelho G, et al. Decompressive craniotomy: Prognostic factors and complications in 89 patients. Arq Neuropsiquiatr 2008;66:369-73.
- 31 Al-Jishi A, Saluja RS, Al-Jehani H, Lamoureux J, Maleki M, Marcoux J, et al. Primary or secondary decompressive craniectomy: Different indication and outcome. Can J Neurol Sci 2011;38:612-20.
- 32 Albanèse J, Leone M, Alliez JR, Kaya JM, Antonini F, Alliez B, et al. Decompressive craniectomy for severe traumatic brain injury: Evaluation of the effects at one year. Crit Care Med 2003;31:2535-8.
- 33 Honeybul S, Ho KM, Lind CR, Gillett GR. Validation of the CRASH model in the prediction of 18-month mortality and unfavorable outcome in severe traumatic brain injury requiring decompressive craniectomy. J Neurosurg 2014;120:1131-7.
- 34 Akyuz M, Ucar T, Acikbas C, Kazan S, Yilmaz M, Tuncer R, et al. Effect of early bilateral decompressive craniectomy on outcome for severe traumatic brain injury. Turk Neurosurg 2010;20:382-9.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Ghajar J. Traumatic brain injury. Lancet 2000;356:923-9.
- 2 Gong J, Wen L, Zhan R, Zhou HJ, Wang F, Liu G, et al. Early decompressing craniectomy in patients with traumatic brain injury and cerebral edema. Asian Biomed 2014;8:53-9.
- 3 Wardlaw JM, Easton VJ, Statham P. Which CT features help predict outcome after head injury? J Neurol Neurosurg Psychiatry 2002;72:188-92.
- 4 Treggiari MM, Schutz N, Yanez ND, Romand JA. Role of intracranial pressure values and patterns in predicting outcome in traumatic brain injury: A systematic review. Neurocrit Care 2007;6:104-12.
- 5 Huang SJ, Hong WC, Han YY, Chen YS, Wen CS, Tsan YS, et al. Clinical outcome of severe head injury in different protocol-driven therapies. J Clin Neurosci 2007;14:449-54.
- 6 Das S, Alam MJ, Islam KM, Elahi F, Mahmud E. Decompressive craniectomy in severe traumatic brain injury – A study of 20 cases. Bangladesh Med J 2014;43:2.
- 7 Timofeev I, Kirkpatrick PJ, Corteen E, Hiler M, Czosnyka M, Menon DK, et al. Decompressive craniectomy in traumatic brain injury: Outcome following protocol-driven therapy. Acta Neurochir Suppl 2006;96:11-6.
- 8 Hartings JA, Vidgeon S, Strong AJ, Zacko C, Vagal A, Andaluz N, et al. Surgical management of traumatic brain injury: A comparative-effectiveness study of 2 centers. J Neurosurg 2014;120:434-46.
- 9 Guerra WK, Gaab MR, Dietz H, Mueller JU, Piek J, Fritsch MJ, et al. Surgical decompression for traumatic brain swelling: Indications and results. J Neurosurg 1999;90:187-96.
- 10 Maas AI, Dearden M, Teasdale GM, Braakman R, Cohadon F, Iannotti F, et al. EBIC-guidelines for management of severe head injury in adults. European brain injury consortium. Acta Neurochir (Wien) 1997;139:286-94.
- 11 Marmarou A. Conduct of head injury trials in the United States: The American brain injury consortium (ABIC). Acta Neurochir Suppl 1996;66:118-21.
- 12 Diringer MN, Videen TO, Yundt K, Zazulia AR, Aiyagari V, Dacey RG Jr., et al. Regional cerebrovascular and metabolic effects of hyperventilation after severe traumatic brain injury. J Neurosurg 2002;96:103-8.
- 13 Doerfler A, Forsting M, Reith W, Staff C, Heiland S, Schäbitz WR, et al. Decompressive craniectomy in a rat model of “malignant” cerebral hemispheric stroke: Experimental support for an aggressive therapeutic approach. J Neurosurg 1996;85:853-9.
- 14 Marshall LF. Head injury: Recent past, present, and future. Neurosurgery 2000;47:546-61.
- 15 Oertel M, Kelly DF, Lee JH, McArthur DL, Glenn TC, Vespa P, et al. Efficacy of hyperventilation, blood pressure elevation, and metabolic suppression therapy in controlling intracranial pressure after head injury. J Neurosurg 2002;97:1045-53.
- 16 Piek J. Decompressive surgery in the treatment of traumatic brain injury. Curr Opin Crit Care 2002;8:134-8.
- 17 Hutchinson PJ, Kolias AG, Timofeev IS, Corteen EA, Czosnyka M, Timothy J, et al. Trial of decompressive craniectomy for traumatic intracranial hypertension. N Engl J Med 2016;375:1119-30.
- 18 Coplin WM, Cullen NK, Policherla PN, Vinas FC, Wilseck JM, Zafonte RD, et al. Safety and feasibility of craniectomy with duraplasty as the initial surgical intervention for severe traumatic brain injury. J Trauma 2001;50:1050-9.
- 19 Münch E, Horn P, Schürer L, Piepgras A, Paul T, Schmiedek P. Management of severe traumatic brain injury by decompressive craniectomy. Neurosurgery 2000;47:315-23.
- 20 Bor-Seng-Shu E, Figueiredo EG, Amorim RL, Teixeira MJ, Valbuza JS, de Oliveira MM, et al. Decompressive craniectomy: A meta-analysis of influences on intracranial pressure and cerebral perfusion pressure in the treatment of traumatic brain injury. J Neurosurg 2012;117:589-96.
- 21 Dennis MS, Burn JP, Sandercock PA, Bamford JM, Wade DT, Warlow CP, et al. Long-term survival after first-ever stroke: The oxfordshire community stroke project. Stroke 1993;24:796-800.
- 22 Göksu E, Uçar T, Akyüz M, Yılmaz M, Kazan S. Effects of decompressive surgery in patients with severe traumatic brain injury and bilateral non-reactive dilated pupils. Ulus Travma Acil Cerrahi Derg 2012;18:231-8.
- 23 Heuts SG, Bruce SS, Zacharia BE, Hickman ZL, Kellner CP, Sussman ES, et al. Decompressive hemicraniectomy without clot evacuation in dominant-sided intracerebral hemorrhage with ICP crisis. Neurosurg Focus 2013;34:E4.
- 24 Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, D'Urso P, et al. Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med 2011;364:1493-502.
- 25 Wettervik TS, Lenell S, Nyholm L, Howells T, Lewén A, Enblad P, et al. Decompressive craniectomy in traumatic brain injury: Usage and clinical outcome in a single centre. Acta Neurochir (Wien) 2018;160:229-37.
- 26 Mendelow AD, Gregson BA, Rowan EN, Francis R, McColl E, McNamee P, et al. Early surgery versus initial conservative treatment in patients with traumatic intracerebral hemorrhage (STITCH[Trauma]): The first randomized trial. J Neurotrauma 2015;32:1312-23.
- 27 Rubiano AM, Villarreal W, Hakim EJ, Aristizabal J, Hakim F, Dìez JC, et al. Early decompressive craniectomy for neurotrauma: An institutional experience. Ulus Travma Acil Cerrahi Derg 2009;15:28-38.
- 28 Taylor A, Butt W, Rosenfeld J, Shann F, Ditchfield M, Lewis E, et al. Arandomized trial of very early decompressive craniectomy in children with traumatic brain injury and sustained intracranial hypertension. Childs Nerv Syst 2001;17:154-62.
- 29 Seelig JM, Becker DP, Miller JD, Greenberg RP, Ward JD, Choi SC, et al. Traumatic acute subdural hematoma: Major mortality reduction in comatose patients treated within four hours. N Engl J Med 1981;304:1511-8.
- 30 Faleiro RM, Faleiro LC, Caetano E, Gomide I, Pita C, Coelho G, et al. Decompressive craniotomy: Prognostic factors and complications in 89 patients. Arq Neuropsiquiatr 2008;66:369-73.
- 31 Al-Jishi A, Saluja RS, Al-Jehani H, Lamoureux J, Maleki M, Marcoux J, et al. Primary or secondary decompressive craniectomy: Different indication and outcome. Can J Neurol Sci 2011;38:612-20.
- 32 Albanèse J, Leone M, Alliez JR, Kaya JM, Antonini F, Alliez B, et al. Decompressive craniectomy for severe traumatic brain injury: Evaluation of the effects at one year. Crit Care Med 2003;31:2535-8.
- 33 Honeybul S, Ho KM, Lind CR, Gillett GR. Validation of the CRASH model in the prediction of 18-month mortality and unfavorable outcome in severe traumatic brain injury requiring decompressive craniectomy. J Neurosurg 2014;120:1131-7.
- 34 Akyuz M, Ucar T, Acikbas C, Kazan S, Yilmaz M, Tuncer R, et al. Effect of early bilateral decompressive craniectomy on outcome for severe traumatic brain injury. Turk Neurosurg 2010;20:382-9.