

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_327_20
Recurrent meningeal melanocytoma of cervical spine: A rare case
Authors

Melanocytomas of the central nervous system are rare benign or intermediate grade localized melanocytic tumors. Despite its benign nature, it can follow a locally aggressive course with propensity to recur. We present the case of a 29 years old female who presented with a recurrent lesion in cervical spine and rapidly progressing quadriparesis. On examination, there was loss of power in right-sided extremities and reduction in sensations in left-sided extremities. Magnetic resonance imaging spine revealed a homogeneously enhancing intradural extramedullary dumbbell-shaped mass lesion at C4/5 level with extension through right C4 neural foramina to the extraforamina space, causing severe spinal cord compression. Intraoperatively, bluish-colored tumor was identified along with underlying hematoma. Gross total excision of the tumor was done. Tumor was received in the histopathology department in multiple black-colored fragments. Microscopically, a heavily pigmented tumor was seen with the sheets and nodules of polygonal cells with large nuclei and prominent nucleoli. Differentials considered were meningeal melanocytoma and malignant melanoma. On immunohistochemistry, the tumor cells showed diffuse positivity for HMB 45 and S100. Ki 67 index was around 1%. On radiological review, the tumor was fairly well circumscribed and did not infiltrate the adjacent tissues. There was no evidence of any lesions elsewhere in the body. Considering these features, the tumor was diagnosed with meningeal melanocytoma. Postoperatively, there was significant immediate improvement in quadriparesis and patient could walk with minimal support.
Introduction
Primary melanocytic neoplasms of the central nervous system (CNS) arise from leptomeningeal melanocytes and can be localized or diffuse. Melanocytosis refers to benign diffuse lesions that do not form masses, whereas the malignant counterpart of these diffuse lesions is termed as “melanomatosis.” Melanomas are malignant melanocytic tumors which form discrete masses while “Melanocytoma” is a term given to benign or intermediate grade localized melanocytic tumors.[[1]]
Melanocytomas are extremely rare neoplasms and account for 0.06%–0.1% of brain tumors with an annual incidence of 1 case per 10 million population. They often present as intradural lesions with dural attachment. Despite its benign nature, it can follow a locally aggressive course with propensity to recur.[[1]],[[2]]
We present a rare case of recurrent meningeal melanocytoma of cervical spine with locally aggressive behavior.
Case Report
A 29 years old female with no comorbidities developed insidious onset gradually progressive pains in the right upper extremity along C5 dermatomal distribution which was soon followed by weakness in right-sided grip. She underwent imaging and was found to have a mass lesion in the cervical spine at C4 level. The radiological appearance of the lesion was suggestive of intradural extramedullary (IDEM) pathology, for which she underwent surgery at an outside hospital. As per her operative notes, near total excision was achieved. Preoperative magnetic resonance imaging [MRI] was not available with the patient.
Histopathology report was suggestive of a pigmented nerve sheath tumor. No immunohistochemistry was performed at the time.
Soon after her surgery, she had relief from pains but weakness persisted. Over the next 2 months, she developed worsening of heaviness in the right upper limb which progressed to lower limb over next fortnight and then to left upper and lower limbs over the next 1 month. There was rapid worsening of quadriparesis.
On examination, her higher functions and cranial nerve examination were found to be normal. She had spastic grip in the right upper limb. Power was Grade I in right wrist extensors as well as flexors. Grade II at elbow flexors, Grade II at right elbow extensors, and Grade II power at right deltoid and shoulder abductors. Left upper and lower limbs had Grade IV power. There was loss of pain and crude touch sensations over the left half of the body in graded manner below C4 dermatome. She also had diminished bilateral biceps reflexes. Triceps reflex was brisk. There was bilateral ankle and patellar clonus, and plantars were mute. Joint position sense was lost all over.
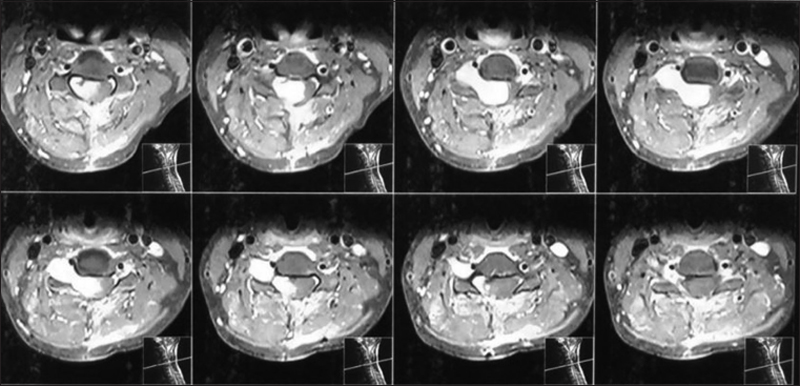
On imaging, MRI showed homogeneously enhancing IDEM mass lesion at C4/5 level with extension into the right C4 neural foramina causing widening of the foramen. The lesion appeared like a dumbbell with the outer component anterior to the vertebral artery in extraforaminal space. The lesion caused severe cord compression on the right side and distortion of the anatomy of the spinal cord [[Figure 1]].
Intraoperatively, bluish colored dumbbell-shaped extremely vascular tumor was identified along with underlying hematoma caused by a rent in the right-sided vertebral artery [[Figure 2]]. Hemostasis was achieved by bipolar coagulation in the area parallel to the vertebral artery. Bleeding was controlled after coagulating and cutting the dorsal spinal dura as well as root sleeve at C4-5 level. Total blood loss during the surgery was approximately 1 L. Gross total excision of the tumor was done and was subjected to histopathological examination.

Tumor was received in the histopathology department in multiple black colored fragments resembling a blood clot. On histology, the tumor was composed of sheets and nodules of heavily pigmented polygonal cells [[Figure 3]]. Focal spindle cell morphology and perivascular arrangement were noted. Nuclei were vesicular with prominent nucleoli. KMnO4 bleach was used to study the cell morphology in detail. There was no significant mitotic activity or necrosis [[Figure 4]].


Differentials considered were meningeal melanocytoma and malignant melanoma due to short duration of recurrence and the presence of large prominent nucleoli in some cells. We did not consider other pigmented lesions such as pigmented nerve sheath tumors or medulloblastoma because the cellular morphology was not consistent with either group of tumors.
On immunohistochemistry, the tumor cells showed diffuse positivity for HMB 45 and S100. Ki 67 index was around 1% [[Figure 5]]. On clinicoradiological review, the tumor was fairly well circumscribed and did not infiltrate the adjacent tissues. There was no evidence of any lesions elsewhere in the body.

Considering the low proliferative index, low mitotic activity, absence of necrosis, and lack of infiltrative nature, tumor was diagnosed with melanocytoma. However, close follow-up was advised since tumor had already shown propensity to recur.
Postoperatively, the patient had significant improvement in her quadriparesis and could walk with minimal support. She received radiation, 56 Gy in 40 fractions. On follow-up 2 months after surgery, she was ambulant without support. Her quadriparesis had completely recovered. All she had been left with was right-sided deltoid (Grade II) and biceps weakness (Grade III).
Discussion
In the CNS, preferential location of the melanocytes is in the upper cervical cord, ventral medulla oblongata, and base of the brain. IDEM compartment of cervical and thoracic spine represents the most common site of occurrence for meningeal melanocytoma. Less commonly, it can arise in trigeminal cave, posterior fossa, or in supratentorial compartment.[[1]] Few cases of intramedullary melanocytomas have also been reported.[[3]] It can occur over a wide age range (9–73 years) with a mean age of 45–50 years. A slight female preponderance has been reported.[[1]],[[4]],[[5]] In the present case, the tumor was detected in a 29 years old female in the C4–C5 IDEM compartment.
Melanocytic neoplasms of CNS can present with a wide variety of clinical symptoms. Diffuse leptomeningeal melanocytosis has known association with neurocutaneous melanosis and NF1 can present with still birth, hydrocephalus, raised intracranial pressure, intracranial hemorrhage, seizures, ataxia, cranial nerve palsies, syringomyelia, sphincter dysfunction, and neuropsychiatric symptoms. Malignant transformation is known and results in rapid clinical worsening.[[6]],[[7]],[[8]] Meningeal melanocytomas and melanomas are mass lesions and present with focal neurological signs associated with their location, such as raised intracranial pressure or hemorrhage, seizures, neuropsychiatric symptoms, and symptoms related to spinal cord compression.[[6]],[[9]],[[10]] The present case during her initial presentation had gradually progressive grip weakness in her right hand along with numbness and reduced sensations in the left lower limb. After surgery following a period of 2 months during which she had improvement in her symptoms, she developed tightness in her right wrist movements. She also had difficulty in walking due to tightness in the right lower limb. There was no history of bowel or bladder complaints. During her recurrence, she presented with rapidly progressing quadriparesis. Her examination predominantly showed the features of hemicord syndrome with loss of power in right-sided extremities and reduction in sensations in left-sided extremities. There were no bowel or bladder complaints.
On neuroimaging, these tumors are typically hyperintense on T1-weighted images and FLAIR, hypointense on T2-weighted images and show homogeneous contrast enhancement.[[6]],[[11]],[[12]] However, imaging appearance is quite variable, depends on the degree of mineralization and has a limited value in differential diagnosis of lesions occurring in this compartment.[[13]] Schwannoma, neurofibroma, and meningioma were considered as a differential diagnoses from radiology perspective. Features were mimicking neurofibroma the most.
Intraoperatively, melanocytomas are often found to be solitary, encapsulated intradural lesions with dural attachment. They are very vascular, and in majority of the cases, there is lack of any parenchymal invasion. Color of these lesions ranges from black to dark brown, reddish brown to blue. Nonpigmented lesions have also been reported.[[4]],[[6]],[[9]],[[10]],[[14]] Intraoperatively, the present lesion looked like a highly vascular solid tumor, bluish in color. Tumor was encapsulated, and there was an ill-defined arachnoid plane between the spinal cord and the tumor capsule. Very rarely, intermediate grade melanocytic tumors are known to invade the CNS. No evidence of infiltrative nature was found in the present case. However, the tumor was associated with significant hemorrhage which was traced to a rent in the right-sided vertebral artery.
Pigmented tumors of CNS include primary melanotic tumors of the CNS, metastatic melanoma, melanotic Schwannoma, medulloblastoma with melanotic differentiation, and rarely glial tumors and teratomas.[[15]] In the present case, tumor was composed of large heavily pigmented polygonal cells with vesicular nuclei and prominent nucleoli. We found no morphological evidence of a spindle cell lesion such as Schwannoma. Neither did we find any areas suspicious of a glial or an embryonal tumor. Considering the radiological finding of a single well-defined mass lesion, our main differentials were melanocytoma and malignant melanoma. Findings in favor of melanocytoma were lack of infiltrative nature of the tumor, very low mitotic activity, and absence of necrosis. Features favoring melanoma included high-grade nuclear features with macronucleoli and short duration of recurrence of the tumor. On immunohistochemistry, tumor cells were positive for melanocytic marker HMB45 and S100. Proliferative index (Ki67) was very low, which was around 1%. Ki 67 index has been reported to range from <1% to 5% in melanocytomas to more than 10% in melanomas. Intermediate values of 5%–10% are found in lesions classified as intermediate grade.[[4]],[[16]] According to the latest edition of the WHO classification of CNS tumors, Ki 67 is <1%–2% in melanocytomas and around 8% in primary melanomas.[[1]] Melanocytomas are positive for HMB45 and S100. Melanotic schwannomas are also positive for S100; however, HMB45 positivity is often only focal. Pigmented meningiomas often stain negative for HMB45 and S100.[[13]],[[14]] Melanocytomas despite their benign nature may behave aggressively and recurrence has been described from 7 months to 5 years after complete excision.[[17]],[[18]],[[19]] Rades et al. in their series described overall recurrence rate of 37% for meningeal melanocytomas. It was 24% after complete tumor resection, 0% after complete tumor resection followed by radiotherapy, 78% after incomplete tumor resection and 24% after incomplete tumor resection followed by radiotherapy.[[20]] Considering above features, final diagnosis of meningeal melanocytoma was given.
Several cases of malignant transformation of meningeal melanocytoma have been described in the literature. Recurrence time for these cases has ranged from 4 months[[21]] to 12 years.[[22]] Local relapse as well as distant metastasis to other areas of brain and even liver, rib and subcutaneous tissue has been described.[[23]]
Given its propensity to recur and a rare chance of malignant transformation, complete surgical resection is the standard treatment for these tumors but it is always associated with morbidity due to heavy blood loss owing to high vascularity of the tumor. Radiotherapy is necessary if complete excision is not possible. It's role in completely excised tumors is debatable.[[17]] In the present case, patient received radiation in the dosage of 56 Gy over 40 fractions. On follow-up, she could walk without support and power was normal in all four limbs except for the weakness in right deltoid and biceps. The weakness is now gradually improving, and she has been put on physical therapy regime for further recovery. She is functionally independent.
Conclusion
Primary melanocytic lesions of CNS include meningeal melanocytosis, meningeal melanomatosis, meningeal melanocytoma, and malignant melanoma. Melanocytomas are considered benign or intermediate grade tumors with propensity to recur and rarely undergo malignant transformation. They must be differentiated from primary and metastatic malignant melanomas and other pigmented lesions of CNS such as Schwannomas. Complete surgical excision is the treatment of choice with definite role of radiotherapy in incompletely resected tumors.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. WHO Classification of Tumours of the Central Nervous System. 4th ed. Lyon: International Agency for Research on Cancer: 2016.
- 2 Jellinger K, Böck F, Brenner H. Meningeal melanocytoma report of a case and review of the literature. Acta Neurochir (Wien) 1988;94:78-87.
- 3 Wagner F, Berezowska S, Wiest R, Gralla J, Beck J, Verma RK, et al. Primary intramedullary melanocytoma in the cervical spinal cord: Case report and literature review. Radiol Case Rep 2015;10:1010.
- 4 Brat DJ, Giannini C, Scheithauer BW, Burger PC. Primary melanocytic neoplasms of the central nervous system. Am J Surg Pathol 1999;23:745-54.
- 5 Wang H, Zhang S, Wu C, Zhang Z, Qin T. Melanocytomas of the central nervous system: A clinicopathological and molecular study. Eur J Clin Invest 2013;43:809-15.
- 6 Liubinas SV, Maartens N, Drummond KJ. Primary melanocytic neoplasms of the central nervous system. J Clin Neurosci 2010;17:1227-32.
- 7 Kadonaga JN, Frieden IJ. Neurocutaneous melanosis: Definition and review of the literature. J Am Acad Dermatol 1991;24:747-55.
- 8 Chang CS, Hsieh PF, Chia LG, Chen CC, Chen CC, Pan ST, et al. Leptomeningeal malignant melanoma arising in neurocutaneous melanocytosis: A case report. Zhonghua Yi Xue Za Zhi (Taipei) 1997;60:316-20.
- 9 Prabhu SS, Lynch PG, Keogh AJ, Parekh HC. Intracranial meningeal melanocytoma: A report of two cases and a review of the literature. Surg Neurol 1993;40:516-21.
- 10 Maiuri F, Iaconetta G, Benvenuti D, Lamaida E, De Caro ML. Intracranial meningeal melanocytoma: Case report. Surg Neurol 1995;44:556-61.
- 11 Uematsu Y, Yukawa S, Yokote H, Itakura T, Hayashi S, Komai N. Meningeal melanocytoma: Magnetic resonance imaging characteristics and pathological features: Case report. J Neurosurg 1992;76:705-9.
- 12 Naul LG, Hise JH, Bauserman SC, Todd FD. CT and MR of meningeal melanocytoma. Am J Neuroradiol 1991;12:315-6.
- 13 Sen R, Sethi D, Goyal V, Duhan A, Modi S. Spinal meningeal melanocytoma. Asian J Neurosurg 2011;6:110-2.
- 14 Litofsky NS, Zee CS, Breeze RE, Chandrasoma PT. Meningeal melanocytoma: Diagnostic criteria for a rare lesion. Neurosurgery 1992;31:945-8.
- 15 Smith AB, Rushing EJ, Smirniotopoulos JG. Pigmented lesions of the central nervous system: Radiologic-pathologic correlation. Radiographics 2009;29:1503-24.
- 16 Navas M, Pascual JM, Fraga J, Pedrosa M, Shakur S, Carrasco R, et al. Intracranial intermediate-grade meningeal melanocytoma with increased cellular proliferative index: An illustrative case associated with a nevus of Ota. J Neurooncol 2009;95:105-15.
- 17 Lin B, Yang H, Qu L, Li Y, Yu J. Primary meningeal melanocytoma of the anterior cranial fossa: A case report and review of the literature. World J Surg Oncol 2012;10:135.
- 18 Rades D, Tatagiba M, Brandis A, Dubben HH, Karstens JH. The value of radiotherapy for the treatment of meningeal melanocytoma. Strahlenther Onkol 2002;178:336-42.
- 19 Rades D, Heidenreich F, Tatagiba M, Brandis A, Karstens JH. Therapeutic options for meningeal melanocytoma. J Neurosurg 2001;95:225-31.
- 20 Rades D, Schild SE, Tatagiba M, Molina HA, Alberti W. Therapy of meningeal melanocytomas. Cancer 2004;100:2442-7.
- 21 Bydon A, Gutierrez JA, Mahmood A. Meningeal melanocytoma: An aggressive course for a benign tumor. J Neurooncol 2003;64:259-63.
- 22 Roser F, Nakamura M, Brandis A, Hans V, Vorkapic P, Samii M. Transition from meningeal melanocytoma to primary cerebral melanoma: Case report. J Neurosurg 2004;101:528-31.
- 23 Wang F, Li X, Chen L, Pu X. Malignant transformation of spinal meningeal melanocytoma: Case report and review of the literature. J Neurosurg Spine 2007;6:451-4.
Address for correspondence
Publication History
Received: 09 July 2020
Accepted: 27 October 2020
Article published online:
16 August 2022
© 2021. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Louis DN, Ohgaki H, Wiestler OD, Cavenee WK. WHO Classification of Tumours of the Central Nervous System. 4th ed. Lyon: International Agency for Research on Cancer: 2016.
- 2 Jellinger K, Böck F, Brenner H. Meningeal melanocytoma report of a case and review of the literature. Acta Neurochir (Wien) 1988;94:78-87.
- 3 Wagner F, Berezowska S, Wiest R, Gralla J, Beck J, Verma RK, et al. Primary intramedullary melanocytoma in the cervical spinal cord: Case report and literature review. Radiol Case Rep 2015;10:1010.
- 4 Brat DJ, Giannini C, Scheithauer BW, Burger PC. Primary melanocytic neoplasms of the central nervous system. Am J Surg Pathol 1999;23:745-54.
- 5 Wang H, Zhang S, Wu C, Zhang Z, Qin T. Melanocytomas of the central nervous system: A clinicopathological and molecular study. Eur J Clin Invest 2013;43:809-15.
- 6 Liubinas SV, Maartens N, Drummond KJ. Primary melanocytic neoplasms of the central nervous system. J Clin Neurosci 2010;17:1227-32.
- 7 Kadonaga JN, Frieden IJ. Neurocutaneous melanosis: Definition and review of the literature. J Am Acad Dermatol 1991;24:747-55.
- 8 Chang CS, Hsieh PF, Chia LG, Chen CC, Chen CC, Pan ST, et al. Leptomeningeal malignant melanoma arising in neurocutaneous melanocytosis: A case report. Zhonghua Yi Xue Za Zhi (Taipei) 1997;60:316-20.
- 9 Prabhu SS, Lynch PG, Keogh AJ, Parekh HC. Intracranial meningeal melanocytoma: A report of two cases and a review of the literature. Surg Neurol 1993;40:516-21.
- 10 Maiuri F, Iaconetta G, Benvenuti D, Lamaida E, De Caro ML. Intracranial meningeal melanocytoma: Case report. Surg Neurol 1995;44:556-61.
- 11 Uematsu Y, Yukawa S, Yokote H, Itakura T, Hayashi S, Komai N. Meningeal melanocytoma: Magnetic resonance imaging characteristics and pathological features: Case report. J Neurosurg 1992;76:705-9.
- 12 Naul LG, Hise JH, Bauserman SC, Todd FD. CT and MR of meningeal melanocytoma. Am J Neuroradiol 1991;12:315-6.
- 13 Sen R, Sethi D, Goyal V, Duhan A, Modi S. Spinal meningeal melanocytoma. Asian J Neurosurg 2011;6:110-2.
- 14 Litofsky NS, Zee CS, Breeze RE, Chandrasoma PT. Meningeal melanocytoma: Diagnostic criteria for a rare lesion. Neurosurgery 1992;31:945-8.
- 15 Smith AB, Rushing EJ, Smirniotopoulos JG. Pigmented lesions of the central nervous system: Radiologic-pathologic correlation. Radiographics 2009;29:1503-24.
- 16 Navas M, Pascual JM, Fraga J, Pedrosa M, Shakur S, Carrasco R, et al. Intracranial intermediate-grade meningeal melanocytoma with increased cellular proliferative index: An illustrative case associated with a nevus of Ota. J Neurooncol 2009;95:105-15.
- 17 Lin B, Yang H, Qu L, Li Y, Yu J. Primary meningeal melanocytoma of the anterior cranial fossa: A case report and review of the literature. World J Surg Oncol 2012;10:135.
- 18 Rades D, Tatagiba M, Brandis A, Dubben HH, Karstens JH. The value of radiotherapy for the treatment of meningeal melanocytoma. Strahlenther Onkol 2002;178:336-42.
- 19 Rades D, Heidenreich F, Tatagiba M, Brandis A, Karstens JH. Therapeutic options for meningeal melanocytoma. J Neurosurg 2001;95:225-31.
- 20 Rades D, Schild SE, Tatagiba M, Molina HA, Alberti W. Therapy of meningeal melanocytomas. Cancer 2004;100:2442-7.
- 21 Bydon A, Gutierrez JA, Mahmood A. Meningeal melanocytoma: An aggressive course for a benign tumor. J Neurooncol 2003;64:259-63.
- 22 Roser F, Nakamura M, Brandis A, Hans V, Vorkapic P, Samii M. Transition from meningeal melanocytoma to primary cerebral melanoma: Case report. J Neurosurg 2004;101:528-31.
- 23 Wang F, Li X, Chen L, Pu X. Malignant transformation of spinal meningeal melanocytoma: Case report and review of the literature. J Neurosurg Spine 2007;6:451-4.