

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_335_17
Nonvestibular schwannoma tumors in the cerebellopontine angle: A single-surgeon experience
Authors

Background: The most common cerebellopontine angle (CPA) tumor is a vestibular schwannoma. Schwannomas account for 8.5% of all intracranial tumors and more than 90% of the tumors originate from the eighth cranial nerve, but one in five CPA tumors are not vestibular schwannoma. These tumors may have different manifestations and require different management strategies. Methods: We report 224 consecutive NVCPAT operated in the Department of Neurosurgery, P.D. Hinduja National Hospital and Medical Research Centre, Mumbai, by the senior author between 2001 and 2014 and discuss the different approaches and outcomes in NVCPAT. Results: The age range was 20–60 years and there were 129 females and 95 male patients. The clinical material consisted of 81 cases of meningioma (36.1%), 44 cases of epidermoid (19.64%), 34 cases of trigeminal schwannoma (15.17%), 26 cases of jugular foramen schwannoma (11.60%), and 39 cases of other tumors (17.41%). In nonvestibular schwannoma (NVS), symptoms and signs from cranial nerve VIII are less frequent and other cranial nerves and cerebellar symptoms and signs predominate. Conclusion: Symptoms and signs are different in NVCPAT from those found in patients with vestibular schwannoma. Hearing loss is not the predominant symptoms. Cerebellar signs and trigeminal dysfunction are more common. The most common approach used in the current series was retrosigmoid craniotomy. Gamma knife radiosurgery was a useful adjunct in a subset of these patients.
Key-words:
Cerebellopontine angle - endolymphatic sac tumors - epidermoid - meningioma - nonvestibular schwannomaIntroduction
About 6%–10% of all intracranial tumors arise in or involve the cerebellopontine angle (CPA) and the vast majority of these (80%) are vestibular schwannomas.[[1]],[[2]],[[3]],[[4]],[[5]] Meningioma and epidermoid account for 10% and 6%, respectively, and the remainder consists of an extremely heterogeneous group of tumors that affect the region.[[1]],[[2]],[[3]],[[4]],[[5]] These tumors often resemble vestibular schwannomas in their clinical presentation and otologists must be aware that approximately one in five CPA tumors is not a vestibular schwannoma. A thorough history and examination will often provide clues leading to a different diagnosis and management strategy. In recent years, advances in neuroradiology have facilitated the preoperative differentiation of CPA lesions and have aided the surgical planning. Magnetic resonance imaging (MRI) is the investigation of choice.
Vestibular schwannomas are usually the cause for the typical symptoms of a CPA syndrome. Hearing and vestibular disturbances are by far the most common symptoms. The usual natural history of vestibular schwannoma is an insidious hearing loss that develops over several years, a pattern quite different from the less common CPA tumors.[[6]] Larger CPA tumors can inflict functional deficits on any of the cranial nerves that traverse the angle or neural structures that form part of its boundaries, the pons, and cerebellum. The progression and sequence of symptoms depend on individual regional anatomy and compliance, growth rate, and invasive nature of the tumor. The sequence of these symptoms may suggest a nonvestibular schwannoma (NVS) lesion.[[1]],[[3]],[[7]] Surprisingly, 30% of patients who present with a CPA syndrome have no diagnosable tumor at all but suffer from cerebrovascular disease, migraine, or other neurological disorder.[[8]] This original article provides approaches to diagnosis of NVS cerebellopontine tumors (NVCPAT) and management guidelines.
Materials and Methods
Between 2001 and 2014, 224 consecutive NVCPAT were operated in the Department of Neurosurgery, P.D. Hinduja National Hospital and Medical Research Centre, Mumbai, by a single surgeon.
Recorded documents were retrospectively studied for age, sex, clinical profile, investigations, microneurosurgical management, complications, and outcomes. Postoperatively, the patients were followed up clinically and radiologically at regular intervals. Postoperative computed tomography (CT) scan was performed in the immediate postoperative period. Follow-up MRI scan of the brain was done 3 months after the operation, 1 year after the operation, and at regular intervals.
Results
The age range was 20–60 years and there were 129 females and 95 male patients. The clinical material consisted of 81 cases of meningioma (36.1%), 44 cases of epidermoid (19.64%), 34 cases of trigeminal schwannoma (15.17%), 26 cases of jugular foramen schwannoma (11.60%), and 39 cases of other tumors (17.41%) [[Table 1]]. Trigeminal neuralgia was found as a significantly frequent sign of epidermoid and meningioma [[Table 2]]. Epidermoid was more common among males (24 out of 44), whereas meningioma was more common in females (61 out of 81 patients). Meningioma was found more commonly in the age group of fifth-to-sixth decade (46 out of 81 patients), whereas epidermoid was found more commonly in third-to-fourth decades (27 out of 44) [[Table 3]]. Other less common tumors operated were malignant skull base tumor (9), glomus jugulare (5), ependymoma (4), hemangioblastoma (4), endolymphatic sac tumor (ELST) (4), and facial nerve schwannoma (4). The other rare diagnoses were choroid plexus papilloma (2), pilocytic astrocytoma (2), cholesteatomas (1), cavernous hemangioma (1), solitary fibrous tumor (1), and melanoma (1). Many approaches were used for resection. Retrosigmoid was the most common approach; other common approaches used were Kawase's, fronto-temporo-orbito-zygomatic approach, far lateral, intralabyrinthine, endonasal, and petrosal [[Graph 1]]. Complete resection of tumor depended on type of NVCPAT and were as follows: meningioma, 55%; epidermoid, 95%; trigeminal schwannoma, 88%; and jugular foramen schwannoma, 62% [[Table 3]].



Two patients died postoperatively in this series, one had epidermoid and the other malignant skull base tumor.

Discussions
Schwannomas account for 8.5% of all intracranial tumors and more than 90% of the tumors originate from the eighth cranial nerve. The CPA is covered or lined by the meninges and in addition to cerebrospinal fluid, contains nerves, vessels, and possibly embryologic remnants. Each of these structures can be the tissue of origin of an NVS CPA lesion
Meningioma
Meningioma accounts for 10%–20% of all intracranial neoplasms. The incidence increases with age and the average age at the time of diagnosis of posterior fossa meningioma is 43.5 years.[[9]] About 5% to 10% of all meningioma are found in the CPA, predominately in middle-aged women. Second to vestibular schwannomas, meningioma is the second most common tumor in the CPA and constitutes approximately 10% of these tumors.[[1]],[[3]],[[10]] Meningioma is generally a benign tumor but is locally aggressive invading bone along the Haversian canals. This feature may produce radiologically demonstrable hyperostosis. Tumors displace or surround the cranial nerves and vessels rather than invade them and can become strongly adherent to these structures.[1.10] The tumor is best classified according to where the bulk of its volume is located and by its relationship to major neurovascular structure, information generally more useful to the surgeon.[[5]],[[10]],[[11]] Hormonal influence of these tumors has been investigated. Meningioma tumor cells contain a high concentration of progesterone receptors, moderate numbers of androgen receptors, and a low level of estrogen receptors. The potential of hormone therapy is being investigated.[[9]] Hearing loss is found at presentation in 50%–80% of patients with meningioma compared with almost all patients with vestibular schwannomas.[[1]],[[4]],[[5]],[[7]],[[10]],[[11]],[[12]],[[13]],[[14]] Tinnitus is experienced by anywhere from 15% to 60% of patients with meningioma compared with 80% with vestibular schwannoma.[[1]],[[4]],[[10]],[[12]],[[13]],[[14]] Disequilibrium troubles 30%–60% of patients with meningioma and is a presenting symptom in 80% of patients with vestibular schwannoma.[[1]],[[4]],[[10]],[[12]],[[13]],[[14]] Facial pain is rarely encountered in patients with vestibular schwannomas but is a presenting symptom in 5%–30% of patients with meningioma.[[11]],[[12]],[[13]],[[14]] The outcome from surgical resection of meningioma varies depending on tumor location and size. In recent series, gross total resection was achieved in 45%–86% and mortality ranged between 0% and 5%. Permanent postoperative facial weakness occurred in 6%–11% with as many as 30% having postoperative facial paresis. Swallowing problems occurred in 2%–12%. Hearing declined in 17% of patients in hearing preservation surgeries, although one large study found 91% of functional hearing preservation in their series.[[12]]
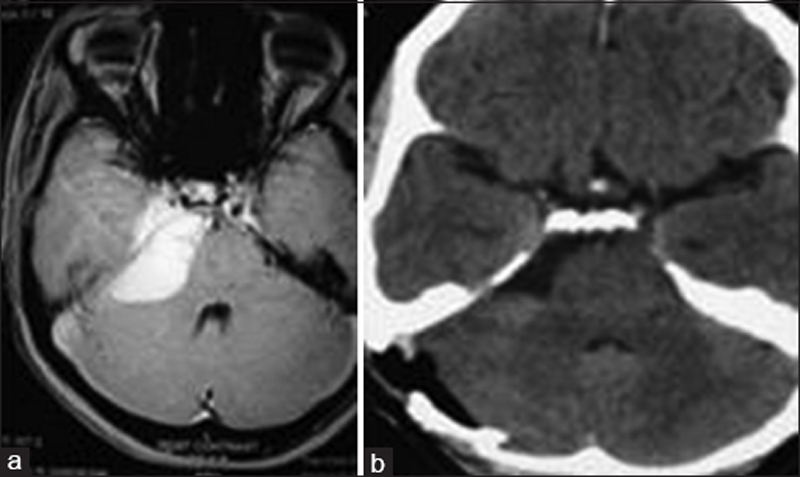
In our series of 81 patients of meningioma (51 patients of petroclival, 27 patients CPA, and 3 patients of jugular foramen meningioma), the male-to-female ratio was 1:4 and the median age was 49 years. Trigeminal nerve dysfunction (36%) was the predominant symptoms followed by hearing loss (32%) and cerebellar signs (22%). The most common surgical approach used was retrosigmoid (77%). Total excision was achieved in 55% of patients and postoperative facial function was preserved in 81% of patients. There was no mortality [[Figure 1]]a and [[Figure 1]]b. Excision may be accomplished through several standard approaches that are also employed for vestibular schwannomas. The choice depends on the patient's hearing status, the size and location of the tumor, and its involvement with neurovascular structures. The retrosigmoid approach has the advantage of offering the possibility of hearing preservation. Other approaches such as middle fossa approach, translabyrinthine approach, transcochlear and transtentorial approach, and sometimes combined approach are used depending on tumor size, location, and severity of seventh and eight nerve dysfunctions.
Radiosurgery may be used for CPA and petroclival meningioma, either primarily or as an adjunct to microsurgery. Good long-term control and a low side-effect profile have been demonstrated.[[15]],[[16]] By the time patients present to the surgeon, most petroclival meningiomas have reached a large size with a wide attachment and the tumor often invades the exit foramina of multiple cranial nerves. Total excision of the tumor with its dural and bony attachment is not possible in such cases without significant risks and unacceptable morbidity. In several cases, the difficulty of excision is further compounded by arterial and brain stem involvement.[[16]] A review of the literature clearly demonstrates the trend toward less aggressive surgery and an emphasis on the functional outcome, as reported in various series [[16]],[[17]],[[18]],[[19]],[[20]],[[21]],[[22]],[[23]],[[24]],[[25]],[[26]],[[27]] [[Table 4]]. Facial pain was the most common new symptom after radiosurgery.[[16]] In one study examining CPA meningioma, facial pain tended to persist after radiosurgery in petroclival meningioma despite effective tumor control.[[28]]

Epidermoid
Epidermoid account for 0.2%–1.8% of all intracranial neoplasm and an equal or slightly male-dominated incidence has been reported.[[3]],[[5]],[[29]],[[30]] About 30% to 40% of epidermoid are found in the CPA, where they account for 5%–9% of all tumors.[[5]],[[29]] Epidermoid is the third most common CPA lesion and represent approximately 6% of such lesion and 1% or all intracranial tumors.[[31]] Epidermoid is thought to develop from sequestered epithelial cells rests from the laterally migrating secondary optic and otic capsule or from developing embryonic neurovasculature but is not associated with other congenital abnormalities.[[18]] These grow slowly through accumulation of keratin and cholesterol from their squamous epithelial lining.[[32]] Their peak age of occurrence is 40 without gender predilection. It tends to spread along normal cleavage planes and surround, not displace, cranial nerves and blood vessels.[[33]] These are benign lesions, although malignant transformation has been reported.[[2]] The gross total resection of such lesions ranges from 33% to 88%.[[34]] In several larger studies, rates of tumor recurrence have ranged from 7% to 45%. Clinical improvements have been seen in 50%–100% of the patients. As in other surgeries of CPA, removal of these tumors has risks of facial weakness (0%–23%), worsening of hearing (8%–10%), and swallowing problems (0%–10%). The resection of epidermoid carries a 3%–8% risk of aseptic meningitis and 0%–4% of hydrocephalus requiring shunt.[[35]]
In our series of 44 patients of epidermoid, the male-to-female ratio was 1.4:1 and the median age was 34.5 year. Trigeminal nerve dysfunction (45%) was the predominant symptom followed by cerebellar sign (20%) and hearing loss (16%). The most common approach used was retrosigmoid (82%). Complete excision was achieved in 95% of patients and postoperative facial function was preserved in 95% of patients. There was one mortality. As with meningioma, hearing loss was less frequent (50%–80%) compared to vestibular schwannoma and early progressive facial nerve symptoms predominated.[[1]],[[4]],[[7]],[[29]],[[35]],[[36]],[[37]] Other less common symptoms were trigeminal neuralgia, facial numbness/spasm, cerebellar signs, and signs of elevated intracranial pressure. The lesions have a characteristic heterogeneous, low-signal-intensity appearance with no gadolinium enhancement on T1 images. Special fluid-attenuated inversion recovery and diffusion sequence MRI scans have proven useful in differentiating between arachnoid cysts and epidermoid.[[38]] Microsurgical removal of epidermoid was the treatment of choice and the retrosigmoid approach was the preferred technique. As with meningioma, alternative approaches such as the translabyrinthine or middle fossa can be employed if required.[[1]],[[3]],[[4]],[[5]],[[7]],[[35]],[[36]],[[39]] The goal of surgery is decompression of the cyst and removal of the capsule. The interior of the tumor is soft and caseous and can be easily removed with suction or curettage. The capsule, however, is more difficult to remove. Because of the pattern of growth, neurovascular structures are often engulfed in the tumor and total excision can be difficult without increased mortality and morbidity.[[1]],[[3]],[[4]],[[5]],[[7]],[[35]],[[36]],[[39]]
Trigeminal nerve schwannoma and other cranial nerve schwannoma
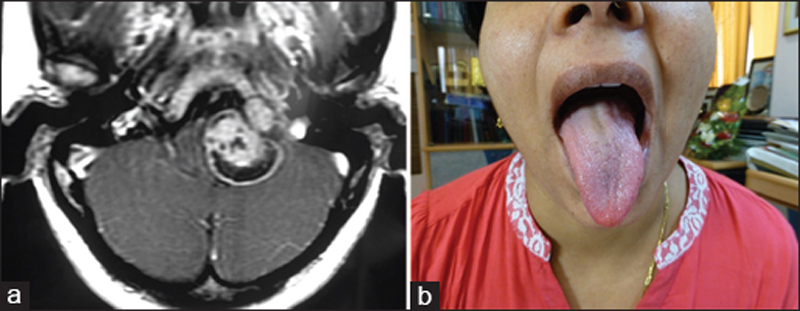
Trigeminal nerve schwannomas tend to involve the ganglion, nerve root, or both. Symptoms of trigeminal dysfunction tend to dominate over dysfunction of nerve VII and the patients may present with facial pain or numbness. Other symptoms of an expanding CPA tumor may also be present.[[1]],[[30]] CT scans demonstrate enlargement of Meckel's cave or foramen lacerum and the tumors tend to be hypo- or isodense and show contrast enhancement. On MRI, the tumors appear iso- or hypointense on T1-weighted images and isointense or hyperintense on T2-weighted images. They enhance as brightly as other schwannomas. Various approaches have been employed and large tumor removal is often possible through combined posterior and middle fossa approaches with lateral opening of Meckel's cave [[1]],[[30]] [[Figure 2]]a and [[Figure 2]]b.

In our series of 34 patients of trigeminal nerve schwannomas, the male-to-female ratio was1.1:1 and median age was 41 years. Trigeminal nerve dysfunction (65%) was the predominant symptoms followed by hearing loss (20%) and cerebellar signs (18%). The most common approach used was subtemporal petrous apex approach. Complete excision was achieved in 88% of patients and postoperative facial function was preserved in 85% of patient. There was no mortality.
Lower cranial nerve schwannomas account for [[30]] The future role of stereotactic radiotherapy or gamma knife for these schwannomas remains to be seen. In the future, more cases are likely to be treated this way and will probably have much the same outcome as with vestibular schwannoma [[40]] [[Figure 3]]a, [[Figure 3]]b and [[Figure 4]]a, [[Figure 4]]b.

In our series of 26 patients of jugular foramen schwannomas, the male-to-female ratio 1.1:1 and the median age was 45.5 years. The hearing loss (58%) was the predominant symptoms followed by cerebellar sign (38%) and trigeminal nerve dysfunction (4%). The most common approach used was retrosigmoid approach. Total excision was achieved in 62% of patients and postoperative facial function was preserved in 73% of patient. There was no mortality. Treatment strategy of jugular foramen tumor depends on the age of patients, size of tumors, and lower cranial nerve involvement [[41]] [[Flow chart 1]].

Paragangliomas (glomus tumors)
Paraganglioma is a benign but locally aggressive tumor and destroys the petrous bone to enlarge to the CPA. Symptoms include pulsatile tinnitus, headache, or hearing loss. On otoscopy, a red pulsatile mass can be seen behind the tympanic membrane with increased vascularization of the floor of the external auditory canal. Most patients have conductive hearing loss but with tumors that occupy the CPA either a mixed loss or profound sensorineural loss is not uncommon. Arteriography demonstrates the extent of the tumor and source of its blood supply.[[1]],[[2]] On CT, tumors appear well defined with adjacent bone erosion and marked enhancement after contrast injection. Paraganglioma has a characteristic “salt and pepper” appearance on both T1- and T2-weighted MRI images because of intratumoral blood vessels and hemorrhages. The tumors enhance intensely after gadolinium administration.[[1]],[[2]] Treatment options include radiosurgery or surgery.
Many centers have moved away from microsurgical resection in favor of stereotactic radiosurgery for such lesions because of the risk of lower cranial nerve dysfunction. Stereotactic radiation therapy is also a primary option for lesions with more limited extension. A newer paradigm for these lesions is dictated by patient symptomatology.[[42]] When pulsatile tinnitus and conductive hearing loss are bothersome to a patient, a targeted debulking of the middle ear and mastoid component may be undertaken. If indicated, based on the growth of the remaining lesion, adjuvant radiotherapy may be pursued. Unlike when complete resection is planned, the authors have found preoperative embolization is not needed when only a limited debulking is planned. In our series, the five cases of glomus tumors were operated by far lateral intralabyrinthine approach [[Figure 5]]a and [[Figure 5]]b.

Endolymphatic sac tumors
ELSTs are uncommon tumors and most often associated with von Hippel–Lindau (VHL) disease, although approximately 20% of cases result from sporadic mutations. Nevoux et al. have posited that sporadic tumors behave quite differently from those associated with VHL.[[43]] VHL may affect other organ systems, including cysts throughout the urogenital system, hemangioblastomas of the central nervous system (that may also present in the CPA), and certain malignancies. A majority of patients with VHL inherit this through an autosomal dominant pattern from mutations on chromosome 3. Pathologically, ELSTs are benign low-grade tumors but may be locally aggressive including erosion into the otic capsule. They are present in 10% of patients with VHL. They may cause progressive hearing loss as well as tinnitus and vertigo.[[44]] Characteristic imaging findings include T1 hyperintensity with heterogeneous enhancement after gadolinium administration. CT may also be helpful in demonstrating a destructive lesion centered at the posterior petrous temporal bone in the region of the vestibular aqueduct. Calcifications may be present as well [[Figure 6]]. Histologically, these lesions are characterized as papillary adenomatous lesions, and in some cases, are classified as adenocarcinomas.[[45]] Early gross total resection is advocated because of the high risk of recurrence when a subtotal resection is undertaken. In addition, larger lesions pose increased risk to postoperative facial nerve function. With larger lesions, preoperative embolization may be prudent because these tumors may be supplied by branches of the external carotid or vertebral arteries.[[30]] In cases where complete surgical resection is not possible or in poor surgical candidates, data suggest a role for adjuvant radiation therapy or primary stereotactic radiotherapy.[[44]],[[45]] Small, less-extensive lesions may be approached from a retrolabyrinthine approach, allowing access to the endolymphatic sac for complete resection of these lesions. This approach also allows for preservation of hearing, as Kim et al. demonstrated in maintaining stable pure-tone average in 30 of 31 ears operated through this approach.[[46]] Depending on a patient's preoperative hearing status, other approaches, including the translabyrinthine route, may be used.[[47]] In our series, all four patients of ELST were operated by intralabyrinthine approach [[Figure 6]]a and [[Figure 6]]b.

Choroid plexus papilloma
Choroid plexus papilloma is a rare tumor. They represent <1% of intracranial neoplasms. Derived from the epithelial cells of the choroid plexus, they have the same microstructure of normal choroid plexus when benign. Most often affecting children, they arise typically in the lateral ventricles. In adults, the most common site is the fourth ventricle. Malignant forms are very rare. Patients with choroid plexus papilloma may present with signs of a CPA tumor and if of significant size, raised intracranial pressure is almost always present. CPA choroid plexus papilloma should be evaluated using MRI. Their prognosis is excellent when total surgical excision is possible. Radiotherapy has been employed when surgery is not possible, but the results are variable.[[2]],[[48]],[[49]]
Choroid plexus papilloma has been reported both extending from the 4th ventricle through the foramen of Luschka and primarily in the CPA. Fourth ventricular tumors and tumors primarily in the CPA tend to present in adults.[[50]] These are benign lesions and can be managed solely with surgery. Less common are more aggressive lesions – so-called atypical papilloma and carcinomas.[[31]] Overall, 6% of papilloma recur and need repeated surgical intervention.[[51]] In the pre-MRI era, a series of 12 choroid plexus papilloma of the CPA were resected either through midline approach through the cerebellomedullary fissure or a retrosigmoid approach. Seven of those patients improved but two patients recurred.
Conclusions
Symptoms and signs are different in NVCPAT from those found in patients with vestibular schwannoma. Hearing loss is not the predominant symptoms. Cerebellar signs and trigeminal dysfunction are more common. The most common approach used in the current series was retrosigmoid craniotomy. Majority was benign tumors and had an excellent outcome. Early diagnosis, proper investigations, and evaluation, along with appropriate decision-making and surgical planning with microsurgical techniques are the essential factors that can result in an optimum outcome with complete resection and no new neurological deficit. Some of these tumors, especially petroclival meningioma and jugular foramen tumors are better managed by safe subtotal excision and radiosurgery.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Moffat DA, Ballagh RH. Rare tumours of the cerebellopontine angle. Clin Oncol (R Coll Radiol) 1995;7:28-41.
- 2 Bonneville F, Sarrazin JL, Marsot-Dupuch K, Iffenecker C, Cordoliani YS, Doyon D, et al. Unusual lesions of the cerebellopontine angle: A segmental approach. Radiographics 2001;21:419-38.
- 3 Lalwani AK. Meningiomas, epidermoids, and other nonacoustic tumors of the cerebellopontine angle. Otolaryngol Clin North Am 1992;25:707-28.
- 4 Grey PL, Moffat DA, Hardy DG. Surgical results in unusual cerebellopontine angle tumours. Clin Otolaryngol Allied Sci 1996;21:237-43.
- 5 Brunori A, Scarano P, Chiappetta F. Non-acoustic neuroma tumor (NANT) of the cerebello-pontine angle: A 15-year experience. J Neurosurg Sci 1997;41:159-68.
- 6 Thomsen J, Terkildsen K, Tos M. Acoustic neuromas. Progression of hearing impairment and function of the eighth cranial nerve. Am J Otol 1983;5:20-33.
- 7 Mallucci CL, Ward V, Carney AS, O'Donoghue GM, Robertson I. Clinical features and outcomes in patients with non-acoustic cerebellopontine angle tumours. J Neurol Neurosurg Psychiatry 1999;66:768-71.
- 8 Martuza RL, Parker SW, Nadol JB Jr., Davis KR, Ojemann RG. Diagnosis of cerebellopontine angle tumors. Clin Neurosurg 1985;32:177-213.
- 9 Glasscock ME, Minor LB, McMenomey SO. Meningiomas of the cerebellopontine angle. In: Jackler R, Brackmann D, editors. Neurotology. St. Louis: Mosby; 1994. p. 795-823.
- 10 Nager GT, Masica DN. Meningiomas of the cerebello-pontine angle and their relation to the temporal bone. Laryngoscope 1970;80:863-95.
- 11 Symon L, Pell M, Singh L. Surgical management of posterior cranial fossa meningiomas. Br J Neurosurg 1993;7:599-609.
- 12 Voss NF, Vrionis FD, Heilman CB, Robertson JH. Meningiomas of the cerebellopontine angle. Surg Neurol 2000;53:439-46.
- 13 Granick MS, Martuza RL, Parker SW, Ojemann RG, Montgomery WW. Cerebellopontine angle meningiomas: Clinical manifestations and diagnosis. Ann Otol Rhinol Laryngol 1985;94:34-8.
- 14 Laird FJ, Harner SG, Laws ER Jr., Reese DF. Meningiomas of the cerebellopontine angle. Otolaryngol Head Neck Surg 1985;93:163-7.
- 15 Nicolato A, Foroni R, Pellegrino M, Ferraresi P, Alessandrini F, Gerosa M, et al. Gamma knife radiosurgery in meningiomas of the posterior fossa. Experience with 62 treated lesions. Minim Invasive Neurosurg 2001;44:211-7.
- 16 Misra BK. Management of petroclival meningioma: The role of excision and radiosurgery. In: Al-Mefty O, editor. Controversies in Neurosurgery II. 2nd ed. New York: Thieme Publishers; 2014. p. 30-6.
- 17 Samii M, Ammirati M, Mahran A, Bini W, Sepehrnia A. Surgery of petroclival meningiomas: Report of 24 cases. Neurosurgery 1989;24:12-7.
- 18 Sekhar LN, Janneta PJ, Burkhat LE, Janosky JE. Meningioma involving the clivus: A six- year experience with 41 patients. Neurosurgery 1990;27:764-781
- 19 Al-Mefty O, Smith RR. Clival and petroclival meningioma. In: Al-Mefty O, editor. Meningiomas. New York: Raven Press; 1991. p. 517-37.
- 20 Kawase T, Shiobara R, Toya S. Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: Surgical method and results in 10 patients. Neurosurgery 1991;28:869-75.
- 21 Bricolo AP, Turazzi S, Talacchi A, Cristofori L. Microsurgical removal of petroclival meningiomas: A report of 33 patients. Neurosurgery 1992;31:813-28.
- 22 Spetzler RF, Daspit CP, Pappas CT. The combined supra- and infratentorial approach for lesions of the petrous and clival regions: Experience with 46 cases. J Neurosurg 1992;76:588-99.
- 23 Jung HW, Yoo H, Paek SH, Choi KS. Long-term outcome and growth rate of subtotally resected petroclival meningiomas: Experience with 38 cases. Neurosurgery 2000;46:567-74.
- 24 Little KM, Friedman AH, Sampson JH, Wanibuchi M, Fukushima T. Surgical management of petroclival meningiomas: Defining resection goals based on risk of neurological morbidity and tumor recurrence rates in 137 patients. Neurosurgery 2005;56:546-59.
- 25 Mathiesen T, Gerlich A, Kihlström L, Svensson M, Bagger-Sjöbäck D. Effects of using combined transpetrosal surgical approaches to treat petroclival meningiomas. Neurosurgery 2007;60:982-91.
- 26 Natarajan SK, Sekhar LN, Schessel D, Morita A. Petroclival meningiomas: Multimodality treatment and outcomes at long-term follow-up. Neurosurgery 2007;60:965-79.
- 27 Bambakidis NC, Kakarla UK, Kim LJ, Nakaji P, Porter RW, Daspit CP, et al. Evolution of surgical approaches in the treatment of petroclival meningiomas: A retrospective review. Neurosurgery 2007;61:202-9.
- 28 Kano H, Awan NR, Flannery TJ, Iyer A, Flickinger JC, Lunsford LD, et al. Stereotactic radiosurgery for patients with trigeminal neuralgia associated with petroclival meningiomas. Stereotact Funct Neurosurg 2011;89:17-24.
- 29 De la Cruz A, Doyle KJ. Epidermoids of the cerebellopontine angle. In: Jackler RK, Brackmann D, editors. Neurotology. St. Louis: Mosby; 1994. p. 823-33.
- 30 Bartels LJ, Arrington JR. Rare tumors of the cerebellopontine angle. In: Jackler RK, Brackmann D, editors. Neurotology. St. Louis: Mosby; 1994. p. 835-61.
- 31 Greenberg M, editor. Handbook of Neurosurgery. 7th ed. New York: Thieme; 2010.
- 32 Springborg JB, Poulsgaard L, Thomsen J. Nonvestibular schwannoma tumors in the cerebellopontine angle: A structured approach and management guidelines. Skull Base 2008;18:217-27.
- 33 Feng R, Gu X, Hu J, Lang L, Bi H, Guo J, et al. Surgical treatment and radiotherapy of epidermoid cyst with malignant transformation in cerebellopontine angle. Int J Clin Exp Med 2014;7:312-5.
- 34 Gopalakrishnan CV, Ansari KA, Nair S, Menon G. Long term outcome in surgically treated posterior fossa epidermoids. Clin Neurol Neurosurg 2014;117:93-9.
- 35 Samii M, Tatagiba M, Piquer J, Carvalho GA. Surgical treatment of epidermoid cysts of the cerebellopontine angle. J Neurosurg 1996;84:14-9.
- 36 Mohanty A, Venkatrama SK, Rao BR, Chandramouli BA, Jayakumar PN, Das BS, et al. Experience with cerebellopontine angle epidermoids. Neurosurgery 1997;40:24-9.
- 37 de Souza CE, Sperling NM, da Costa SS, Yoon TH, Abdel Hamid M, de Souza RA, et al. Congenital cholesteatomas of the cerebellopontine angle. Am J Otol 1989;10:358-63.
- 38 Dutt SN, Mirza S, Chavda SV, Irving RM. Radiologic differentiation of intracranial epidermoids from arachnoid cysts. Otol Neurotol 2002;23:84-92.
- 39 Talacchi A, Sala F, Alessandrini F, Turazzi S, Bricolo A. Assessment and surgical management of posterior fossa epidermoid tumors: Report of 28 cases. Neurosurgery 1998;42:242-51.
- 40 Misra BK, Purandare HR, Ved RS, Bagdia AA, Mare PB. Current treatment strategy in the management of vestibular schwannoma. Neurol India 2009;57:257-63.
- 41 Misra BK. Neurological Society of India guest lecture: Optimally invasive skull base surgery. Clin Neurosurg 2010;57:79-90.
- 42 Miller JP, Semaan M, Einstein D, Megerian CA, Maciunas RJ. Staged gamma knife radiosurgery after tailored surgical resection: A novel treatment paradigm for glomus jugulare tumors. Stereotact Funct Neurosurg 2009;87:31-6.
- 43 Nevoux J, Nowak C, Vellin JF, Lepajolec C, Sterkers O, Richard S, et al. Management of endolymphatic sac tumors: Sporadic cases and von Hippel-Lindau disease. Otol Neurotol 2014;35:899-904.
- 44 Carlson ML, Thom JJ, Driscoll CL, Haynes DS, Neff BA, Link MJ, et al. Management of primary and recurrent endolymphatic sac tumors. Otol Neurotol 2013;34:939-43.
- 45 Balasubramaniam S, Deshpande RB, Misra BK. Gamma knife radiosurgery in jugular foramen endolymphatic sac adenocarcinoma. J Clin Neurosci 2009;16:710-1.
- 46 Kim HJ, Hagan M, Butman JA, Baggenstos M, Brewer C, Zalewski C, et al. Surgical resection of endolymphatic sac tumors in von Hippel-Lindau disease: Findings, results, and indications. Laryngoscope 2013;123:477-83.
- 47 Friedmann DR, Grobelny B, Golfinos JG, Roland JT Jr. Nonschwannoma tumors of the cerebellopontine angle. Otolaryngol Clin North Am 2015;48:461-75.
- 48 Kieserman S, Linstrom C, McCormick S, Petschenik AJ. Choroid plexus papilloma of the cerebellopontine angle. Am J Otol 1996;17:119-22.
- 49 van Swieten JC, Thomeer RT, Vielvoye GJ, Bots GT. Choroid plexus papilloma in the posterior fossa. Surg Neurol 1987;28:129-34.
- 50 Talacchi A, De Micheli E, Lombardo C, Turazzi S, Bricolo A. Choroid plexus papilloma of the cerebellopontine angle: A twelve patient series. Surg Neurol 1999;51:621-9.
- 51 Jeibmann A, Wrede B, Peters O, Wolff JE, Paulus W, Hasselblatt M, et al. Malignant progression in choroid plexus papillomas. J Neurosurg Pediatr 2007;107:199-202.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Moffat DA, Ballagh RH. Rare tumours of the cerebellopontine angle. Clin Oncol (R Coll Radiol) 1995;7:28-41.
- 2 Bonneville F, Sarrazin JL, Marsot-Dupuch K, Iffenecker C, Cordoliani YS, Doyon D, et al. Unusual lesions of the cerebellopontine angle: A segmental approach. Radiographics 2001;21:419-38.
- 3 Lalwani AK. Meningiomas, epidermoids, and other nonacoustic tumors of the cerebellopontine angle. Otolaryngol Clin North Am 1992;25:707-28.
- 4 Grey PL, Moffat DA, Hardy DG. Surgical results in unusual cerebellopontine angle tumours. Clin Otolaryngol Allied Sci 1996;21:237-43.
- 5 Brunori A, Scarano P, Chiappetta F. Non-acoustic neuroma tumor (NANT) of the cerebello-pontine angle: A 15-year experience. J Neurosurg Sci 1997;41:159-68.
- 6 Thomsen J, Terkildsen K, Tos M. Acoustic neuromas. Progression of hearing impairment and function of the eighth cranial nerve. Am J Otol 1983;5:20-33.
- 7 Mallucci CL, Ward V, Carney AS, O'Donoghue GM, Robertson I. Clinical features and outcomes in patients with non-acoustic cerebellopontine angle tumours. J Neurol Neurosurg Psychiatry 1999;66:768-71.
- 8 Martuza RL, Parker SW, Nadol JB Jr., Davis KR, Ojemann RG. Diagnosis of cerebellopontine angle tumors. Clin Neurosurg 1985;32:177-213.
- 9 Glasscock ME, Minor LB, McMenomey SO. Meningiomas of the cerebellopontine angle. In: Jackler R, Brackmann D, editors. Neurotology. St. Louis: Mosby; 1994. p. 795-823.
- 10 Nager GT, Masica DN. Meningiomas of the cerebello-pontine angle and their relation to the temporal bone. Laryngoscope 1970;80:863-95.
- 11 Symon L, Pell M, Singh L. Surgical management of posterior cranial fossa meningiomas. Br J Neurosurg 1993;7:599-609.
- 12 Voss NF, Vrionis FD, Heilman CB, Robertson JH. Meningiomas of the cerebellopontine angle. Surg Neurol 2000;53:439-46.
- 13 Granick MS, Martuza RL, Parker SW, Ojemann RG, Montgomery WW. Cerebellopontine angle meningiomas: Clinical manifestations and diagnosis. Ann Otol Rhinol Laryngol 1985;94:34-8.
- 14 Laird FJ, Harner SG, Laws ER Jr., Reese DF. Meningiomas of the cerebellopontine angle. Otolaryngol Head Neck Surg 1985;93:163-7.
- 15 Nicolato A, Foroni R, Pellegrino M, Ferraresi P, Alessandrini F, Gerosa M, et al. Gamma knife radiosurgery in meningiomas of the posterior fossa. Experience with 62 treated lesions. Minim Invasive Neurosurg 2001;44:211-7.
- 16 Misra BK. Management of petroclival meningioma: The role of excision and radiosurgery. In: Al-Mefty O, editor. Controversies in Neurosurgery II. 2nd ed. New York: Thieme Publishers; 2014. p. 30-6.
- 17 Samii M, Ammirati M, Mahran A, Bini W, Sepehrnia A. Surgery of petroclival meningiomas: Report of 24 cases. Neurosurgery 1989;24:12-7.
- 18 Sekhar LN, Janneta PJ, Burkhat LE, Janosky JE. Meningioma involving the clivus: A six- year experience with 41 patients. Neurosurgery 1990;27:764-781
- 19 Al-Mefty O, Smith RR. Clival and petroclival meningioma. In: Al-Mefty O, editor. Meningiomas. New York: Raven Press; 1991. p. 517-37.
- 20 Kawase T, Shiobara R, Toya S. Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: Surgical method and results in 10 patients. Neurosurgery 1991;28:869-75.
- 21 Bricolo AP, Turazzi S, Talacchi A, Cristofori L. Microsurgical removal of petroclival meningiomas: A report of 33 patients. Neurosurgery 1992;31:813-28.
- 22 Spetzler RF, Daspit CP, Pappas CT. The combined supra- and infratentorial approach for lesions of the petrous and clival regions: Experience with 46 cases. J Neurosurg 1992;76:588-99.
- 23 Jung HW, Yoo H, Paek SH, Choi KS. Long-term outcome and growth rate of subtotally resected petroclival meningiomas: Experience with 38 cases. Neurosurgery 2000;46:567-74.
- 24 Little KM, Friedman AH, Sampson JH, Wanibuchi M, Fukushima T. Surgical management of petroclival meningiomas: Defining resection goals based on risk of neurological morbidity and tumor recurrence rates in 137 patients. Neurosurgery 2005;56:546-59.
- 25 Mathiesen T, Gerlich A, Kihlström L, Svensson M, Bagger-Sjöbäck D. Effects of using combined transpetrosal surgical approaches to treat petroclival meningiomas. Neurosurgery 2007;60:982-91.
- 26 Natarajan SK, Sekhar LN, Schessel D, Morita A. Petroclival meningiomas: Multimodality treatment and outcomes at long-term follow-up. Neurosurgery 2007;60:965-79.
- 27 Bambakidis NC, Kakarla UK, Kim LJ, Nakaji P, Porter RW, Daspit CP, et al. Evolution of surgical approaches in the treatment of petroclival meningiomas: A retrospective review. Neurosurgery 2007;61:202-9.
- 28 Kano H, Awan NR, Flannery TJ, Iyer A, Flickinger JC, Lunsford LD, et al. Stereotactic radiosurgery for patients with trigeminal neuralgia associated with petroclival meningiomas. Stereotact Funct Neurosurg 2011;89:17-24.
- 29 De la Cruz A, Doyle KJ. Epidermoids of the cerebellopontine angle. In: Jackler RK, Brackmann D, editors. Neurotology. St. Louis: Mosby; 1994. p. 823-33.
- 30 Bartels LJ, Arrington JR. Rare tumors of the cerebellopontine angle. In: Jackler RK, Brackmann D, editors. Neurotology. St. Louis: Mosby; 1994. p. 835-61.
- 31 Greenberg M, editor. Handbook of Neurosurgery. 7th ed. New York: Thieme; 2010.
- 32 Springborg JB, Poulsgaard L, Thomsen J. Nonvestibular schwannoma tumors in the cerebellopontine angle: A structured approach and management guidelines. Skull Base 2008;18:217-27.
- 33 Feng R, Gu X, Hu J, Lang L, Bi H, Guo J, et al. Surgical treatment and radiotherapy of epidermoid cyst with malignant transformation in cerebellopontine angle. Int J Clin Exp Med 2014;7:312-5.
- 34 Gopalakrishnan CV, Ansari KA, Nair S, Menon G. Long term outcome in surgically treated posterior fossa epidermoids. Clin Neurol Neurosurg 2014;117:93-9.
- 35 Samii M, Tatagiba M, Piquer J, Carvalho GA. Surgical treatment of epidermoid cysts of the cerebellopontine angle. J Neurosurg 1996;84:14-9.
- 36 Mohanty A, Venkatrama SK, Rao BR, Chandramouli BA, Jayakumar PN, Das BS, et al. Experience with cerebellopontine angle epidermoids. Neurosurgery 1997;40:24-9.
- 37 de Souza CE, Sperling NM, da Costa SS, Yoon TH, Abdel Hamid M, de Souza RA, et al. Congenital cholesteatomas of the cerebellopontine angle. Am J Otol 1989;10:358-63.
- 38 Dutt SN, Mirza S, Chavda SV, Irving RM. Radiologic differentiation of intracranial epidermoids from arachnoid cysts. Otol Neurotol 2002;23:84-92.
- 39 Talacchi A, Sala F, Alessandrini F, Turazzi S, Bricolo A. Assessment and surgical management of posterior fossa epidermoid tumors: Report of 28 cases. Neurosurgery 1998;42:242-51.
- 40 Misra BK, Purandare HR, Ved RS, Bagdia AA, Mare PB. Current treatment strategy in the management of vestibular schwannoma. Neurol India 2009;57:257-63.
- 41 Misra BK. Neurological Society of India guest lecture: Optimally invasive skull base surgery. Clin Neurosurg 2010;57:79-90.
- 42 Miller JP, Semaan M, Einstein D, Megerian CA, Maciunas RJ. Staged gamma knife radiosurgery after tailored surgical resection: A novel treatment paradigm for glomus jugulare tumors. Stereotact Funct Neurosurg 2009;87:31-6.
- 43 Nevoux J, Nowak C, Vellin JF, Lepajolec C, Sterkers O, Richard S, et al. Management of endolymphatic sac tumors: Sporadic cases and von Hippel-Lindau disease. Otol Neurotol 2014;35:899-904.
- 44 Carlson ML, Thom JJ, Driscoll CL, Haynes DS, Neff BA, Link MJ, et al. Management of primary and recurrent endolymphatic sac tumors. Otol Neurotol 2013;34:939-43.
- 45 Balasubramaniam S, Deshpande RB, Misra BK. Gamma knife radiosurgery in jugular foramen endolymphatic sac adenocarcinoma. J Clin Neurosci 2009;16:710-1.
- 46 Kim HJ, Hagan M, Butman JA, Baggenstos M, Brewer C, Zalewski C, et al. Surgical resection of endolymphatic sac tumors in von Hippel-Lindau disease: Findings, results, and indications. Laryngoscope 2013;123:477-83.
- 47 Friedmann DR, Grobelny B, Golfinos JG, Roland JT Jr. Nonschwannoma tumors of the cerebellopontine angle. Otolaryngol Clin North Am 2015;48:461-75.
- 48 Kieserman S, Linstrom C, McCormick S, Petschenik AJ. Choroid plexus papilloma of the cerebellopontine angle. Am J Otol 1996;17:119-22.
- 49 van Swieten JC, Thomeer RT, Vielvoye GJ, Bots GT. Choroid plexus papilloma in the posterior fossa. Surg Neurol 1987;28:129-34.
- 50 Talacchi A, De Micheli E, Lombardo C, Turazzi S, Bricolo A. Choroid plexus papilloma of the cerebellopontine angle: A twelve patient series. Surg Neurol 1999;51:621-9.
- 51 Jeibmann A, Wrede B, Peters O, Wolff JE, Paulus W, Hasselblatt M, et al. Malignant progression in choroid plexus papillomas. J Neurosurg Pediatr 2007;107:199-202.