

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_377_20
Clinicopathological correlation of glioma patients with respect to immunohistochemistry markers: A prospective study of 115 patients in a Tertiary Care Hospital in North India
Authors

Background: With the incorporation of molecular subtyping in glioma patients in 2016 WHO classification, there is a need to understand the immunohistochemistry (IHC) marker expression in various glioma patients and to clinically correlate with various subgroups. Objective: Aim of the study was to assess IHC marker expression profile in glioma patients and to clinically correlate them in various subgroups. Materials and Methods: The prospective study included 115 glioma patients. IHC markers (isocitrate dehydrogenase [IDH] 1, ATRX, P53, Ki-67 antibody) were done in all patients. Patients received treatment as per the grade of tumor. The patients were followed in 3 monthly intervals, for a period of 12 months. SPSS software version 20.0 was used for statistical analysis. Tables were prepared in Microsoft Excel sheet. Kaplan–Meier method was used for survival analysis. Results: There were 11 Grade 1, 33 Grade 2, 26 Grade 3, and 45 glioblastoma multiforme (GBM) patients out of which 10 patients were secondary GBM cases. IDH1 mutation is frequent in Grade 2 and Grade 3 tumors of both astrocytic and oligodendroglia tumors. Its mutation is also common in secondary GBM patients. ATRX mutation is specific to astrocytic lineage, Grade 2, Grade 3, and secondary GBM patients. Conclusion: Molecular nature of DA and AA cases can be accurately confirmed by combined IDH1 and ATRX IHC thereby avoiding costly investigations such as fluorescence in situ hybridization. In astrocytic tumors, p53 can act as a surrogate marker. IDH-mutant glioma patients have better prognoses than IDH wild gliomas.
Introduction
Central nervous tumors are the tumors which constitute about 1%–2% of all the neoplasm.[[1]] As central nervous system (CNS) tumors have variable histology, divergent morphological, and differentiation features, therefore, they pose major diagnostic challenges.[[2]] Nowadays, for the diagnosis of brain tumors, advances in immunohistochemistry (IHC), molecular pathology, and biomarkers play important role.[[3]]
Molecular parameters are included in the classification of CNS tumors in the recent update 2016 CNS WHO which has broken the century-old rule of diagnosis dependent only on microscopy.[[4]]
Tumor markers in CNS have both diagnostic and prognostic importance. Various clinical decisions are being made based of results of these biomarkers whether for screening, diagnosis, treatment, or prediction monitoring.[[5]],[[6]]
In patients with brain tumors, the clinical outcome depends on various factors such as age, clinical status, extent of tumor resection as well as the histological type, tumor grade, and other molecular alterations.[[7]]
Gliomas are the most common tumors in CNS system in children, and adults characterize predominantly by astrocytic or oligodendroglia morphology.[[8]]
It has been recently found that molecular subgrouping of gliomas is better than histological classification to stratify patients into prognostically distinct groups.[[9]] For diagnosis of gliomas, there are certain molecular parameters which include isocitrate dehydrogenase (IDH) 1-R132H mutation, ATRX mutation, and 1p/19q co-deletion. 1p/19q co-deletion is not detectable by IHC but is mutually exclusive to ATRX and p53 mutation in IDH1 gliomas.[[10]]
IHC is a long-standing, affordable, and widely available technology which was originally described by Coons et al. in 1941.[[11]]
Thus, IHC approaches with defined protocols and materials have become an essential means of assessing molecular genetic changes and therefore important aspect of current practice.
Materials and Methods
Study design
This present prospective study was undertaken in department of neurosurgery at a tertiary care center from October 2018 to December 2019. Study was initiated after approval from ethical committee. Each patient/guardian gave informed consent to obtain samples and its use for study purpose.
Study aim
-
To study IHC tumor marker expression profile in glioma patients
-
To clinically correlate IHC tumor marker expression in glioma patients.
Sample size
One hundred and fifteen patients were included whose radiological, clinical, and histological findings were suggested of gliomas and who underwent surgery at our institution. After surgical excision of the tumor, the part of tumor which was most viable and was devoid of macroscopic evident necrosis was taken as specimen. It was fixed in 10% formalin and sent for histopathology followed by immunohistochemical analysis.
The WHO classification of glioma was used for pathological grading. Postoperative radiotherapy/chemotherapy was uniformly given as recommended. Treatment of all patients included maximum surgical resection, radiation, and chemotherapy as recommended by the WHO. All Grade 1 patients had no further treatment after surgery.
Histopathological evaluation
Hematoxylin and eosin-stained slides were evaluated and the diagnosis was confirmed as per the WHO classification of CNS tumors.
Immunohistochemistry staining
IHC staining was done using one representative block in all cases. It was performed using primary antibody against the antigens for IDH1, ATRX, p53, and Ki-67. Biocare reagents were used for the staining procedure, and evaluation was done manually by two observers under microscope. All the procedures were done as per standard protocols.
IDH-R132H mutation was determined using IHC of mutation-specific anti 1DH antibodies (HPA035248-100 UL) in glioma patients. IDH1 protein expression was assessed. The proportion of cases with >10% cells stained positive was labeled as IDH-R132H mutant [[Figure 1]] and [[Figure 5]].
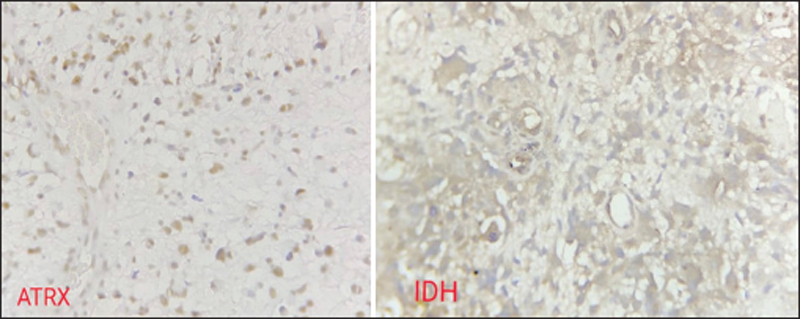
ATRX mutation was determined by IHC using polyclonal antibody (HPA001906-100 UL). Tumors with >50% stained cells are defined as ATRX retained and tumors with <50% stained cells are defined as ATRX loss. Endothelial cells, cortical neurons, and infiltrating inflammatory cells were generally positive and served as internal positive controls [[Figure 1]] and [[Figure 5]].
KI-67 IHC analysis was done by calculating the proportion of malignant cells stained positive for nuclear antigen. It was done in a quantitative and visual way using light microscopes (magnification, x400). The Ki67 percentage score is defined as the percentage of positively stained tumor cells among the total number of malignant cells assessed. Cases with >5% are stained positive and <5% are stained negative which are defined as positive and negative, respectively [[Figure 2]].

Similarly, p53 positivity was determined, and tumors with >10% cells stained on IHC are labeled as strong p53 immunoreactivity [[Figure 2]].
Statistical analysis
All Analysis were performed using IBM Statistical Product and Service Solution (SPSS) software version 20.0 (Armonk, Newyork, USA) 2011. Charts and tables were prepared in Microsoft Excel sheet. Mean (± standard deviation [SD]) was used for normally distributed continuous data. Survival analysis was done with Kaplan–Meier method. The survival was calculated from the time of surgery, till the patient remained in follow-up or the patient died in follow-up period. The patients were followed in 3 monthly intervals, for a period of 12 months.
Results
A total of 115 glioma patients were stained for IHC markers IDH1-R132H, ATRX, p53, and Ki-67 antibody. In our dataset, clinical, radiological features were consistent with histological diagnosis.
Descriptive analysis
In our study, 46 were female patients and 69 were male patients. Overall, there was male preponderance in our study. The most common clinical symptom observed was headache (87.8%) of patients, followed by seizure (67.8%), weakness of body (18.26%), and altered sensorium (11.3%).
KPS (Karnofsky Performance Status) score was evaluated in all patients. KPS score <70% was found in 16 patients (6.67%), 70–80% in 33 patients (36.19%), and above 80% in 66 patients (57.14%). The tumor was found in the left side in 51 patients, and right side in 53 patients and in midline in 11 patients. Hence, in our dataset, tumor was found in increased frequency in right side of the brain than left.
On histopathological analysis, tumor was found to be WHO Grade 1 in 11 (9.56%), WHO Grade 2 in 33 (28.69%) of patients, WHO Grade 3 in 26 (22.6%), and WHO Grade 4 in 45 (39.13%) of patients.
Postoperative therapy
In our study, WHO Grade 1 patients did not receive any radiotherapy or chemotherapy, all WHO Grade 2 patients received only radiotherapy, and WHO Grade 3 and Grade 4 patients received both radiotherapy and temozolomide chemotherapy.
Survival analysis
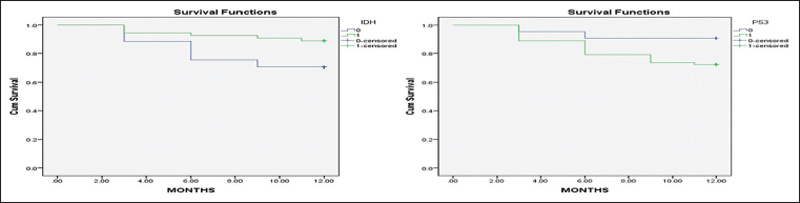
The patients were followed 3 monthly. At 3 months, 10 patients expired; at 6 months, 19 patients expired; at 9 months, 23 patients expired; and at 12 months, 24 patients expired with total of 91 patients (79.31%) survived along with the association of markers with survival association of markers IDH1-R132H, ATRX, p53, Ki-67 antibody with tumors were identified [[Figure 3]] and [[Figure 4]].


All Grade 1 patients were alive with no reoccurrence during 1 year of follow-up. Among Grade 2 out of 33 patients, 3 expired. Among the living patients, there was one case of reoccurrence. In Grade 3 patients out of 26, 4 patients expired. In 45 Grade 4 patients, 17 expired during 1 year.
IHC analysis
IHC marker association as per the WHO grade.
It is shown in [[Table 1]].

IHC marker association as per the diagnosis.
It is shown in [[Table 2]].

Discussion
In the recent years, advancement in molecular testing in glial tumors has helped to understand better about the pathogenesis and biology. Classification of gliomas into different prognostic groups, helps in the development of for various protocols for management of patients.[[12]] The commonly used IHC markers in glial tumors are IDH, ATRX, P53, and Ki-67 antibody index.
Molecular analysis of astrocytic lineage gliomas
Astrocytic lineage includes pilocytic astrocytoma, diffuse astrocytoma (DA), anaplastic astrocytoma, and glioblastoma.
Anaplastic astrocytoma (AA) and DA have identical IHC profile which is characterized by ATRX and IDH mutation.[[12]]
In both oligodendroglial and astrocytic tumors, IDH is well-established molecular marker. The prevalence of IDH mutation is not consistent in DA as it ranges from 54% to 90%.[[13]],[[14]] In pilocytic astrocytoma and glioblastoma, IDH mutation is rare.[[12]]
In our dataset, IDH1 mutation was not seen in PA whereas in DA, it was 73.6% and 64.28% in AA. Our results were comparable with other studies which showed that IDH1 mutations were more common in DA than AA.[[15]]
As per previous studies, high-grade gliomas with IDH mutation had shown better outcome.[[16]],[[17]] In high-grade glioma, the prognostic role of IDH mutation is unambiguously accepted; there is uncertainty about its prognostic role in glial tumors of low grade. Sanson et al. demonstrated that IDH1-mutated DA has shown longer overall survival than IDH1 wild cases (150.9 vs. 60.1 months).[[18]] There are few other studies which suggested that prognosis is better in Grade 2 IDH-mutant gliomas patients.[[14]] However, in some studies, there was no improved outcome in IDH mutant glioma patients.[[19]]
In our study, it was found that mutant IDH1 patients had better prognosis in term of overall survival in both DA and AA case. Among Grade 2 and Grade 3 tumors, Grade 2 tumors had better prognosis in our study, consolidating the importance of grading on the basis of histomorphological features. There was a study done by Ruess et al. in which little difference in survival was found between IDH mutant DA and AA.[[20]]
ATRX mutation is common in astrocytic lineage. IHC is used to determine nuclear ATRX expression. It occurs predominate in Grade 2 and Grade 3 astrocytic lineage glioma, i.e., DA and AA. It is found rarely in primary glioblastoma multiforme (GBM) and ODG.[[21]] In our study, ATRX loss was seen in 73.6% of DA and 64.2% of AA cases.
Accordingly, the presence of ATRX mutation which is depicted as loss of nuclear ATRX expression is helpful for deciding astrocytic lineage. Molecular diagnostic classification for diffuse gliomas is based on ATRX status with IDH1/IDH2 mutation and 1p/19q co-deletion status which is viewed as better than customary classification.
Therefore, tumors with loss of ATRX expression, IDH mutation, and intact 1p/19q have been classified as astrocytomas. Since 1p/19q co-deletion and ATRX mutation are mutually exclusive, all diffuse glioma patients need to be tested for IDH1 and ATRX status.[[12]]
Glioblastoma
In our study, we had 45 cases of glioblastoma. Out of which, only 14 cases (31.11%) were positive for IDH1. Similarly, ATRX was lost in 11 cases (24.44%). P53 was positive in 35 cases and Ki-67 antibody was >5% in all cases of glioblastoma. 35 were primary GBM cases, remaining 10 were secondary GBM.
In primary GBM cases, 6 were IDH mutant and 4 had ATRX loss. In secondary GBM cases, 8 were IDH positive and 7 had ATRX loss. P53 was positive in 27 primary GBM cases and 8 secondary GBM cases.
Among 45 GBM patients, 17 patients expired in 12 months of follow-up. Out of 17 patients, 13 were IDH negative and these results were suggestive of better survival among IDH-positive patients. Our results were comparable with previous results by various studies.[[22]]
Weller et al. studied in 301 GBM patients and found that IDH1 mutation in GBM has better progression-free and overall survival.
Few studies have demonstrated that some relationship exists between aberrant expression of ATRX, p53, and IDH1 proteins in GBM patients and their OS.[[17]]
Molecular analysis of oligodendroglial lineage gliomas
In our study, 83.33% ODG cases and 58.33% of anaplastic ODG had IDH1 mutation. Among 12 Grade 2 ODG patients, all patients survived for 12 months and among Grade 3 ODG patients, 1 patient expired after 6 months of follow-up. The expired patient was IDH negative, p53 positive with high Ki-67 index.
In ODG patients with negative IDH1, 1p/19q co-deletion by fluorescence in situ hybridization (FISH) needs to be done to confirm the diagnosis and if p53 is positive that is indicative of bad prognosis in these patients.[[23]]
Grade 2 patients with IDH mutation, with 1p/19q co-deletion, and retained ATRX are labeled as oligodendrogliomas. Cases with astrocytic morphology with retained ATRX or cases with ODG morphology with loss of ATRX are subjected to 1p/19q co-deletion status by FISH.[[2]]
p53
Frequency of p53 immunopositivity is higher in high-grade glioma patients (78.87) than that in low-grade gliomas (50%). In our study, p53 was positive in 77 (66.95%) patients. p53 was highly positive in Grade 3 and Grade 4 tumors. Out of 45 patients in Grade 4, 35 were positive (77.77%) for p53, 21 (80.76%) were positive for Grade 3, and only 19/31 patients (61.29%) were positive for Grade 2 patients.
For identification of p53 mutational analysis, p53 IHC is used as highly specific marker. In Grade 2 and Grade 3 tumors, p53 mutation is invariably associated with IDH1-R132H tumors and p53 mutation is mutually exclusive 1p/19q co-deletion. Hence, p53 is a valuable IHC marker and selected for analysis. There is a strong correlation between p53 mutation which is mutually exclusive with 1p/19q co-deletion, and ATRX loss is also mutually exclusive with 1p/19q co-deletion which suggests the importance of p53 and ATRX IHC without 1p/19q co-deletion mutational analysis.[[24]],[[25]] The association of p53 mutation in low-grade glioma is suggestive of aggressive behavior of the tumor which is usually observed after 3–4 years from diagnosis as this is the time required for the p53 mutation to expand which was observed by widespread p53 positivity in recurrences.[[26]]
Ki-67 antibody
Ki-67 expression is a marker of cancer cell proliferation and its higher value is associated with poor prognosis. High-grade gliomas have high Ki-67 antibodies. High Ki-67 expression in 19.4% cases of low-grade gliomas is associated with poor seizure control rate which is most common symptom in these patients. Ki-67 indices were comparable between similar grade gliomas. Ki-67 antibody is useful for low- and high-grade gliomas but to differentiate between different grades and categorize them is difficult. Hence, Ki-67 is not considered alone as a tumor-grade marker but in collaboration with other IHC markers and histomorphological features.[[27]]
Conclusion
The molecular IHC characterization with immunomarkers IDH1-R132H, ATRX, p53, Ki-67 anticipated that the low Grades 1 and 2 gliomas with DAs, oligodendroglioma, pilocytic astrocytoma had best prognosis, trailed by molecular group of AAs and poor result among glioblastoma patients. Molecular nature of DA and AA cases can be precisely determined by combined IDH1 and ATRX IHC markers thus reducing the need of costly investigations like FISH. In astrocytic tumors, p53 can act as a surrogate marker. Anyway, this system of classification cannot replace genetic analysis, yet at the same time can possibly precisely predict molecular subgrouping of all glioma patients. As there is unusual expression in our study, further assessment and long-term follow-up need to be done to consolidate their relationship with survival and prognosis.[[12]]
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Goyal R, Mathur SK, Gupta S, Goyal R, Kumar S, Batra A, et al. Immunohistochemical expression of glial fibrillary acidic protein and CAM5.2 in glial tumors and their role in differentiating glial tumors from metastatic tumors of central nervous system. J Neurosci Rural Pract 2015;6:499-503.
- 2 Madabhushi V, Venkata RI, Garikaparthi S, Kakarala SV, Duttaluru SS. Role of immunohistochemistry in diagnosis of brain tumors: A single institutional experience. J NTR Univ Health Sci 2015;4:103-11.
- 3 Mukherjee T, Dutta R, Ghosh J, Sharma M. Brain tumors with review of literature: Immunohistochemistry or biomarkers versus histomorphology. Neurooncol Open Access 2016;1.
- 4 Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol 2016;131:803-20.
- 5 Yang P, Cai J, Yan W, Zhang W, Wang Y, Chen B, et al. Classification based on mutations of TERT promoter and IDH characterizes subtypes in grade II/III gliomas. Neuro Oncol 2016;18:1099-108.
- 6 Fan Z, Liu Y, Li S, Liu X, Jiang T, Wang Y, et al. Association of tumor growth rates with molecular biomarker status: A longitudinal study of high-grade glioma. Aging (Albany NY) 2020;12:7908-26.
- 7 Cai J, Zhang C, Zhang W, Wang G, Yao K, Wang Z, et al. ATRX, IDH1-R132H and Ki-67 immunohistochemistry as a classification scheme for astrocytic tumors. Oncoscience 2016;3:258-65.
- 8 Rodriguez FJ, Vizcaino MA, Lin MT. Recent advances on the molecular pathology of glial neoplasms in children and adults. J Mol Diagn 2016;18:620-34.
- 9 Takano S, Ishikawa E, Sakamoto N, Matsuda M, Akutsu H, Noguchi M, et al. Immunohistochemistry on IDH ½, ATRX, p53 and Ki-67 substitute molecular genetic testing and predict patient prognosis in grade III adult diffuse gliomas. Brain Tumor Pathol 2016;33:107-16.
- 10 Cancer Genome Atlas Research Network, Brat DJ, Verhaak RG, Aldape KD, Yung WK, Salama SR, et al. Comprehensive, integrative genomic analysis of diffuse lower-grade gliomas. N Engl J Med 2015;372:2481-98.
- 11 Jaiswal S. Role of immunohistochemistry in the diagnosis of central nervous system tumors. Neurol India 2016;64:502-12.
- 12 Chatterjee D, Radotra BD, Kumar N, Vasishta RK, Gupta SK. IDH1, ATRX, and BRAFV600E mutation in astrocytic tumors and their significance in patient outcome in north Indian population. Surg Neurol Int 2018;9:29.
- 13 Ichimura K, Pearson DM, Kocialkowski S, Bäcklund LM, Chan R, Jones DT, et al. IDH1 mutations are present in the majority of common adult gliomas but rare in primary glioblastomas. Neuro Oncol 2009;11:341-7.
- 14 Zou P, Xu H, Chen P, Yan Q, Zhao L, Zhao P, et al. IDH1/IDH2 mutations define the prognosis and molecular profiles of patients with gliomas: A meta-analysis. PLoS One 2013;8:e68782.
- 15 Agarwal S, Sharma MC, Jha P, Pathak P, Suri V, Sarkar C, et al. Comparative study of IDH1 mutations in gliomas by immunohistochemistry and DNA sequencing. Neuro Oncol 2013;15:718-26.
- 16 Zeng A, Hu Q, Liu Y, Wang Z, Cui X, Li R, et al. IDH1/2 mutation status combined with Ki-67 labeling index defines distinct prognostic groups in glioma. Oncotarget 2015;6:30232-8.
- 17 Weller M, Felsberg J, Hartmann C, Berger H, Steinbach JP, Schramm J, et al. Molecular predictors of progression-free and overall survival in patients with newly diagnosed glioblastoma: A prospective translational study of the German Glioma Network. J Clin Oncol 2009;27:5743-50.
- 18 Sanson M, Marie Y, Paris S, Idbaih A, Laffaire J, Ducray F, et al. Isocitrate dehydrogenase 1 codon 132 mutation is an important prognostic biomarker in gliomas. J Clin Oncol 2009;27:4150-4.
- 19 Thon N, Eigenbrod S, Kreth S, Lutz J, Tonn JC, Kretzschmar H, et al. IDH1 mutations in grade II astrocytomas are associated with unfavorable progression-free survival and prolonged postrecurrence survival. Cancer 2012;118:452-60.
- 20 Reuss DE, Mamatjan Y, Schrimpf D, Capper D, Hovestadt V, Kratz A, et al. IDH mutant diffuse and anaplastic astrocytomas have similar age at presentation and little difference in survival: A grading problem for WHO. Acta Neuropathol 2015;129:867-73.
- 21 Park SH, Won J, Kim SI, Lee Y, Park CK, Kim SK, et al. Molecular testing of brain tumor. J Pathol Transl Med 2017;51:205-23.
- 22 Khan I, Waqas M, Shamim MS. Prognostic significance of IDH 1 mutation in patients with glioblastoma multiforme. J Pak Med Assoc 2017;67:816-7.
- 23 Pai T, Epari S, Desai S, Wadile A, Gupta T, Goda JS, et al. Histological spectrum of oligodendroglial tumors: Only a subset shows 1p/19q codeletion. Neurol India 2017;65:113-20.
- 24 Shao LW, Pan Y, Qi XL, Li YX, Ma XL, Yi WN, et al. ATRX loss in adult supratentorial diffuse astrocytomas correlates with p53 over expression and IDH1 mutation and predicts better outcome in p53 accumulated patients. Histol Histopathol 2016;31:103-14.
- 25 Thon N, Eigenbrod S, Grasbon-Frodl EM, Ruiter M, Mehrkens JH, Kreth S, et al. Novel molecular sterotactic biopsy procedures reveal intratumoral homogeneity of loss of hetrozygosity of 1p/19q and TP53 mutation in World Health Organisation grade 2 gliomas. J Neuropathol Exp Neurol 2009;68:1219-28.
- 26 Kannan K, Inagaki A, Silber J, Gorovets D, Zhang J, Kastenhuber ER, et al. Whole-exome sequencing identifies ATRX mutation as a key molecular determinant in lower-grade glioma. Oncotarget 2012;3:1194-203.
- 27 Skjulsvik AJ, Mørk JN, Torp MO, Torp SH. Ki-67/MIB-1 immunostaining in a cohort of human gliomas. Int J Clin Exp Pathol 2014;7:8905-10.
Address for correspondence
Publication History
Received: 03 August 2020
Accepted: 21 July 2020
Article published online:
16 August 2022
© 2021. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Goyal R, Mathur SK, Gupta S, Goyal R, Kumar S, Batra A, et al. Immunohistochemical expression of glial fibrillary acidic protein and CAM5.2 in glial tumors and their role in differentiating glial tumors from metastatic tumors of central nervous system. J Neurosci Rural Pract 2015;6:499-503.
- 2 Madabhushi V, Venkata RI, Garikaparthi S, Kakarala SV, Duttaluru SS. Role of immunohistochemistry in diagnosis of brain tumors: A single institutional experience. J NTR Univ Health Sci 2015;4:103-11.
- 3 Mukherjee T, Dutta R, Ghosh J, Sharma M. Brain tumors with review of literature: Immunohistochemistry or biomarkers versus histomorphology. Neurooncol Open Access 2016;1.
- 4 Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol 2016;131:803-20.
- 5 Yang P, Cai J, Yan W, Zhang W, Wang Y, Chen B, et al. Classification based on mutations of TERT promoter and IDH characterizes subtypes in grade II/III gliomas. Neuro Oncol 2016;18:1099-108.
- 6 Fan Z, Liu Y, Li S, Liu X, Jiang T, Wang Y, et al. Association of tumor growth rates with molecular biomarker status: A longitudinal study of high-grade glioma. Aging (Albany NY) 2020;12:7908-26.
- 7 Cai J, Zhang C, Zhang W, Wang G, Yao K, Wang Z, et al. ATRX, IDH1-R132H and Ki-67 immunohistochemistry as a classification scheme for astrocytic tumors. Oncoscience 2016;3:258-65.
- 8 Rodriguez FJ, Vizcaino MA, Lin MT. Recent advances on the molecular pathology of glial neoplasms in children and adults. J Mol Diagn 2016;18:620-34.
- 9 Takano S, Ishikawa E, Sakamoto N, Matsuda M, Akutsu H, Noguchi M, et al. Immunohistochemistry on IDH ½, ATRX, p53 and Ki-67 substitute molecular genetic testing and predict patient prognosis in grade III adult diffuse gliomas. Brain Tumor Pathol 2016;33:107-16.
- 10 Cancer Genome Atlas Research Network, Brat DJ, Verhaak RG, Aldape KD, Yung WK, Salama SR, et al. Comprehensive, integrative genomic analysis of diffuse lower-grade gliomas. N Engl J Med 2015;372:2481-98.
- 11 Jaiswal S. Role of immunohistochemistry in the diagnosis of central nervous system tumors. Neurol India 2016;64:502-12.
- 12 Chatterjee D, Radotra BD, Kumar N, Vasishta RK, Gupta SK. IDH1, ATRX, and BRAFV600E mutation in astrocytic tumors and their significance in patient outcome in north Indian population. Surg Neurol Int 2018;9:29.
- 13 Ichimura K, Pearson DM, Kocialkowski S, Bäcklund LM, Chan R, Jones DT, et al. IDH1 mutations are present in the majority of common adult gliomas but rare in primary glioblastomas. Neuro Oncol 2009;11:341-7.
- 14 Zou P, Xu H, Chen P, Yan Q, Zhao L, Zhao P, et al. IDH1/IDH2 mutations define the prognosis and molecular profiles of patients with gliomas: A meta-analysis. PLoS One 2013;8:e68782.
- 15 Agarwal S, Sharma MC, Jha P, Pathak P, Suri V, Sarkar C, et al. Comparative study of IDH1 mutations in gliomas by immunohistochemistry and DNA sequencing. Neuro Oncol 2013;15:718-26.
- 16 Zeng A, Hu Q, Liu Y, Wang Z, Cui X, Li R, et al. IDH1/2 mutation status combined with Ki-67 labeling index defines distinct prognostic groups in glioma. Oncotarget 2015;6:30232-8.
- 17 Weller M, Felsberg J, Hartmann C, Berger H, Steinbach JP, Schramm J, et al. Molecular predictors of progression-free and overall survival in patients with newly diagnosed glioblastoma: A prospective translational study of the German Glioma Network. J Clin Oncol 2009;27:5743-50.
- 18 Sanson M, Marie Y, Paris S, Idbaih A, Laffaire J, Ducray F, et al. Isocitrate dehydrogenase 1 codon 132 mutation is an important prognostic biomarker in gliomas. J Clin Oncol 2009;27:4150-4.
- 19 Thon N, Eigenbrod S, Kreth S, Lutz J, Tonn JC, Kretzschmar H, et al. IDH1 mutations in grade II astrocytomas are associated with unfavorable progression-free survival and prolonged postrecurrence survival. Cancer 2012;118:452-60.
- 20 Reuss DE, Mamatjan Y, Schrimpf D, Capper D, Hovestadt V, Kratz A, et al. IDH mutant diffuse and anaplastic astrocytomas have similar age at presentation and little difference in survival: A grading problem for WHO. Acta Neuropathol 2015;129:867-73.
- 21 Park SH, Won J, Kim SI, Lee Y, Park CK, Kim SK, et al. Molecular testing of brain tumor. J Pathol Transl Med 2017;51:205-23.
- 22 Khan I, Waqas M, Shamim MS. Prognostic significance of IDH 1 mutation in patients with glioblastoma multiforme. J Pak Med Assoc 2017;67:816-7.
- 23 Pai T, Epari S, Desai S, Wadile A, Gupta T, Goda JS, et al. Histological spectrum of oligodendroglial tumors: Only a subset shows 1p/19q codeletion. Neurol India 2017;65:113-20.
- 24 Shao LW, Pan Y, Qi XL, Li YX, Ma XL, Yi WN, et al. ATRX loss in adult supratentorial diffuse astrocytomas correlates with p53 over expression and IDH1 mutation and predicts better outcome in p53 accumulated patients. Histol Histopathol 2016;31:103-14.
- 25 Thon N, Eigenbrod S, Grasbon-Frodl EM, Ruiter M, Mehrkens JH, Kreth S, et al. Novel molecular sterotactic biopsy procedures reveal intratumoral homogeneity of loss of hetrozygosity of 1p/19q and TP53 mutation in World Health Organisation grade 2 gliomas. J Neuropathol Exp Neurol 2009;68:1219-28.
- 26 Kannan K, Inagaki A, Silber J, Gorovets D, Zhang J, Kastenhuber ER, et al. Whole-exome sequencing identifies ATRX mutation as a key molecular determinant in lower-grade glioma. Oncotarget 2012;3:1194-203.
- 27 Skjulsvik AJ, Mørk JN, Torp MO, Torp SH. Ki-67/MIB-1 immunostaining in a cohort of human gliomas. Int J Clin Exp Pathol 2014;7:8905-10.