

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_58_19
Onyx embolization of distal middle cerebral artery aneurysm in a patient with nontraumatic subdural hematoma
Authors

Distal cortical middle cerebral artery (MCA) aneurysm is a rare entity. Despite the challenging procedure, the role of endovascular treatment is emerging due to its safety and efficacy in obliterating the microaneurysm. We report a 25-year-old male, who presented with a history of dizziness and headache for almost 2 weeks. Computed tomography scan showed a right front parietal subdural hematoma (SDH). We could not identify any underlying defining etiology of SDH neither head injury nor coagulopathy disorder. Therefore, diagnostic cerebral angiogram was performed, which showed a microaneurysm in the distal right MCA cortical branch. Hence, complete obliteration of this microaneurysm was performed using Onyx for endovascular embolization. Therefore, this case report demonstrates the efficacy of this modality in the treatment of microaneurysms with SDH.
Introduction
Spontaneous subdural hematoma (SDH) is rarely associated with rupture of intracranial aneurysms (1%–2%).[[1]] The incidence of distal middle cerebral artery (MCA) aneurysm ranges from 1% to 1.7% of the intracranial aneurysms.[[2]] Due to complexity of location as well as the configuration of aneurysm, surgical management is considered as a reliable option.[[3]] However, we embolized the distal cortical MCA microaneurysm using Onyx.
Case Report
A 25-year-old Sudanese male, working in the military, presented in May 2018 to the emergency department with headache, dizziness, and vomiting. The patient has on and off headache for the past 2 weeks, mainly in the occipital region associated with multiple episodes of vomiting. There was no previous history of direct head trauma or any coagulation disorders.
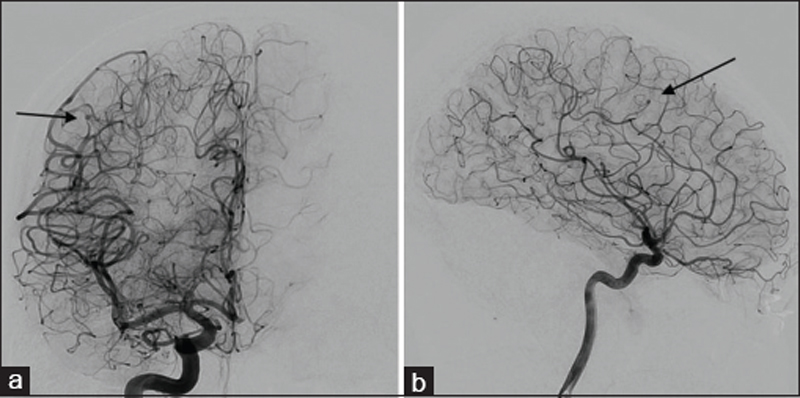
General physical examination revealed normal vital signs. The neurological examination revealed an alert, oriented patient with no focal neurological deficit. Routine blood investigations, including complete blood count, electrolytes, renal, and coagulation profiles, were within normal values. Brain computed tomography scan revealed a 4-mm thick right parietal acute SDH [[Figure 1]]. A subsequent brain and spine magnetic resonance imaging (MRI), on the 4th day, was negative for subarachnoid hemorrhage but indicated the right front parietal subacute SDH with marginal blooming at the interface of subdural collection with the cerebral cortex, whereas spinal axis MRI was unremarkable. Conventional cerebral angiograms (digital subtraction angiography) revealed a 1.5-mm diameter aneurysm in the distal perirolandic cortical branch of the right MCA [[Figure 2]]a and [[Figure 2]]b. The remaining intracranial arteries appeared unremarkable.

Due to small size of the parent artery and distal location, the patient was ineligible for the conventional therapy as it carried a high risk of rerupture and rebleeding. Endovascular embolization using Onyx was considered a viable treatment option. The procedure was discussed with the patient and his family, and an informed consent was obtained.
Under general anesthesia and local anesthesia using 1% lidocaine, cerebral angiography was performed through the right common femoral artery. A 6-French Arrow guide catheter was navigated in the right internal carotid artery (ICA), and an intermediate catheter was advanced with Sonic microcatheter to the cavernous part of the ICA in a coaxial fashion. Thereafter, the Sonic microcatheter was navigated into the cortical branch (M4) of the right MCA and positioned close to the microaneurysm. Onyx 18 was injected and noted to be migrating distal to the aneurysm bulb [[Figure 3]]. Complete occlusion of the aneurysm with Onyx 18 was successfully achieved. This also resulted in the cessation of flow to the distal segment of the aneurysm. A postprocedure cerebral angiogram confirmed the complete obliteration of the microaneurysm as well as the distal part of the parent artery [[Figure 4]]a and [[Figure 4]]b.


Postprocedure period was uneventful; the anesthesia was reversed and the patient was noted to be alert with no neurological deficit. There was no evidence of postendovascular complications on the follow-up MRI and magnetic resonance angiogram in the next day. An area of high intensity consistent with early subacute infarct in the right frontal region was noted [[Figure 5]]. Furthermore, there was no significant interval change as compared to the last MRI. Transthoracic echocardiography revealed no intracardiac mass, thrombi, or vegetation. Therefore, the patient was discharged with analgesics. The patient had no neurological signs and symptoms 2 weeks after discharge.

Discussion
Only 1%–2% of the cases of spontaneous SDH are associated with rupture of intracranial aneurysm.[[1]] This accumulation of blood could be directly through rupture of aneurysm in the subdural space [[4]],[[5]] or indirect through tear in the arachnoid membrane because of intracerebral bleeding.[[6]] There does not exist clear indications for either endovascular or direct surgical operations for distal microaneurysms. However, surgical management with neuronavigation in the form of clipping, trapping, or trapping plus bypass are considered an optimal choice due to the distant location of the aneurysm and tortuous course of the parent artery.[[3]],[[7]] The micro neurosurgical clipping of cortical aneurysms helps in preserving the parent artery by determining the patency of the parent vessel or the retrograde blood flow. This direct visualization helps in evaluating the thickness of the parent and perforated arteries, besides determining whether the parent vessel is closed either completely or incompletely. In addition, it can also evaluate the retrograde blood flow and thus can determine whether or not to go for a bypass procedure depending upon the flow to the parent arteries.[[8]],[[9]],[[10]] Similarly, endovascular treatment (EVT) is also gaining importance in terms of its safety and efficacy as an alternative treatment.[[11]] In a case series by Lv et al.,[[11]] all patients treated with EVT were stable with no recanalization. Now, the use of Onyx, a liquid embolic material, is becoming more common for obliterating the aneurysms.[[12]],[[13]] However, the obliteration of microaneurysms through EVT possesses a potential ischemic risk, as these aneurysms are distant, are small and have tortuous route.[[11]] In our case report, the patient recovered well with no neurological deficit.
The provocative tests with local anesthetics (propofol, etomidate, barbiturates etc.,) are essential before sacrificing the parent artery to predict the successful treatment with endovascular therapy, without neurological deficits.[[14]] However, in our case, balloon occlusion test using Hyperglide balloon 4 mm × 10 mm for 5 min was done as the lesion was located in the noneloquent area. Onyx 18 becomes solidified when it comes in contact with water or blood.[[15]] It has nonadhesive quality and longer working time and can be injected multiple times without removing the catheter until the aneurysm is completely obliterated.[[15]] We found this concentration to be very suitable to embolize distal aneurysm with low risk of adhesion to the catheter. Hence, endovascular treatment using Onyx offers effective modality of treatment for microaneurysm.
Other embolic materials such as N-butyl cyanoacrylate or soft coils can be a treatment of choice for complex aneurysms.[[16]] The approach to distal aneurysms for coiling would be difficult as the microcatheter would not provide enough support for the soft coils.[[16]],[[17]]
Our study limitations are as follows. First, as this is a case report we cannot generalize the efficacy of Onxy embolization to a large population. Second, provocative test with local anesthesia was not performed. Third, nonavailability of the soft coils in our center; thus we cannot compare the safety and efficacy of soft coils versus Onyx in treating microaneurysms.
Conclusion
We demonstrated good clinical functional outcome in a patient with spontaneous SDH associated with a distal cortical MCA aneurysm who underwent Onyx embolization. Onyx achieved complete obliteration of the aneurysm with no deterioration in the neurological status.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
By the Asian Journal of Neurosurgery, and Medical Research Council, Hamad Medical Corporation.
-
References
- 1 Lee SM, Park HS, Choi JH, Huh JT. Ruptured mycotic aneurysm of the distal middle cerebral artery manifesting as subacute subdural hematoma. J Cerebrovasc Endovasc Neurosurg 2013;15:235-40.
- 2 Baltacioǧlu F, Cekirge S, Saatci I, Oztürk H, Arat A, Pamir N. Distal middle cerebral artery aneurysms. Endovascular treatment results with literature review. Interv Neuroradiol 2002;8:399-407.
- 3 Lee SH, Bang JS. Distal middle cerebral artery M4 aneurysm surgery using navigation-CT angiography. J Korean Neurosurg Soc 2007;42:478-80.
- 4 Kocak A, Ates O, Durak A, Alkan A, Cayli S, Sarac K, et al. Acute subdural hematomas caused by ruptured aneurysms: Experience from a single Turkish center. Turk Neurosurg 2009;19:333-7.
- 5 Mrfka M, Pistracher K, Augustin M, Kurschel-Lackner S, Mokry M. Acute subdural hematoma without subarachnoid hemorrhage or intraparenchymal hematoma caused by rupture of a posterior communicating artery aneurysm: Case report and review of the literature. J Emerg Med 2013;44:e369-73.
- 6 Ishibashi A, Yokokura Y, Sakamoto M. Acute subdural hematoma without subarachnoid hemorrhage due to ruptured intracranial aneurysm – Case report. Neurol Med Chir (Tokyo) 1997;37:533-7.
- 7 Raza SM, Papadimitriou K, Gandhi D, Radvany M, Olivi A, Huang J. Intra-arterial intraoperative computed tomography angiography guided navigation: A new technique for localization of vascular pathology. Neurosurgery 2012;71:ons240-52.
- 8 Gross BA, Du R. STA-MCA bypass. Acta Neurochir (Wien) 2012;154:1463-7.
- 9 Raabe A, Nakaji P, Beck J, Kim LJ, Hsu FP, Kamerman JD. Prospective evaluation of surgical microscope-integrated intraoperative near-infrared indocyanine green videoangiography during aneurysm surgery. J Neurosurg 2005;103:982-9.
- 10 Suzuki K, Kodama N, Sasaki T, Matsumoto M, Ichikawa T, Munakata R. Confirmation of blood flow in perforating arteries using fluorescein cerebral angiography during aneurysm surgery. J Neurosurg 2007;107:68-73.
- 11 Lv N, Zhou Y, Yang P, Li Q, Zhao R, Fang Y, et al. Endovascular treatment of distal middle cerebral artery aneurysms: Report of eight cases and literature review. Interv Neuroradiol 2016;22:12-7.
- 12 Chalouhi N, Tjoumakaris S, Gonzalez LF, Hasan D, Alkhalili K, Dumont AS, et al. Endovascular treatment of distal intracranial aneurysms with onyx 18/34. Clin Neurol Neurosurg 2013;115:2528-32.
- 13 Utoh J, Miyauchi Y, Goto H, Obayashi H, Hirata T. Endovascular approach for an intracranial mycotic aneurysm associated with infective endocarditis. J Thorac Cardiovasc Surg 1995;110:557-9.
- 14 Feliciano CE, de León-Berra R, Hernández-Gaitán MS, Torres HM, Creagh O, Rodríguez-Mercado R, et al. Provocative test with propofol: Experience in patients with cerebral arteriovenous malformations who underwent neuroendovascular procedures. AJNR Am J Neuroradiol 2010;31:470-5.
- 15 Kurdi M, Baeesa S, Bin-Mahfoodh M, Kurdi K. Onyx embolization of ruptured intracranial aneurysm associated with behçet's disease. Case Rep Vasc Med 2013;2013:797045.
- 16 Lee CY. Embolization with NBCA for ruptured aneurysm located in the moyamoya-like collateral network associated with isolated middle cerebral artery occlusion. Asian J Neurosurg 2018;13:1236-8.
- 17 Lee JY, Kim MK, Cho BM, Park SH, Oh SM. Surgical experience of the ruptured distal anterior cerebral artery aneurysms. J Korean Neurosurg Soc 2007;42:281-5.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Lee SM, Park HS, Choi JH, Huh JT. Ruptured mycotic aneurysm of the distal middle cerebral artery manifesting as subacute subdural hematoma. J Cerebrovasc Endovasc Neurosurg 2013;15:235-40.
- 2 Baltacioǧlu F, Cekirge S, Saatci I, Oztürk H, Arat A, Pamir N. Distal middle cerebral artery aneurysms. Endovascular treatment results with literature review. Interv Neuroradiol 2002;8:399-407.
- 3 Lee SH, Bang JS. Distal middle cerebral artery M4 aneurysm surgery using navigation-CT angiography. J Korean Neurosurg Soc 2007;42:478-80.
- 4 Kocak A, Ates O, Durak A, Alkan A, Cayli S, Sarac K, et al. Acute subdural hematomas caused by ruptured aneurysms: Experience from a single Turkish center. Turk Neurosurg 2009;19:333-7.
- 5 Mrfka M, Pistracher K, Augustin M, Kurschel-Lackner S, Mokry M. Acute subdural hematoma without subarachnoid hemorrhage or intraparenchymal hematoma caused by rupture of a posterior communicating artery aneurysm: Case report and review of the literature. J Emerg Med 2013;44:e369-73.
- 6 Ishibashi A, Yokokura Y, Sakamoto M. Acute subdural hematoma without subarachnoid hemorrhage due to ruptured intracranial aneurysm – Case report. Neurol Med Chir (Tokyo) 1997;37:533-7.
- 7 Raza SM, Papadimitriou K, Gandhi D, Radvany M, Olivi A, Huang J. Intra-arterial intraoperative computed tomography angiography guided navigation: A new technique for localization of vascular pathology. Neurosurgery 2012;71:ons240-52.
- 8 Gross BA, Du R. STA-MCA bypass. Acta Neurochir (Wien) 2012;154:1463-7.
- 9 Raabe A, Nakaji P, Beck J, Kim LJ, Hsu FP, Kamerman JD. Prospective evaluation of surgical microscope-integrated intraoperative near-infrared indocyanine green videoangiography during aneurysm surgery. J Neurosurg 2005;103:982-9.
- 10 Suzuki K, Kodama N, Sasaki T, Matsumoto M, Ichikawa T, Munakata R. Confirmation of blood flow in perforating arteries using fluorescein cerebral angiography during aneurysm surgery. J Neurosurg 2007;107:68-73.
- 11 Lv N, Zhou Y, Yang P, Li Q, Zhao R, Fang Y, et al. Endovascular treatment of distal middle cerebral artery aneurysms: Report of eight cases and literature review. Interv Neuroradiol 2016;22:12-7.
- 12 Chalouhi N, Tjoumakaris S, Gonzalez LF, Hasan D, Alkhalili K, Dumont AS, et al. Endovascular treatment of distal intracranial aneurysms with onyx 18/34. Clin Neurol Neurosurg 2013;115:2528-32.
- 13 Utoh J, Miyauchi Y, Goto H, Obayashi H, Hirata T. Endovascular approach for an intracranial mycotic aneurysm associated with infective endocarditis. J Thorac Cardiovasc Surg 1995;110:557-9.
- 14 Feliciano CE, de León-Berra R, Hernández-Gaitán MS, Torres HM, Creagh O, Rodríguez-Mercado R, et al. Provocative test with propofol: Experience in patients with cerebral arteriovenous malformations who underwent neuroendovascular procedures. AJNR Am J Neuroradiol 2010;31:470-5.
- 15 Kurdi M, Baeesa S, Bin-Mahfoodh M, Kurdi K. Onyx embolization of ruptured intracranial aneurysm associated with behçet's disease. Case Rep Vasc Med 2013;2013:797045.
- 16 Lee CY. Embolization with NBCA for ruptured aneurysm located in the moyamoya-like collateral network associated with isolated middle cerebral artery occlusion. Asian J Neurosurg 2018;13:1236-8.
- 17 Lee JY, Kim MK, Cho BM, Park SH, Oh SM. Surgical experience of the ruptured distal anterior cerebral artery aneurysms. J Korean Neurosurg Soc 2007;42:281-5.