

RSS-Feed abonnieren
DOI: 10.4103/ijmbs.ijmbs_16_21
Solid organ transplantation medicine in Arab countries: A Narrative Review Focused on Ethical Aspects
Autoren

Introduction: Ethical issues have been at the center of transplantation medicine for the past 60 years. Arab countries are not without ethical concerns with living donations as the dominant type of organ source. There is no comprehensive review of the ethical consideration evolvement. This narrative review aims to examine the English medical literature over the past 25 years. Materials and Methods: This is a narrative review of the international literature from two online databases (PubMed and Scopus). The combined search term “Ethics and Transplantation” was coupled with the individual names of the countries of the Arab countries. Relevant literature was narrated in a concise thematic account. Results: The themes that emerged from the review process included global concern on transplantation ethics that touched on the Middle East and North Africa (MENA) region. Some reports on transplantation practice status in the MENA region address clinical practice, organization, and ethical considerations. Organ-specific reports focused on renal and liver transplantation. Several other researchers addressed the knowledge and attitudes of health-care professionals of transplantation and posttransplantation care. The ethics of transplantation medicine has focused on the donation and financially motivated provision of organs (mainly kidneys). A few authors have underscored the implications of the Istanbul declaration on the prevention of trafficking of human organs to the practice of transplant medicine. Being a Muslim-majority region, several authors addressed the ethical and medicolegal aspects of transplantation from an Islamic perspective. Conclusions: Ethical issues in transplantation are evolving in Arab countries. They are mostly related to religious and cultural backgrounds. A broader dialog between the medical community, Islamic scholars, and legislators must continue to align concepts such as brain death and donor compensation. Furthermore, a concerted effort is required to inform the public and further the transplant agenda.
Key-words:
Arab countries - ethics - Islamic - kidney - liver - medico-legal - middle east - North Africa - organ donation - organ transplantation - reviewIntroduction
Ethical concerns accompanied clinical transplantation from its inception. Dr. Joseph Murray, (1919–2012) who performed the first successful living donor kidney transplant in 1954, was concerned about the ethics of removing a vital organ from a normal, healthy human being.[[1]]
The perpetual shortage of donor organs continues to generate debate about the ethical principles applied in transplantation medicine. Several living donor issues continue to stimulate discussion and research interest.[[2]],[[3]],[[4]],[[5]] These include donations in the presence of hypertension, diabetes, and donations from the elderly. Other ethical concerns emerged with procuring organs from brain dead donors. Obtaining proper consent, separation of the event of death to the family, organ donation approaches, procuring organs from older donors, risk of transmission of disease, and donation after circulatory death are among such concerns.[[6]]
Solid-organ transplantation in the Middle East and North Africa region began in Iran in 1968 and other countries followed. By 2012, there were 31,280 renal transplants, with 92.9% performed in five countries (Egypt, KSA, Iraq, Syria, and Jordan); 3407 liver transplants: 91.9% in Egypt and KSA; 301 heart transplants: 87.7% in KSA and Lebanon; and 62 lung transplants: 61 in the KSA.[[7]] In many countries, transplantation has evolved through distinct stages of development, and at present, living-related donors continue to be the primary source of transplant organs.
The field of transplantation is packed with questions about guardianship and allocation of scarce resources (stewardship) and physician–patient relationship, in addition to principles such as altruism, autonomy, sanctity of life, and end of life questions including when precisely does life end.[[8]],[[9]],[[10]],[[11]],[[12]],[[13]]
An early account by Daar[[14]] indicated that Islamic opinion is in favor of transplantation of organs from both living and deceased donors.[[14]] Muslim jurists allowed bone grafts (autograft, allograft, and xenograft) for widely broken bones. Ibnosina discussed this subject in 1037 in his book Al-Kanoon. In 1959, the Muftis of Egypt and Tunisia allowed, under specific conditions, corneal transplants from dead persons.[[15]] Thereafter, many fatwas (jurisprudence) on organ transplantation were issued from different parts of the Muslim world. In Amman, Jordan, the International Islamic Jurist Council recognized brain death as a recognized sign of death in Islam in October 1986. In 1990 and 2003, the International Islamic Fiqh Academy and the Islamic Fiqh Academy issued important fatwas on organ transplantation.[[16]]
Despite these fatwas, various Muslim scholars' opinions on organ transplantation and brain death are far from unanimous. Opinions vary from a person's body being amānah (trust) from Allah that he/she has no right to part with any part of it, to the sacredness of the human body that considers it act of aggression against the human body, tantamount to its mutilation, if organs were to be removed after death for transplantation.[[17]] On the other hand, medical practice in Arab countries is a hybrid of several systems dependent on past prenational economic developments. This review is focused mainly on the general aspects of transplantation ethics in the Arab countries.
Materials and Methods
This is a narrative, nonsystematic review of the literature retrieved from two online databases: Scopus (Elsevier) and PubMed (National Library of Medicine, USA). The combined search term (Morocco OR Tunisia OR Algeria OR Libya OR Egypt OR Sudan OR Syria OR Lebanon OR Saudi OR Emirates OR Yemen OR Bahrain OR Kuwait OR Qatar OR Somalia OR Oman OR Jordan OR Palestine) AND (Ethics AND Transplantation) was used to identify the relevant records. No time or record type filters were applied. The initial electronic search retrieved 255 records in PubMed and 71 papers in Scopus with a very high degree of overlap. The retrieved articles were amalgamated and examined for relevance. Nonhuman studies and purely technical reports of no particular concern to the Arab countries or ethical considerations are excluded. Reference was also made to international studies with contributions from the Arab countries with relevance specific to the region. The selected articles were reviewed and narrated thematically. We have deliberately excluded particular issues related to bone marrow, stem cell work, assisted reproduction as their ethical challenges are somewhat different and would deserve a separate discussion. An initial draft was prepared, and all authors jointly developed the whole manuscript's intellectual content further using a single version loaded online on Google Docs drive. The resulting product was refined through several multilateral rounds of discussion including a couple of video conference sessions to review the final manuscript. All authors approved the final version of the manuscript before submission. The aim is to provide a concise thematic overview of the literature on the subject.
Results
Most of the publications cover kidney or liver transplantation. Several themes emerged from the review process. The themes are not preset but reflect the available literature retrieved by the authors [[Table 1]].

Organ shortage and the unresolved issue of deceased organ donation
The issue of deceased organ donation (DOD) remains problematic in the region. Patients and their families are often left to seek alternative kidney transplant routes such as buying kidneys from living unrelated donors through transplant tourism.[[17]] A review by Paris and Nour addressed the ethical use, procurement, and allocation of donor organs in Egypt. They concluded that the Egyptian system does not legally recognize brain death, which encourages illegal trade in transplant organs.[[18]] There is no consensus about the definition of brain death by the Egyptian medical community.[[19]],[[20]]
Contrary to a prevailing idea that opposition to DOD in Egypt is related to Islamic concerns, Hamdy[[21]] drew on Egypt's ethnographic fieldwork. She argued that the main problems are how to guarantee the protection of vulnerable individuals, equitable distribution of organs, and fair access to health care. However, the public is confused about Muslim scholar's stance on brain death and deceased donation. Further work is needed to educate the public and Islamic scholars on criteria and the need for brain death and DOD.
Questions about deceased donation faced by medical professionals practicing in the Arab world were addressed in a couple of studies. Muliira and Muliira conducted a literature review examining nurses' roles in working with Muslim potential deceased organ donors.[[22]] Despite manifesting several stereotypical views about Muslims and their perspectives on important issues, the authors concluded that nurses need to be educated. They need to know that organ donation is permissible by the majority of Muslim scholars despite differences in opinions.
In another study by Alwadaei et al., 12 western-educated doctors were interviewed in Bahrain; a Muslim country with dominant western culture.[[23]] The study highlighted the difficulty doctors faced in engaging nonmedical people in end-of-life decisions because of their reluctance to talk about death and ambiguity of current law regarding the boundaries of medical responsibilities. There were divergent views among doctors from those who considered end-of-life decisions purely medical to those who thought of it as purely religious. Physicians are left threading a fine line between their often western training about informed consent, for example, and a prevailing sociocultural view of “doctor knows best” (or at least should), in the presence of a rising culture of litigation.
Bioethical considerations in living organ donation
Due to a lack of DOD, living donor transplantation filled the gap in managing end-organ failure. Therefore, early ethical concerns focused on living donation. Daar et al.[[24]] proposed a classification of living donor renal transplantation under five categories: (1) living-related donation; (2) emotionally related donation; (3) altruistic donation; (4) “rewarded” gifting; and (5) rampant commercialism.[[24]] Categories 1, 2, and 3 they argued were resolved, 4 remain hotly debated (even today), while category 5 is blatantly unethical.
Qatar is a multiethnic society with differences in language, socio-economic status, and cultural barriers. This situation created a significant challenge to the growth of their kidney transplant program.[[25]],[[26]] The possible economic impact on donors and the potential for exploitation of economically disadvantaged for transplant commercialism. To protect living kidney donors (LKDs), the Organ Donation Fund was created in 2001 to compensate living donors for any costs or loss of earnings they might incur during the donation process.[[24]],[[26]]
Abdeldayem et al.[[27]] analyzed living liver donors' motives among 193 consecutive living-liver donors between 2003 and 2013 at Menoufia, Egypt. In their group of donors (mean age 26 years), two-thirds were males, offspring donating to parents were 32%, and parents to their offspring 15%. For many donors, donation seemed an attempt to reduce their anxiety and handle the fear of losing a beloved person to a life-threatening disease. For others, the wish to maintain the relationship with the recipient was a common argument often expressed by spouses. The authors could not be confident of the absence of coercion during the liver donation process but argued that serious effort is made to ensure the voluntary nature.
Wahab et al.[[28]] reported their experience of the impact of exclusion of potential LKDs from donation. 792 out of 1004 potential living liver donors were excluded in this single-center study in Mansoura, Egypt. 639 (80.7%) potential donors were excluded by the transplant team for medical or psychosocial reasons, while 18.7% withdrew themselves during the process and in 5 the family declined donation. Interestingly, 96.2% of liver transplant recipients in this study had previous experience with multiple potential donors. In the absence of deceased donor programs, searching for a potential suitable donor by simultaneously screening and evaluating multiple potential donors carries significant cost implications and can result in over emphasis on the medical criteria for living liver donation while overlooking the voluntary and altruistic nature of living donation.[[28]] The same practice may lead to potential donors be put under undue pressure, or even be coerced into donation.[[29]],[[30]]
Evaluating potential living donors is a demanding process for the potential donor, their families, and is a resource intensive endeavor. The realization rate of potential kidney donors is around 25% and identifying donors who are more likely to complete the process and end up actually donating can save significant amounts of time and effort, not to mention the anguish of all parties concerned.[[31]],[[32]]
Attitudes toward organ donation
Information about the attitudes toward organ donation in the Arab countries is the result of multiple surveys of patients, relatives, professionals, and public members.[[33]],[[34]],[[35]],[[36]],[[37]],[[38]],[[39]],[[40]],[[41]],[[42]],[[43]],[[44]] According to an extensive multicenter survey in Saudi Arabia, Bahrain, and Egypt by the Renal Transplant Study Group, end-stage renal disease patients tended to take the initiative in seeking living unrelated renal transplantation, despite physician discouragement, and the significant financial burden.[[33]]
A survey of 702 Tunisian physicians, nurses, and technicians by Tebourski et al., 59% were favorable toward organ donation.[[34]] Humane reasons were the main rationale for acceptance of organ donation, while religious reservations (26.4%), personal reasons (20.9%), and no specific reasons (22.8%) were cited for refusing organ donation. Intensive care unit staff in a tertiary in Saudi hospital were surveyed by Alsultan in 2011 when 80% of the 154 participants acknowledged that organ donation is a legal practice in Saudi Arabia, but nearly a quarter were unaware of their hospital's organ donation policy.[[35]] Only 57% were willing to donate their organs. In another study from Saudi Arabia, 698 adults attending outpatient clinics at a tertiary care hospital were surveyed about their views on various forms of consent for DOD.[[36]] The authors showed that most respondents were in favor of DOD, a mandated choice system was the most preferred and presumed consent system was the least preferred option.
A survey in Morocco targeted various officials related to organ transplantation as well as leaders of ethics committees and religious groups for their views about organ donation.[[37]] Respondents indicated their preference for promoting living organ donation initially, followed by the gradual introduction of measures to encourage DOD. It was interesting to note that respondents expressed an ambition for a rather relatively high DOD rate (30/million). A large proportion of participants (93%) suggested a “suitable moral” motivation for organ donors. In another study from Morocco, Flayou et al. studied the attitudes of the medical staff toward organ donation.[[38]] A third of respondents knew about the law that governs organ donation in Morocco. Participants expressed more willingness to donate organs after death than during their life (82 vs. 66%), and reasons for refusal of organ donation included a misunderstanding of risks, desire for respect of the corpse, in addition to religious and ethical motives.
Furthermore, Alashek et al. indicated that 30% of survey participants favored donating their organs after death, while 60% refused and 10% were undecided.[[39]] Those willing to donate tended to be young, single males with a college degree or higher, while lack of adequate knowledge about the importance of DOD and uncertainty about its religious implications were the main reasons for refusing it. The effect of educational sessions on attitudes about organ donation was studied by Hammad et al.[[40]] They surveyed 2682 adults (age 18–70 years) before and after a teaching session on brain death and organ procurement. Respondents were questioned about circumstances of death, the conditions of conversations around organ donation, and reasons for acceptance or refusal of donation. Prior to the educational session, 72.1% reported they understood brain death versus 88% after the teaching session. The concept of brain death was accepted by 64% versus 68% before and after teaching, respectively. Presumed consent was agreed to by 35% before versus 40% after the intervention. Fifty-one percent of participants thought their religion was against brain death versus 58%. While 51% wanted to carry a donor card before teaching (vs. 59% after), and those who were agreeable to consent to organ donation in case of brain death of a relative (46% before vs. 56% after), the proportion of respondents actually carrying a donor card did not change before and after the educational session (11.3%). El Hangouche et al.[[41]] evaluated the knowledge and perception of the public in Morocco toward organ donation as well as to identify the reasons and determinants for refusal of organ donation. This opinion survey included a representative sample of 2000 participants. They showed 55.2% of the participants were women, the median age was 21 years, and 60.8% of included participants had secondary education. Almost two-thirds showed a low to mid-level of knowledge about organ donation and transplantation in Morocco. About half of the participants refused to donate their organs. Concern about risk of medical error and the belief in trafficking of procured organs were the main reasons for refusal, seen in 66% and 62% of the interviewees, respectively. Regression models showed that the older, the less educated, and the less informed a person is, the less he accepted organ donation. The authors concluded that promotion of organ donation in Morocco should involve a regular information and awareness among the general population. In another study, Alam[[42]] evaluated factors affecting the knowledge and/or attitudes of the Saudi Arabian public with respect to organ donation and transplantation in a cross-sectional study on 948 participants between 20 and 60 years of age during 2005. The study revealed that 58.5% of participants heard about the existence of SCOT, 91.1% knew the need for organ donation, and 92.7 knew that organ donation could save lives. The organ donation campaign was known to 62.3% of the participants. Of these participants, 57.9% were made aware of organ donation campaigns through TV ads, 52.8% from magazines and newspapers, and 11.7% from scientific sources. While 23.7% of the participants were unaware of any issued Islamic fatwa regarding organ donation, another 36.1% did not respond to this question revealing a lack of knowledge. Forty-two percent of the respondents agreed to donate their organs after death. Among the various reasons against organ donation, 27.5% feared that the act of organ donation contradicted their religious beliefs, while 3.5% believed that there was no benefit to organ donation. It is concluded that a need for proper information dissemination exists. A multidisciplinary approach is suggested including government support backed by strong recommendations from knowledgeable religious sources. More recently, Tarzi et al.[[43]] evaluated the attitude and knowledge of organ donation among Syrians and the willingness of this population to donate their organs. A cross-sectional study in four hospitals in Aleppo, Syria in November 2019. Involved a total of 303 participants. The majority of participants (82%) heard about organ donation with television (55%), social media (25%), and the internet (25%) being the most common sources of information. When assessing knowledge about brain death, only 40% answered 3 or more questions (out of 5) correctly. Fifty-eight percent of respondents agreed with the idea of organ donation and 62% would like to donate their organs 1 day. The leading motivation to organ donation was the desire to help (77%), while the most common reason to refuse donation was the refusal to disfigure a dead body by removing an organ (41%). Religious reasons were cited as motivation for organ donation by 43% of participants and a reason for refusing to donate organs by 24% most respondents (88%) were unaware of the laws and legislations related to organ donation in Syria. When asked if religion and law were encouraging organ donation, 76% of respondents would donate their organs. Although more positive attitude was found in those with better brain death knowledge (score ≥3), this did not translate into more willingness to donate organs in this group of participants. Palestinian university students from Nablus were surveyed by Al-Labadi et al.[[44]] about their knowledge and willingness toward corneal donation.[[44]] Of the 634 students who completed the questionnaire, 93% were unaware of the existence of an eye bank, and 407 did not show willingness toward corneal donation. Disapproval by the family was the most common reason for unwillingness to donate a cornea.
Notably, several of these surveys did not seem to include questions about receiving a transplant organ for self or a close relative. Budiani-Saberi and Mostafa[[45]] identified three specific areas to be addressed in order to promote organ donation and protect living donors: Legislation to govern brain death and deceased donation, the criminalization of the buying, selling, and brokering of organs from live donors; and a sustained public education program about organ donation and brain death to target the medical, religious, academic, and legal institutions.
Outcome of commercial organ transplantation
The shortage of live donor transplant organs and the lack of DOD programs led many patients and their relatives to seek transplant organs abroad. In one study by Al Rahbi and Salmi,[[46]] unavailability of a live-related donor was the main cited reason for seeking a commercial transplant (71%). Other reasons included objection and anxiety about getting a kidney donated by a family member (13% and 9%, respectively), in addition to a perceived need for a prompt transplant (3%). Few years ago, China, Philippines, Egypt, and Pakistan were well-recognized destinations for those seeking commercial transplants. In fact, Egypt was called out by the WHO as 1 of 5 organ transplant “hot spots” in the world.[[47]] Transplant tourism has serious ethical concerns due to the exploitative nature of the practice, and the international swell of opinion against it has culminated in the Declaration of Istanbul, an international document banning the trade in human organs.[[48]],[[49]],[[50]],[[51]],[[52]],[[53]]
Several studies have reported on complications of commercial organ transplantation. In two studies predating the Declaration of Istanbul, Qunibi[[54]],[[55]] retrospectively reported on 540 patients who had received commercial renal transplantation in India between 1978 and 1993,[[54]] and compared the findings with those of 75 recipients of living-related renal transplantation performed in two participating centers in the Middle East.[[55]] Despite patient and graft survival rates being similar in recipients of commercial and local transplants, infections such as HIV and hepatitis B virus were more in the commercial transplant group. Ben Hamida et al.,[[56]] on the other hand, highlighted the poor outcome of commercial renal transplantation in twenty cases seen in Tunisia between (1995 and 1999), 14 transplanted in Iraq, and 6 between Egypt and Pakistan. All were living unrelated commercial kidney transplants costing USD 10,000 each.[[56]]
Abdeldayem et al.[[57]] reported on 15 patients who received liver transplants in China and concluded that 11 of them had no suitable donors or no donor in Egypt. Patient survival at 6 and 12 months was 80% and 73%, respectively. Four patients died, 2 while still in China, and 82% of the survivors developed complications.
By 2018, Oman, 42 living unrelated donors (LURD) commercial pediatric kidney transplants were reported over a 22-year period.[[58]] In the same report, living related donors (LRD) transplants had better patient and graft survival, and fewer surgical complications than LURD renal transplants 42.8 versuss 17.8%. A similar previous study from Oman highlighted the disruptive nature of commercial transplantation on the local transplant programs by taking the pressure off health-care officials to further develop the full array of local DD and living donor programs.[[59]]
In the post DOI era, AlBugami et al.[[32]] reported on the outcome of 86 kidney transplant tourists compared to local kidney transplants. Patient and graft 1 year survival were worse in the commercial transplant group (91% vs. 98%, P < 0.001 and 87% vs. 98%, P < 0.001, respectively).[[32]] In addition, transplanted tourists had a higher rate of acute cellular rejection (20% vs. 7%, P < 0.001), with higher rates of serious viral, bacterial, and fungal infections compared with the locals.
Living organ donors who fall victim to commercial transplant practices continue to suffer after their donation. For a start, they may have not been candidates to donate to start with, in addition to the lack of long-term care postdonation. Organizations such as the coalition for organfailure solutions try to fill this gap by conducting outreach programs that include identifying victims of organ trafficking, assessing their consequences, and arranging support services.[[60]] Paradoxically, the international ban of commercial transplantation following the DOI may have driven transplant tourism further into the black market, with such transplants now performed in appalling settings.
Beyond the declaration of Istanbul
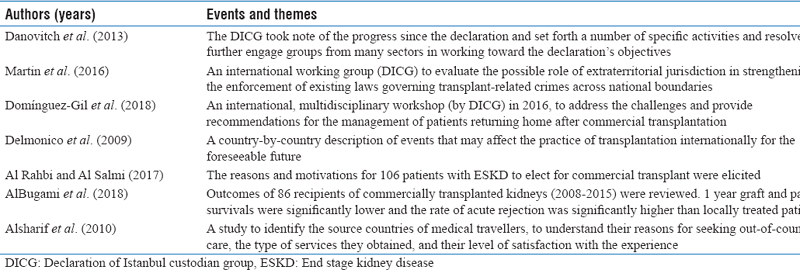
The Transplantation Society and the International Society of Nephrology developed the Declaration of Istanbul on Organ Trafficking and Transplant Tourism in May 2008.[[48]] Its principles included the condemnation of transplant commercialism, organ trafficking, and transplant tourism, and it underlined the urgency of putting the principles into action. The declaration and its principles were soon endorsed by various professional bodies and governmental organizations. The Declaration of Istanbul Custodian Group (DICG) was subsequently formed and sought to promote and uphold the DOI principles, and encouraged cooperation among professional bodies and various international and national organizations. Some of the repercussion of the declarations are presented in [[Table 2]].[[49]],[[50]],[[51]],[[52]],[[53]] For instance, at a fifth anniversary meeting in Qatar in April 2013, the DICG took note of progress made and set forth in a Communiqué a number of specific activities and resolved to further engage groups from many sectors in working toward the Declaration's objectives.[[49]] Trading in transplant organs may be a criminal offence that governments can prosecute when committed in their territories. Organ brokers, however, tend to orchestrate their activities across borders, and in parts of the world where they know they will not be prosecuted. The DICG suggested that states be encouraged to include provisions on extraterritorial jurisdiction in their laws on transplant-related crimes.[[50]] A call has also been made to encourage collaboration between professionals and international authorities to develop a global registry of transnational transplant activities.
Patients who return home after receiving commercial organ transplant abroad present health-care professionals and authorities with a challenging ethical dilemma, not to mention the medical and legal problems that arise. Duty of care dictates that such patients are provided the care posttransplant patient needs. This, however, may lead inadvertently to promoting transplant tourism by way of real-life examples. Any apparent ease with which transplant tourists are accepted back into the system of care in their home countries, may also be deleterious to local transplant programs. For patients who can afford it, why have a family member go through the donation process and part with one of their kidneys are part of their liver if they can buy it abroad, and return to seamlessly resume care at their local transplant unit. With emphasis on tracing, registration, and reporting of such episodes of commercial transplantations, the DICG suggested a set of recommendations that included the resumption of posttransplant care for returning transplant tourists.[[51]]
Expansion of the donor pool
The demand for transplant organs exceeds the supply. Such demand led to attempts to expand the donor pool to include donation after circulatory death, broader living donor criteria, and exchanged paired kidney donation.
Al Sebayel et al. 2014 reported a 7-year experience of a mobile donor action team in Riyadh, Saudi Arabia, to promote DOD.[[61]] They pursued an “aggressive approach toward organ donation through field work and provision of incentives for donors' families and the health workers dealing with the donation logistics.” Although the authors concluded this intervention had increased deceased donation rates (3-fold increase) in Riyadh, and that it is “ethically and morally accepted,” the approach raises more questions about the quality of consent obtained in such, usually, tragic circumstances associated with brain death, and of a possible moral hazard in incentivizing health professional to increase organ donation.
Shaheen et al.[[62]] argued that appointing an organ donation coordinator may result in early identification and better donor management, which may help the donor pool. The authors drew from the Spanish and US experiences of similar schemes that resulted in significant DOD improvements. Shaheen et al. concluded that the current Saudi rate of deceased donor donation of 22 possible deceased donors per million population and a 20% procurement rate can be much improved through adoption of a Saudi Proactive Detection Program.[[63]]
Other initiatives included moving to a presumed consent for deceased donors and compensation of living donors.[[64]] Both approaches come with significant ethical concerns attached. The presumed consent model raises questions about the state owning its citizens body parts after their death, and utilizing them as a national resource, in addition to raising the prospect of litigation by families who do not recognize brain death as a concept. Some find it difficult to differentiate very clearly between buying organs and payments made to organ donors, often made as compensation for loss of earnings.
A shift toward some form of reward to organ donors has become more noticeable, Qatar and the US being recent examples.[[64]] Yacoubian et al.[[65]] examined the various spectrum of donor compensation models; from reimbursing costs and lost earnings, to monetary or nonmonetary forms of appreciation without direct intention to encourage donation (rewarded gifting) to a market model. Some governments created monetarily valued and socially valued incentives for prospective living-anonymous donors. Khetpal and Mossialos reported on the case of six countries with established living-anonymous kidney donation practices included two Middle Eastern countries (Iran and Saudi Arabia).[[66]] The six countries used different packages of incentives to encourage living donation. The authors concluded that the degree of altruism expressed could be stratified into four models; with Iran occupied the least altruistic model and Saudi Arabia was among most altruistic.
Donation after cardiac death (DCD) is another strategy to expand the donor pool. This form of DOD remains shrouded in controversy in the Arab world, not least because the donation after brain death (DBD) is yet to be universally accepted in most jurisdictions in the Arab world. Hence, adding yet another form of deceased donation can be expected to lead to more confusion among the public, and possibly even among health-care workers. Both DCD and DBD approaches must comply with the “dead donor rule” in that the potential donor must be dead before organ retrieval. In addition, death must neither be caused nor hastened by the organ retrieval team.[[67]] Significant efforts lie ahead at professional and societal levels before DCD programs can be more widely acceptable in the Arab world. Reflecting on one's own personal, institutional, and national experiences, achievements, and challenges can be very rewarding.[[68]]
Islamic perspectives
The Arab countries are a Muslim-majority region. Predictably, the moral guidance on the organ transplantation will consider the religious principles and religious roots of cultural norms and practices. Several authors considered these issues from a bioethical and religious view point. A detailed discussion of the subject is beyond the scope of this review. However, a limited bibliography is included in [[Table 3]] to provide a guidance to readers on the extent of interest in this aspect of the topic. To prevent duplication, these are not included in the list of cited literature. Some of the authors focused purely on the religious aspects and others included comments on practices and how these principles are perceived and practices [[Table 3]].

Conclusions
In Arab countries, the debate on transplantation ethics continues. Various issues are remaining unresolved around DOD and living donor advocacy. Although some progress has been made in certain areas, especially with the Istanbul Declaration and its ban on the illegal practice of organ trafficking, and the call to hold perpetrators accountable for their actions, a broader dialogue between the medical community, Islamic scholars, and legislators needs to continue in order to align concepts such as brain death and donor compensation in our region. Furthermore, public trust and awareness around organ transplantation lack in many Arabic organ transplantation areas and a concerted effort is required to inform the public and further the transplant agenda.
Authors' contribution
SAB and EAE proposed the study, performed the literature searches, and drafted the manuscript. KBA lead further developments of the manuscript. All authors reviewed the whole document for intellectual content, style, and presentation. All authors approved the manuscript's final version.
Compliance with ethical principles
No ethical approval is required.
Reviewers:
Not Applicable (Commissioned Review)
Editors:
Elhadi H Aburawi (Abu Dhabi, UAE)
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Murray JE. The first successful organ transplants in man. J Am Coll Surg 2005;200:5-9.
- 2 GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020;395:709-33.
- 3 Yang CW, Harris DC, Luyckx VA, Nangaku M, Hou FF, Garcia Garcia G, et al. Global case studies for chronic kidney disease/end-stage kidney disease care. Kidney Int Suppl (2011) 2020;10:e24-48.
- 4 Bello AK, Alrukhaimi M, Ashuntantang GE, Bellorin-Font E, Benghanem Gharbi M, Braam B, et al. Global overview of health systems oversight and financing for kidney care. Kidney Int Suppl (2011) 2018;8:41-51.
- 5 Van Biesen W, Jha V, Abu-Alfa AK, Andreoli SP, Ashuntantang G, Bernieh B, et al. Considerations on equity in management of end-stage kidney disease in low- and middle-income countries. Kidney Int Suppl (2011) 2020;10:e63-71.
- 6 Fitzgerald A, Mayrhofer-Reinhartshuber D, Suske M, Fitzgerald RD. Recent thoughts about the ethics of renal transplantation. Saudi J Kidney Dis Transpl 2005;16:540-6.
- 7 Masri M, Haberal M. Solid-organ transplant activity in MESOT countries. Exp Clin Transplant 2013;11:93-8.
- 8 Freeman RB, Bernat JL. Ethical issues in organ transplantation. Prog Cardiovasc Dis 2012;55:282-9.
- 9 Daar AS. Ethical issues a Middle East perspective. Transplant Proc 1989;21:1402-4.
- 10 Abouna GM, Kumar MS, Samhan M, Dadah SK, John P, Sabawi NM. Commercialization in human organs: A middle eastern perspective. Transplant Proc 1990;22:918-21.
- 11 Bakdash T, Scheper-Hughes N. Is it ethical for patients with renal disease to purchase kidneys from the world's poor? PLoS Med 2006;3:e349.
- 12 Chamsi-Pasha H, Albar MA. Kidney transplantation: Ethical challenges in the Arab world. Saudi J Kidney Dis Transpl 2014;25:489-95.
- 13 Chamsi-Pasha H, Chamsi-Pasha MA, Albar MA. Ethical challenges of deactivation of cardiac devices in advanced heart failure. Curr Heart Fail Rep 2014;11:119-25.
- 14 Daar AS. Organ donation—world experience; the Middle East. Transplant Proc 1991;23:2505-7.
- 15 Albar M. Organ transplantation: A Sunni Islamic perspective. Saudi J Kidney Dis Transpl 2012;23:817-22.
- 16 Ebrahim AF. Organ transplantation: Contemporary Sunni Muslim legal and ethical perspectives. Bioethics 1995;9:291-302.
- 17 Daar AS. The body, the soul and organ donation: Beliefs of the major world religions. Nefrologia 1994;14:78-81.
- 18 Paris W, Nour B. Organ transplantation in Egypt. Prog Transplant 2010;20:274-8.
- 19 Hamdy S. Not quite dead: Why Egyptian doctors refuse the diagnosis of death by neurological criteria. Theor Med Bioeth 2013;34:147-60.
- 20 Daar AS, Salahudeen AK, Pingle A, Woods HF. Ethics and commerce in live donor renal transplantation: classification of the issues. Transplant Proc 1990;22:922-4.
- 21 Hamdy S. Our Bodies Belong to God: Organ Transplants, Islam, and the Struggle for Human Dignity in Egypt. Berkeley: University of California Press, 2012. ISBN 9780520271760.
- 22 Muliira RS, Muliira JK. A review of potential Muslim organ donors' perspectives on solid organ donation: Lessons for nurses in clinical practice. Nurs Forum 2014;49:59-70.
- 23 Alwadaei S, Almoosawi B, Humaidan H, Dovey S. Waiting for a miracle or best medical practice? End-of-life medical ethical dilemmas in Bahrain. J Med Ethics 2019;45:367-72.
- 24 Daar AS, Salahudeen AK, Pingle A, Woods HF. Ethics and commerce in live donor renal transplantation: Classification of the issues. Transplant Proc 1990;22:922-4.
- 25 Almaslamani Y, Almalki H, Fadhil R, Khalaf H, Asim M. Transplantation in Qatar. Transplantation 2016;100:2487-8.
- 26 Asim M, Al-Maslamani Y, Al-Malki H. Safe and ethical living kidney donation in Qatar: A national health system's approach. Qatar Med J 2017;2017:3.
- 27 Abdeldayem H, Kashkoush S, Hegab BS, Aziz A, Shoreem H, Saleh S. Analysis of donor motivations in living donor liver transplantation. Front Surg 2014;1:25.
- 28 Wahab MA, Hamed H, Salah T, Elsarraf W, Elshobary M, Sultan AM, et al. Problem of living liver donation in the absence of deceased liver transplantation program: Mansoura experience. World J Gastroenterol 2014;20:13607-14.
- 29 Al-Khader AA, Al-Sulaiman M. How to recognize an unwillng kidney donor. Saudi Med J 1992;13:1-3.
- 30 Daar AS. Living-organ donation: Time for a donor charter. Clin Transpl 1994;13:376-80.
- 31 Al-Khader AA. A model for scoring and grading willingness of a potential living related donor. J Med Ethics 2005;31:338-40.
- 32 AlBugami MM, AlOtaibe FE, Alabadi AM, Hamawi K, Bel'eed-Akkari K. Transplant tourism following the declaration of Istanbul: Poor outcomes and nephrologist dilemma. Nephrology (Carlton) 2018;23:1139-44.
- 33 Physicians attitudes toward living non-related renal transplantation (LNRRT). The Living non-Related Renal Transplant Study Group. Clin Transplant 1993;7:289-95.
- 34 Tebourski F, Jaouadi N, Ben Alaya D, Benamar-Elgaaied A, Ayed M. Attitude of health personnel to organ donation and transplantation. Tunis Med 2003;81:482-7.
- 35 Alsultan M. The perception of organ donation among health-care providers in the intensive care units at a tertiary center. Saudi J Kidney Dis Transpl 2012;23:724-8.
- 36 Hammami MM, Abdulhameed HM, Concepcion KA, Eissa A, Hammami S, Amer H, et al. Consenting options for posthumous organ donation: Presumed consent and incentives are not favored. BMC Med Ethics 2012;13:32. https://doi.org/10.1186/1472-6939-13-32.
- 37 Hachicha J, Yaich S, Charfeddine K, Masmoud M, Jarraya F, Kharrat M, et al. Living and cadaver donor transplant programs in the Maghreb. Saudi J Kidney Dis Transpl 2013;24:150-6.
- 38 Flayou K, Kouam N, Miara H, Raoundi O, Ouzeddoun N, Benamar L, et al. Attitudes toward organ donation among personnel from the University Hospital of Rabat. Saudi J Kidney Dis Transpl 2016;27:758-61.
- 39 Alashek W, Ehtuish E, Elhabashi A, Emberish W, Mishra A. Reasons for unwillingness of libyans to donate organs after death. Libyan J Med 2009;4:110-3.
- 40 Hammad S, Alnammourah M, Almahmoud F, Fawzi M, Breizat AH. Questionnaire on brain death and organ procurement. Exp Clin Transplant 2017;15:121-3.
- 41 El Hangouche AJ, Alaika O, Rkain H, Najdi A, Errguig L, Doghmi N, et al. Knowledge, attitudes, and practice of organ donation in Morocco: A cross-sectional survey. Saudi J Kidney Dis Transpl 2018;29:1358-65.
- 42 Alam AA. Public opinion on organ donation in Saudi Arabia. Saudi J Kidney Dis Transpl 2007;18:54-9.
- 43 Tarzi M, Asaad M, Tarabishi J, Zayegh O, Hamza R, Alhamid A, et al. Attitudes towards organ donation in Syria: A cross-sectional study. BMC Med Ethics 2020;21:123.
- 44 Al-Labadi L, Gammoh Y, Shehada R, Shahin R, Jbarah W, Amro M, et al. University students' knowledge of corneal donation and willingness to donate corneas in the occupied Palestinian territory: A cross-sectional study. Lancet 2018;391 Suppl 2:S22.
- 45 Budiani-Saberi D, Mostafa A. Care for commercial living donors: The experience of an NGO's outreach in Egypt. Transpl Int 2011;24:317-23.
- 46 Al Rahbi F, Al Salmi I. Commercial kidney transplantation: Attitude, knowledge, perception, and experience of recipients. Kidney Int Rep 2017;2:626-33.
- 47 Shimazono Y. The state of the international organ trade: A provisional picture based on integration of available information. Bull World Health Organ 2007;85:955-62.
- 48 Participants in the International Summit on Transplant Tourism and Organ Trafficking. The declaration of Istanbul on organ trafficking and transplant tourism. Exp Clin Transplant 2008;6:171-9.
- 49 Danovitch GM, Chapman J, Capron AM, Levin A, Abbud-Filho M, Al Mousawi M, et al. Organ trafficking and transplant tourism: The role of global professional ethical standards-the 2008 Declaration of Istanbul. Transplantation 2013;95:1306-12.
- 50 Martin DE, Van Assche K, Domínguez-Gil B, López-Fraga M, Budiani-Saberi D, Lavee J, et al. Prevention of transnational transplant-related crimes-what more can be done? Transplantation 2016;100:1776-84.
- 51 Domínguez-Gil B, Danovitch G, Martin DE, López-Fraga M, Van Assche K, Morris ML, et al. Declaration of Istanbul Custodian Group working group on ethical travel for transplantation. Management of patients who receive an organ transplant abroad and return home for follow-up care: Recommendations from the declaration of Istanbul custodian group. Transplantation 2018;102:e2-9.
- 52 Delmonico FL. The implications of Istanbul declaration on organ trafficking and transplant tourism. Curr Opin Organ Transplant 2009;14:116-9.
- 53 Alsharif MJ, Labonté R, Lu Z. Patients beyond borders: A study of medical tourists in four countries. Global Soc Policy 2010;10:315-35.
- 54 Commercially motivated renal transplantation: Results in 540 patients transplanted in India. The Living Non-Related Renal Transplant Study Group. Clin Transplant 1997;11:536-44.
- 55 Qunibi WY. Commercial renal transplantation: Clinical and ethical issues. Ann Saudi Med 1994;14:1-4.
- 56 Ben Hamida F, Ben Abdallah T, Goucha R, Hedri H, Helal I, Karoui C, et al. Outcome of living unrelated (commercial) renal transplantation: Report of 20 cases. Transplant Proc 2001;33:2660-1.
- 57 Abdeldayem HM, Salama I, Soliman S, Gameel K, Gabal AA, El Ella KA, et al. Patients seeking liver transplant turn to China: Outcomes of 15 Egyptian patients who went to China for a deceased-donor liver transplant. Exp Clin Transplant 2008;6:194-8.
- 58 Al Riyami MS, Al Saidi S, Al Ghaithi B, Al Maskari A, Lala S, Mohsin N, et al. Pediatric renal transplantation in Oman: A single-center experience. Oman Med J 2018;33:7-14.
- 59 Mohsin N, Al-Busaidy Q, Al-Marhuby H, Al-Lawati J, Daar AS. Deceased donor renal transplantation and the disruptive effect of commercial transplants: The experience of Oman. Indian J Med Ethics 2014;11:153-6.
- 60 Budiani-Saberi D, Columb S. A human rights approach to human trafficking for organ removal. Med Health Care Philos 2013;16:897-914.
- 61 Al Sebayel M, Alenazi AM, Sabbagh R, Al Ageel T, Al Enazi M, Al Bahili H, et al. Donor organ shortage crisis: A case study review of a financial incentive-based system. Transplant Proc 2014;46:2030-5.
- 62 Shaheen FA, Souqiyyeh MZ, Attar B, Ibrahim A, Alsayyari A. Organ donation from deceased donors: A proactive detection program in Saudi Arabia. Exp Clin Transplant 2015;13 Suppl 3:1-3.
- 63 SCOT Data. Organ transplantation in Saudi Arabia-2013. Saudi J Kidney Dis Transpl 2014;25:1359-68.
- 64 Khedmat H, Taheri S. Ethical disputes in living donor kidney transplantation: What should we do to save lives? Saudi J Kidney Dis Transpl 2010;21:971-4.
- 65 Yacoubian AA, Dargham RA, Khauli RB. A review of the possibility of adopting financially driven live donor kidney transplantation. Int Braz J Urol 2018;44:1071-80.
- 66 Khetpal V, Mossialos E. An ethical appraisal of living-anonymous kidney donation using Adam Smith's Theory of Moral Sentiments. Health Policy 2018;122:1212-21.
- 67 Zamperetti N, Bellomo R, Ronco C. Defining death in non-heart beating organ donors. J Med Ethics 2003;29:182-5.
- 68 Zmerli S. History, law and ethics of kidney transplantation through my experience of 60 patients. Tunis Med 2009;87:3-5.
Corresponding author
Publikationsverlauf
Eingereicht: 22. Februar 2021
Angenommen: 22. Februar 2021
Artikel online veröffentlicht:
14. Juli 2022
© 2021. The Libyan Authority of Scientific Research and Technologyand the Libyan Biotechnology Research Center. All rights reserved. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License,permitting copying and reproductionso long as the original work is given appropriate credit. Contents may not be used for commercial purposes, oradapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Murray JE. The first successful organ transplants in man. J Am Coll Surg 2005;200:5-9.
- 2 GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020;395:709-33.
- 3 Yang CW, Harris DC, Luyckx VA, Nangaku M, Hou FF, Garcia Garcia G, et al. Global case studies for chronic kidney disease/end-stage kidney disease care. Kidney Int Suppl (2011) 2020;10:e24-48.
- 4 Bello AK, Alrukhaimi M, Ashuntantang GE, Bellorin-Font E, Benghanem Gharbi M, Braam B, et al. Global overview of health systems oversight and financing for kidney care. Kidney Int Suppl (2011) 2018;8:41-51.
- 5 Van Biesen W, Jha V, Abu-Alfa AK, Andreoli SP, Ashuntantang G, Bernieh B, et al. Considerations on equity in management of end-stage kidney disease in low- and middle-income countries. Kidney Int Suppl (2011) 2020;10:e63-71.
- 6 Fitzgerald A, Mayrhofer-Reinhartshuber D, Suske M, Fitzgerald RD. Recent thoughts about the ethics of renal transplantation. Saudi J Kidney Dis Transpl 2005;16:540-6.
- 7 Masri M, Haberal M. Solid-organ transplant activity in MESOT countries. Exp Clin Transplant 2013;11:93-8.
- 8 Freeman RB, Bernat JL. Ethical issues in organ transplantation. Prog Cardiovasc Dis 2012;55:282-9.
- 9 Daar AS. Ethical issues a Middle East perspective. Transplant Proc 1989;21:1402-4.
- 10 Abouna GM, Kumar MS, Samhan M, Dadah SK, John P, Sabawi NM. Commercialization in human organs: A middle eastern perspective. Transplant Proc 1990;22:918-21.
- 11 Bakdash T, Scheper-Hughes N. Is it ethical for patients with renal disease to purchase kidneys from the world's poor? PLoS Med 2006;3:e349.
- 12 Chamsi-Pasha H, Albar MA. Kidney transplantation: Ethical challenges in the Arab world. Saudi J Kidney Dis Transpl 2014;25:489-95.
- 13 Chamsi-Pasha H, Chamsi-Pasha MA, Albar MA. Ethical challenges of deactivation of cardiac devices in advanced heart failure. Curr Heart Fail Rep 2014;11:119-25.
- 14 Daar AS. Organ donation—world experience; the Middle East. Transplant Proc 1991;23:2505-7.
- 15 Albar M. Organ transplantation: A Sunni Islamic perspective. Saudi J Kidney Dis Transpl 2012;23:817-22.
- 16 Ebrahim AF. Organ transplantation: Contemporary Sunni Muslim legal and ethical perspectives. Bioethics 1995;9:291-302.
- 17 Daar AS. The body, the soul and organ donation: Beliefs of the major world religions. Nefrologia 1994;14:78-81.
- 18 Paris W, Nour B. Organ transplantation in Egypt. Prog Transplant 2010;20:274-8.
- 19 Hamdy S. Not quite dead: Why Egyptian doctors refuse the diagnosis of death by neurological criteria. Theor Med Bioeth 2013;34:147-60.
- 20 Daar AS, Salahudeen AK, Pingle A, Woods HF. Ethics and commerce in live donor renal transplantation: classification of the issues. Transplant Proc 1990;22:922-4.
- 21 Hamdy S. Our Bodies Belong to God: Organ Transplants, Islam, and the Struggle for Human Dignity in Egypt. Berkeley: University of California Press, 2012. ISBN 9780520271760.
- 22 Muliira RS, Muliira JK. A review of potential Muslim organ donors' perspectives on solid organ donation: Lessons for nurses in clinical practice. Nurs Forum 2014;49:59-70.
- 23 Alwadaei S, Almoosawi B, Humaidan H, Dovey S. Waiting for a miracle or best medical practice? End-of-life medical ethical dilemmas in Bahrain. J Med Ethics 2019;45:367-72.
- 24 Daar AS, Salahudeen AK, Pingle A, Woods HF. Ethics and commerce in live donor renal transplantation: Classification of the issues. Transplant Proc 1990;22:922-4.
- 25 Almaslamani Y, Almalki H, Fadhil R, Khalaf H, Asim M. Transplantation in Qatar. Transplantation 2016;100:2487-8.
- 26 Asim M, Al-Maslamani Y, Al-Malki H. Safe and ethical living kidney donation in Qatar: A national health system's approach. Qatar Med J 2017;2017:3.
- 27 Abdeldayem H, Kashkoush S, Hegab BS, Aziz A, Shoreem H, Saleh S. Analysis of donor motivations in living donor liver transplantation. Front Surg 2014;1:25.
- 28 Wahab MA, Hamed H, Salah T, Elsarraf W, Elshobary M, Sultan AM, et al. Problem of living liver donation in the absence of deceased liver transplantation program: Mansoura experience. World J Gastroenterol 2014;20:13607-14.
- 29 Al-Khader AA, Al-Sulaiman M. How to recognize an unwillng kidney donor. Saudi Med J 1992;13:1-3.
- 30 Daar AS. Living-organ donation: Time for a donor charter. Clin Transpl 1994;13:376-80.
- 31 Al-Khader AA. A model for scoring and grading willingness of a potential living related donor. J Med Ethics 2005;31:338-40.
- 32 AlBugami MM, AlOtaibe FE, Alabadi AM, Hamawi K, Bel'eed-Akkari K. Transplant tourism following the declaration of Istanbul: Poor outcomes and nephrologist dilemma. Nephrology (Carlton) 2018;23:1139-44.
- 33 Physicians attitudes toward living non-related renal transplantation (LNRRT). The Living non-Related Renal Transplant Study Group. Clin Transplant 1993;7:289-95.
- 34 Tebourski F, Jaouadi N, Ben Alaya D, Benamar-Elgaaied A, Ayed M. Attitude of health personnel to organ donation and transplantation. Tunis Med 2003;81:482-7.
- 35 Alsultan M. The perception of organ donation among health-care providers in the intensive care units at a tertiary center. Saudi J Kidney Dis Transpl 2012;23:724-8.
- 36 Hammami MM, Abdulhameed HM, Concepcion KA, Eissa A, Hammami S, Amer H, et al. Consenting options for posthumous organ donation: Presumed consent and incentives are not favored. BMC Med Ethics 2012;13:32. https://doi.org/10.1186/1472-6939-13-32.
- 37 Hachicha J, Yaich S, Charfeddine K, Masmoud M, Jarraya F, Kharrat M, et al. Living and cadaver donor transplant programs in the Maghreb. Saudi J Kidney Dis Transpl 2013;24:150-6.
- 38 Flayou K, Kouam N, Miara H, Raoundi O, Ouzeddoun N, Benamar L, et al. Attitudes toward organ donation among personnel from the University Hospital of Rabat. Saudi J Kidney Dis Transpl 2016;27:758-61.
- 39 Alashek W, Ehtuish E, Elhabashi A, Emberish W, Mishra A. Reasons for unwillingness of libyans to donate organs after death. Libyan J Med 2009;4:110-3.
- 40 Hammad S, Alnammourah M, Almahmoud F, Fawzi M, Breizat AH. Questionnaire on brain death and organ procurement. Exp Clin Transplant 2017;15:121-3.
- 41 El Hangouche AJ, Alaika O, Rkain H, Najdi A, Errguig L, Doghmi N, et al. Knowledge, attitudes, and practice of organ donation in Morocco: A cross-sectional survey. Saudi J Kidney Dis Transpl 2018;29:1358-65.
- 42 Alam AA. Public opinion on organ donation in Saudi Arabia. Saudi J Kidney Dis Transpl 2007;18:54-9.
- 43 Tarzi M, Asaad M, Tarabishi J, Zayegh O, Hamza R, Alhamid A, et al. Attitudes towards organ donation in Syria: A cross-sectional study. BMC Med Ethics 2020;21:123.
- 44 Al-Labadi L, Gammoh Y, Shehada R, Shahin R, Jbarah W, Amro M, et al. University students' knowledge of corneal donation and willingness to donate corneas in the occupied Palestinian territory: A cross-sectional study. Lancet 2018;391 Suppl 2:S22.
- 45 Budiani-Saberi D, Mostafa A. Care for commercial living donors: The experience of an NGO's outreach in Egypt. Transpl Int 2011;24:317-23.
- 46 Al Rahbi F, Al Salmi I. Commercial kidney transplantation: Attitude, knowledge, perception, and experience of recipients. Kidney Int Rep 2017;2:626-33.
- 47 Shimazono Y. The state of the international organ trade: A provisional picture based on integration of available information. Bull World Health Organ 2007;85:955-62.
- 48 Participants in the International Summit on Transplant Tourism and Organ Trafficking. The declaration of Istanbul on organ trafficking and transplant tourism. Exp Clin Transplant 2008;6:171-9.
- 49 Danovitch GM, Chapman J, Capron AM, Levin A, Abbud-Filho M, Al Mousawi M, et al. Organ trafficking and transplant tourism: The role of global professional ethical standards-the 2008 Declaration of Istanbul. Transplantation 2013;95:1306-12.
- 50 Martin DE, Van Assche K, Domínguez-Gil B, López-Fraga M, Budiani-Saberi D, Lavee J, et al. Prevention of transnational transplant-related crimes-what more can be done? Transplantation 2016;100:1776-84.
- 51 Domínguez-Gil B, Danovitch G, Martin DE, López-Fraga M, Van Assche K, Morris ML, et al. Declaration of Istanbul Custodian Group working group on ethical travel for transplantation. Management of patients who receive an organ transplant abroad and return home for follow-up care: Recommendations from the declaration of Istanbul custodian group. Transplantation 2018;102:e2-9.
- 52 Delmonico FL. The implications of Istanbul declaration on organ trafficking and transplant tourism. Curr Opin Organ Transplant 2009;14:116-9.
- 53 Alsharif MJ, Labonté R, Lu Z. Patients beyond borders: A study of medical tourists in four countries. Global Soc Policy 2010;10:315-35.
- 54 Commercially motivated renal transplantation: Results in 540 patients transplanted in India. The Living Non-Related Renal Transplant Study Group. Clin Transplant 1997;11:536-44.
- 55 Qunibi WY. Commercial renal transplantation: Clinical and ethical issues. Ann Saudi Med 1994;14:1-4.
- 56 Ben Hamida F, Ben Abdallah T, Goucha R, Hedri H, Helal I, Karoui C, et al. Outcome of living unrelated (commercial) renal transplantation: Report of 20 cases. Transplant Proc 2001;33:2660-1.
- 57 Abdeldayem HM, Salama I, Soliman S, Gameel K, Gabal AA, El Ella KA, et al. Patients seeking liver transplant turn to China: Outcomes of 15 Egyptian patients who went to China for a deceased-donor liver transplant. Exp Clin Transplant 2008;6:194-8.
- 58 Al Riyami MS, Al Saidi S, Al Ghaithi B, Al Maskari A, Lala S, Mohsin N, et al. Pediatric renal transplantation in Oman: A single-center experience. Oman Med J 2018;33:7-14.
- 59 Mohsin N, Al-Busaidy Q, Al-Marhuby H, Al-Lawati J, Daar AS. Deceased donor renal transplantation and the disruptive effect of commercial transplants: The experience of Oman. Indian J Med Ethics 2014;11:153-6.
- 60 Budiani-Saberi D, Columb S. A human rights approach to human trafficking for organ removal. Med Health Care Philos 2013;16:897-914.
- 61 Al Sebayel M, Alenazi AM, Sabbagh R, Al Ageel T, Al Enazi M, Al Bahili H, et al. Donor organ shortage crisis: A case study review of a financial incentive-based system. Transplant Proc 2014;46:2030-5.
- 62 Shaheen FA, Souqiyyeh MZ, Attar B, Ibrahim A, Alsayyari A. Organ donation from deceased donors: A proactive detection program in Saudi Arabia. Exp Clin Transplant 2015;13 Suppl 3:1-3.
- 63 SCOT Data. Organ transplantation in Saudi Arabia-2013. Saudi J Kidney Dis Transpl 2014;25:1359-68.
- 64 Khedmat H, Taheri S. Ethical disputes in living donor kidney transplantation: What should we do to save lives? Saudi J Kidney Dis Transpl 2010;21:971-4.
- 65 Yacoubian AA, Dargham RA, Khauli RB. A review of the possibility of adopting financially driven live donor kidney transplantation. Int Braz J Urol 2018;44:1071-80.
- 66 Khetpal V, Mossialos E. An ethical appraisal of living-anonymous kidney donation using Adam Smith's Theory of Moral Sentiments. Health Policy 2018;122:1212-21.
- 67 Zamperetti N, Bellomo R, Ronco C. Defining death in non-heart beating organ donors. J Med Ethics 2003;29:182-5.
- 68 Zmerli S. History, law and ethics of kidney transplantation through my experience of 60 patients. Tunis Med 2009;87:3-5.