

Subscribe to RSS
DOI: 10.4103/ijmbs.ijmbs_64_19
Procalcitonin and other inflammatory markers in patients with sepsis and septic shock: A single-center experience
Authors

Objective: The objective of the study was to compare the diagnostic value of serum procalcitonin (PCT), C-reactive protein (CRP), lactic acid, and white blood cells (WBC) as markers of sepsis in critically ill patients in the main tertiary hospital in Qatar. Materials and Methods: The PCT levels and other inflammatory markers (CRP, lactic acid, and WBC) were retrospectively reviewed in 137 consecutive adult patients with a suspected diagnosis of sepsis who admitted to the Internal Medicine inpatient service (i.e., Medical Wards and Medical Intensive Care Unit) at Hamad General Hospital, Qatar. The serum PCT was measured by chemiluminescence immunoassay and the results were compared with commonly used inflammatory markers between the patients with and without proven sepsis. Results: A significantly higher PCT level was observed among patients with severe sepsis and septic shock compared to those without sepsis (19.34 ± 50 and 25.91 ± 61.3 vs. 4.72 ± 10, respectively; P = 0.011). No significant differences were found in CRP and WBC between these groups. Nonsurvivors of both septic and nonseptic groups had a mean PCT level of 22.48 ± 8.26 significantly higher than that measured in survivors of both the groups (P = 0.01), a difference not evident in other inflammatory parameters. Conclusions: PCT is a highly efficient inflammatory laboratory parameter for the diagnosis of severe sepsis and septic shock, but WBC and CRP levels were of little value. PCT value assists in the diagnosis of septic shock, hence supporting appropriate disposition of patients. The levels of PCT also have prognostic implications with regard to mortality suggesting intensification of antibiotic therapy and supportive measures including appropriate family counseling.
Introduction
Sepsis, severe sepsis, and septic shock are the spectra of the deleterious host response to infection. Even with optimal treatment, mortality due to severe sepsis or septic shock is approximately 40% and can exceed 50% in the sickest patients.[[1]] Patients with systemic infection and organ dysfunction or shock are often difficult to distinguish from patients with similar clinical signs and laboratory finding but without infection.
Serum procalcitonin (PCT), normally produced in the C-cells of the thyroid gland, is the precursor of calcitonin. A specific protease cleaves serum PCT to calcitonin, catacalcin, and an N-terminal residue. Normally, PCT is not released into the blood as it is all cleaved, and hence, they are undetectable in healthy individuals and its level increases in severe infections. In these conditions, serum PCT is probably produced by extra-thyroid tissues as high levels of PCT are found even in those patients who have undergone total thyroidectomy. Parenchymal cells (including the kidney, liver, lung, muscles, and adipocytes) provide the main source of circulating PCT in sepsis.[[2]] PCT is detec[[Table 3]]–4 h after an inflammatory stimulus and peaks at 14 h and the remaining elevated for 24 h, with a half-life in the serum of 22–35 h.[[3]] The pathophysiological role of serum PCT during sepsis is not clear.[[4]],[[5]]
PCT has been studied extensively, and its efficacy as a marker of bacterial infection and critical illness has been proved. As positive bacteriological results may be caused by contamination and negative results do not exclude sepsis, a sensitive biomarker helps to guide treatment decisions.
In Qatar, there has been a large expat population from different parts of the world. The aim of the present study was to assess the efficacy of PCT and compare it with routinely used inflammatory markers (i.e., C-reactive protein [CRP], lactic acid, and white blood cells [WBC] count) for the diagnosis and prognosis and compare their clinically informative values in these patients.
Materials and Methods
This retrospective observational study was conducted at Hamad General Hospital, Hamad Medical Corporation, Qatar. The PCT levels and routinely used inflammatory markers (i.e., CRP, lactic acid, and WBC) were measured in 137 consecutive adult patients with a suspected diagnosis of sepsis who admitted to the Internal Medicine Inpatient Service (i.e., Medical Wards and/or Medical Intensive Care Unit) during the period. The inclusion criteria to the study include: (1) adult patients above 18 years of age, (2) the laboratory data for the inflammatory markers including PCT were collected at the time of hospital admission before specific treatment inform of antibiotics was started, and (3) data were collected also at least twice a week during the whole hospital stay. Patients with liver cirrhosis and/or on hemo- or peritoneal dialysis were excluded from the study due to the conflicting evidence on cutoff value of PCT in cirrhotic patients[[6]] and variation of PCT values in relation to dialysis.[[7]] The serum PCT was measured by chemiluminescent immunoassay, and its cutoff value for sepsis at our center was 0.5 ng/ml. Demographic characteristics, underlying etiology, microbiology data, and biochemical markers were the main study parameters. Data were collected using an approved form, and the study was approved by the Ethical Committee of Hamad Medical Corporation (Approval #13282/13). Systemic inflammatory response syndrome (SIRS) is diagnosed in the presence of more than one of the following: (1) temperature higher than 38°C or lower than heart rate or higher than 90 beats/min and (2) hyperventilation evidenced by respiratory rate higher than 20/min or arterial partial pressure of arterial carbon dioxide lower than 32 mmHg. Sepsis defined as SIRS plus infection. Septic shock is defined as sepsis with arterial hypotension despite adequate resuscitation.[[8]]
Statistical analysis
Descriptive statistics in the form of mean, standard deviations (SD), and frequency with percentages were calculated for interval and categorical variables, respectively. Chi-square tests between categorical variables and Student's t-test for interval variables as appropriate were performed. Multivariable logistic regression analysis was used for prediction for different biomarkers. P (two-tailed) <0.05 was considered as statistically significant level. SPSS software version 19 (IBM, New York city, NY, USA) was used for the analysis.
Results
The cohort comprised 137 patients to the hospital with a suspected diagnosis of infection. Further hospital workup revealed that 127 patients (92.7%) had proven sepsis (37 with sepsis and 76 with septic shock) compared with 10 patients (7.3%) without sepsis who were considered as patients with SIRS. There were 88 males (64.2%) and 49 females (35.8%). The mean age ± SD was 56.5 ± 19.7 years. The demographic analysis revealed a higher mean age in the infected group that was statistically significant (57.9 ± 19.2 vs. 38.4 ± 17.8, respectively, P = 0.002) and those with multiple comorbidities (two or more) were more prone to develop infections. The detailed demographic and clinical characteristics as well as biochemical markers of the studied cohort are shown in [[Table 1]]. Patients with proven sepsis had longer median hospital length of stay than nonproven sepsis patients (7 days vs. 24 days, respectively, P = 0.000). The serum PCT results were compared with other inflammatory markers between the patients with and without proven sepsis [[Table 1]]. Overall, the PCT level was significantly higher in the proven sepsis group compared with nonproven sepsis group (19.3 ± 50.2 vs. 4.7 ± 10, respectively, P = 0.011).

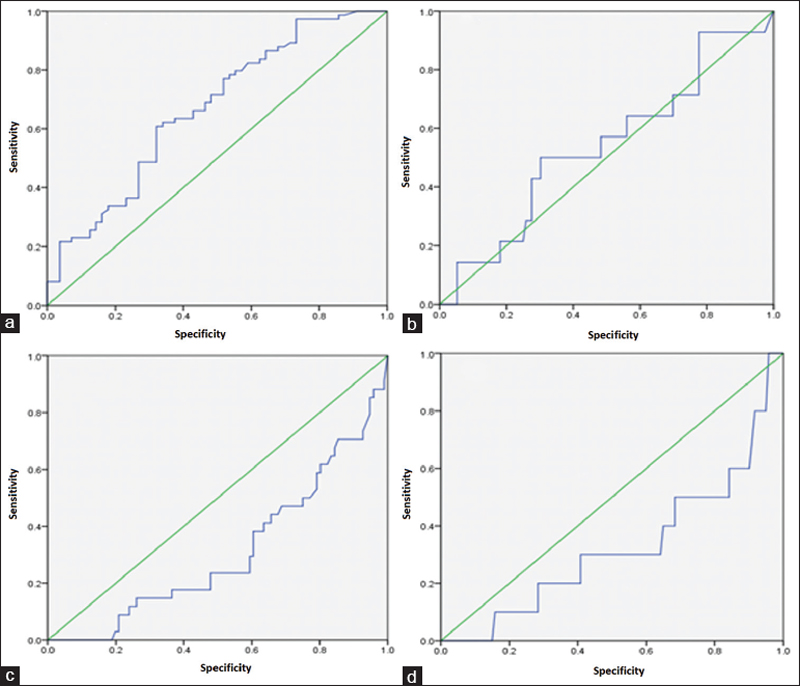
When the cohort was sub-grouped into SIRS (noninfected) and infected (sepsis, severe sepsis, and septic shock) [[Table 2]] and [[Table 3]], a significantly higher PCT level was observed among the infected patients with severe sepsis and septic shock compared to the noninfected (19.34 ± 50 and 25.91 ± 61.3 vs. 4.72 ± 10, respectively; P = 0.01). No significant differences were observed in CRP, lactic acid, and WBC between these groups. There was a trend to an increased mean and cutoff values of all biochemical parameters in septic shock patients in comparison to severe sepsis and sepsis, although this trend was not approached the statistical significance. The significant difference was seen only in lactic acid between sepsis and septic shock patients (P = 0.006) [[Table 4]] and [[Figure 1]].



Nonsurvivors of both septic and nonseptic groups had a mean PCT level of 22.48 ± 8.26 that significantly higher than that measured in survivors of both the groups (P = 0.01), a difference not evident in other inflammatory parameters. PCT values failed to reveal a decreasing trend in nonsurvivors [[Figure 2]].

In the infected patients, Gram-negative bacteria were the most common organisms detected from blood, urine, sputum, peritoneal fluid, and liver abscess aspirates (Klebsiella pneumoniae, Escherichia coli, and Pseudomonas aeruginosa mainly) followed by Gram-positive organism (Streptococcus species and Staphylococcus aureus mainly) and fungus.
Discussion
In the present study, a higher percentage of male than female patients with sepsis was found. Martin et al.[[9]] studied the demography, temporal incidence, and changes in incidence and outcome of sepsis over 20 years in the United States who reported that sepsis was more common in men, accounting for 48.1% of cases on average per year and men were more likely to have sepsis than women with a mean annual relative risk of 1.28. We found that the mean age of the patients is higher in the sepsis group than in the non-sepsis group which was expected since immunity decreaseswith age. Pneumonia was the most common source in the infected group (38%) than in the noninfected group (2%). According to Calandra et al.,[[10]] six common infection sites identified in the causation of sepsis were pneumonia, bloodstream infections including infective endocarditis, intravascular catheter-related sepsis, intra-abdominal infections, urosepsis, and surgical wound infections.
Higher acute physiology and chronic health evaluation (APACHE) and sepsis-related organ failure assessment (SOFA) scores were noted in patients progressing through the spectrum of sepsis, severe sepsis, and septic shock, and PCT was higher in patients with higher severity scores. The sensitivity and specificity of PCT are low to diagnose infection as the attributing cause for SIRS. Similar findings were found in a meta-analysis where larger studies revealed sensitivity and specificity as low as 42% and 48%, respectively, despite which they concluded that PCT should be included in the diagnostic guidelines for sepsis.[[11]]
Mortality in our series was also higher in the infected than the noninfected group, with a percentage rate of 33%. Previous reports have shown that mortality in patients with sepsis was varied between 16.8% and 34%.[[9]],[[12]] Our findings of an increasing trend of PCT monitored every 48–72 h revealed a significantly higher mortality rate in the infected than noninfected group and that may suggest an important prognostic value of PCT as an indicator of poor prognosis in uncontrolled septic patients. In a large prospective study, daily PCT was measured in 472 critical care patients and correlated the results with all-cause mortality in a 90-day study period.[[13]] They found that a high maximum PCT and an increase of PCT value following the first reading >1.0 ng/mL were both independent predictors of 90-day mortality. The relative risk of mortality increased daily as the PCT value continue to rise after the fi rst reading >1.0 ng/mL: 1.8 (95% confi dence interval [CI] 1.4–2.4) for 1 day; 2.2 (95% CI 1.6–3.0) for 2 days; and 2.8 (95% CI 2.0–3.8) for 3 days. Although APACHE and SOFA scores are also higher and correlate with mortality, they are mainly used for research purposes, and hence, PCT, a rapidly available biochemical test, can assist in intensification of therapy and day-to-day decision-making.
Conclusions
PCT is a highly efficient inflammatory laboratory parameter for the diagnosis of severe sepsis and septic shock and might be used as an indicator of poor prognosis in uncontrolled septic patients, but WBC and CRP levels were of little value.
Authors' contributions
All the authors contributed to the study conception, its planning, data collection, and analysis. They have developed their assigned parts of the manuscript and reviewed the other parts. All the authors reviewed and agreed the final version of the manuscript.
Compliance with ethical principles
The study was approved by the Research Ethical Committee of Hamad Medical Corporation, Doha, Qatar and all participants provided informed consent.
Reviewers:
Elmukhtar Habas (Tripoli, Libya)
Marwan Muhammad (Columbus OH, USA)
Sean Kelly (Columbus OH, USA)
Editors:
Salem A Beshyah (Abu Dhabi, UAE)
Conflict of Interest
There are no conflicts of interest.
Acknowledgments
The study was funded by a grant from the Medical Research Department, Hamad Medical Corporation, Qatar (#13282/13).
Financial support and sponsorship
Nil.
-
References
- 1 Sasse KC, Nauenberg E, Long A, Anton B, Tucker HJ, Hu TW. Long-term survival after intensive care unit admission with sepsis. Crit Care Med 1995;23:1040-7.
- 2 Christ-Crain M, Müller B. Procalcitonin in bacterial infections--hype, hope, more or less? Swiss Med Wkly 2005;135:451-60.
- 3 Reinhart K, Karzai W, Meisner M. Procalcitonin as a marker of the systemic inflammatory response to infection. Intensive Care Med 2000;26:1193-200.
- 4 Meisner M. The prognostic value of procalcitonin. In: Meisner M, editor. Procalcitonin (PCT). A New, Innovative Infection Parameter. Biochemical and Clinical Aspects. 3rd ed. New York: Thieme Publishers; 2000. p. 63-8.
- 5 Becker KL, Nylén ES, White JC, Müller B, Snider RH Jr. Clinical review 167: Procalcitonin and the calcitonin gene family of peptides in inflammation, infection, and sepsis: A journey from calcitonin back to its precursors. J Clin Endocrinol Metab 2004;89:1512-25.
- 6 Elefsiniotis IS, Skounakis M, Vezali E, Pantazis KD, Petrocheilou A, Pirounaki M, et al. Clinical significance of serum procalcitonin levels in patients with acute or chronic liver disease. Eur J Gastroenterol Hepatol 2006;18:525-30.
- 7 Herget-Rosenthal S, Klein T, Marggraf G, Hirsch T, Jakob HG, Philipp T, et al. Modulation and source of procalcitonin in reduced renal function and renal replacement therapy. Scand J Immunol 2005;61:180-6.
- 8 Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016;315:801-10.
- 9 Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 2003;348:1546-54.
- 10 Calandra T, Cohen J; International Sepsis Forum Definition of Infection in the ICU Consensus Conference. The international sepsis forum consensus conference on definitions of infection in the intensive care unit. Crit Care Med 2005;33:1538-48.
- 11 Uzzan B, Cohen R, Nicolas P, Cucherat M, Perret GY. Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: A systematic review and meta-analysis. Crit Care Med 2006;34:1996-2003.
- 12 Sands KE, Bates DW, Lanken PN, Graman PS, Hibberd PL, Kahn KL, et al. Epidemiology of sepsis syndrome in 8 academic medical centers. JAMA 1997;278:234-40.
- 13 Jensen JU, Heslet L, Jensen TH, Espersen K, Steffensen P, Tvede M. Procalcitonin increase in early identification of critically ill patients at high risk of mortality. Crit Care Med 2006;34:2596-602.
Corresponding author
Publication History
Received: 21 October 2019
Accepted: 25 November 2019
Article published online:
07 July 2022
© 2019. The Libyan Authority of Scientific Research and Technologyand the Libyan Biotechnology Research Center. All rights reserved. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License,permitting copying and reproductionso long as the original work is given appropriate credit. Contents may not be used for commercial purposes, oradapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Sasse KC, Nauenberg E, Long A, Anton B, Tucker HJ, Hu TW. Long-term survival after intensive care unit admission with sepsis. Crit Care Med 1995;23:1040-7.
- 2 Christ-Crain M, Müller B. Procalcitonin in bacterial infections--hype, hope, more or less? Swiss Med Wkly 2005;135:451-60.
- 3 Reinhart K, Karzai W, Meisner M. Procalcitonin as a marker of the systemic inflammatory response to infection. Intensive Care Med 2000;26:1193-200.
- 4 Meisner M. The prognostic value of procalcitonin. In: Meisner M, editor. Procalcitonin (PCT). A New, Innovative Infection Parameter. Biochemical and Clinical Aspects. 3rd ed. New York: Thieme Publishers; 2000. p. 63-8.
- 5 Becker KL, Nylén ES, White JC, Müller B, Snider RH Jr. Clinical review 167: Procalcitonin and the calcitonin gene family of peptides in inflammation, infection, and sepsis: A journey from calcitonin back to its precursors. J Clin Endocrinol Metab 2004;89:1512-25.
- 6 Elefsiniotis IS, Skounakis M, Vezali E, Pantazis KD, Petrocheilou A, Pirounaki M, et al. Clinical significance of serum procalcitonin levels in patients with acute or chronic liver disease. Eur J Gastroenterol Hepatol 2006;18:525-30.
- 7 Herget-Rosenthal S, Klein T, Marggraf G, Hirsch T, Jakob HG, Philipp T, et al. Modulation and source of procalcitonin in reduced renal function and renal replacement therapy. Scand J Immunol 2005;61:180-6.
- 8 Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016;315:801-10.
- 9 Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 2003;348:1546-54.
- 10 Calandra T, Cohen J; International Sepsis Forum Definition of Infection in the ICU Consensus Conference. The international sepsis forum consensus conference on definitions of infection in the intensive care unit. Crit Care Med 2005;33:1538-48.
- 11 Uzzan B, Cohen R, Nicolas P, Cucherat M, Perret GY. Procalcitonin as a diagnostic test for sepsis in critically ill adults and after surgery or trauma: A systematic review and meta-analysis. Crit Care Med 2006;34:1996-2003.
- 12 Sands KE, Bates DW, Lanken PN, Graman PS, Hibberd PL, Kahn KL, et al. Epidemiology of sepsis syndrome in 8 academic medical centers. JAMA 1997;278:234-40.
- 13 Jensen JU, Heslet L, Jensen TH, Espersen K, Steffensen P, Tvede M. Procalcitonin increase in early identification of critically ill patients at high risk of mortality. Crit Care Med 2006;34:2596-602.