Keywords
Head and neck - malignant germ cell tumor - yolk sac tumor
Introduction
Yolk sac tumor (YST) also known as “endodermal sinus tumor” is the most common malignant
germ cell tumor involving gonads. Although rare, these tumors are also known to arise
from an extragonadal site including the head and neck region. While sharing a report
of a large YST of temporal region in a 3-year-old boy, we are highlighting certain
peculiarities of YST in the head and neck region.
Case Report
A 3-year-old boy presented with a painless, progressive swelling in the right temporal
region for the past 1 year. The swelling of 15 cm × 10 cm was involving temporal region,
infratemporal fossa, and parotid region, giving the appearance of a conjoint second
head as shown radiologically in [Figure 1]. Open biopsy from the lesion showed mixed germ cell tumor consisting of teratoma
and YST. Whole-body positron emission tomography ruled out metastasis. He was given
five cycles of cisplatin, bleomycin, and etoposide combination chemotherapy, for which
tumor responded significantly with 90% reduction in volume as shown radiologically
in [Figure 2]. Although the residual tumor was excised, the pathological examination of surgical
specimen did not show any residual tumor. The patient was kept under close follow-up,
and he is disease free at 2 years postsurgery with serum alpha-fetoprotein levels
of 0.88 ng/ml (normal range: 0.89–8.78 ng/ml) and beta-hCG levels of 1.20 mIU/ml (normal
range: <5 m IU/ml).
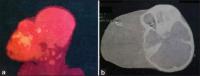 Figure 1: Pretreatment radiological images: (a) positron emission tomography and (b)
plain computer tomography, both showing huge tumor giving the appearance of conjoint
head
Figure 1: Pretreatment radiological images: (a) positron emission tomography and (b)
plain computer tomography, both showing huge tumor giving the appearance of conjoint
head
 Figure 2: Postchemotherapy radiological images: (a) plain computer tomography, (b)
contrast enhanced computer tomography, both demonstrating significant reduction of
tumor bulk following chemotherapy
Figure 2: Postchemotherapy radiological images: (a) plain computer tomography, (b)
contrast enhanced computer tomography, both demonstrating significant reduction of
tumor bulk following chemotherapy
Discussion
As per the MAKEI (Maligne Keimzelltumoren) group, the largest group to have prospectively
studied the germ cell tumors of head and neck region, the YST in head and neck constitutes
1% of malignant germ cell tumors of the body.[1]
[Table 1] depicts the most of the reported cases of YSTs involving head and neck region in
the past 20 years.
Table 1
Reported cases of yolk sac tumors in head and neck region over the last 20 years
|
Author
|
Year
|
Age (years)
|
Sex
|
Site
|
Side
|
Treatment
|
Prognosis
|
|
*Duration not available. NA – Not available; PPS – Parapharyngeal space; S – Surgical
excision; CT – Chemotherapy; RT – Radiotherapy; DF – Disease-free
|
|
Kusumakumari et al.[2]
|
1997
|
6 mn
|
Female
|
Orbit
|
Left
|
S
|
Progression
|
|
|
1.5
|
Male
|
Palate
|
NA
|
S
|
NA
|
|
|
1
|
Female
|
Skull base
|
Right
|
CT
|
Progression
|
|
Bresters et al.[3]
|
2003
|
3
|
Female
|
Sino-orbital
|
Right
|
CT + S + RT
|
Progression
|
|
Mishra et al.[4]
|
2007
|
59
|
Male
|
Sinonasal
|
Right
|
CT + S + RT
|
DF at 1 year
|
|
Kiratli et al.[5]
|
2008
|
2yr 5mn
|
Female
|
Orbit
|
Left
|
S + CT
|
DF at 9 years
|
|
Fujino et al.[6]
|
2009
|
4
|
Male
|
Orbit
|
Right
|
CT + S
|
DF at 1.5 year
|
|
Furtado et al.[7]
|
2011
|
10
|
Female
|
Thyroid
|
Right
|
CT
|
DF*
|
|
Zhang et al.[8]
|
2013
|
1yr 4mn
|
Female
|
Floor of mouth
|
Bilateral
|
S
|
Progression
|
|
Hauser et al.[9]
|
2013
|
2
|
Female
|
PPS
|
Left
|
CT + S
|
DF at 1 year
|
|
Arumugam et al.[10]
|
2016
|
3
|
Female
|
Skull base
|
Bilateral
|
S + CT
|
DF*
|
YSTs of the head and neck appear to have a female predilection [Table 1], in contrast to the gonadal germ cell tumors which frequently involve males. With
respect to the laterality, YSTs in the head and neck region frequently seems to arise
on the right side similar to the gonadal germ cell tumors. From [Table 1], it is clear that the YST in head and neck region is the disease of childhood. According
to the MAKEI group, among all those children with head and neck germ cell tumor, there
is a statistically higher chance of having malignant component (of YST) in those over
the age of 1 year, as compared to those diagnosed in infancy.[1] This peculiar observation seems to hold good even for the index case and for the
majority listed in [Table 1].
In general, the YSTs in head and neck are commonly found to involve sino-nasal and
orbital regions [Table 1]. However, it was seen in the soft tissue of the temporal and infratemporal fossae
in our case. Similar involvement of soft tissue areas like parapharyngeal space and
skull base has also been described rarely in the literature.[9],[10]
In the MAKEI study group, all patients with YST except one had a favorable outcome
with multimodal therapy. It is interesting to find that all children with YST in the
group were over the age of 1 year, suggesting an improved survival with age. Similarly,
cases in [Table 1] also seem to follow the same trend. Among the three cases described by Kusumakumari,
two patients who had treatment failure were actually of age <1 year.[2] It seems that the age of diagnosis of YST influences the overall prognosis in those
affected. However, this fact needs to be verified by a systematic review or meta-analysis.
Another important factor which seems to have a direct bearing on survival in YSTs
of head and neck is the therapeutic regimen. Unlike for benign germ cell tumors, mere
excision of the YSTs may not be adequate in achieving the cure. In fact, as it is
evident from [Table 1], any treatment modality for YST, which is less than multimodality regimen, has resulted
in the unfavorable outcome. The combination chemotherapy based on high-dose cisplatin
along with surgical excision and/or radiotherapy seems to be the optimal treatment
regimen for treating YSTs, and this has contributed to the betterment of disease-free
survival rates in recent times [Table 1]. However, radiotherapy is known to be deleterious in children and might hamper their
overall growth. Thus, surgery is the preferred modality in children along with combination
chemotherapy consisting of cisplatin, etoposide/ifosfamide, and bleomycin.[1] In our case, although the excised specimen did not show any residual tumor tissue,
we believe that the surgical excision has helped in achieving a complete cure, by
eradicating the microscopic and molecularly altered tissue. Similar results of favorable
outcome have been reported in the past by excising the pathologically tumor-free primary
site, after the significant remission with chemotherapy.[9] Furthermore, there are reports of recurrence at the unattended primary sites even
after dramatic response to the chemotherapy.[3]
In summary, the YST of head and neck commonly involve children over the age of 1 year.
However, it seems to be more aggressive if diagnosed in children of <1 year age. It
has a predilection toward the female child, and if extra-axially located, it is commonly
seen on the right side. These YSTs can be treated favorably with multimodality therapy
consisting of cisplatin-based combination chemotherapy with surgery and/or radiotherapy.
However, surgical excision with chemotherapy seems to be the ideal regimen in improving
survival as the radiotherapy has adverse effects on growing child, and the surgery
eradicates the genetically altered tissue at the tumor bed.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
In the form the patient(s) has/have given his/her/their consent for his/her/their
images and other clinical information to be reported in the journal. The patients
understand that their names and initials will not be published and due efforts will
be made to conceal their identity, but anonymity cannot be guaranteed.





