Methods
We followed the standard guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [9] and the Strengthening the Reporting of Observational studies in Epidemiology statement [10] to conduct and report the current systematic review and meta-analysis.
Criteria for study selection
Our systematic review included both prospective randomized controlled trials (RCTs), as well as prospective and retrospective nonrandomized a.k.a observational studies examining the effects of NSAIDs among men with PCa. However, we excluded experimental studies a. k. a cell lines,in vitro and animal studies, and studies with shorter duration (≤6 months) of follow-up. The main outcomes of interest for our review were PCM, ACM, BCR, and development of metastases.
Data sources and searches
We searched electronic databases (Medline [Ovid], Scopus, and the Cochrane library) to identify published articles on topic of our interest from the inception of each database to the 2nd week of March 2016. In addition, we also searched the Web of Science (WOS) to identify gray literature related to conference abstracts from the inception of WOS to the 3rd week of July 2016. We searched these databases using keywords such as “Non-steroidal anti-inflammatory drugs,” “Aspirin,” “prostate neoplasm,” and “prostate cancer.” We reported the details of search strategy for each database in Appendix 1 with keywords and number of retrieved citations per string. Further, we created a weekly alter for new citations' electronic databases. As of now, we included articles available in weekly search until October 10, 2016. Furthermore, we also scanned through the reference lists of identified studies for additional relevant studies.
Data extraction and quality assessment
Two authors (NR and DT) independently assessed the retrieved articles and gray literature for inclusion of articles in the review. We also checked the agreement for inclusion and exclusion of studies between two authors using the kappa statistic. In case of discrepancies about the inclusion or exclusion between two authors, a third author (ADR) resolved the issues with consensus. Three authors (ADR, NR, and DT) independently extracted information from the included studies using a data extraction template. The data extraction template has information on study design, country of participants, year of publication, sample size, inclusion and exclusion criteria of individual studies, PCa stage and severity-related variables, duration of NSAID use, and type and other baseline characteristics. In addition, we also extracted reported outcomes from each study on BCR, metastases, ACM, and PCM with details on statistical parameters such as number of events, median time to outcomes, unadjusted rates of outcomes, and unadjusted and adjusted hazard ratios (HRs).
We utilized the Newcastle Ottawa scale (NOS) tool to examine the risk of bias in included observational studies. The NOS allots up to nine points for the least risk of bias in three domains: (1) selection of study groups (four points); (2) comparability of groups (two points); and (3) ascertainment of exposure and outcomes (three points) for cohort studies. The risk of bias or poor quality was considered as “high” with one or four score total scores, “fair” with a total score of 4–6, and “good” with a total score 7 or more.[11] In addition, we used the Cochrane Risk of Bias assessment tool to evaluate the risk of bias for performance, selection, reporting, and detecting bias domain for RCTs.[12]
Data synthesis and analysis
We computed a pooled hazard ratio (pHR) with 95% confidence interval (CI) for all clinical outcomes reported in the included studies using random-effects models. We used the Cochrane Chi-square (Cochran Q) statistic and the I2 test to analyze heterogeneity across included studies.[13] In the presence of heterogeneity of pooled estimates, we performed subgroup analyses by study design, countries of studies, cancer stage, primary cancer treatment, types of NSAIDs, timing of NSAID exposures, and potential adjusted confounders. We also determined the presence of publication bias for observational studies using Egger's method (Kendall's Tau)[14] and using a contour-enhanced funnel plot to determine other causes of publication bias by examining the symmetry of the plot.[15] All the analyses were performed using Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Results
We identified 4219 citations through electronic databases and other resources. Out of the 4219 citations, we removed 875 duplicates with 3344 citations eligible for first-level screening. We excluded 3068 citations in the first pass based on title and abstract and 237 citations in the second level screening based on full-text information. We excluded the following studies: animal models,in vitro studies, reviews, RCTs on interventions other than NSAIDs, RCTs or observational studies on NSAID use in noncancer population, and studies assessing the risk of PCa with the use of NSAIDs. Finally, a total of 26 studies (39 references) met inclusion criteria for our review. [Figure 1] depicts the study selection process as per the PRISMA framework from the retrieved citations.
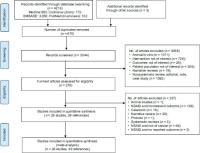 Figure 1: Systematic review and meta-analyses flow chart for study selection for the systematic review on nonsteroidal anti-inflammatory drugs and clinical outcomes in men with prostate cancer. RCT: Randomized Controlled Trials
Figure 1: Systematic review and meta-analyses flow chart for study selection for the systematic review on nonsteroidal anti-inflammatory drugs and clinical outcomes in men with prostate cancer. RCT: Randomized Controlled Trials
Characteristics of included studies
[Table 1] describes the general characteristics of included studies published between 2001 and 2016. We identified 24 observational studies and two randomized controlled studies with a total pooled cohort of 89,436 men with PCa. The included studies had a total of 69,247 men from 20 retrospective cohort studies,[16],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30],[31],[32],[33],[40],[41] 13,855 men from two prospective cohort studies,[34],[35] 1619 men from one case cohort study [36] and 4715 men from one nested case–control study,[37] and 300 men from two prospective randomized controlled studies.[38],[39] Seventeen studies were carried out in the United States,[16],[17],[18],[20],[21],[26],[27],[28],[31],[32],[33],[34],[35],[38],[39],[40],[41] three in the United Kingdom (UK),[22],[29],[37] two in Canada,[24],[36] one each in Belgium,[19] Greece,[30] Finland,[41] and Norway.[25] The sample size of the study cohort ranged between 74[27] and 11,779.[29] With respect to types of NSAID use, 23 of the included studies reported aspirin as the NSAID, one of the each studies reported Exisulind and Ketorolac, and two studies did not specify the type of NSAIDs. The proportion of men with NSAID use ranged from 9.7%[30] to 66%.[18] All the included studies had at least 1 year of median follow-up period with a maximum median duration of 9.25 years in a study.[32]
Table 1
Study characteristics of included studies
|
Study name
|
Study design
|
Time frame
|
Study sample
|
Types of NSAID
|
Number of NSAID users
|
Percentage of NSAID users
|
Follow-up (median, IQR), in years
|
Stage of cancer
|
|
aCardwell et al. had a total of 453 cases and 1619 men in the subcohort, bStock et al. had 1184 cases and 3531 controls of which 617 cases and 1365 controls used any NSAID, cOther NSAID use includes the use of diclofenac, naproxen, indomethacin, and ibuprofen. IQR - Interquartile range; NCCS - Nested case-control study; NSAIDs - Nonsteroidal anti-inflammatory drugs; PCa - Prostate cancer; PCS - Prospective cohort study; RCS - Retrospective cohort study; RCT - Randomized controlled trial; ASA - Aspirin
|
|
Radical prostatectomy
|
|
Goluboff, 2001, US
|
RCT
|
2000-2001
|
94
|
Exisulind
|
47
|
50
|
1
|
Any PCa
|
|
Forget, 2011, Belgium
|
RCS
|
1993-2006
|
1111
|
Ketorolac
|
278
|
25
|
3.16 (1.33-5.75)
|
Any PCa
|
|
Mondul, 2011, US
|
RCS
|
1993-2006
|
2399
|
ASA
|
1584
|
66
|
7
|
Localized PCa
|
|
Kontraros, 2013, Greece
|
RCS
|
1999-2010
|
588
|
ASA
|
74
|
13
|
p: 3.4 (SD: 2.6)
|
Any PCa
|
|
Ishak-Howard, 2014, US
|
RCS
|
1999-2009
|
539
|
ASA
|
270
|
50
|
p: 7.9 (SD: 4.7)
|
Any PCa
|
|
Zaorsky, 2015, US
|
RCS
|
1991-2008
|
189
|
ASA
|
60
|
32
|
4.17 (0.28, 17.8)
|
Localized PCa
|
|
Radiation therapy
|
|
Zaorsky, 2011, US
|
RCS
|
1989-2006
|
2051
|
ASA
|
743
|
36
|
6.3 (1.5-19.9)
|
Localized PCa
|
|
Caon, 2014, Canada
|
RCS
|
2000-2007
|
3851
|
ASA
|
917
|
24
|
8.0
|
Localized PCa
|
|
Jacobs, 2014b, US
|
RCS
|
2005-2008
|
74
|
ASA
|
41
|
55
|
4.63
|
Advanced PCa
|
|
Choe, 2010, US
|
RCS
|
1988-2005
|
662
|
ASA
|
196
|
30
|
4.08
|
Any PCa
|
|
Osborn, 2016, US
|
RCS
|
2003-2010
|
469
|
ASA
|
147
|
31
|
5.08 (2.42-6.83)
|
Any PCa
|
|
Active surveillance
|
|
Agarwal, 2015, US
|
RCS
|
1994-2000
|
102
|
NSAIDs
|
51
|
50
|
9.25 (6.1-12.2)
|
Localized PCa
|
|
Any prostate cancer treatment
|
|
Ratansinghe, 2004, US
|
PCS
|
1971-1992
|
9,869
|
ASA
|
3934
|
40
|
|
Any PCa
|
|
D’Amico, 2008, US
|
RCT
|
1995-2001
|
206
|
ASA
|
86
|
42
|
8.2 (7.0-9.5)
|
Any PCa
|
|
Choe, 2012, US
|
RCS
|
-
|
5955
|
ASA
|
1817
|
31
|
5.83
|
Any PCa
|
|
Dhillon, 2012, US
|
PCS
|
1990-2005
|
3986
|
ASA
|
1586
|
40
|
p: 8.4
|
Any PCa
|
|
Cardwell, 2013a, UK
|
NCCS
|
1998-2006
|
4715
|
ASA
|
1982
|
42
|
p: 6.0
|
Any PCa
|
|
Daugherty, 2013, US
|
RCS
|
1993-2009
|
3857
|
ASA
|
-
|
-
|
5
|
Any PCa
|
|
Flahavan, 2013, UK
|
RCS
|
2001-2006
|
2936
|
ASA
|
1131
|
39
|
5.5
|
Any PCa
|
|
Grytli, 2014, Norway
|
RCS
|
2004-2009
|
3561
|
ASA
|
1149
|
32
|
3.25
|
Any PCa
|
|
Stock, 2008b, Canada
|
Case-Cohort
|
1990-1999
|
1619
|
ASA + others
|
419
|
26
|
-
|
Any PCa
|
|
|
|
|
NSAIDs
|
|
|
|
|
|
Veitonmaki, 2015,
|
RCS
|
1996-2012
|
6537
|
ASA + others
|
NSAID:
|
NSAID:
|
7.5
|
Any PCa
|
|
Finland
|
|
|
|
NSAIDs
|
5,591;
|
86%; ASA:
|
|
|
|
|
|
|
|
ASA: 637
|
10
|
|
|
|
Katz, 2010, US
|
RCS
|
1990-2003
|
7042
|
NSAIDs
|
1830
|
26
|
4(0-16)
|
Any PCa
|
|
Jacob, 2014C-1, US
|
RCS
|
1992-2010
|
8427
|
ASA
|
4827
|
57
|
p: 9.3
|
Localized PCa
|
|
Jacobs, 2014-C2, US
|
RCS
|
1992-2010
|
7118
|
ASA
|
4151
|
58
|
p: 8.4
|
Localized PCa
|
|
Assayag, 2015, UK
|
RCS
|
1996-2012
|
11,779
|
ASA
|
4147
|
35
|
p: 5.4 (SD: 2.9)
|
Localized PCa
|
Seven of the included studies restricted their study cohort to localized PCa [18],[20],[24],[28],[29],[31],[32] and one study included men with advance PCa,[27] whereas the rest of studies did not restrict their cohort based on PCa stage. Six studies included men with PCa treated with radiation therapy (RT),[16],[23],[24],[27],[31],[33] five studies restricted the study cohort to men with PCa treated with radical prostatectomy (RP),[18],[19],[20],[26],[38] one study had men with active surveillance,[32] and the rest of the included men were diagnosed with PCa without restricting them to any primary PCa treatment such as RP/RT.
Characteristics of men with prostate cancer
[Table 2] describes the demographic, comorbidity, and lifestyle characteristics of men among the included studies by NSAID use. Majority of the included studies had 60–66 years of median or mean age of men with PCa. Five of the included studies had 1%–2% of cohort with African-American race distributed evenly between NSAID users and nonusers,[18],[26],[27],[29],[38] whereas one study [33] included only African-American men with PCa. Eleven studies reported the status of chronic conditions.[17],[20],[22],[23],[24],[28],[29],[30],[33],[37],[39] Five studies reported significant greater rate scores of Charlson Comorbidity Index or Adult Comorbidity Score-27 among NSAID users as compared to nonusers,[20],[22],[24],[30],[39] whereas six studies reported greater rates of difference in types of chronic conditions, specifically diabetes, heart disease, and hypertension among NSAID users as compared to nonusers.[17],[23],[24],[27],[29],[37] With regard to lifestyle characteristics, eight studies reported body mass index of the study cohort and majority of the studies had greater proportions of overweight or obese men in both NSAID users and nonusers.[17],[18],[26],[27],[29],[35],[36],[37] Six studies reported had the smoking status of study cohort and out of those all the studies had more than one-third of past or current smokers across NSAID users and nonusers.[17],[18],[22],[27],[36],[37]
Table 2
Demographic, comorbidity, and lifestyle characteristics of study population by nonsteroidal anti-inflammatory drugs use among the included studies
|
Study name
|
Study groups
|
Age (years)
|
Race/ ethnicity (%)
|
Comorbidities (%)
|
BMI (kg/m2)
|
Smoking (%)
|
|
μ - mean; M - median; AA - African-American; ASA - Aspirin; BMI - Body mass index; CCI - Charlson Comorbidity Score; COPD - Chronic obstructive pulmonary disease; CVD - Cardiovascular disease; DM - Diabetes mellitus; HF - Heart failure; HTN - Hypertension; LT - Less than; MI - Myocardial infarction; NSAID - Nonsteroidal anti-inflammatory drugs; OD - Once daily; UK - United kingdom; US - United states; W - Whites; ACS - Adult Comorbidity Score-27; C/P - Current smoker or past smoker
|
|
Radical prostatectomy
|
|
Mondul, 2011, US
|
Overall
|
p: 56.9
|
W: 92.5
|
-
|
p: 26.5
|
C: 1;P: 30
|
|
|
|
|
AA: 02
|
|
|
|
|
Zaorsky, 2015, US
|
NSAID-users
|
M: 65 (51, 80)
|
-
|
ACE-27 score: 0: 20
|
-
|
-
|
|
|
Nonusers
|
M: 61 (43, 77)
|
|
ACE-27 score: 0: 33
|
|
|
|
Ishak-Howard, 2014, US
|
Overall
|
p: 65 (9)
|
W: 97; AA:
|
-
|
BMI >25:
|
-
|
|
|
|
|
2.4
|
|
73%
|
|
|
Goluboff, 2001, US
|
NSAID-users
|
p: 68
|
W: 92; AA: 4
|
-
|
-
|
-
|
|
|
Nonusers
|
p: 66
|
W: 90; AA: 4
|
|
|
|
|
Forget, 2011, Belgium
|
Overall
|
p: 65 (7)
|
-
|
-
|
-
|
-
|
|
Kontraros, 2013, Greece
|
Overall
|
p: 65 (6)
|
-
|
DM: 18
|
-
|
-
|
|
Radiation therapy
|
|
Zaorsky, 2011, US
|
Overall
|
M: 69 (36, 86)
|
-
|
-
|
-
|
-
|
|
Caon, 2014, Canada
|
No-statin/no ASA
|
p: 71
|
-
|
CCI 0: 73
|
-
|
-
|
|
|
Statin/no ASA
|
p: 71
|
|
CCI 0: 51
|
|
|
|
|
ASA/statin
|
p: 72
|
|
CCI 0: 62
|
|
|
|
|
Statin + ASA
|
p: 72
|
|
CCI 0: 40
|
|
|
|
Jacobs, 2014b, US
|
NSAID-users
|
M: 70 (53, 86)
|
-
|
-
|
-
|
-
|
|
|
Nonusers
|
M: 66 (49, 84)
|
|
|
|
|
|
Choe, 2010, US
|
NSAID-users
|
M: 70 (42, 83)
|
-
|
-
|
-
|
-
|
|
|
Nonusers
|
M: 68 (44, 83)
|
|
|
|
|
|
Osborn, 2016, US
|
NSAID users
|
M: 69
|
AA: 100
|
-
|
-
|
-
|
|
|
Nonusers
|
M: 68
|
AA: 100
|
|
|
|
|
Active surveillance
|
|
Agarwal, 2015, US
|
NSAID-users
|
70 (68,73)
|
-
|
-
|
-
|
-
|
|
|
Nonusers
|
|
|
|
|
|
|
D’Amico, 2008, US
|
Overall
|
M: 72.5 (49-
|
-
|
ACE-27 score:
|
-
|
-
|
|
|
|
82)
|
|
severe: 3
|
|
|
|
Choe, 2012, US
|
NSAID-users
|
66 (42, 86)
|
-
|
-
|
-
|
|
|
|
Nonusers
|
63 (39, 85)
|
|
|
|
|
|
Dhillon, 2012, US
|
NSAID-users
|
p: 70 (7)
|
-
|
-
|
p: 26 (4)
|
-
|
|
|
Nonusers
|
p: 68 (8)
|
|
|
p: 26 (3)
|
|
|
Cardwell, 2013, UK
|
Case
|
>60: 99
|
-
|
MI: 11; DM: 12
|
p: 26 (4)
|
C: 19; P: 34
|
|
|
Control
|
>60: 99
|
|
MI: 10; DM: 11
|
p: 26 (4)
|
C: 14; P: 34
|
|
Daugherty, 2013, US
|
NSAID-users
|
-
|
-
|
-
|
-
|
-
|
|
|
Nonusers
|
|
|
|
|
|
|
Flahavan, 2013, UK
|
NSAID-users
|
p: 72 (6)
|
-
|
CCI: 11 (6)
|
-
|
C: 14; P: 20
|
|
|
Nonusers
|
p: 70 (7)
|
|
CCI: 7 (6)
|
|
c: 18; P: 18
|
|
Grytli, 2014, Norway
|
NSAID-users
|
p: 76 (8)
|
-
|
-
|
-
|
-
|
|
|
Nonusers
|
|
|
|
|
|
|
Stock, 2008a, Canada
|
Sub-cohort
|
p: 67
|
-
|
-
|
>25: 55
|
P/C: 60
|
|
|
Case
|
p: 68
|
|
|
>25: 55
|
P/C: 64
|
|
Veitonmaki, 2015, Finland
|
NSAID never
|
p: 67
|
-
|
CCI-0: 58
|
-
|
-
|
|
|
NSAID ever
|
p: 67
|
|
CCI-0:59
|
|
|
|
|
ASA ever
|
p: 68
|
|
CCI-0: 31
|
|
|
|
Katz, 2010, US
|
NSAID-users
|
p: 64 (8)
|
-
|
HTN: 49; HF: 28
|
>25: 74
|
C: 7
|
|
|
Nonusers
|
|
|
HTN: 38; HF: 16
|
>25: 71
|
C: 11
|
|
Jacob, 2014 C-1, US
|
NSAID user-OD
|
<75: 68
|
W: 98; AA: 1
|
DM: 13; CVD: 37
|
p: 26.4
|
C: 5;P: 61
|
|
|
NSAID-use LT
|
<75: 73
|
W: 98%;
|
DM: 9; CVD: 11
|
p: 26.3
|
C: 5; P: 59
|
|
|
OD
|
<75: 70
|
AA: 1
|
DM: 9; CVD: 12
|
p: 26.2
|
C: 5; P: 57
|
|
|
Nonusers
|
|
W: 97; AA: 2
|
|
|
|
|
Jacobs, 2014-C2, US
|
NSAID user-OD
|
<75: 69.9
|
W: 99; AA: 1
|
DM: 14; CVD: 44
|
p: 26
|
C: 3; P: 63
|
|
|
NSAID-use LT
|
<75: 72.4
|
W: 97; AA: 1
|
DM: 9; CVD: 15
|
p: 26
|
C: 3; P: 60
|
|
|
OD
|
<75: 71.4
|
W: 97; AA: 2
|
DM: 12; CVD: 17
|
p: 26
|
C: 4; P: 59
|
|
|
Nonusers
|
|
|
|
|
|
|
Assayag, 2015, UK
|
NSAID-users
|
p: 74 (8)
|
W: 69; AA: 1
|
HTN: 63; HF: 16; MI: 8
|
>30: 16
|
-
|
|
|
Nonusers
|
p: 70 (7)
|
W: 67; AA: 1
|
HTN: 36; HF: 6; MI: 1
|
>30: 10
|
|
[Table 3] describes PCa-related clinical and cancer-related treatment characteristics by NSAID use. Fourteen studies reported the status of prostate-specific antigen (PSA) levels [16],[18],[19],[20],[23],[25],[26],[28],[29],[31],[35],[36],[38],[39] and those studies did not find significant difference in PSA levels between NSAID users and nonusers. Sixteen studies reported Gleason score,[16],[18],[19],[20],[22],[25],[26],[28],[29],[30],[31],[35],[37],[38],[21],[29],[39] of which two studies included >50% of men with Gleason score >7. Thirteen studies reported tumor stage,[16],[18],[19],[20],[22],[25],[26],[27],[28],[30],[35],[36],[39] of which two studies [20],[36] had significant differences in the proportion of men with T2/3 stages among NSAID users and nonusers. Nine studies [16],[20],[21],[24],[25],[31],[33],[38],[39] reported the National Comprehensive Cancer Network scores of which one study [20] had significant difference in medium- and high-risk PCa among NSAID users and nonusers. Fifteen studies reported androgen deprivation therapy (ADT)[16],[17],[18],[21],[22],[24],[25],[27],[28],[29],[30],[31],[35],[36],[37] of which two studies [18],[31] did not have any men with ADT users among NSAIDs users and no users.
Table 3
Prostate cancer and its treatment-related characteristics among the included studies
|
Study ID
|
Study groups
|
Prostate tumor characteristics
|
Prostate Cancer Therapy
|
|
PSA level (ng/ml)
|
Gleason Score
|
Tumor stage
|
NCCN risk categories
|
ADT (%)
|
RP (%)
|
RT (%)
|
AW/WW (%)
|
|
μ - mean; M - median; AA - African-American; ASA - Aspirin; M/H - Medium- or high-risk prostate cancer; NCCN - National Cancer Comprehensive Network; LT - Less than; MI - Myocardial infarction; NSAIDs - Nonsteroidal anti-inflammatory drugs; OD - Once daily; PSA - Prostate-specific antigen
|
|
Radical prostatectomy
|
|
Mondul, 2011, US
|
Overall
|
p: 6.7
|
>7: 6.3%
|
T2/3a: 29%
|
-
|
None
|
All
|
None
|
None
|
|
Zaorsky, 2015, US
|
NSAID-users
|
M: 0.67
|
>7: 4%
|
T2/3: 32%
|
M/H: 32%
|
-
|
All
|
-
|
None
|
|
Nonusers
|
M: 0.50
|
>7: 11%
|
T2/3: 68%
|
M/H: 66%
|
|
|
|
|
|
Ishak-Howard, 2014, US
|
Overall
|
p: 2.1
|
>7: 17%
|
T2/3: 90%
|
-
|
-
|
All
|
-
|
None
|
|
Goluboff, 2001, US
|
NSAID-users
|
p: 2.2
|
p: 6.6
|
-
|
M/H: 22%
|
-
|
All
|
-
|
None
|
|
Nonusers
|
p: 2.7
|
p: 6.5
|
|
M/H: 27%
|
|
|
|
|
Forget, 2011, Belgium
|
Overall
|
>10: 38%
|
>7: 24%
|
T2/3: 100%
|
-
|
-
|
All
|
-
|
None
|
|
Kontraros, 2013, Greece
|
Overall
|
M: 7.6
|
>7: 51%
|
-
|
-
|
-
|
-
|
All
|
None
|
|
Radiation therapy
|
|
Zaorsky, 2011, US
|
Overall
|
>10: 30%
|
>7: 26%
|
T2/3: 42%
|
M/H 56%
|
None
|
None
|
All
|
None
|
|
Caon, 2014, Canada
|
No-statin/no
|
-
|
-
|
-
|
M/H: 84%
|
71%
|
None
|
All
|
None
|
|
ASA
|
|
|
|
M/H: 73%
|
61%
|
|
|
|
|
Statin/no ASA
|
|
|
|
M/H: 84%
|
63%
|
|
ASA/Statin
|
|
|
|
M/H:81%
|
59%
|
|
|
|
|
Statin + ASA
|
|
|
|
|
|
|
|
|
|
|
Jacobs, 2014b, US
|
NSAID-users
|
p: 49
|
> 7: 77%
|
T2c/3b:
|
-
|
96%
|
-
|
All
|
None
|
|
Nonusers
|
p: 40
|
7: 62%
|
44%
|
|
|
86%
|
|
|
|
|
|
|
|
T2c/3b:
|
|
|
|
|
|
|
|
|
|
|
48%
|
|
|
|
|
|
|
|
Choe, 2010, US
|
NSAID-users
|
M: 8.1
|
> 7: 10%
|
T3: 4%
|
M/H:62%
|
44%
|
-
|
All
|
None
|
|
Nonusers
|
M: 8.5
|
>7: 9%
|
T3: 7%
|
M/H
|
62%
|
40%
|
|
|
|
|
Osborn, 2016, US
|
NSAID-users
|
-
|
-
|
-
|
M/H: 78%
|
39%
|
-
|
All
|
-
|
|
Nonusers
|
|
|
|
M/H
|
: 72%
|
39%
|
|
|
|
|
Any prostate cancer treatment
|
|
D’Amico, 2008, US
|
Overall
|
>10: 61%
|
> 7: 15%
|
T2: 52%
|
|
|
NR
|
|
|
|
|
Choe, 2012, US
|
NSAID-users
|
M: 5.9
|
> 7: 7%
|
T3: 2%
|
M/H: 58%
|
11%
|
63%
|
37%
|
00%
|
|
Nonusers
|
M: 6.0
|
>7: 8%
|
T3: 3%
|
M/H: 58%
|
08%
|
70%
|
30%
|
00%
|
|
Dhillon’ 2012’ US
|
NSAID-users
|
M: 7.2
|
>7: 7%
|
T3: 3%
|
|
7%
|
44%
|
39%
|
4%
|
|
Nonusers
|
M: 7.2
|
>7: 7%
|
T3: 4%
|
|
7%
|
50%
|
33%
|
4%
|
|
Cardwell’ 2013’ UK
|
Case
|
-
|
>7: 54%
|
-
|
-
|
82%
|
2.4%
|
21%
|
|
|
Control
|
|
>7: 73%
|
|
|
59%
|
7.6%
|
21%
|
|
|
Flahavan’ 2013’ UK
|
NSAID-users
|
-
|
>7: 16%
|
T3: 13%
|
-
|
48%
|
3.6%
|
39%
|
-
|
|
Nonusers
|
|
>7: 16%
|
T3: 13%
|
|
43%
|
7.4%
|
38%
|
|
|
Grytli’ 2014’ Norway
|
Overall
|
>10: 92%
|
>7: 53%
|
T2/3: 86%
|
H: 100%
|
70%
|
-
|
-
|
|
|
Stock’ 2008’ Canada
|
Sub-cohort
|
>10: 61%
|
-
|
T3/4: 8%
|
-
|
32%
|
41%
|
59%
|
|
|
Case
|
>10: 84%
|
|
T3/4: 23%
|
|
32%
|
17%
|
83%
|
|
|
Veitonmaki’ 2015’
|
NSAID never
|
-
|
>7: 40%
|
-
|
-
|
42%
|
22%
|
35%
|
19.2%
|
|
Finland
|
NSAID ever
|
|
>7: 42%
|
|
|
41%
|
26%
|
37%
|
17.3%
|
|
Aspirin ever
|
|
>7: 41%
|
|
|
44%
|
18%
|
39%
|
17.6%
|
|
KatZ’ 2010’ US
|
NSAID-users
|
-
|
-
|
-
|
-
|
15%
|
|
|
|
|
Nonusers
|
|
|
|
|
15%
|
|
|
|
|
Jacobs’ 2014-C1’ US
|
NSAID
|
-
|
-
|
T3/4: 3%
|
-
|
-
|
30%
|
40%
|
12%
|
|
user-OD
|
|
|
T3/4: 3%
|
|
|
38%
|
32%
|
10%
|
|
NSAID-use LT OD Nonusers
|
|
|
T3/T4: 3%
|
|
|
34%
|
33%
|
12%
|
|
Jacobs’ 2014-C2’ US
|
NSAID
|
-
|
-
|
T3/4: 3%
|
-
|
-
|
34%
|
39%
|
11%
|
|
user-OD
|
|
|
T3/4: 2%
|
|
|
37%
|
34%
|
11%
|
|
NSAID-use LT OD Nonusers
|
|
|
T3/4: 3%
|
|
|
37%
|
34%
|
11%
|
|
Assayag’ 2015’ UK
|
NSAID users
|
>10: 46%
|
>7: 45%
|
-
|
-
|
62%
|
38%
|
52%
|
|
|
Nonuser
|
>10: 42%
|
>7: 46%
|
|
|
56%
|
47%
|
62%
|
|
Quality assessment of included studies
We used NOS tool to determine the quality of the included observational studies and the Cochrane risk of bias tool for RCT. Twenty-four of the included observational studies had a fair or good quality as per the NOS scale and two of the included observational studies had low risk for selection, performance bias, and unclear risk for reporting bias. Details on each of the three domains for risk of bias selection, ascertainment of exposure and outcomes, and comparability for observational studies are provided in Appendix 1.1-1.3 [SUPPORTING:1] [SUPPORTING:2] [SUPPORTING:3] and the risk of bias table for RCT are provided in Appendix 1.4. [SUPPORTING:4] Out of the 24 observational studies, ten utilized single institutional data,[18],[19],[20],[21],[23],[26],[28],[31],[32],[33] seven utilized survey or prospective cohort data,[16],[17],[27],[30],[34],[35],[40] and six studies utilized cancer registry-linked electronic medical records or administrative claim databases.[22],[24],[25],[29],[36],[37] The coding algorithms for PCa were not defined with their diagnostic accuracy in single institutional data. With respect to exposure of interest, five studies [20],[28],[29],[31],[33] reported the use of NSAID postcancer or postcancer therapy, five studies [22],[24],[28],[34],[40] reported the precancer period or precancer treatment period NSAID exposure, and rest of the studies measured NSAID at any time during the study period. Except one study,[27] all other observational studies conducted multivariable regression analysis controlling for the potential confounders while examining association between NSAID use and clinical outcomes. However, only Fourteen studies [18],[19],[22],[23],[24],[25],[26],[28],[29],[31],[33],[35],[41] controlled for co-medications.
Nonsteroidal anti-inflammatory drug use and clinical outcomes
We conducted meta-analyses of the included studies to evaluate the association between NSAID use and several clinical outcomes in men with PCa. Due to the presence of significant heterogeneity in the pooled estimates, we performed several subgroup analyses by types of NSAIDs, pre-, post- or any NSAID use, and type of PCa treatment.
Prostate cancer-specific mortality
Eleven studies reported the association between NSAID use and PCM,[16],[22],[24],[25],[28],[29],[30],[33],[35],[36],[40] of which three studies found an inverse relationship between aspirin use and PCM,[16],[25],[33] while two studies found an increased risk of PCM associated with aspirin use,[29],[30] whereas rest of the six studies did not find any association between NSAID use and PCM.
Overall, any type of NSAID use was not associated with the risk of PCM (pHR: 0.95; 95% CI: 0.79, 1.05; P = 0.19; I2 = 62%) with significant heterogeneity [Figure 2]. In the subgroup analyses by timing of aspirin use, we found that aspirin use, irrespective of prior to or following PCa diagnosis, was not associated with PCM (pHR: 0.95; 95% CI: 0.77, 1.16; P = 0.60; studies = 11, I2 = 88%). Furthermore, aspirin use prior to PCa diagnosis or primary treatment was not significantly associated with PCM (pHR: 1.00; 95% CI: 0.83, 1.19; P = 0.97; studies = 5; I2 = 51%), and so was for ever (pHR: 1.34; 95% CI: 0.71, 2.51; P = 0.36; studies = 2; I2 = 97%) or postdiagnosis or postcancer aspirin use (pHR: 0.94; 95% CI: 0.72, 1.23; P = 0.67; studies = 8; I2 = 86%). In contrast, postdiagnosis or post-treatment NSAID use was associated with 2.5 times increased risk of PCM (pHR: 2.50; 95% CI: 1.75, 3.57; P < 0.0001; studies = 1). However, one study reported a nonsignificant association between precancer diagnosis NSAID use and PCM (pHR: 1.03; 95% CI: 0.79, 1.34; P = 0.83).
 Figure 2: Forest plot of comparison: Nonsteroidal anti-inflammatory drug users versus nonusers for prostate cancer-specific mortality
Figure 2: Forest plot of comparison: Nonsteroidal anti-inflammatory drug users versus nonusers for prostate cancer-specific mortality
Nine studies reported the association between NSAID use and PCM among men who had RP, RT, or other therapies.[16],[22],[25],[28],[29],[30],[35],[36],[40] In this subgroup, NSAID use was not significantly associated with PCM (pHR: 1.02; 95% CI: 0.79, 1.30; P = 0.90; studies = 10; I2 = 91%). Among men with PCa who had RT as the primary treatment, NSAID use was not significantly associated with PCM (pHR: 0.91; 95% CI: 0.65, 1.27; P = 0.58). Two studies [16],[29] which controlled for time of NSAID exposure using time-dependent NSAID use reported a lower though nonsignificant risk of PCM due to NSAID use (pHR: 0.84; 95% CI: 0.25, 2.76; P = 0.77; studies = 2; I2 = 91%).
Three studies reported the risk of PCM by NSAID dose.[22],[28],[36] As compared to nonusers, either high-dose or low-dose NSAID was associated with 5% reduction in the PCM, though the association was not significant.
Nonsteroidal anti-inflammatory drug use and all-cause mortality
Three studies reported ACM as an outcome.[17],[22],[29] NSAID use was not associated with ACM in the pooled analysis with significant heterogeneity (pHR: 0.82; 95% CI: 0.54, 1.24; P = 0.19; I2 = 73%) [Figure 3]. To find the cause of heterogeneity, leave-one-out sensitivity analysis was performed which did not alter the study finding.
 Figure 3: Forest plot of comparison: Nonsteroidal anti-inflammatory drug users versus nonusers for all-cause mortality
Figure 3: Forest plot of comparison: Nonsteroidal anti-inflammatory drug users versus nonusers for all-cause mortality
Nonsteroidal anti-inflammatory drug use and biochemical recurrence
The hazard of BCR was reported in five studies.[16],[19],[20],[23],[26] Overall, NSAID use was not significantly associated with reducing the hazards of BCR using random-effects model (pHR: 0.82, 95% CI: 0.54, 1.24, P = 0.34, 5 studies, I2: 73%) with significant heterogeneity. We carried out subgroup analyses to explore the possible reasons of heterogeneity. NSAID use in men who had RP (pHR: 0.79, 95% CI: 0.45, 1.38, P = 0.41, 3 studies, I2: 69%) or RT (pHR: 0.85, 95% CI: 0.35, 2.03, P = 0.71, 2 studies, I2: 88%) was not significantly associated with reducing the risk of BCR [Figure 4]
 Figure 4: Forest plot of comparison: Nonsteroidal anti-inflammatory drug users versus nonusers for biochemical recurrence
Figure 4: Forest plot of comparison: Nonsteroidal anti-inflammatory drug users versus nonusers for biochemical recurrence
Nonsteroidal anti-inflammatory drug use and metastases
Two studies [16],[27] examined the hazards of metastases with the use of NSAID. Both the studies found a beneficial effect of NSAID in the univariate analysis and did not have a sufficient sample size to conduct multivariable analyses.
Discussion
Our review aimed to generate evidence on the effects of NSAIDs on cancer prognosis among men with PCa. We found 24 observational studies and two RCTs examining the impact of NSAIDs on different cancer prognostic outcomes. We found that NSAID use was not associated with BCR, metastases, ACM, and PCM in pooled estimates with significant heterogeneity. To account for heterogeneity, we conducted various subgroup analyses and observed significant findings across those subgroup analyses which reduced the heterogeneity in some cases.
First, as majority of the included studies used aspirin as the main NSAID class, we did a subgroup analysis by types of NSAID as aspirin users and nonaspirin NSAID. We did not find any conclusive evidence on the beneficial effect of NSAIDs and PCM. Our findings are also similar to a previous systematic review by Elwood et al. examining the association between NSAID and PCM. Elwood et al. found no association between NSAID and PCM in a pooled estimate of nine studies with significant heterogeneity. However, in that study, they observed a significant association with omission of one study.[29] This difference in our findings could be due to negative or no association observed in the newer additional studies included in our review.
There has been significant heterogeneity in the pooled estimates even after subgroup analyses, which suggest the variation in the analytic samples among the included studies. Most of the studies had utilized secondary preexisting data and the study was based on a data-driven design approach rather than design-driven data collection approach. For example, there have been great variations on timing of NSAID use as pre/postdiagnosis, or pre/post-treatment NSAID use, or ever use of NSAID. Both pre- and post-diagnosis NSAID could not serve as meaningful treatment to inhibit progression of cancer if men do not adhere to medications or used for symptomatic pain relief. One of the major biases with NSAIDs is bias by treatment indications. NSAID can be used for different indications at different stages of prostate cancer having low or high comorbidity burden. For example, aspirin can be used to prevent primary prevention of heart disease in men with localized PCa as well as to relieve pain in men with metastatic PCa, which have drastically different prognosis.
Second, the timing of aspirin in the postdiagnosis or post-treatment suffers from two major biases: immortal time bias and lag time bias. With respect to immortal time bias, men using NSAID in the follow-up period should be alive until they receive the NSAID postdiagnosis. This leads to misclassification of unexposed person-time as exposed person-time. In addition, if NSAID is initiated few days before death due to palliative pain relief, then there would be very short NSAID exposure time for fatal event. Therefore, such exposure may not provide conclusive findings due to design limitations. Although two studies have controlled for time of NSAID exposure using time-dependent NSAID use, both the studies yielded mixed results on the NSAID use and PCM. Such results may be again due to variation in the population.
Further, we also explored relationship between NSAID and clinical outcomes by high-risk PCa. Again, study findings among those with high-risk PCa had mixed findings. These could be due to effect modification due to hormone therapy use in high-risk PCa with aspirin. A study found that aspirin was associated with abnormal liver function and the serum level of aspirin is also expected to be higher due to low level of testosterone which leads to inhibit the metabolism of aspirin. Eventually, men using NSAID are at risk of abnormal liver function [42] and affect the adherence to hormone therapy in men with PCa. Therefore, the proportion of patients using hormone therapy could serve as a potential confounder for the association between NSAID use and clinical outcomes in men with PCa.
Strengths and limitations of our study findings suggest the need for well-designed observational studies to examine the association between NSAID use and clinical outcomes among homogeneous PCa population, i.e., stage or primary PCa treatment controlling for important covariate including adherence and persistence or duration of NSAID use.





