

Subscribe to RSS
DOI: 10.4103/ijps.IJPS_214_17
The refinement of the median tubercle of cleft lip
Authors
Address for correspondence:
Publication History
Publication Date:
26 July 2019 (online)


ABSTRACT
Aim: Repair of cleft lip aims to bring symmetry and provide normal aesthetics for the lip. Several techniques have been employed; however, the finer aspect of median lip tubercle has not been emphasised in cleft lip repair. Materials and Methods: We have modified cleft lip repair, both unilateral and bilateral, preserving all the tissues of the median tubercle to provide normal-looking median tubercle of the lip. The modified technique was carried out by a single surgeon on 322 cases of unilateral cleft lip and 68 cases of bilateral cleft lip. Follow-up was done for 1–3 years on these children to evaluate the outcome. Results: The evaluation showed excellent results in more than 80% of patients in unilateral cleft lip repair, on 1–3 years of follow-up; 20% had acceptable results. Of 68 patients with bilateral cleft lip, none had any complication, and excellent results were obtained in 70%. Result was rated acceptable in 30%; 15% may need revision surgery for white roll and vermilion adjustment. Conclusion: We present the technique of reconstructing a normal-looking median tubercle in cleft lip repair. The technique was modified based on the study of normal upper lip and embryology of cleft lip, with emphasis on creating better median tubercle of the lip.
INTRODUCTION
Components of upper lip include two labial elements as follows: philtrum with philtral columns and vermilion and a median tubercle. Median tubercle is the most prominent part of the lip highlighting beauty and sexuality, particularly in women. The median tubercle is generally visualised as a small central projection in the upper lip; however, in reality, it is a broad gradual elevation of approximately the central one-third of the lip. A line drawing shows the extent of central prominence visible in normal lips [[Figure 1]]. This median elevation has racial, sexual and individual variations. The tubercle has been found to have more blood vessels and nerve supply analogue to erectile tissue. Literature yields very little details about the anatomical extent, variability and measurement of median tubercle in various age groups. Tubercle of the lip is less studied in medical sciences as compared to sciences related to eroticism.
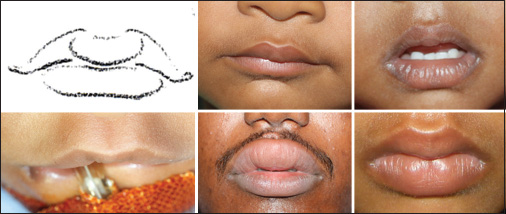
In unilateral cleft lip repair, the techniques of repair emphasise on the reconstruction of Cupid's bow and avoiding picking of vermilion, but bestows minimum attention to reconstruction of the median tubercle. By emphasising on measurements and moving different flaps, one misses the perception of natural beauty and individuality of the lip. In the present techniques of cleft lip repair, the incision directed medially or straight down on vermilion from point ‘3’ (cphc) of Cupid's bow is likely to result in a violation of the central tubercle or excising a part of the tubercle as excess vermilion [[Figure 2]].

In bilateral cleft lip repair, there is even more confusion. Manchester technique for bilateral cleft lip repair utilises the prolabium mucosa for tubercle, but it has poor aesthetic outcome due to several reasons.[[1]] Utilisation of lateral vermilion with white roll to reconstruct central tubercle was suggested by Millard, and emphasised by Noordhoff and Mulliken.[[2] [3] [4]] This technique is based on several observations and assumptions which are as follows: (1) Cupid's bow of prolabium is rounded; (2) White roll is indistinct and absent in prolabium; (3) Colour of central vermilion is not the same as lateral lip vermilion and (4) it is difficult to get an accurate approximation of vermilion for good aesthetic outcome.
Embryology and applied anatomy
Embryology of the cleft lip formation is the basis for this method and some pertinent points are emphasised.[[5]]
Unilateral cleft lip
In unilateral cleft lip, failure of fusion leads to elevation of cleft edge of lip, pulling the lip tubercle to alveolus. The tubercle can be distinctly visualised, as fanning of mucosa from the labial frenulum with many individual variations, as shown in [Figure 3].

Bilateral cleft lip
In bilateral cleft lip, failure of fusion of median nasal process with maxillary process results in folding in of prolabium mucosa and adherence to premaxilla [[Figure 4]]. The prolabium is bereft of muscle with poorly defined white roll in a bilateral cleft lip and consists of philtral skin with vermilion of the median tubercle and soft tissue which is highly vascular. Mulliken et al.[[6]] described that, in normal anatomy, the white roll prominence is due to underlying marginalis orbicularis oris muscles. For this reason, the prolabium bereft of muscle does not have visible white roll.

Increase capillaries in vermilion, decreased melanin and increased non-keratinised tissue give reddish hue to vermilion, especially at tubercle.[[6]] We studied the histopathology of soft tissue of prolabium, which is normally discarded. This soft tissue showed marked vascularity with thick-walled and congested blood vessels [[Figure 5]] similar to erectile tissue. In the current practices of bilateral cleft lip repair, the prolabial vermilion with highly vascularised soft tissue is excised, and central tubercle is reconstructed by lateral vermilion which is bereft of similar vascularised tissue.[[2] [3] [4]] This has also been our practice and long-term follow-up showed that the central tubercle reconstructed by lateral vermilion becomes thinner and more pigmented, without normal anterior bulge of central tubercle often with whistle tip deformity.

Keeping the above facts and observations in mind, we modified unilateral and bilateral cleft lip repair as described below.
Surgical procedures
Unilateral cleft lip repair
One needs to observe the cleft lip as an artist to define the central tubercle tissue. After marking the Cupid's bow points, a line is drawn on the lip including the whole tubercle curving near the midline on the mucosal side [[Figure 6]]. After incising the tubercle that is obliquely oriented, it is made more horizontally aligned. This tissue is rotated towards the free border with the help of skin hook to visualise the tubercle shape [[Figure 6]]. The rest of labial repair is completed with the alignment of the white line. The excess vermilion from the lateral segment is de-epithelialised and placed medially under the tubercle to support its prominence It also forms a soft groove, which naturally exists on either side of the tubercle.

Bilateral cleft lip repair
As per the current practices of bilateral cleft lip repair, the narrow philtrum, approximately 5–6 mm at lower border and 3–4 mm at upper border, is marked. After marking, the skin is incised, and most of the dry and wet mucosa of prolabium are taken with philtral skin. The prolabium is lifted from premaxilla, taking all soft tissue and leaving only two ‘m’ flaps on premaxilla. The prolabium mucosa is unfolded, leaving skin with minimum soft tissue protecting sub-dermal plexus for philtrum, and pushing the soft tissue towards the free vermilion border [[Figure 7]]. The ‘m’ flaps are sutured over the premaxilla to deepen the buccogingival sulcus. Further routine surgical steps are carried out. After repair of the muscle layer, excess of lateral vermilion is de-epithelialised, and the pars marginalis is sutured in midline. The central vermilion of prolabial mucosa with vascularised soft tissue is draped on this muscle, creating a central bulge on anterior-inferior border of the lip. While suturing dry mucosa of vermilion to that of lateral segment, adjustment of pigmented and red mucosa needs careful attention. The vermilion mucosa is pulled across free border of the lip reaching mucosal aspect. After surgery, the tubercle often looks congested [[Figure 8]]; however, there is no loss of any tubercle or any breakdown of the lip.


MATERIALS AND METHODS
This new modification was adopted in the repair of 322 cases of unilateral cleft lip and 68 cases of bilateral cleft lip. The results were analysed at duration of 1.5–3 years postoperatively by two surgeons other than the operating surgeon. Only results pertaining to aesthetics of the median lip tubercle were analysed. The evaluation categorised the cases in two categories as follows: (1) Excellent and (2) Acceptable. In addition, any patient needing revision surgery pertaining to the central tubercle adjustment was noted. Intrarater and interrater reliability were determined using kappa statistics. Intrarater reliability was 0.886, while interrater reliability was 0.864 for unilateral cleft lip evaluation. For bilateral cleft lip, the intrarater reliability was 0.872 and the interrater reliability was 0.793.
RESULTS
We have been practising this technique for unilateral cleft lip repair for the past 4 years, getting better median tubercle definition [[Figure 9]]. As per evaluation, excellent results are achieved in 80% and acceptable results in 20% of unilateral cleft lip repair cases. Acceptable results in the unilateral cleft lip are due to the displacement of median tubercle to one side due to smaller or collapsed maxillary segment.

Bilateral cleft lip repair had a long learning curve through the 1–3 years of follow-up, showing a normal-looking central tubercle, with good volume and natural redness. In bilateral cleft lip repair, we had results classified as excellent in 70% [[Figure 10a]], acceptable in 30%; 15% may need revision surgery for white roll and vermilion adjustment. The white roll, not visible preoperatively, becomes more defined in median tubercle with muscle repair in all bilateral lips. Lateral view shows good protrusion of upper lip in comparison with the lower lip, unlike in traditional cleft lip repair. We did not observe any dryness or crusty central vermillion on long-term results. The probable explanation can be good underlying vascularity keeping it warm and moist. This procedure has shown good results in different types of bilateral cleft lip repair, either with protruding and/or twisted premaxilla or with small and hypoplastic prolabium with median facial dysplasia [[Figure 10b]].

DISCUSSION
During long-term evaluation of cleft lip repair in our institute, we observed that aesthesis of median tubercle definition was absent. This was particularly so in the bilateral lip, where the median tubercle was not well defined, absent and often with whistle tip deformity due to inadequate bulk provided by the lateral segment vermilion.
As Millard quotes in cleft craft, ‘the losses have followed most often when surgeon ignored the first principle of plastic surgery know the normal’.[[7]] To improve the aesthetic outcome of tubercle, we carefully observed the anatomy of the cleft lip, which also brings out the individuality of every lip.
With present practices in unilateral cleft lip, we achieve symmetry but curves of lip, and particularly the central tubercle, are missing. We drew attention to ensure that, whatever be the technique used, the central tubercle tissue is envisaged and preserved to reconstruct the tubercle.
In bilateral cleft lip, we utilised the precious tissue of prolabium, especially mucosa and soft tissue which is excised and thrown. Using this tissue, a natural-looking median tubercle with good protrusion of lip was obtained.
To rebut the observations and presumptions of Millard, Noordhoff, and Mulliken point wise:
-
Cupid's bow is rounded – In normal population, most lips have rounded Cupid's bow (60% of children in the study of normal lip in our centre did not have triangular Cupid's bow [unpublished])
-
White roll is indistinct and absent in prolabium – Although this is a correct observation, it is a wrong assumption. Visible distinct white roll demands marginalis orbicularis oris.[[6]] The distinct well-defined white roll is visible after repairing the marginalis muscle under it, as shown in all our results [[Figure 10a and b]]
-
Colour of median vermilion is not the same as lateral lip vermilion – This is natural and desirable to enhance the central tubercle
-
Difficult to get an accurate approximation of vermilion for good aesthetic outcome – These technical details can be learnt by surgeons.
We followed the principles quoted by Ralph Millard in Cleft Craft for cleft lip repair, ‘that it concerned with describing in intricate details of logical way of finding the missing pieces and fitting them carefully into puzzle so that the final picture is complete, normal and happy in function and appearance’.[[7]] Nature has given unique beauty to each individual. Tubercles of the lip are different in every individual. Therefore, it is paramount to visualise the mediantubercle tissue, preserve it and utilise it to create the median tubercle.
Heightened perception and keen observation of deformities of cleft lip, the available tissue and supplementing our scientific knowledge to repair the lip will bring out a lip which is closest to what nature intends to create before cleft happened!
CONCLUSION
Reconstruction of lip tubercle is not given its due during cleft lip repair. Long term results of repaired cleft lip often lack definition of natural looking median tubercle. Hence we modified the technique cleft lip repair based on embryology for reconstructing a natural-looking median tubercle. Our results showed natural looking tubercle in unilateral and bilateral cleft lip repair after follow up of 1-3 years in majority of patients. We shall present our long-term results of these techniques in future.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
-
REFERENCES
- 1 Manchester WM. The repair of bilateral cleft lip and palate. Br J Surg 1965; 52: 878-82
- 2 Mulliken JB. Principles and techniques of bilateral complete cleft lip repair. Plast Reconstr Surg 1985; 75: 477-87
- 3 Millard Jr DR. Cleft Craft. Vol. 2. Boston: Little Brown; 1977: p. 259-374
- 4 Noordhoff MS. Reconstruction of vermilion in unilateral and bilateral cleft lips. Plast Reconstr Surg 1984; 73: 52-61
- 5 Yoon H, Chung IS, Seol EY, Park BY, Park HW. Development of the lip and palate in staged human embryos and early fetuses. Yonsei Med J 2000; 41: 477-84
- 6 Mulliken JB, Pensler JM, Kozakewich HP. The anatomy of Cupid's bow in normal and cleft lip. Plast Reconstr Surg 1993; 92: 395-403
- 7 Millard Jr DR. Cleft Craft. Vol. 1. Boston: Little Brown; 1976: p. 15
Address for correspondence:
-
REFERENCES
- 1 Manchester WM. The repair of bilateral cleft lip and palate. Br J Surg 1965; 52: 878-82
- 2 Mulliken JB. Principles and techniques of bilateral complete cleft lip repair. Plast Reconstr Surg 1985; 75: 477-87
- 3 Millard Jr DR. Cleft Craft. Vol. 2. Boston: Little Brown; 1977: p. 259-374
- 4 Noordhoff MS. Reconstruction of vermilion in unilateral and bilateral cleft lips. Plast Reconstr Surg 1984; 73: 52-61
- 5 Yoon H, Chung IS, Seol EY, Park BY, Park HW. Development of the lip and palate in staged human embryos and early fetuses. Yonsei Med J 2000; 41: 477-84
- 6 Mulliken JB, Pensler JM, Kozakewich HP. The anatomy of Cupid's bow in normal and cleft lip. Plast Reconstr Surg 1993; 92: 395-403
- 7 Millard Jr DR. Cleft Craft. Vol. 1. Boston: Little Brown; 1976: p. 15