Sir,
Tissue approximation techniques have evolved from employing insect claws and linen glue strips.[[1]] Surgical aims for suturing are well known. Patient characteristics, suturing materials and techniques, added to consideration of duration, anatomical zones, function, and aesthesis decide final outcomes.[[2]] Despite advent of different technologies and methods, hand suturing techniques remain unparalleled in versatility.
The simple interrupted, continuous, vertical or horizontal mattress sutures, all have their utilities and drawbacks. The hybrid mattress suture judiciously balances the pros and cons of vertical and horizontal mattress suturing and is executed with speed.[[3]] Wu et al. employ a combination of vertical and horizontal mattress on opposite sides of the defect, a technique suited to closing unequal size margins.[[4]]
We have devised a hybrid technique of vertical and horizontal mattress suturing as a buried variant.
TECHNIQUE
A demonstrative model made of silicon sheets placed in step form is illustrated for clarity of depth and obliquity of suture course. The needle is held obliquely along the long axis of the wound. It is inserted from the deep surface of the flap 1–2 cm away from the incision apex and 1–2 cm lateral to the cut edge. The needle moves obliquely through the tissue towards the incision apex and brings the suture from deep subcutaneous to superficial dermis and from 1 to 2 cm lateral entry in tissues to medial cut edge of the wound. The needle exits subepidermally near the wound apex [[Figure 1]]. The suture returns from the opposite edge as a reverse mirror image to exit at the same depth and distance on the opposite wound edge as the entry site [[Figure 2]]. We employ absorbable sutures on reverse cutting needles, the sizes being dictated by tissue thickness.
 Figure 1: Needle inserted deep subcutaneously and passed towards wound apex, suture moving from deeper to superficial layers and lateral to medial to exit at the dermal level
Figure 1: Needle inserted deep subcutaneously and passed towards wound apex, suture moving from deeper to superficial layers and lateral to medial to exit at the dermal level
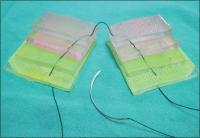 Figure 2: Completed suture before knotting, showing depth and obliquity
Figure 2: Completed suture before knotting, showing depth and obliquity
On tying the knot, the dermis and epidermis oppose with accuracy towards the apex where the suture is dermal. Deeper tissues approximate well with dead space obliteration at the site of buried knot where the needle is entering and exiting [[Figure 3]]. The closed wound edge resembles a downward slope from wound edge distally. The second interrupted hybrid mattress suture is similarly started at a more distal location from wound apex with the needle exiting subepidermally on top of the earlier deeper suture and knot. Progressing interrupted suturing leads to wound closure [[Figure 4]].
 Figure 3: End on view of tied suture
Figure 3: End on view of tied suture
 Figure 4: Sequential buried hybrid mattress suturing in progress
Figure 4: Sequential buried hybrid mattress suturing in progress
Oblique insertion of the needle along with the long wound axis allows for easy suturing in constrained spaces. A single hybrid buried suture brings two depths (deep fascial/subcutaneous and dermal layers) of tissues together across a wider length than interrupted stitches achieving deep dead space obliteration and accurate epidermal alignment. Wound edge vascularity remains uncompromised while ensuring haemostasis. The closure is air and waterproof, and we have been routinely using it with suction drains where indicated. There are no suture track marks and no removal is needed.
We routinely employ hybrid sutures in skin closure or flap inset across diverse regions of variable skin thickness with success. The technique is easily grasped on demonstration and proficiency reached after a few cases. We feel that hybrid buried mattress suturing has potential for application in various situations and may prove to be a useful addition to existing suturing techniques.
Financial support and sponsorship
Nil.






