
Subscribe to RSS
DOI: 10.4103/ijri.IJRI_194_17
Doppler indices of superior thyroid artery in clinically euthyroid adults
Subject Editor:


Abstract
Context: Ultrasonography of thyroid gland is a frequently performed investigation. Many of the diffuse thyroid pathologies are associated with altered vascularity. In view of potential applications and scant available data, there is a need to find normal values of Doppler indices of superior thyroid artery (STA). Aims: To find the normal range of Doppler indices like mean peak systolic velocity (PSV), resistivity index (RI), and pulsatility index (PI) of STA in clinically euthyroid adult individuals. Settings and Design: Prospective cross-sectional observational study. Materials and Methods: A study was done in the Department of Radiodiagnosis of a tertiary care hospital, involving clinically euthyroid adult volunteers. Ultrasonography of the thyroid gland with Doppler of bilateral STAs was performed and mean values of PSV, RI, and PI were calculated. Results: A total of 208 subjects, with a mean age of 37.7 years, underwent Doppler evaluation of STA; 148 of them were women and 60 were men. The mean PSV obtained was 16.94 ± 5.3 cm/s. Mean PI and RI were 0.93 ± 0.31 and 0.5 ± 0.13, respectively. There was no significant difference in the values obtained among both the genders. Conclusion: Mean values of Doppler indices of STA in euthyroid individuals have been found in this study.
#
Keywords
Peak systolic velocity - pulsatility index - resistivity index - superior thyroid artery - thyroid functionIntroduction
Ultrasonography of thyroid gland is routinely sought, though hormonal assays are more specific in evaluating thyroid status.[1],[2] In early stages of diseases, thyroid glandular parenchyma are often found normal.[3],[4] Pathological studies have found altered glandular vascularity in various diseases.[5],[6] Doppler studies on thyrotoxicosis have found high systolic velocities.[7],[8],[9],[10] There is lack of data if Doppler indices of supplying arteries predict abnormalities at an earlier stage. Limited studies have been done to establish normal Doppler parameters of thyroid arteries [11],[12] and no study exists in Indian context. This study intends to find normal ranges of Doppler indices of superior thyroid arteries (STAs).
#
Materials and Methods
A prospective, cross-sectional, observational study was done in a tertiary care hospital from December 2016 to February 2017, involving clinically euthyroid individuals. Prior Institutional Ethical Committee clearance was obtained. All subjects underwent the study voluntarily. Informed consent was taken prior to performing the study. Some of them had undergone thyroid hormone analysis earlier, voluntarily. All the subjects underwent detailed clinical evaluation including history taking, resting pulse rate, neck examination, etc., prior to ultrasonography. All the subjects were clinically euthyroid, with no clinical manifestations of thyroid-related conditions.
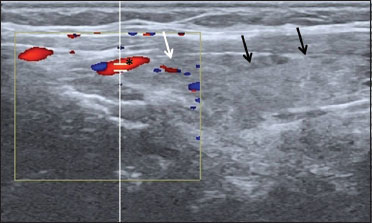
The subjects were made to rest for 10 min on the examination couch before proceeding with Doppler evaluation of the thyroid gland. They were made to lie in supine position with the neck extended by placing a pillow underneath the neck. GE Logic S6 ultrasound machine was used for the study. Linear probe of frequency 7–12 MHz was used with a coupling agent (ultrasound gel). Initially, B-mode scan was done to look for echogenicity of the gland and also to look for any lesions. The normal gland is granular and homogeneously echogenic as shown in [Figure 1].[11],[13] Cases with incidentally found thyroid nodule or altered parenchymal echo pattern were excluded from the study. Subsequently, STA was identified as the first branch of external carotid artery that arises anteriorly at the level of hyoid bone. In most cases, the vessel could be traced up till the upper pole of thyroid gland, where the artery was sampled using color Doppler mode, as shown in [Figure 2]. Spectral waveform was taken with a sample gate size of 1 mm and Doppler angles of 30–60°, as depicted in [Figure 3]. Peak systolic velocity (PSV), pulsatility index (PI), and resistivity index (RI) of bilateral STAs were calculated. PI represents the variability of the flow velocity in the sampled vessel. RI signifies the resistance offered to the blood flow by distal vascular bed. The observations were tabulated in Microsoft Excel 2010 worksheet. Mean values were calculated for all parameters. Mann–Whitney U test was used to compare the values between both the genders.


#
Results
A total of 249 adults volunteered for ultrasonography of thyroid gland during the study period. Twenty-nine of these were found to have small nodules in the thyroid gland and another 12 were found to have altered echotexture of the thyroid gland on B-mode scan. These 41 subjects were excluded from the study and were advised to consult endocrinologist for management. Doppler evaluation of bilateral STAs was done in the remaining 208 individuals. Hence, a total of 416 STAs were assessed in this study. This sample size was found to be adequate based on precision-based sample size calculation formulae with a confidence interval of 95%.
The 208 subjects were aged between 21 and 64 years of age, with a mean age of 37.7 years. This included 148 women and 60 men. Of these 208 subjects, 136 had undergone thyroid hormone analysis in the previous 6 months, the results of which were normal. Forty-eight more individuals underwent thyroid hormone assays after the Doppler study, which were normal. The remaining 24 participants did not undergo hormonal assay and were found clinically euthyroid with normal sonological appearance of thyroid gland.
In 178 individuals the STAs could be easily traced at the superior poles of the thyroid gland where they enter the gland. These portions of the arteries were sampled with Doppler and spectral tracings were obtained. In the remaining 30 individuals, the STAs could not be exactly delineated at the superior poles of the gland and hence sampled much closer to their origins from the external carotid arteries.
Each examination lasted for an average of 9 min. All the STAs sampled showed an initial steep systolic upstroke and a more gradual initial downstroke, followed by a plateau in diastolic phase on spectral tracing. None of them showed absent/reversed flow in diastolic phase. The flow indices were calculated automatically. Wherever there were ambiguities with automatically calculated values, manual calculations were performed.
The mean PSV obtained was 16.94 ± 5.3 cm/s. The mean PI was 0.93 ± 0.31 and RI was 0.55 ± 0.13. The mean PSV, PI, and RI among females and males are depicted in [Table 1]. The values obtained were not significantly different in both the genders (P > 0.05 for all parameters, Mann–Whitney U test).
|
Doppler parameter |
Average of all subjects |
Average in females |
Average in males |
|---|---|---|---|
|
*P>0.05 - Mann Whitney U test for all three parameters |
|||
|
Peak systolic velocity* |
16.94±5.3 cm/sec |
16.84±5.7 cm/sec |
17.18±4.45 cm/sec |
|
Pulsatility index* |
0.93±0.31 |
0.89±0.37 |
1.02±0.32 |
|
Resistivity index* |
0.55±0.13 |
0.54±0.16 |
0.59±0.11 |
#
Discussion
B-mode ultrasonography of the thyroid gland, though often performed, may not reflect the actual thyroid status, and may reveal a normal appearing thyroid gland in early stages of various diseases. In a study by Trimboli et al.,[3] a normal appearing thyroid gland on B-mode ultrasound scan did not correlate with normal thyroid hormone levels in 25% cases. Most of them showed mild increase in thyroid stimulating hormone levels, which in turn may progress to frank hypothyroidism.[14]
Thyroid gland is a highly vascular organ. Some studies have documented altered vascularity of the thyroid glandular parenchyma in diffuse thyroid diseases. Jebreel et al.[5] found that there was varying expression of vascular endothelial growth factor gene in different types of thyroid pathologies, both benign and malignant.
In this context it would be interesting to note whether vascular changes preclude the gross morphological changes of thyroid gland and whether such vascular changes could be detected by Doppler evaluation of the supplying arteries. Bogazzi et al.[8] observed increased thyroid vascularity in some forms of thyrotoxicosis as well as Graves’ disease. Zhao et al. and Uchida et al. have effectively demonstrated STAPSV of above 40–50 cm/s as corresponding to Graves’ disease and concluded that PSV of STA was reliable to differentiate various etiologies of thyrotoxicosis.[9],[15]
Though these studies have quoted cut-off PSV values for Graves’ disease, handful of studies have been done to establish normal values of Doppler indices of STA.
In the present study, STA was selected for the Doppler study as it was easily accessible, being superficial, and more consistent in its location than inferior thyroid artery.[16] All the subjects included in this study were residents of a geographical area, not considered to have high prevalence of iodine deficiency disorders.
Macedo et al. included 165 euthyroid individuals of Brazil (as against 208 in the present study) and found mean PSV of STA to be 25.84 cm/s and PI and RI to be 1.03 and 0.62, respectively, which are higher than values obtained in the present study (PSV – 16.94 cm/s, PI – 0.93, and RI – 0.55). PSV of STA in females was found to be significantly higher in males than in the study by Macedo et al.[11] No such significant differences were seen in the present study. Other than this, literature search did not reveal any study done exclusively to find normal values of STA flow parameters. Most of studies used healthy controls for comparison and identification of abnormality, in view of lack of established normal reference ranges.
Varsamidis et al. in their study found the mean PSV of STA in control subjects to be 26.2 cm/s, which is higher than that found in the current study. However, the number of control subjects included by Varsamidis et al. was only 14.[17] Kim et al. enrolled 60 control subjects to compare PSV of STA in Graves’ disease and destructive thyroiditis and found a mean PSV of 17.55 cm/s, which is similar to the present study.[18]
Having included a higher number of subjects than other similar studies, the normal values established in the present study for STA may be considered reference values for further studies in Indian scenario. Further studies may focus on interpreting the Doppler changes of STA in various thyroid abnormalities and also find whether STA Doppler indices can help predict thyroid disorders at an earlier stage.
Limitations
Thyroid hormone assays were not done in all subjects. Hence possibility of some individuals having subclinical thyroid functional alteration cannot be ruled out, in spite of them showing normal sonological appearance.
Inferior thyroid artery is also a major source of blood supply to thyroid gland and Doppler assessment of inferior thyroid artery was not done in the present study owing to deeper location and increased frequency of its variations.
#
#
Conclusion
Mean values of Doppler indices of STA in euthyroid individuals have been found in this study, which may be used as reference for future studies on potential applications in assessing thyroid status and identifying diffuse thyroid disorders at an earlier stage.
#
#
Conflict of Interest
There are no conflicts of interest.
-
References
- 1 Soto GD, Halperin I, Squarcia M, Lomeña F, Domingo MP. Update in thyroid imaging. The expanding world of thyroid imaging and its translation to clinical practice. Hormones (Athens) 2010; 9: 287-98
- 2 Chaudhary V, Bano S. Thyroid ultrasound. Indian J Endocrinol Metab 2013; 17: 219-27
- 3 Trimboli P, Rossi F, Condorelli E, Laurenti O, Ventura C, Nigri G. et al. Does normal thyroid gland by ultrasonography match with normal serum thyroid hormones and negative thyroid antibodies?. Exp Clin Endocrinol Diabetes 2010; 118: 630-2
- 4 Vejbjerg P, Knudsen N, Perrild H, Laurberg P, Pedersen IB, Rasmussen LB. et al. The association between hypoechogenicity or irregular echo pattern at thyroid ultrasonography and thyroid function in the general population. Eur J Endocrinol 2006; 155: 547-52
- 5 Jebreel AE, England J, Bedford K, Murphy J, Karsai L, Atkin S. Vascular endothelial growth factor (VEGF), VEGF receptors expression and microvascular density in benign and malignant thyroid diseases. Int J Exp Pathol 2007; 88: 271-7
- 6 Wang JF, Milosveski V, Schramek C, Fong GH, Becks GP, Hill DJ. Presence and possible role of vascular endothelial growth factor in thyroid cell growth and function. J Endocrinol 1998; 157: 5-12
- 7 Ruchała M, Szczepanek E. Thyroid ultrasound—a piece of cake. Endokrynol Pol 2010; 61: 330-44
- 8 Bogazzi F, Bartalena L, Brogioni S, Burelli A, Manetti L, Tanda ML. et al. Thyroid vascularity and blood flow are not dependent on serum thyroid hormone levels: Studies in vivo by color flow Doppler sonography. Eur J Endocrinol 1999; 140: 452-6
- 9 Zhao X, Chen L, Li L, Wang Y, Wang Y, Zhou L. et al. Peak systolic velocity of superior thyroid artery for the differential diagnosis of thyrotoxicosis. PLoS One 2012; 7: e50051
- 10 Huang SM, Chow NH, Lee HL, Wu TJ. The value of color flow Doppler ultrasonography of the superior thyroid artery in the surgical management of Graves’ disease. Arch Surg 2003; 138: 146-51
- 11 Macedo TA, Chammas MC, Jorge PT, De Souza LP, Farage L, Pegoraro BL. et al. Reference values for Doppler ultrasound parameters of the thyroid in a healthy iodine-non-deficient population. Br J Radiol 2007; 80: 625-30
- 12 Ueda M, Inaba M, Kumeda Y, Nagasaki T, Hiura Y, Tahara H. et al. The significance of thyroid blood flow at the inferior thyroid artery as a predictor for early Graves’ disease relapse. Clin Endocrinol (Oxford) 2005; 63: 657-62
- 13 Ghervan C. Thyroid and parathyroid ultrasound. Med Ultrason 2011; 13: 80-4
- 14 Díez JJ, Iglesias P. Spontaneous subclinical hypothyroidism in patients older than 55 years: An analysis of natural course and risk factors for the development of overt thyroid failure. J Clin Endocrinol Metab 2004; 89: 4890-7
- 15 Uchida T, Takeno K, Goto M, Kanno R, Kubo S, Takahashi S. et al. Superior thyroid artery mean peak systolic velocity for the diagnosis of thyrotoxicosis in Japanese patients. Endocr J 2010; 57: 439-43
- 16 Toni R, Della Casa C, Castorina S, Roti E, Ceda G, Valenti G. A meta-analysis of inferior thyroid artery variations in different human ethnic groups and their clinical implications. Ann Anat 2005; 187: 371-85
- 17 Varsamidis K, Varsamidou E, Mavropoulos G. Color Doppler sonography in the detection of parathyroid adenomas. Head Neck 1999; 21: 648-51
- 18 Kim TK, Lee EJ. The value of the mean peak systolic velocity of the superior thyroidal artery in the differential diagnosis of thyrotoxicosis. Ultrasonography 2015; 34: 292-6
Publication History
Article published online:
26 July 2021
© 2018. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Thieme Medical and Scientific Publishers Private Ltd.
A-12, Second Floor, Sector -2, NOIDA -201301, India
-
References
- 1 Soto GD, Halperin I, Squarcia M, Lomeña F, Domingo MP. Update in thyroid imaging. The expanding world of thyroid imaging and its translation to clinical practice. Hormones (Athens) 2010; 9: 287-98
- 2 Chaudhary V, Bano S. Thyroid ultrasound. Indian J Endocrinol Metab 2013; 17: 219-27
- 3 Trimboli P, Rossi F, Condorelli E, Laurenti O, Ventura C, Nigri G. et al. Does normal thyroid gland by ultrasonography match with normal serum thyroid hormones and negative thyroid antibodies?. Exp Clin Endocrinol Diabetes 2010; 118: 630-2
- 4 Vejbjerg P, Knudsen N, Perrild H, Laurberg P, Pedersen IB, Rasmussen LB. et al. The association between hypoechogenicity or irregular echo pattern at thyroid ultrasonography and thyroid function in the general population. Eur J Endocrinol 2006; 155: 547-52
- 5 Jebreel AE, England J, Bedford K, Murphy J, Karsai L, Atkin S. Vascular endothelial growth factor (VEGF), VEGF receptors expression and microvascular density in benign and malignant thyroid diseases. Int J Exp Pathol 2007; 88: 271-7
- 6 Wang JF, Milosveski V, Schramek C, Fong GH, Becks GP, Hill DJ. Presence and possible role of vascular endothelial growth factor in thyroid cell growth and function. J Endocrinol 1998; 157: 5-12
- 7 Ruchała M, Szczepanek E. Thyroid ultrasound—a piece of cake. Endokrynol Pol 2010; 61: 330-44
- 8 Bogazzi F, Bartalena L, Brogioni S, Burelli A, Manetti L, Tanda ML. et al. Thyroid vascularity and blood flow are not dependent on serum thyroid hormone levels: Studies in vivo by color flow Doppler sonography. Eur J Endocrinol 1999; 140: 452-6
- 9 Zhao X, Chen L, Li L, Wang Y, Wang Y, Zhou L. et al. Peak systolic velocity of superior thyroid artery for the differential diagnosis of thyrotoxicosis. PLoS One 2012; 7: e50051
- 10 Huang SM, Chow NH, Lee HL, Wu TJ. The value of color flow Doppler ultrasonography of the superior thyroid artery in the surgical management of Graves’ disease. Arch Surg 2003; 138: 146-51
- 11 Macedo TA, Chammas MC, Jorge PT, De Souza LP, Farage L, Pegoraro BL. et al. Reference values for Doppler ultrasound parameters of the thyroid in a healthy iodine-non-deficient population. Br J Radiol 2007; 80: 625-30
- 12 Ueda M, Inaba M, Kumeda Y, Nagasaki T, Hiura Y, Tahara H. et al. The significance of thyroid blood flow at the inferior thyroid artery as a predictor for early Graves’ disease relapse. Clin Endocrinol (Oxford) 2005; 63: 657-62
- 13 Ghervan C. Thyroid and parathyroid ultrasound. Med Ultrason 2011; 13: 80-4
- 14 Díez JJ, Iglesias P. Spontaneous subclinical hypothyroidism in patients older than 55 years: An analysis of natural course and risk factors for the development of overt thyroid failure. J Clin Endocrinol Metab 2004; 89: 4890-7
- 15 Uchida T, Takeno K, Goto M, Kanno R, Kubo S, Takahashi S. et al. Superior thyroid artery mean peak systolic velocity for the diagnosis of thyrotoxicosis in Japanese patients. Endocr J 2010; 57: 439-43
- 16 Toni R, Della Casa C, Castorina S, Roti E, Ceda G, Valenti G. A meta-analysis of inferior thyroid artery variations in different human ethnic groups and their clinical implications. Ann Anat 2005; 187: 371-85
- 17 Varsamidis K, Varsamidou E, Mavropoulos G. Color Doppler sonography in the detection of parathyroid adenomas. Head Neck 1999; 21: 648-51
- 18 Kim TK, Lee EJ. The value of the mean peak systolic velocity of the superior thyroidal artery in the differential diagnosis of thyrotoxicosis. Ultrasonography 2015; 34: 292-6