Key-words:
Body mass index - cesarean delivery - caesarean-section - fetomaternal - mortality
- parity - Rh factor - vaginal delivery
Introduction
The cesarean-section (CS) was introduced in clinical practice as a lifesaving procedure
both for the mother and the infant.[[1]] The proportion of CS to the total births is considered as one of the important
indicators of emergency obstetric care.[[2]] The rate of CD has increased dramatically over the past decade. The observation
was that in the case of perinatal mortality, there was no benefit of CS for the countries
with a high perinatal mortality rate (>20/1000).[[3]] About 18.5 million CS are performed yearly worldwide and continues to rise in the
developed as well as in many developing nations.[[4]] The rates in many countries have increased beyond the WHO-recommended level of
5%–15%. In high-income as well as low-income countries the rates have gone up phenomenally
in the last few decades.[[5]] In India the average rate was increased from 21.8% to 25.4% with two states, Kerala
and Goa, have shown the highest percentage of CS delivery.[[6]] The rate of CD is relatively much higher in private hospitals rather than in public
health facilities.[[7]]
There was a lack of sufficient evidence to evaluate fully the risk and benefits of
planned CD. However, a number of studies have found that cesarean cases at maternal
request are actually rare and many personal and societal reasons including fear of
labor pain, future sexual dissatisfaction, etc., are behind some reasons.[[8]] Surgical intervention during pregnancy is usually performed to ensure the safety
of the mother and child under conditions of obstetric risks but becomes malpractice.[[9]]
It is often argued that CS also depends upon the power of decision-making in the home
and seeking medicalized health care was associated with higher maternal education,
family incomes, and women's fear of the physiological consequences of a normal delivery.[[10]] There are, for instance, practice styles among physicians, or attitudes among obstetricians,
fear of litigation, the physician's convenience, and most importantly, economic incentives
may favor and determines the choice of CS delivery. Economic motives may include both
doctors' fear of malpractice as well as economic gain.[[11]] In general, it is argued that besides the medical factors, the physician's interests
determine the choice of CS.
Women's height is correlated to the pelvic size and is currently used to predict cephalopelvic
disproportion.[[12]] Umbilical cord prolapses were associated with an increased risk of neonatal hypoxic
brain injury and perinatal death. A history of infertility treatment among nulliparous women >40 years old with singleton
pregnancies increases the risk for cesarean delivery (CD) independently of other known
risk factors. The reported rate of perinatal diagnosis of Cord Entanglement was found
to be 23%. Patients with oligohydramnios have significantly higher incidences of fetal
heart rate decelerations and CS than patients with adequate amniotic fluid. Neonates
with oligohydramnios are twice as likely to develop pulmonary hypoplasia and more
likely to experience neonatal death when compared to those with adequate fluid. Induction
of labor following CS is associated with a significantly higher incidence of repeat
CS in women who have not had a previous vaginal delivery (VD). Lack of progress in
labor (also known as dystocia or failure to progress) is a dominant reason for CD.
The planned CS is better than the planned VD for the term fetus in the breech presentation.[[13]]
As CD at one period of time was performed only subsequent to maternal death, but the
risk of maternal death has been estimated to be several times due to CD. Still, there
are several problems which make it difficult to interpret them. Some reports suggested
that there may not be an increased risk of maternal death with elective CD compared
with VD however maternal mortality has become rare in affluent countries, but the
picture is quite blurred for developing Nations. The risk of maternal death due to
CD is significantly high when compared with VD, particularly when performed during
labor.[[14]]
Anesthetic complications, hemorrhage and sepsis, which are mostly preventable in affluent
countries, may make major contributions toward maternal mortality in adverse conditions.
This needs to be taken into account by clinicians and women when considering the risk-benefit
equation.[[15]] CD is a major surgical procedure and should only be practiced when conditions clearly
demand it. The present study will reveal the factors that provoked CD and will also
be a major breakthrough in finding out the genuine reasons for dramatically increasing
cesarean cases. Research is needed to adequately compare outcomes of planned and unplanned
CD. This study will review current research on the rise in CD and its implications
related to risks, benefits, ethics, practice, and future research. It includes certain
clinical and nonclinical parameters which will help out in assessing, analyzing, and
interpretation of the factors that provoked CD. The major clinical parameters will
support this up to a great extent to this study.
Materials and Methods
The short-term retrospective study for about 3 months was conducted at Department
of Obstetrics and Gynecology, Pt. Deen Dayal Upadhyay Hospital and Northern Railway
divisional hospital Moradabad, India. The study was designed to ascertain the short
term prevalence of CD and its associated outcomes in Moradabad. The prevalence of
CD in India was 10.2%[[16]] so the sample size required was calculated accordingly with a relative precision
of 10.2% of prevalence with a confidence level of 95%, using the formula: Z (1α/2) pq/d. The calculated sample size obtained was 140 but to make study optimized we have
taken the sample size of 345.[[17]] The Body Mass Index 34 and socioeconomic Status 35 of the subjects were calculated
in accordance to previous reported studies.[[18]]
Data collection
A case record form was designed, reviewed by an expert panel and was pre-tested on
25 cases and was scaled up for study. The first section of the questionnaire was designed
to project the basic demographic details such as body weight, age, height, diet, personal
background (religion, education, occupation, socioeconomic status), etc., While second
section of the questionnaire was designed to record clinical manifestations related
to pregnancy or delivery like past or present hormonal therapy, postmenopausal complications,
gravida parity, duration between successive gravida parity, mode of delivery whether
normal or cesarean, etc. with concerned complications. The data were collected using
various data sources from IPD/MICU visited patients.
The questionnaire was completed by collecting required data from Maternity records
and laboratory investigation reports (if available) of labor/cesarean ward with the
cooperation of present staff. The personal interaction with patients or her attendant
was done to precise the accuracy of desired parameters which were mentioned in the
questionnaire. Informed consent was taken from the subject or representative of the
subject before data collection.
Inclusion criteria
-
Woman hospitalized in the respective hospital
-
A woman should be above of age 18 years
-
Postpartum woman available during data collection
-
Those who are willing to participate actively.
Exclusion criteria
-
A woman not hospitalized in the respective hospital
-
A woman less than the age of 18 years
-
Postpartum woman not available during data collection
-
Those who are not willing to participate.
Statistical analysis
The groups were compared by applying Fisher's exact test for the analysis of categorical
variables, and Wilcoxon's rank-sum test for the analysis of continuous variables that
were not normally distributed. A two-sided P < 0·05 indicated statistically significance.
Results
Patient participation was strictly abided by the provisions of inclusion and exclusion
criteria and an informed consent form required before their admission in the study.
The study includes postpartum hospitalized females and was classified into two groups,
i.e., CD and VD. Out of 345 deliveries, 125 were CD and their prevalence for a particular
course of duration was found to be 36.23%. The evaluated baseline data are summarized
in [[Table 1]].
 Table 1: Caesarean section delivery and its determinant factors
Table 1: Caesarean section delivery and its determinant factors

Late-age pregnancy abide cesarean-section
As the age of the mother increases, there was more possibility of going through CS.
Mothers aged (30 or more) have greater chances of CS delivery than younger counterparts
[[Table 1]].
Optimized body mass index prevents cesarean-section
The study suggested the effect of body mass index and its known confounders such as
gestational age, birth weight, maternal age, and maternal height on CS. The BMI of
the mother signifies positive relation of CS with body mass index. The risk of CD
increased consistently and significantly (P < 0.001) with increased BMI. However, differential limits of normal BMI signify that
maximum births with the least % of CS occurred with the upper limit of normal BMI
and lower limit of normal BMI possessed high % of CS. This signifies the inverse relation
of CS with differential levels of normal BMI range.
Educational supremacy favours caesarean-section
The maximum number of births cases were of illiterate women but possessed the least
% of CS however births belonging to highly educated women was found to show high %
of CS. This signifies that as the education profile was getting high the possibility
of CS increased that showed the existence of a statistical association between Education
and CS (P < 0.001).
Religious intervention favours caesarean-section in Muslims
175 deliveries were belonged to Muslims with 42.85% of CS however 170 deliveries in
Hindu possess 29.41% of CS which signifies that there were more CS in the Muslim community
among other religions.
Low nutritional value diet might put the mother to cesarean-section
CS was more experience by Non-vegetarian mothers with 42.93% as compared to vegetarians,
possessed 27.92% of CS. Junk food eater mothers with 55.46% of CS however Non-Junk
food eater mothers experienced only 26.106% of CS. This signifies there was a positive
relation of CS with Junk food and non-vegetarian dietary habits.
Rh negative factor: An indication for cesarean-section
As per Rh factor concerned the data represented that majority of deliveries in women
are with positive Rh factor with 34.71% of CS cases. Although only 8 births in women
with negative Rh factor was found, the probability of CS in terms of percentage was
significantly high (87.5%).
Infertility treatment might instigate cesarean-section
Although hormonal therapy improves pre- and post -maternal complications it might
instigate CS occurrence. The population taking Hormonal therapy has more probability
in terms of percentage (78.84) to undergo CS [[Table 1]].
Impact of parity on cesarean-section
There was 31.53% of CS during first parity, however a significant increase in CS was
found up to third parity (53.65%) but after third parity the occurrence of CS deliveries
decreased [[Table 2]]. In the first parity among the total births, there were five postpartum women which
had previous miscarriages. All five women went through CS. In 1st, 2nd, and 3rd parities among the total births there were six postpartum women had previous fetal
demised and all 6 women went through CS.
 Table 2: Women underwent caesarean section as per parity
Table 2: Women underwent caesarean section as per parity
Increased parity gap provoked caesarean-section
The gap between successive parity that was taken in months, there was 28.62% of CS
with parity gap of 12–24 months however 100% possibility of CS was found with parity
gap of more than 48 months that signifies the proportionate possibility of CS with
an increased duration between parities [[Table 3]].
 Table 3: Women underwent caesarean section as per duration between successive parity
Table 3: Women underwent caesarean section as per duration between successive parity
Cesarean-section results increased bodyweight of new-born
The average maximum weight of new-born is 3.08 kg and the mean weight for all age
groups was found to be 2.89 kg. The possibility of CS was increased with increasing
baby weight [[Table 4]].
 Table 4: Women underwent caesarean section as per new born weight and gender
Table 4: Women underwent caesarean section as per new born weight and gender
Cesarean-section prevents infant mortality
The mortality % of CD was 14.28% however for VD it was 85.71% which signifies that
CS prevents infant mortality [[Table 5]].
 Table 5: Women underwent caesarean section as per mortality
Table 5: Women underwent caesarean section as per mortality
Maternal and foetal complications provoked cesarean-section possibility
[[Table 6]] represented summarized clinical interventions that provoked CS like cephalopelvic
disproportion, infertility, cord entanglement, previous fetal demised and meconium
stained etc., however major complications include oligohydramnios and previous lower
segment cesarean (LSC). The above-mentioned medical complications were major factors
responsible for CS. Overall there was 99.2% possibility of undergoing CS if a woman
possessing all the above medical complications.
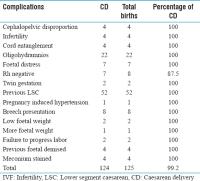 Table 6: Women underwent caesarean section as per medical factors
Table 6: Women underwent caesarean section as per medical factors
Discussion
Women today embark on pregnancy at a late age; therefore their chances of undergoing
CD were high. Our findings related to maternal age suggested that late age maternity
endorsed CS possibility as several studies suggest that women were more prone to complications
as the age of pregnancy and delivery increases.[[19]],[[20]] This study suggested that the risk of CD increased consistently and significantly
with increased BMI but optimized BMI favors the VD because higher BMI increases the
rate of cephalopelvic disproportion/Failure to progress which favors CS. It is often
argued that the power of decision-making in the home and seeking medicalized health
care were associated with higher maternal education and family incomes. The study
suggests that the proportion of CS is much higher among mothers having secondary and
higher education than without education or primary education. In India, the proportion
of CD is very high among mothers with high educational background, which perhaps illustrates
that women with higher educational attainment can make decisions about their own health
care. Researchers have found a strong correlation between increasing CS deliveries
with socioeconomic and cultural factors. In some instances, doctors' preferences for
the surgical procedure and women's demands are responsible for the increasing trend
of CS which imposed a financial burden on the patients. This study supports the fact
that as the majority of CS cases belong to the upper socioeconomic class. Besides,
this different rates of CS in public and private hospitals suggested that non-medical
factors such as economic gain and pressures of private practice may motivate doctors
to perform surgical deliveries. Another factor related to decision-making for CS is
giving birth in auspicious time or on some special day. In a country like India, where
religion and religious believes takes place before any other things, childbirth in
an auspicious day perhaps an important factor for opting surgical intervention. Our
study represented the correlation between religious beliefs and CS among different
communities and it was found that the majority of CS deliveries were from the Muslim
community followed by the Hindu community. It has also been noticed from the voices
of women that preference for having birth on some special day for religious and cultural
reasons exists which sometime comes from family members or the woman herself opted.[[21]] The higher order births are less likely to deliver by CS, this fact is supported
by our study but only after third parity as delivery complications are significantly
lower among higher-order pregnancies. However, this study on the other hand also showed that up to 3rd parity probability of CS was more likely to occur. The factor that provoked for the
performance of CS is large size of the baby at birth and the possibility of CS was
increased with increasing baby weight. Larger size babies are at higher risk of being
delivered by CS. Moreover, babies with birth weight more than 3 kg are also at high
risk. In India, CS is widely perceived as safer than vaginal birth for babies.[[22]],[[23]] The perinatal mortality, neonatal mortality, or serious neonatal mortality was
significantly lower for the planned CS group than for the planned vaginal birth group.
The prevalence of obesity in pregnant has reached pandemic proportions across nations.
Junk food and nonveg stuffs are considered to have low nutritional values than pure
vegetarian diets and also these items were more prone to provoked obesity during pregnancy
due to limited or less physical activity. CS in these women poses many surgical, anesthetic,
and logistical challenges.[[24]] We found a significant positive correlation of CS in overweight pregnant women
who have Junk food and non-vegetarian dietary habits. The probability of CS in Rh-negative
mothers in terms of percentage was significantly high and was supported by the fact
that the Rh-negative patients were undergoing CS for the presence of significant fetomaternal
hemorrhage.[[25]] The history of infertility treatment among women > 40 years old with singleton
pregnancies increases the risk for CD independently of other known risk factors. Although
hormonal therapy improves pre- and post-maternal complications, it might instigate
CS occurrence. This study reveals that the population taking Hormonal therapy has
more probability to undergo CS. Cephalopelvic disproportion is a major risk factor
for maternal and perinatal morbidity and mortality. Women's height is correlated to
the pelvic size and is currently used to predict Cephalopelvic disproportion. The
pregnancies conceived by IVF and ovulation induction have led to an increase in the
number of multiple births and these babies are usually delivered by CS.[[26]] The reported rate of perinatal diagnosis of Cord Entanglement is only 23% and fetal
movements may increase tightening of an already entangled umbilical cord which could
lead to occlusion and fetal distress. Patients with oligohydramnios have significantly
higher incidences of fetal heart rate decelerations and CS than patients with adequate
amniotic fluid. Neonates with oligohydramnios are twice as likely to develop pulmonary
hypoplasia and more likely to experience neonatal death when compared to those with
adequate fluid. The induction of labor following CS is associated with a significantly
higher incidence of repeat CS in women who have not had a previous VD.[[27]] Many Caesareans are done during the latent phase of labor and in the second stage
of labor when it is not prolonged. Repeated lower section caesareans (LSC) and lack
of progress in labor (also known as dystocia or failure to progress) are the most
common reasons for CD.[[28]] Number of clinical interventions that provoked CS were reported during the study
like cephalopelvic disproportion, infertility, cord entanglement, previous fetal demised
and meconium stained etc., however, major complications include oligohydramnios and
previous LSC.[[29]]
Conclusion
This study illustrates the major factors that provoked CD. It acknowledges that the
provision of CD is universally accepted as it ensures feto-maternal safety. The mortality
of maternal with CD was found to be lower as compared to VD. Although number of studies
suggested that CS delivery is a major risk of maternal so the present study suggested
that there are some demographic and medical factors which are directly or indirectly
molding the occurrence of CS deliveries. At some point, medical advisors and pregnant
women can change the scenario of CD of India. It was recommended from the study that
the obstetrical interventions should be evidence-based and the intervention should
strictly be applied to women with complications.






