

Subscribe to RSS
DOI: 10.4103/wjnm.WJNM_73_19
Rapidly lethal secondary hemophagocytic lymphohistiocytosis predicted by fluorodeoxyglucose positron-emission tomography/computed tomography
Authors


Abstract
Secondary hemophagocytic lymphohistiocytosis (sHLH) is a rare disease with either an indolent or aggressive course. A 29-year-old male presented with fever, polyarthralgias, splenomegaly, retroperitoneal adenopathy, and laboratory findings consistent with Epstein—Barr-mediated sHLH. Consistent with a prior survival analysis by Kim et al., splenic maximum standardized uptake value (SUVmax) >2.52 and bone marrow SUVmax>3.13 on 18F-fuorodeoxyglucose positron emission tomography/computed tomography (18FDG-PET/CT) predicted an aggressive disease with poor treatment response. Despite optimal treatment, the patient rapidly progressed to death within 3 months of symptom onset. This case underscores the potential lethal nature of sHLH, and the evolving role of 18FDG-PET/CT in predicting disease severity and treatment response.
Keywords
Fluorodeoxyglucose positron emission tomography/computed tomography - maximum standardized uptake value - rapidly lethal - secondary hemophagocytic lymphohistiocytosis - survival analysisIntroduction
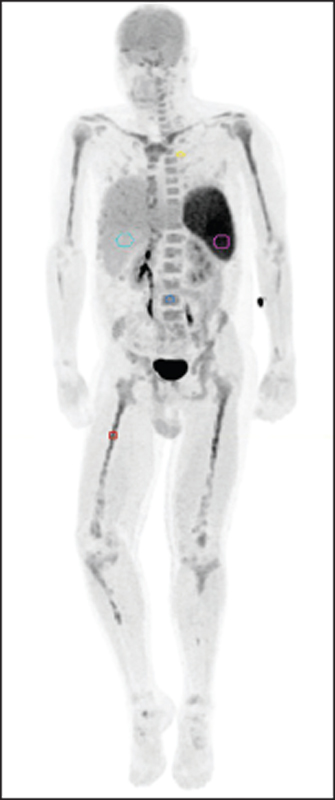
Here, we present a 29-year-old male with rapidly lethal hemophagocytic lymphohistiocytosis (HLH) who died within 3 months of symptom onset despite prompt diagnosis and treatment. The patient initially had 1 month of cyclical fevers and severe lower hemibody polyarthralgias. Diagnostic workup demonstrated profound pancytopenia, thrombocytopenia, hepatosplenomegaly, hypofibrinogenemia, hyperferritinemia, and elevated phosphatase, thus meeting HLH diagnostic criteria.[1] Bone marrow (BM) biopsy revealed hemophagocytosis. Epstein—Barr Virus (EBV) titers suggested recent or past infection, with high viral load clinically consistent with EBV-HLH. An 18F-fluorodeoxyglucose positron-emission tomography/computed tomography (18F-FDG PET/CT) maximum intensity projection [Figure 1] demonstrated diffuse splenic and osseous hypermetabolism.
Axial and sagittal fused images [Figure 2a], [Figure 2b], [Figure 2c], [Figure 2d] demonstrate maximum standardized uptake value (SUVmax) values from multiple sites, notably, 7.1 in the spleen and 4.2 in L 4BM, as well as hypermetabolic peripancreatic and retroperitoneal adenopathy (white arrows). Subsequently, he was treated with HLH-94 protocol of dexamethasone and etoposide with rituxan for EBV viremia. Originally, he improved on this regimen; however, he relapsed with fevers, transaminitis, pancytopenia, disseminated intravascular coagulation, hyperferritinemia, and hypertriglyceridemia, prompting salvage therapy initiation. Two days later, the patient went into cardiac arrest and despite aggressive resuscitation efforts, succumbed to multiorgan failure.

Discussion
HLH is a rare, multiorgan disease, with similarities to lymphoma/leukemia, which can run an indolent or aggressive course. HLH pathophysiology is characterized by unchecked activation of cytotoxic T lymphocytes, natural killer cells, and macrophages resulting in hypercytokinemia and immune-mediated injury of multiple organ. This results in cyclical fevers, splenomegaly, and cytopenia with histological evidence of hemophagocytosis leading to elevated ferritin, lactate dehydrogenase, and soluble CD25.[1],[2] HLH can be broadly classified into two groups: primary HLH and secondary HLH (sHLH), with the former being due to genetic defects in cellular cytotoxicity, while the latter is associated with viral infections, especially EBV, malignancy, and autoimmune diseases.[3] The etiologic distributions of sHLH vary significantly in different studies: a summary study found a 50%:57% infection to neoplasm;[4] another found EBV in 70% cases;[5] and finally, another found in 53.3% with treatment response and mortality ratios of 50:50.[6]
While diagnostic criteria are firmly established based on clinical and pathology findings,[1] identifying patients with aggressive sHLH remains a diagnostic dilemma. As 18F-FDG is absorbed in activated immune cells, including macrophages and T lymphocytes, multiple case studies of HLH have reported hypermetabolism on 18F-FDG PET-CT.[7],[8] Kaplan—Meier survival analysis conducted by Kim et al. demonstrated that PET-CT parameters potentially predict poor outcomes in HLH,[9] whereas clinical parameters failed to do so. Specifically, patients with an SUVmax>2.52 in spleen, SUVmax>3.13 in BM, and spleen to liver and BM to liver SUV ratios exceeding 1.19 and 1.27, respectively, were most likely to have an aggressive, potentially lethal disease course.[9] Our patient demonstrated an SUVmax= 7.1 in the spleen and diffuse BM hypermetabolism with a representative L4 vertebrae SUVmax= 4.2. Liver SUVmax was 2.3 with spleen to liver and BM to liver SUV ratios of 3.09 and 1.83, respectively. As predicted by the analysis in Kim et al., the patient had an aggressive disease with poor treatment response and rapidly succumbed to sHLH. Therefore, we corroborate the evolving distinctive role of PET-CT in stratification of HLH disease severity. 18F-FDG PET-CT offers the best currently available means of identifying which patients have aggressive disease, thus requiring salvage therapy, and those patients in whom current treatment regimens are likely to be successful.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer 2007;48:124-31.
- 2 Fox CP, Shannon-Lowe C, Gothard P, Kishore B, Neilson J, O'Connor N, et al. Epstein-barr virus-associated hemophagocytic lymphohistiocytosis in adults characterized by high viral genome load within circulating natural killer cells. Clin Infect Dis 2010;51:66-9.
- 3 Lu J, Fang Q, Ma C, Su F, Chen G, Huang M, et al. Atypical epstein-barr virus-associated hemophagocytic lymphohistiocytosis simulating lymphadenitis on 18F-FDG PET/CT and its differential diagnosis. Hell J Nucl Med 2017;20:254-7.
- 4 Ramos-Casals M, Brito-Zerón P, López-Guillermo A, Khamashta MA, Bosch X. Adult haemophagocytic syndrome. Lancet 2014;383:1503-16.
- 5 Park HS, Kim DY, Lee JH, Lee JH, Kim SD, Park YH, et al. Clinical features of adult patients with secondary hemophagocytic lymphohistiocytosis from causes other than lymphoma: An analysis of treatment outcome and prognostic factors. Ann Hematol 2012;91:897-904.
- 6 Ahn JS, Rew SY, Shin MG, Kim HR, Yang DH, Cho D, et al. Clinical significance of clonality and epstein-barr virus infection in adult patients with hemophagocytic lymphohistiocytosis. Am J Hematol 2010;85:719-22.
- 7 Yuan L, Kan Y, Meeks JK, Ma D, Yang J 18F-FDG PET/CT for identifying the potential causes and extent of secondary hemophagocytic lymphohistiocytosis. Diagn Interv Radiol 2016;22:471-5.
- 8 Wang J, Wang D, Zhang Q, Duan L, Tian T, Zhang X, et al. The significance of pre-therapeutic F-18-FDG PET-CT in lymphoma-associated hemophagocytic lymphohistiocytosis when pathological evidence is unavailable. J Cancer Res Clin Oncol 2016;142:859-71.
- 9 Kim J, Yoo SW, Kang SR, Bom HS, Song HC, Min JJ. Clinical implication of F-18 FDG PET/CT in patients with secondary hemophagocytic lymphohistiocytosis. Ann Hematol 2014;93:661-7.
Address for correspondence
Publication History
Received: 27 September 2019
Accepted: 06 October 2019
Article published online:
19 April 2022
© 2020. Sociedade Brasileira de Neurocirurgia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Henter JI, Horne A, Aricó M, Egeler RM, Filipovich AH, Imashuku S, et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer 2007;48:124-31.
- 2 Fox CP, Shannon-Lowe C, Gothard P, Kishore B, Neilson J, O'Connor N, et al. Epstein-barr virus-associated hemophagocytic lymphohistiocytosis in adults characterized by high viral genome load within circulating natural killer cells. Clin Infect Dis 2010;51:66-9.
- 3 Lu J, Fang Q, Ma C, Su F, Chen G, Huang M, et al. Atypical epstein-barr virus-associated hemophagocytic lymphohistiocytosis simulating lymphadenitis on 18F-FDG PET/CT and its differential diagnosis. Hell J Nucl Med 2017;20:254-7.
- 4 Ramos-Casals M, Brito-Zerón P, López-Guillermo A, Khamashta MA, Bosch X. Adult haemophagocytic syndrome. Lancet 2014;383:1503-16.
- 5 Park HS, Kim DY, Lee JH, Lee JH, Kim SD, Park YH, et al. Clinical features of adult patients with secondary hemophagocytic lymphohistiocytosis from causes other than lymphoma: An analysis of treatment outcome and prognostic factors. Ann Hematol 2012;91:897-904.
- 6 Ahn JS, Rew SY, Shin MG, Kim HR, Yang DH, Cho D, et al. Clinical significance of clonality and epstein-barr virus infection in adult patients with hemophagocytic lymphohistiocytosis. Am J Hematol 2010;85:719-22.
- 7 Yuan L, Kan Y, Meeks JK, Ma D, Yang J 18F-FDG PET/CT for identifying the potential causes and extent of secondary hemophagocytic lymphohistiocytosis. Diagn Interv Radiol 2016;22:471-5.
- 8 Wang J, Wang D, Zhang Q, Duan L, Tian T, Zhang X, et al. The significance of pre-therapeutic F-18-FDG PET-CT in lymphoma-associated hemophagocytic lymphohistiocytosis when pathological evidence is unavailable. J Cancer Res Clin Oncol 2016;142:859-71.
- 9 Kim J, Yoo SW, Kang SR, Bom HS, Song HC, Min JJ. Clinical implication of F-18 FDG PET/CT in patients with secondary hemophagocytic lymphohistiocytosis. Ann Hematol 2014;93:661-7.