

Subscribe to RSS
DOI: 10.5935/1984-0063.20170019
Retrospectively reported month-to-month variation in sleeping problems of people naturally exposed to high-amplitude annual variation in daylength and/or temperature
Authors

ABSTRACT
Compared to literature on seasonal variation in mood and well-being, reports on seasonality of trouble sleeping are scarce and contradictive. To extend geography of such reports on example of people naturally exposed to high-amplitude annual variation in daylength and/or temperature. Participants were the residents of Turkmenia, West Siberia, South and North Yakutia, Chukotka, and Alaska. Health and sleep-wake adaptabilities, month-to-month variation in sleeping problems, well-being and behaviors were self-assessed. More than a half of 2398 respondents acknowledged seasonality of sleeping problems. Four of the assessed sleeping problems demonstrated three different patterns of seasonal variation. Rate of the problems significantly increased in winter months with long nights and cold days (daytime sleepiness and difficulties falling and staying asleep) as well as in summer months with either long days (premature awakening and difficulties falling and staying asleep) or hot nights and days (all 4 sleeping problems). Individual differences between respondents in pattern and level of seasonality of sleeping problems were significantly associated with differences in several other domains of individual variation, such as gender, age, ethnicity, physical health, morning-evening preference, sleep quality, and adaptability of the sleep-wake cycle. These results have practical relevance to understanding of the roles playing by natural environmental factors in seasonality of sleeping problems as well as to research on prevalence of sleep disorders and methods of their prevention and treatment in regions with large seasonal differences in temperature and daylength.
INTRODUCTION
Despite close association between disordered sleep and depressed mood[1], the findings on seasonal variation in mood and well-being are reported rather frequently as compared to only few reports on seasonal variation in sleeping problems. Moreover, the studies of the effects of season on rate of sleeping problems are mostly limited to populations from Scandinavian countries. These effects were found to be significant in several Norwegian studies[2] - [6], but the significance of these effects was not confirmed in one of the largest Norwegian studies[7]. In one more Norwegian study significant seasonality of sleeping problems was found only in a specific group of respondents experiencing seasonal variation in their well-being, energy, sleep length, socialization, body weight, etc.[8]. Besides, the significant effects of season on frequency of sleeping problems were also documented in astudy the neighboring Finland population[9].
The present paper was mostly aimed on extending geography of studies of seasonal variation in sleeping problems. Compared to Norway and Finland, amplitude of the annual rhythm of air temperature is approximately the same or even higher in such regions as Alaska, Chukotka, North and South Yakutia, West Siberia, and Turkmenia. Therefore, the hypothesis was that, irrespective of degree of seasonal differences in daylength in these six regions, they are characterized by the patterns of month-to-month variation in sleeping problems with more prominent increase in frequency of either all or some of these problems in cold and hot months as compared to other months with more comfortable air temperatures (i.e., winter or summer vs. spring and fall).
A failure to recognize significance of seasonal variation in sleeping problems in a large population sample can be, at least partly, explained by individual variation in responses to questions about particular problems with sleep. Consequently, this paper additionally aimed on examination of possibility of modulation of month-to-month variation in sleeping problems by differences between individuals in sleep-wake behavioral traits, sleep duration, physical and mental health, age, gender, ethnicity, etc.
In sum, the following hypotheses were tested in the present analysis:
sleeping problems demonstrate significant month-to-month variation with peaks in months with extremely cold or hot air temperatures and extremely short or long days;
both pattern and level of seasonality of sleeping problems are modified by differences in several domains of individual variation including gender, age, ethnicity, physical and mental health, sleep quality, morning-evening preference and other traits or adaptive abilities of the sleep-wake cycle.
METHODS
Participants
Questionnaire data were obtained from 2398 residents of Turkmenia, West Siberia, South and North Yakutia, Chukotka, and Alaska. In each of these regions the questionnaire datasets were collected during, at least, two winter seasons. The respondents voluntarily agreed to participate in a questionnaire survey aimed on a search for health correlates of the daily sleep-wake cycle[10]. [Table 1] contains brief description of these regions, [Table 2] includes the list of 12 collected samples and Tables A1 provides some details on studied populations.









The sleep seasonality data have not been reported yet, but some of questionnaire data on self-scored sleep-wake pattern and health have been published previously[10] - [12]. Data on sleep-wake pattern and health were additionally included in some of present analyses to examine possible impact of individual sleep-wake pattern and health ([Tables 3], [4], [A2]-[A4]) on retrospectively reported seasonality of sleep disturbances ([Table 2]).
SWPAQ
A short (40-item) version of the Sleep Wake Pattern Assessment Questionnaire or SWPAQ[13] , [14] was designed to self-assess individual traits of sleep-wake behavior named Nighttime Sleepability (12-item S scale), Anytime Sleepability (4-item f sub-scale), Anytime Wakeability (4-item w sub-scale), Morning Lateness (12-item M-scale), and Evening Lateness (8-item E-scale). Negative score signifies either inability (S, f, and w <0) or earliness (M and E <0). Details on evaluation of psychometric features and cross-validation of the Russian and English versions of this questionnaire using the students' samples were reported previously[11].
Evidence for external validity of these constructs were provided in several previously published reports[11] , [15] - [19]. To determine test-retest reliability of this questionnaire, it was administered in winter and summer to a subsample of the West Siberian depressives (n=23 of 59). [Table A5] illustrates differences between winter and summer scores on SWPAQ scales and sub-scales as well as correlations between them. All 5 SWPAQ scores (S, f, w, M, and E) were included in the present analysis as covariates or factors ([Tables 3], [4], and [A2]-[S4]).
Health Scorings
In order to self-assess the presence and severity of symptoms of depression, anxiety, and somatic dysfunction, respondents were asked to complete three questionnaire scales combined in one scale. Each question asked a respondent to indicate how often during the past week he/she had experienced a particular symptom. Responses about frequency of symptoms ranged from 0 (never or rarely) to 3 (most or all of the time) on a four-point scale. The 20-item Center for Epidemiological Studies -Depression scale or CES-D[20] and the 20-item Zung Self-Rating Anxiety Scale or SAS[21] were used for self-assessment of symptoms of depression and anxiety, respectively.
Scores > 16 indicated moderate or severe depressive and anxiety symptoms ([Tables 4]). Somatic symptoms suggesting alternations of body functioning due to depression, anxiety and physical conditions were self-assessed with 12-item somatization subscale of Symptom Checklist Inventory or SCL S[22] , [23]. A score >6 was identified as indicating a perceived moderate or severe alternation of the body functions ([Table 4]).
Additionally, respondents answered to a simple question asking whether their current general health is very poor, poor, fair, good or excellent. Such Health score ranged from 1 to 5, respectively, with scores 1 or 2 interpreted as indicating perceived problems with health and well-being ([Table 4]). In total, 4 different health scores (CES-D, SAS, SCL S, and Health) were included in the present analysis ([Tables 3], [4], [A2], and [A3]). Sample-averaged scores are given in [Table A1].
SPAQ
All respondents completed the Seasonal Pattern Assessment Questionnaire or SPAQ[24] in its modified version. The SPAQ is a retrospective questionnaire for self-assessment of seasonality of well-being, mood and behaviors. The first part of the SPAQ inquires "To what degree do the following change with the seasons?" for six items, sleep length, social activity, mood, weight, appetite, and energy level. Responses to each item were 0 (none), 1 (mild), 2 (moderate), 3 (marked), or 4 (extreme). The sum of these six items is the Global Seasonality Score (GSS) that, therefore, ranges from 0 to 24. The severity of problems with seasonality is also queried by a single "Problem" question: "How much of a problem are these seasonal changes?" with choices being 0 (none), 1 (mild), 2 (moderate), 3 (marked), 4 (severe), or 5 (disabling).
To determine test-retest reliability of these questionnaire scorings, it was administered twice to a subsample of the West Siberian sample of depressives (n=20 of 59), first in winter when they were suffering from mild or moderate winter depression and then in summer when they remitted. It seemed that retrospective self-assessments did not change much because the differences between winter and summer GSS and Problem scorings were found to be non-significant (Paired t-test: t=1.4 and 0.8, respectively, p>0.05 for both). The Spearman coefficient of correlation was very high for GSS (0.845, p<0.001) thus suggesting its excellent test-retest reliability. However, the coefficient was lower albeit still significant for Problem scoring (0.458, p<0.05).
The present analysis focused on the second part of the SPAQ requesting respondents to fill in the month or months of the year (if any) when they feel best, feel worst, eat least, eat most, socialize least, socialize most, lose most weight, gain most weight, etc. (i.e., "Are any month(s) during the year when you .?"). This original list included only two sleep characteristics, sleep most and sleep least, that are not always pointing at any problems with sleep. Therefore, several additional questions were added to these 10 questions.
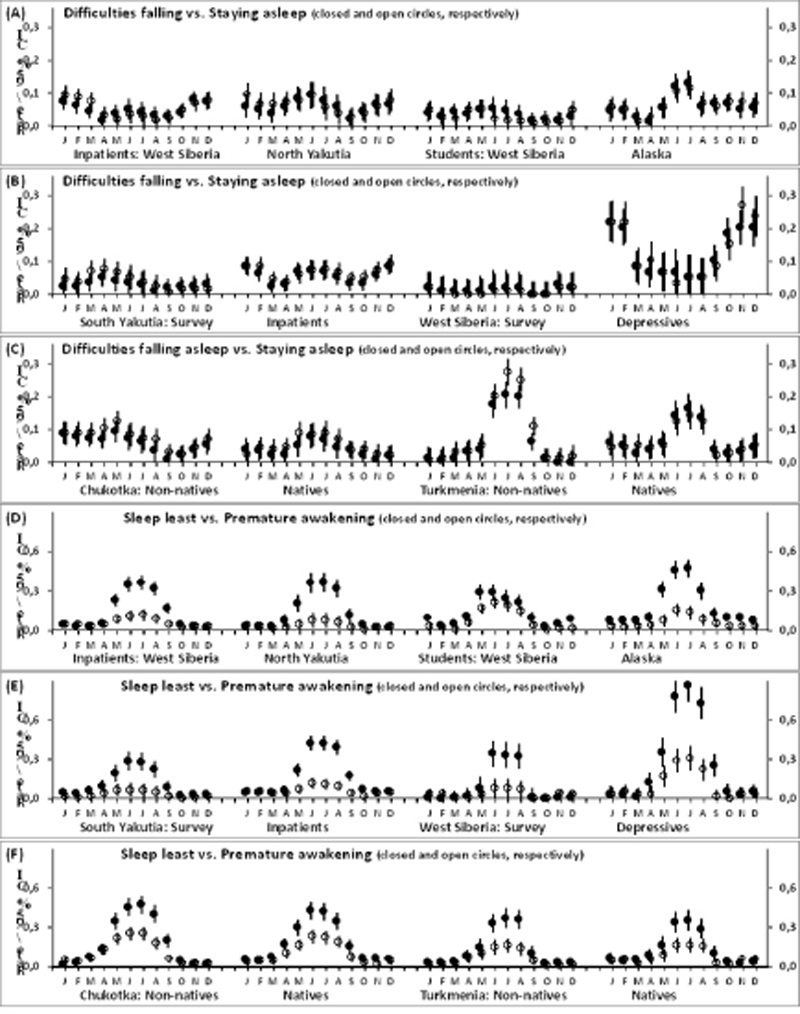
Four of these additional questions asked about common symptoms of disturbed sleep, such as daytime sleepiness, difficulties falling asleep, difficulties staying asleep, and premature awakening. [Figures 1A]-[F] and [2A]-[C] illustrate month-to-month variation in rate of each of these four sleeping problems and, additionally, in two sleep length characteristics from the original list of 10 questions in each of 12 collected samples.

After answering the questions about seasonality of their sleep lengths respondents were also asked to roughly estimate what is the maximal, minimal, and mean length. Mean sleep length (S length) was included in the present analysis as one of modulators of retrospectively reported seasonality ([Tables 3], [4], [A2], and [A3]).
The responses to the set of four questions about sleeping problems were summed for calculation of 4-item sleep score. Similarly, three other sums of four responses were obtained to score seasonality of several depression symptoms (feel worst, least energetic, socialize least, and most irritable) and bipolar neuro-vegetative symptoms prevailing either in spring-summer months or in fall-winter months (either sleep least, feel best, most energetic and socialize most or sleep most, eat most, gain most weight and crave most for carbohydrate-enriched food, respectively).
Summation of answers Yes=1 to each set of four questions provided a score ranging from 0 to 4. Month-to-month variation in 4-item sleep score is illustrated in [Figure 2D]-[F] for each of 12 samples, and variation in four 4-item scores observed in the whole sample is illustrated in [Figure 3]. Percentage of respondents from each sample who reported seasonality of, at least, one of four sleeping problems is given in the 3rd column of [Table 2].

The questionnaires' content and the procedure of questionnaire administration complied with the ethical standards on human studies of the Ethics Committee of the Siberian Branch of the Russian Academy of Medical Sciences and with the Helsinki Declaration of 1975, as revised in 2008. Each respondent studied in clinical settings gave written informed consent.
Statistical Analysis
The SPSS statistical software package (IBM, Armonk, NY, USA, version 22.0) was used to run ANCOVAs and repeated measure ANOVAs (rANOVAs) and ANCOVAs (rANCOVAs) to detect significant month-to-month variation in 4-item scores. Degrees of freedom were corrected using Greenhouse-Geisser correction controlling for type 1 error associated with violation of the sphericity assumption, but the original degrees of freedom are reported in the tables.
Additionally, difference between sleep scores averaged over two winter (January and February) and two fall months (September and October) was calculation as well as difference between mean summer score (June and July) and the same mean fall score. Two ANCOVAs were applied to test whether these differential (winter and summer vs. fall) scores can be significantly different in 12 samples ([Table A4]).
RESULTS
Seasonal variation in for separate sleeping problems
Patterns of month-to-month variation in only two of four sleeping problems, difficulties falling and staying asleep, showed close similarity ([Figure 1A]-[C]). Most often, they had a two-peak wave-form, whereas the pattern of premature awakening suggested annual rather than semi-annual (one-peak rather than two-peak) rhythmicity. It resembled that of sleep shortening, but was characterized by lower amplitude ([Figure 1D]-[F]). The pattern of variation in daytime sleepiness demonstrated some similarity to the pattern of sleep lengthening but only in five northern regions, West Siberia, South and North Yakutia, Chukotka, and Alaska ([Figure 1A]-[C]). It closely resembled the pattern of such depressive symptom as least energetic (not shown) in any of six regions (i.e., these five northern regions and the southernmost region of Turkmenia).
Variation in sum of sleeping problems
As it is shown in [Table 2], percentage of respondents answered "Yes" to, at least, one of 4 questions about seasonality of sleep problems was very high, from 24% to 61% in 11 samples, and 93% in the 12th sample of seasonally depressed women. Highly significant intercept was yielded by one-way rANOVAs of 4-item sleep score ([Table 2]) indicating that seasonality of problematic sleep was perceived by respondents from any of 12 samples. In overall, such seasonality was noted by every other respondent in the merged sample of almost 24 hundred respondents living under natural exposure to high-amplitude annual variation in temperature and/or day length.
Seasonal variation in sum of sleeping problems
Difference between winter and fall sleep scores reported by Chukotka non-natives was significantly higher than that of Chukotka natives, Alaskan students, and Turkmenia non-natives and natives ([Table A4]). Comparison of respondents in the region with summer hot temperature and the regions with winter short day indicated that annual rhythmicity of sleeping problems was higher in the former region. For instance, there was a strong summer peak of these problems in the southern region. Difference between summer and fall sleep scores reported by respondents from the samples of Turkmenia non-natives and natives was significantly higher than in samples from northern regions ([Table A4] and [Figure 2D]-[F]). The only exception were non-native residents of Chukotka villages who were exposed consequently to such natural sleep disturbing factors as long nights in November and December, then cold temperatures till April, and, finally, short days from May to August ([Table A4] and [Figure 2D]-[F]).
Since the cumulative impact of all natural environmental factors usually reached its peak twice during each year, in winter and summer seasons, but not in intermediate months, a bimodal (semi-annual) rhythm was revealed in the vast majority of samples after summing responses to four questions about sleeping problems ([Figure 2]D-F).
After averaging over 12 samples, winter and summer peaks of similar height emerged ([Figure 3], left curves). Amplitude of such two-peak variation was lower compared to amplitude of variation in other three 4-item scores calculated for assessing seasonality of depressive and bipolar neuro-vegetative symptoms ([Figure 3], other curves). Nevertheless, one-way rANOVA of for 4-item sleep score ([Table 2]) yielded highly significant main effect of repeated measure Month. For all but one sample, highly significance effect was documented (p<0.001).
Values of partial eta-squared varied within a range from 0.02 to 0.25 indicating that the effect sizes were either small or moderate or large. Small sizes (partial eta-squared between 0.02 and 0.05) were most usually found, whereas sizes were large only in samples of West Siberian winter depressives and residents of Turkmenia. Much higher values (from 0.18 to 0.72) were obtained for Intercept, because more than a half of respondents (52.63% in total) reported seasonality of, at least, one of four sleeping problems ([Table 2]). Therefore, the result of comparison of partial eta-squared values for Month and Intercept suggested a considerable individual difference between respondents in retrospectively reported month(s) with problematic sleep ([Table 2]).
Influence of individual differences on seasonal variation in sleeping problems
Results of rANCOVAs of sleep score ([Tables A2] and [A3]) suggested that main effects of repeated measure Month turned to become non-significant after accounting for 11 covariates including age, four health self-scorings, 5 self-scorings of sleep-wake traits, and sleep length. Similarly, ANCOVAs of two differential scores did not yield significant main effect after accounting for covariates (see notes to [Table A4]). In contrast, these effects remained significant when rANCOVAs was run for all four 4-item seasonality scores ([Tables 3] and [4]). Again, such findings on sleep score suggested contribution of individual differences to variation in retrospectively reported month(s) with problematic sleep.
Results given in [Table A3] provide some details on the revealed difference in patterns of month-to-month variation in sleeping problems. For instance, differences detected in pairs of samples from the same region emerged as significant interaction between independent factor Sample and repeated measure Month. Such interaction reflects, for example, the fact that some samples from northern Russian regions were and some other were not characterized by high rate of sleeping problems in months belonging to calendar spring season. Significant dissimilarity between several studied samples on amplitude of annual variation was also documented. Particularly, difference between winter and fall sleep scores was dissimilar in several samples from the same region ([Table A4]).
Additionally, rANCOVAs revealed relationships between particular domains of individual variation and difference between respondents in sleep seasonality. [Tables 3], [4], [A2]-[A4] and [Figure 3] illustrate that seasonality of sleeping problems was more likely reported by female respondents of younger age with symptoms of somatic disfunctioning, low nighttime sleepability, low anytime wakeability, and morning lateness. As expected, significant main effect was yielded irrespective of sample for only one of 11 covariates.
This was Nighttime Sleepability (scale S of the SWPAQ) designed to self-assess sleep quality ([Figure 2D]-[F] and [Tables 2], [A2]-[A4]). Individual differences in pattern of seasonality of sleeping problems, such as difference in height of winter peak relative to summer peaks, were related to differences between respondents in gender, severity of physical health problems, and various sleep-wake traits. Female gender and anytime sleepability/wakeinability were associated with higher scores in winter months. Poor physical health and morning/evening lateness were associated with higher summer scores ([Figure 3]). Surprisingly, any of rANCOVAs with depression and anxiety self-scorings as covariates ([Tables 3], [A2]-[A4]) or factors ([Table 4]) did not reveal significance of their effects on level and pattern of seasonal changes in trouble sleeping. Similarly, these rANCOVAs indicated that a significant linear relationship of mean sleep duration to self-reported seasonality of sleeping problems was not revealed ([Tables 2] and [3]).
DISCUSSION
Although symptoms of sleep disturbances usually coexist with symptoms of depression, findings on month-to-month variation in trouble sleeping are mixed and rare as compared to more often reported results on seasonal variation in mood and well-being. Conflicting conclusions about seasonality of sleeping problems were made in several studies of Scandinavian populations. Such seasonality was found to be significant in the majority of them[2] - [6] , [9], but not in one of the largest Norwegian study[7].
Moreover, one more study revealed significant seasonality of sleeping problems only in those of respondents who also experienced seasonality of their well-being, mood and behaviors[8]. The present paper extended geography of reports on month-to-month variation in sleeping problems. The results of analysis of retrospective self-ratings made by almost 24 hundred people living under natural exposure to high-amplitude annual variation in temperature and/or day length indicate that more than a half of them retrospectively reported seasonality of, at least, one of four studied sleeping problems.
Each of the three patterns of month-to-month variation in four sleeping problems can be linked to certain seasonal extremes of photic and temperature environment. Hot nights and long days were found to be associated with increase of premature awakening and difficulties falling and staying asleep. Hot days were additionally associated with increase of daytime sleepiness. Long nights, either without or combined with cold temperatures, were related to increase of daytime sleepiness and difficulties falling and staying asleep.
Thus, natural seasonal factors seemed to modulate frequencies of the four sleeping problems in certain months of the year. For example, in the absence of access to air conditioning, hot temperatures in summer were related to the largest from the observed seasonal rises of sleeping problems. Moreover, three of four sleeping problems tended to increase in response to either long days without hot temperatures or short days with cold temperatures. Moreover, comparison of seasonality of sleep score in samples collected in different regions suggested that cold temperature can be an additional to a day length contributor to winter sleeping problems. In general, the results of the present analysis supported the hypothesis that sleeping problems demonstrate significant month-to-month variation with peaks in months with extremely cold or hot air temperatures that might be or might not be combined with extremely short or long days, respectively.
It appears that the rates of all four sleeping problems cannot simultaneously increase under such natural environmental conditions as long days or short days accompanied by cold temperatures. If difficulties with initiating and maintaining sleep increased in months with extremal photic and temperature environmental conditions of both winter and summer seasons, the extremes of winter season were not associated with premature awakenings.
Moreover, daytime sleepiness seems to represent another group of symptoms of sleep-wake disturbance that was separated by factor analysis from the main group including disturbances before, during and after night sleep[25]. Therefore, it came as no surprise that month-to-month variation in daytime sleepiness more resembled the variation in some of neuro-vegetative symptoms of depression, such as lack of energy and other daytime impairments than any of sleep characteristics including sleep lengthening.
Notably, we earlier showed that the phase of annual variation in these symptoms as well the phase of annual variation in mood and well-being seemed to remarkably delay relative to the phase of annual rhythm of day length, Instead, these phases were in synch with the annual rhythm of air temperature that was approximately a month behind the annual rhythm of day length[19].
In contrast, the annual variation in phase characteristics of the sleep-wake cycle (e.g., the phases of seasonal problems associated with going to bed and awakening) only slightly delayed relative to the phase of annual rhythm of photoperiod, and a phase of seasonal variation in sleep length showed an intermediate position (approximately two-week delay).
These differences between phases of annual variation in the studied sleep and depressive symptoms suggested a possibility of their differential relationship with environmental annual rhythms[19]. However, a cross-sectional questionnaire study does not allow examination of causal relationship between such annual rhythmicities in physical environment and annual or semi-annual rhythmities of sleep and mood problems.
It is likely that individual differences in presence or absence of each of several sleeping problems led to manifestation of individual differences in pattern of month-to-month variation in score summing these problems. For instance, two respondents can differ in the particular list of their sleep complaints (e.g., difficulty falling asleep might be typical for one whereas premature awakening might be typical for another), and this can be a reason for a difference between them in the pattern of seasonal changes in such summing score.
At least, differences between respondents in the level and pattern of annual or semi-annual (one- or two-peak) variation in sum of four sleeping problems were found to be significantly associated with other differences between them, including differences in gender, age, ethnicity, physical health, morning-evening preference, sleep quality, and such adaptabilities of the sleep-wake cycle as anytime wakeability and anytime sleepability. For instance, significant interactions with morning lateness ([Tables 3] and [4]) indicated that, depending upon individual chronotype, sleep problems might be more or less prevalent in summer season ([Figure 3F]). In general, the result of the present analysis supported the hypothesis of import contribution of individual differences to both level and pattern of seasonal oscillations of sleep problems.
This result can explain the failure of some of large questionnaire studies to uncover such oscillations on a population level when Sivertsen et al.[7] asked Norwegians living at latitude 63°-65° about their sleep quality in each of 11 different months rather than about experience associated with changes in sleep quality throughout the year). Moreover, this result provides support and further extends the finding of Øyane et al.[8] on seasonality of sleeping problems self-reported by people experiencing seasonal changes in well-being, mood and behaviors. It was found in the present study that sleeping problems peaked at winter more frequently in self-reports of people representing winter type of seasonal depression as compared to people from three other West Siberian samples.
As can be seen in [Table A5], Nighttime Sleepability (S) was the only SWPAQ' s scale which score significantly changed with change from winter to summer season thus indicating significant improvement of subjective sleep quality and the lack of shift of other (trait-like) characteristics of their sleep-wake pattern. However, our experimental experience showed that it is hard to confirm such high amplitude seasonality of trouble sleeping in analysis of the corresponding objective polysomnographic measurements in laboratory conditions where winter depressives are not exposed to additional sleep disturbing influences of their home environment[26].
Notably, seasonality of sleeping problems simply became non-significant after accounting for several various sources of individual differences between the respondents. In contrast, seasonality still remained significant in the analysis of the whole set of 16 (4x4) responses to questions about month(s) of feeling best or worst, eating least or most, etc.
This result can provide a partial explanation of why the literature on seasonality in human populations contains disproportionally smaller amount of definitely positive findings on month-to-month changes in trouble sleeping compared to findings on significant seasonality of mood and well-being (e.g., such literature include the cited above study of Øyane et al.[8] who applied the SPAQ in its original version). Unlike relationship between individual patterns of the daily sleep-wake cycle and mental health[10], seasonality of sleeping problems was not significantly modulated by self-scored levels of depression and anxiety after accounting for other covariates including physical health problems manifested in somatic complaints and low general health self-scoring.
This result can be an additional partial explanation of the contrast between numerous findings on well-being and mood seasonality and inconclusive results on seasonality of sleep disturbances in general population exposed to high-amplitude annual variation in day length. There was no indication of a link between mean sleep duration and seasonality of sleeping problems. However, only a linear relationship was tested in the present analysis. Therefore, a non-linear (U-shaped) relationship that was earlier shown for association between sleep duration and self-scored health[12] cannot be excluded.
The present results have practical relevance to understanding of contribution of seasonal environmental factors to frequency of sleep disorders. This contribution is necessary to take into account in studies of prevalence of these disorders and in clinical trials aimed on their preventing and treating in regions with large seasonal differences in day length and/or temperature. Moreover, it is needed to take into account in such studies and trials that there are several domains of individual differences contributing to variation in pattern and/or level of seasonality of sleeping problems, such as the differences in gender, age, ethnicity, physical health, morning-evening preference, sleep quality, and adaptability of the sleep-wake cycle.
However, several limitations of this study require acknowledgement. The collected samples do not represent the general populations of six regions. Therefore, it is hard to generalize the present results to other groups of people living on huge territory from Turkmenia to Alaska. The application of cross-sectional and non-repeated measures design was a serious methodological limitation of the present study. Moreover, respondents were not blind to the seasonality hypothesis when they were directly asked about perceived seasonal changes.
Definitely, rates of month-to-month variation obtained from retrospective reports were considerably overestimated. Agreement to participate in the questionnaire survey can also have impact on these rates because it is likely that those people who experienced serious health and sleep problems in certain seasons expressed their interest in filling the questionnaires more often than those who did not.
Unfortunately, a possibility of evaluation of confounding influence of other than temperature and day length environmental factors causing seasonal sleep disturbance was not considered in the present study. In particular, impact of outdoor light exposure and any of factors from workplace or residential home environment on sleep was not assessed.
A list of individual differences between respondents that were analyzed in the present report is far from being comprehensive. In particular, possible influence of none of cultural and psychological differences was assessed in the present questionnaire study. However, remarkable contribution of such differences to retrospective self-ratings cannot be excluded.
Finally, none of the analyzed variables was obtained by means of objective measurements in home settings. This can be one of the directions of future research. Another direction can be to study seasonal variation in sleeping problems longitudinally.
CONCLUSIONS
In the present study, seasonality of sleeping problems was reported by more than a half of respondents. Four sleeping problems demonstrated three different patterns of month-to-month variation. Natural periodic environment seemed to contribute to the pattern and amplitude of annual rhythmicity of each sleeping problem. Increase of all four sleeping problems was associated with only one seasonal factor, hot summer temperatures. Individual differences in sleep seasonality were significantly linked to several other domains of individual variation. Present results have practical relevance to understanding of importance of seasonal environmental factors and individual differences for manifestation of various symptoms of disturbed sleep-wake cycle.
Conflict of Interests
The authors have no conflict of interests to declare.
-
REFERENCES
- 1 Sivertsen B, Salo P, Mykletun A, Hysing M, Pallesen S, Krokstad S, et al. The bidirectional association between depression and insomnia: the HUNT study. Psychosom Med. 2012;74(7):758-65.
- 2 Husby R, Lingjaerde O. Prevalence of reported sleeplessness in northern Norway in relation to sex, age and season. Acta Psychiatr Scand. 1990;81(6):542-7.
- 3 Pallesen S, Nordhus IH, Nielsen GH, Havik OE, Kvale G, Johnsen BH, et al. Prevalence of insomnia in the adult Norwegian population. Sleep. 2001;24(7):771-9.
- 4 Friborg O, Bjorvatn B, Amponsah B, Pallesen S. Associations between seasonal variations in day length (photoperiod), sleep timing, sleep quality and mood: a comparison between Ghana (5°) and Norway (69°). J Sleep Res. 2012;21(2):176-84.
- 5 Friborg O, Rosenvinge JH, Wynn R, Gradisar M. Sleep timing, chronotype, mood, and behavior at an Arctic latitude (69°N). Sleep Med. 2014;15(7):798-807.
- 6 Johnsen MT, Wynn R, Bratlid T. Is there a negative impact of winter on mental distress and sleeping problems in the subarctic: the Tromsø Study. BMC Psychiatry. 2012;12:225.
- 7 Sivertsen B, Overland S, Krokstad S, Mykletun A. Seasonal variations in sleep problems at latitude 63°-65° in Norway: The Nord-Trondelag Health Study, 1995-1997. Am J Epidemiol. 2011;174(2):147-53.
- 8 Øane NM, Ursin R, Pallesen S, Holsten F, Bjørvatn B. Self-reported seasonality is associated with complaints of sleep problems and deficient sleep duration: the Hordaland Health Study. J Sleep Res. 2008;17(1):63-72.
- 9 Ohayon MM, Partinen M. Insomnia and global sleep dissatisfaction in Finland. J Sleep Res. 2002;11(4):339-46.
- 10 Putilov AA. Association of morning and evening lateness with self-scored health: Late to bed and early to rise makes a man healthy in his own eyes. Biol Rhythm Res. 2008;39(4):321-33.
- 11 Putilov AA, Putilov DA. Sleepless in Siberia and Alaska: Cross-validation of factor structure of the individual adaptability of the sleep-wake cycle. Ergonomia. 2005;27(3):207-226.
- 12 Putilov AA. Patterns of association of health problems with sleep-wake timing and duration. J Sleep Disord Treat Care. 2013;2(4). DOI: 10.4172/2325-9639.1000120
- 13 Putilov AA. A questionnaire for self-assessment of individual traits of sleep-wake cycle. Bull Sib Branch USSR Acad Med Sci. 1990;1:22-25. (in Russian).
- 14 Putilov AA. A questionnaire for self-assessment of individual profile and adaptability of sleep-wake cycle. In: Gutenbrunner C, Hildebrandt G, Moog R, eds. Chronobiology and Chronomedicine 1991: Basic Research and Application: Proceedings of the 7th Annual Meeting of the European Society for Chronobiology, Marburg, 1991. Frankfurt am Main: Peter Lang; 1993. p. 492-8.
- 15 Putilov AA. Association of the circadian phase with two morningness-eveningness scales of an enlarged version of the sleep-wake pattern assessment questionnaire. In: Hornberger S, Peter Knauth P, Giovanni Costa G, Folkard S, eds. Shiftwork in the 21st Century - Challenges for Research and Practice. Series: Arbeitswissenschaft in der betrieblichen Praxis. Frankfurt am Main: Peter Lang; 2000. p. 317-22.
- 16 Putilov AA. Validation of nighttime sleepability scale against objective and subjective measures of sleep quality. Sleep Hypn. 2016. E-pub ahead of print. DOI: 10.5350/Sleep.Hypn.2016.18.0131
- 17 Putilov AA, Donskaya OG, Verevkin EG. How many diurnal types are there? A search for two further "bird species". Pers Individ Dif. 2015;72:12-7.
- 18 Putilov AA, Donskaya OG, Budkevich EV, Budkevich RO. Reliability and external validity of the six scales of 72-item Sleep-Wake Pattern Assessment Questionnaire (SWPAQ). Biol Rhythm Res. 2017;48(2):275-85. DOI: 10.1080/09291016.2016.1254872
- 19 Putilov AA, Russkikh GS, Danilenko KV. Phase of melatonin rhythm in winter depression. Adv Exp Med Biol. 1999;460:441-58.
- 20 Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385-401.
- 21 Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371-9.
- 22 Derogatis LR, Lipman RS, Covi L. SCL-90: an outpatient psychiatric rating scale--preliminary report. Psychopharmacol Bull. 1973;9(1):13-28.
- 23 Derogatis LR, Rickels K, Rock AF. The SCL-90 and the MMPI: a step in the validation of a new self-report scale. Br J Psychiatry. 1976;128:280-9.
- 24 Rosenthal NE, Bradt GH, Wehr TA. Seasonal Pattern Assessment Questionnaire. Bethesda: National Institute of Mental Health; 1984.
- 25 Koffel E, Watson D. The two-factor structure of sleep complaints and its relation to depression and anxiety. J Abnorm Psychol. 2009;118(1):183-94.
- 26 Palchikov VE, Zolotarev DY, Danilenko KV, Putilov AA. Effects of season and of bright light administered at different times of day on sleep EEG and mood in patients with seasonal affective disorder. Biol Rhythm Res. 1997;28(2):166-84.
Corresponding author:
Publication History
Received: 12 April 2017
Accepted: 25 July 2017
Article published online:
11 October 2023
© 2023. Brazilian Sleep Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
REFERENCES
- 1 Sivertsen B, Salo P, Mykletun A, Hysing M, Pallesen S, Krokstad S, et al. The bidirectional association between depression and insomnia: the HUNT study. Psychosom Med. 2012;74(7):758-65.
- 2 Husby R, Lingjaerde O. Prevalence of reported sleeplessness in northern Norway in relation to sex, age and season. Acta Psychiatr Scand. 1990;81(6):542-7.
- 3 Pallesen S, Nordhus IH, Nielsen GH, Havik OE, Kvale G, Johnsen BH, et al. Prevalence of insomnia in the adult Norwegian population. Sleep. 2001;24(7):771-9.
- 4 Friborg O, Bjorvatn B, Amponsah B, Pallesen S. Associations between seasonal variations in day length (photoperiod), sleep timing, sleep quality and mood: a comparison between Ghana (5°) and Norway (69°). J Sleep Res. 2012;21(2):176-84.
- 5 Friborg O, Rosenvinge JH, Wynn R, Gradisar M. Sleep timing, chronotype, mood, and behavior at an Arctic latitude (69°N). Sleep Med. 2014;15(7):798-807.
- 6 Johnsen MT, Wynn R, Bratlid T. Is there a negative impact of winter on mental distress and sleeping problems in the subarctic: the Tromsø Study. BMC Psychiatry. 2012;12:225.
- 7 Sivertsen B, Overland S, Krokstad S, Mykletun A. Seasonal variations in sleep problems at latitude 63°-65° in Norway: The Nord-Trondelag Health Study, 1995-1997. Am J Epidemiol. 2011;174(2):147-53.
- 8 Øane NM, Ursin R, Pallesen S, Holsten F, Bjørvatn B. Self-reported seasonality is associated with complaints of sleep problems and deficient sleep duration: the Hordaland Health Study. J Sleep Res. 2008;17(1):63-72.
- 9 Ohayon MM, Partinen M. Insomnia and global sleep dissatisfaction in Finland. J Sleep Res. 2002;11(4):339-46.
- 10 Putilov AA. Association of morning and evening lateness with self-scored health: Late to bed and early to rise makes a man healthy in his own eyes. Biol Rhythm Res. 2008;39(4):321-33.
- 11 Putilov AA, Putilov DA. Sleepless in Siberia and Alaska: Cross-validation of factor structure of the individual adaptability of the sleep-wake cycle. Ergonomia. 2005;27(3):207-226.
- 12 Putilov AA. Patterns of association of health problems with sleep-wake timing and duration. J Sleep Disord Treat Care. 2013;2(4). DOI: 10.4172/2325-9639.1000120
- 13 Putilov AA. A questionnaire for self-assessment of individual traits of sleep-wake cycle. Bull Sib Branch USSR Acad Med Sci. 1990;1:22-25. (in Russian).
- 14 Putilov AA. A questionnaire for self-assessment of individual profile and adaptability of sleep-wake cycle. In: Gutenbrunner C, Hildebrandt G, Moog R, eds. Chronobiology and Chronomedicine 1991: Basic Research and Application: Proceedings of the 7th Annual Meeting of the European Society for Chronobiology, Marburg, 1991. Frankfurt am Main: Peter Lang; 1993. p. 492-8.
- 15 Putilov AA. Association of the circadian phase with two morningness-eveningness scales of an enlarged version of the sleep-wake pattern assessment questionnaire. In: Hornberger S, Peter Knauth P, Giovanni Costa G, Folkard S, eds. Shiftwork in the 21st Century - Challenges for Research and Practice. Series: Arbeitswissenschaft in der betrieblichen Praxis. Frankfurt am Main: Peter Lang; 2000. p. 317-22.
- 16 Putilov AA. Validation of nighttime sleepability scale against objective and subjective measures of sleep quality. Sleep Hypn. 2016. E-pub ahead of print. DOI: 10.5350/Sleep.Hypn.2016.18.0131
- 17 Putilov AA, Donskaya OG, Verevkin EG. How many diurnal types are there? A search for two further "bird species". Pers Individ Dif. 2015;72:12-7.
- 18 Putilov AA, Donskaya OG, Budkevich EV, Budkevich RO. Reliability and external validity of the six scales of 72-item Sleep-Wake Pattern Assessment Questionnaire (SWPAQ). Biol Rhythm Res. 2017;48(2):275-85. DOI: 10.1080/09291016.2016.1254872
- 19 Putilov AA, Russkikh GS, Danilenko KV. Phase of melatonin rhythm in winter depression. Adv Exp Med Biol. 1999;460:441-58.
- 20 Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385-401.
- 21 Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371-9.
- 22 Derogatis LR, Lipman RS, Covi L. SCL-90: an outpatient psychiatric rating scale--preliminary report. Psychopharmacol Bull. 1973;9(1):13-28.
- 23 Derogatis LR, Rickels K, Rock AF. The SCL-90 and the MMPI: a step in the validation of a new self-report scale. Br J Psychiatry. 1976;128:280-9.
- 24 Rosenthal NE, Bradt GH, Wehr TA. Seasonal Pattern Assessment Questionnaire. Bethesda: National Institute of Mental Health; 1984.
- 25 Koffel E, Watson D. The two-factor structure of sleep complaints and its relation to depression and anxiety. J Abnorm Psychol. 2009;118(1):183-94.
- 26 Palchikov VE, Zolotarev DY, Danilenko KV, Putilov AA. Effects of season and of bright light administered at different times of day on sleep EEG and mood in patients with seasonal affective disorder. Biol Rhythm Res. 1997;28(2):166-84.