

Subscribe to RSS
DOI: 10.5935/2526-8732.20200027
Locally Advanced and Metastatic Pancreatic Cancer: Survival analysis and prognostic factors in a case series
Câncer pancreático localmente avançado e metastático: Análise de sobrevivência e fatores prognósticos em uma série de casos
Authors
Financial support: none to declare.
ABSTRACT
Objective: Systemic treatment of advanced pancreatic adenocarcinoma has resulted in increased survival of patients, but real-life data are scarce, particularly in developing countries. This study aims to analyze the survival of patients with locally advanced, unresectable, or metastatic pancreatic cancer and factors related to better survival. Methods: an analytical study with a retrospective and prospective part of data from patients with locally advanced or metastatic pancreatic adenocarcinoma treated between January 2012 to December 2018 in the oncology department of the Real Hospital de Beneficência Portuguesa, in Recife (Brazil). Results: Thirty-five patients were assessed. The median age was 68 years old (71.4% = 65 years old), the majority was male (65.7%), with Eastern Cooperative Oncology Group (ECOG) 0 and 1 (65.7%) and metastatic disease (68.6%). The median overall survival was 13.93 months and was longer for patients with ECOG 0 or 1 (20.4 months; p=0.021), Neutrophil-lymphocyte ratio (NLR) <4 (15.63 months; p=0.029) and who received local therapy (23.68 months; p=0.006). Conclusion: An overall median survival, similar to that of other clinical studies, was observed. Such survival was even better in patients with a good clinical condition (ECOG 0 or 1), low NLR, and who received some local therapy.
RESUMO
Objetivo:O tratamento sistêmico do adenocarcinoma pancreático avançado resultou em aumento da sobrevida dos pacientes, mas os dados da vida real são escassos, principalmente em países em desenvolvimento. Este estudo tem como objetivo analisar a sobrevida de pacientes com câncer de pâncreas localmente avançado, irressecável ou metastático e fatores relacionados a uma melhor sobrevida. Métodos: estudo analítico com parte retrospectiva e prospectiva de dados de pacientes com adenocarcinoma pancreático localmente avançado ou metastático atendidos entre janeiro de 2012 a dezembro de 2018 no serviço de oncologia do Real Hospital Português, Recife, PE, Brasil. Resultados: Trinta e cinco pacientes foram avaliados. A mediana de idade foi de 68 anos (71,4% = 65 anos), a maioria era do sexo masculino (65,7%), com Eastern Cooperative Oncology Group (ECOG) 0 e 1 (65,7%) e doença metastática (68,6%). A sobrevida global mediana foi de 13,93 meses e foi mais longa para pacientes com ECOG 0 ou 1 (20,4 meses; p = 0,021), proporção de neutrófilos-linfócitos (NLR) <4 (15,63 meses; p = 0,029) e que receberam terapia local (23,68 meses; p = 0,006). Conclusão: Foi observada uma sobrevida global mediana, semelhante à de outros estudos clínicos. Essa sobrevida foi ainda melhor em pacientes com bom estado clínico (ECOG 0 ou 1), baixo nível de NLR e que receberam alguma terapia local.
Keywords:
Survival Analysis - Prognosis - Antineoplastic Combined Chemotherapy Protocols - Pancreatic Neoplasms - AdenocarcinomaDescritores:
Análise de sobrevivência - Prognóstico - Antineoplastic Combined Chemotherapy Protocols - Neoplasias pancreáticas - AdenocarcinomaINTRODUCTION
Pancreatic cancer represents the seventh leading cause of cancer mortality in the world, and the second leading cause of cancer death in the United States[1]. Most patients with such neoplasm present at an advanced stage of the disease at diagnosis, approximately 50% with metastatic disease, and 25% to 35% with borderline or locally advanced disease[2]. Gemcitabine plus nab-paclitaxel or FOLFIRINOX represent the first line of chemotherapy treatment in locally advanced and metastatic disease with median overall surival of 8.5 and 11.1 months, respectively[3] [4]. A limitation to be considered concerning randomized controlled trials is the fact that their eligibility criteria are stringent and, as a result, only a small portion of patients with advanced pancreatic cancer is considered able to participate in the studies. Not surprisingly, such a highly select study population generally does not accurately reflect the population of patients in need of treatment[5].
Due to the low survival associated with this neoplasia, different research has directed efforts to identify predictive markers that help to optimize the treatment. Among them, the carbohydrate antigen 19-9 (CA19-9), the performance index evaluated by the ECOG (Eastern Cooperative Oncology Group), age, local therapies, and the status of chronic inflammation represented by the neutrophil/lymphocyte (NLR) and platelet/lymphocyte (PLR) ratio[6] [7].
These last two have been particularly studied due to the advance in the knowledge of immunology in cancer. The NLR is calculated from the absolute values of neutrophils and lymphocytes obtained through the blood count. Many studies indicate that a low NLR (usually less than four or five) is associated with better survival in patients with metastatic pancreatic cancer[8] [9]. PLR (platelet/lymphocyte ratio), calculated from the absolute values of platelets and lymphocytes, was also an unfavorable predictor of overall survival and progression-free survival in patients with pancreatic cancer[10].
Finally, has been studied if local therapy can improve survival in patients with locally advanced pancreatic cancer. A series of cases from a retrospective study by the Johns Hopkins group, for example, showed that patients with locally advanced pancreatic cancer who underwent radiation therapy, at some point in their treatment, had a median overall survival of 13.7 months and 61% disease control in one year[11] and two other studies that used radiotherapy in patients with locally advanced disease reached a median overall survival of 15 months and 12.2 months, respectively[12] [13]. Nevertheless, a large randomized phase III study LAP07 did not show any benefit for radiotherapy being added to chemotherapy[4].
The present study evaluated the clinical and epidemiological characteristics and the factors that influenced the survival of patients with metastatic and unresectable locally advanced pancreatic adenocarcinoma, treated in a private reference hospital for the treatment of cancer in the Brazilian state of Pernambuco.
METHODOLOGY
Study design
Ours is a longitudinal analytical study with a retrospective and prospective part.
Study population
Patients with histological diagnosis of locally advanced or metastatic pancreatic adenocarcinoma who received chemotherapy treatment were selected from the medical archives of the Real Instituto de Oncologia of Hospital Português. The period of diagnosis and treatment was between January 2012 and December 2018, with a minimum of 12 months of follow-up. All patients ongoing active therapy or best supportive care between July 2019 to December 2019 was included in the analyses and represents the prospective part of the study, if they were alive and have completed 12 months of follow-up until December 2019.
Study location and period
Clinical oncology service of the Real Hospital Português and data collected from electronic medical records from July 2019 to December 2019.
Eligibility criteria
Adult patients (> 18 years old)
Histological diagnosis of pancreatic adenocarcinoma Stage III or IV
Patients who underwent at least one chemotherapy treatment session
Medical data on treatment and clinical follow-up available in medical records Minimum of 12-month follow-up period
Exclusion criteria
Patients without the complete data required for the study
Loss of continued service follow-up
Another active tumor (except non-melanoma skin cancer)
Statistical analysis
To characterize the studied sample, the relative (percentage) and absolute (N) frequencies of the classes of each qualitative variable were calculated. For quantitative variables, averages and medians were used to summarize the information, and standard, minimum and maximum deviations to indicate data variability. The level of significance assumed is 5%. Statistical analyzes were performed using SPSS - Statistical Package for Social Sciences, version 21.0 (IBM, Armonk, NY).
For survival analysis, death was considered an event of interest. Initially, we calculated the survival probabilities for the total number of patients using the Kaplan-Meier method. Such a method allows the survival curve to be constructed with estimates of the probabilities of survival as a function of the followup time. Thus, it is possible to know the chance that a patient will survive “so many” months after the diagnosis. These estimates are independent of the patient's condition; that is, information about other measures of the patient is not being considered here. To assess the influence of these variables, such as Clinical Staging, ECOG, NLR and PLR, Kaplan-Meier curves were constructed for the categories of each qualitative variable. In this type of analysis, a significance test is performed for each variable that indicates whether the variable in question influences the patient's survival. To compare the curves, we used the Log-Rank test. The results (graphs and test results) are shown below.
ETHICAL ASPECTS
The research was approved by the Human Research Ethics Committee of Pernambuco's Real Hospital Português de Beneficência. Opinion Number: 3.705.999.
RESULTS
Clinical-demographic characteristics
Forty-three medical records of patients diagnosed with locally advanced or metastatic pancreatic adenocarcinoma were identified in the oncology department. Eight patients were treated in another center and therefore excluded due to loss of followup. Finally, thirty-five patients met all inclusion and exclusion criteria. Most patients were diagnosed between 2016 and 2018 (n=31). The average age was 68 years old, and greater than 70% of patients were older than 65 years of age. Other clinical, demographic and laboratory characteristics are shown in[Table 1].
Survival analysis
The median survival for our entire cohort was 13.39 months, as shown in[Figure 1] (below).

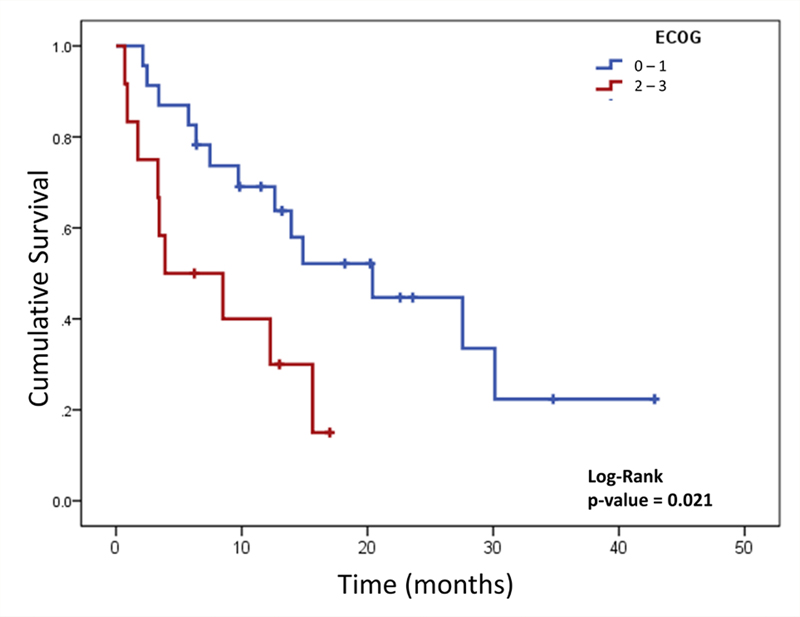
[Table 2] shows survival as a function of clinical and laboratory variables analyzed, and [figures 2]–[4] represent the survival curves according to the variables that show a clinically significant difference, which were ECOG, NLR and local therapy.


|
Variable |
N |
Median survival (months) |
Deaths |
95% IC |
p-value |
|---|---|---|---|---|---|
|
Age (years) <65 |
10 |
14.87 |
05 |
5.58 - 24.15 |
0.270 |
|
=65 |
25 |
13.93 |
17 |
6.25 - 21.61 |
|
|
Clinical Staging Locally Advanced |
11 |
13.93 |
7 |
7.88 - 19.99 |
0.653 |
|
Metastatic |
24 |
14.87 |
15 |
6.29 - 23.44 |
|
|
ECOG 0 - 1 |
23 |
20.4 |
13 |
9.05 - 31.74 |
0.021 |
|
2 - 3 |
12 |
3.9 |
9 |
1.00 - 11.72 |
|
|
NLR < 4 |
21 |
15.63 |
11 |
2.17 - 29.10 |
0.029 |
|
= 4 |
13 |
8.5 |
10 |
0.39 - 16.61 |
|
|
PLR < 150 |
14 |
20.4 |
8 |
2.42 - 38.38 |
0.436 |
|
= 150 |
20 |
12.27 |
13 |
6.87 - 17.67 |
|
|
CA 19-9 < 250 |
16 |
15.01 |
7 |
9.22 - 18.77 |
0.519 |
|
= 250 |
17 |
13.93 |
13 |
5.91 - 21.96 |
|
|
Local therapy[*] Yes |
07 |
23.68 |
2 |
11.23 - 35.17 |
0.006 |
|
No |
28 |
9.73 |
20 |
1.85 - 17.1 |
|
ECOG (Eastern Cooperative Oncology Group. ECOG 0, n =1; ECOG 1, n =22; ECOG 2, n =11; ECOG 3, n =1); NLR (neutrophil / lymphocyte ratio, n=34); PLR (platelet / lymphocyte ratio, n=34); CA 19-9 (carbohydrate antigen 19-9, n=33);
* Local therapy (n=7 [4 patients with locally advanced disease and 3 patients with metastatic disease) ; radiotherapy, n=6; radioablation, n=1); for survival analysis, the Kaplan-Meier model was used and comparisons were assessed using the Log-Rank test. The p value was considered statistical when p <0.05.
Of the 35 treated patients, 11 had locally advanced disease, and 24 had metastatic disease at diagnosis. In locally advanced disease, FOLFIRINOX was the first line of treatment in nine patients (81%). Twenty-eight patients (24 with initial metastatic disease and 4 with locally advanced disease who developed metastases) received first- line therapy. FOLFIRINOX (18 patients, 64.3%), Gemcitabine plus nab-paclitaxel (5 patients, 18%), and gemcitabine monotherapy (4 patients, 14%) were the most widely used chemotherapy regimens. The median survival for first-line patients who received FOLFIRINOX was 12 months (n=27), and those who received gemcitabine + nab- paclitaxel was 13 months (n=5). Seventeen patients (70.8%) with metastatic disease received a second line of chemotherapy treatment. Gemcitabine plus nab-paclitaxel and gemcitabine alone were used as second-line in 41% and 29% of the patients, respectively.
Between ECOG 2 patients (n=11) the first line therapy was gemcitabine alone (n=5), FOLFIRINOX (n=4), and gemcitabine plus nab-paclitaxel (n=2), only three patients received a second line with was gemcitabine plus nab-paclitaxel (n=1), FOLFOX (n=1) and fluorouracil plus leucovorin (n=1). ECOG 3 patient (n=1) received FOLFIRINOX as first line followed by gemcitabine as monotherapy.
DISCUSSION
The present study observed a median overall survival of 13.93 months in patients with unresectable and metastatic locally advanced pancreatic adenocarcinoma-results superior to those found in the two main studies in this group of patients. Those studies observed a higher overall survival for FOLFIRINOX (11.1 months) and the combination gemcitabine plus nab-paclitaxel (8.5 months) in the first line of treatment when compared with gemcitabine alone[3] [4], while our sample had a median survival of 12 months and 13 months, respectively. A study conducted at Instituto do Câncer do Estado de São Paulo, involving 61 patients with advanced pancreatic adenocarcinoma, 31 of whom with metastatic disease, had similar survival to that found in our series[15].
The ability to predict poor survival for patients with a disease as severe as pancreatic cancer is essential in the initial management before treatment to select patients most likely to receive polychemotherapy such as FOLFIRINOX and gemcitabine plus nab-paclitaxel. For that, possible factors associated with worse survival were evaluated, such as age, disease stage, ECOG, NLR, PLR, CA 19-9, and the use of local therapy.
The median age observed was 68 years old, above that reported in the PRODIGE and MPACT studies, which were 61 and 62 years old, respectively[3] [4]. In the present study, we did not note a difference in overall survival when considering the age of 65 years (p=0.27) or 75 years (p=0.16). It's known that in older patients with numerous comorbidities, the treatment of advanced malignancy, such as pancreatic cancer, may not result in clinical benefit and increase the risk of toxicities, clinical decompensation and undertreatment, leading to worse overall survival[16]. Despite this, age has not been a predictor of worse survival in patients selected for clinical trials[7] [17].
Our sample did not show any difference in overall survival when comparing the locally advanced and metastatic clinical stages (13.9 months x 14.8 months; p=0.653). However, despite data in the literature pointing to better survival in locally advanced disease[17] [18] [19], such survival is similar to that observed in our patients.
About one-third of our population had ECOG 2 (n=11, 31.4%), which is different from that observed in clinical studies, where the majority of patients are recruited with better performance. Therefore, more real-life studies are essential to assess the impact of treatments on clinical practice. In the MPACT study 8% of the patients included had ECOG 2 and this group of patients had a worse survival when compared with those with better ECOG[6] [7]. Our sample showed a median overall survival of 3.9 months that is similar to that observed in the MPACT study for the group of ECOG 2 patients who received gemcitabine plus nabpaclitaxel. Likewise, patients with better performance status also had better overall survival (20.4 months x 3.9 months; p=0.021).
Another prognostic factor that has been widely studied is the inflammatory factor. The search for markers of systemic inflammation measured by pretreatment NLR and PLR is a prognostic factor in several studies, which point to a worse survival outcome in patients with elevated NLR and PLR[8] [9] [10]. In our series, a cutoff point indicated by the literature was used and it was observed that patients with an NLR of less than four survived almost twice as long when compared with those with an NLR greater than or equal to four (15.6 months x 8.5 months; p=0.029). However, concerning PLR, when using the cut-off point of 150, as suggested in the literature[10], no difference in overall survival was shown.
The CA 19-9 marker is also studied as a prognostic factor for pancreatic cancer, with contradictory results and variable cut-off points. In some studies, a high value before treatment predicts advanced disease, unresectability, recurrence, and worse overall survival[20] [21] [22] [23]. On the other hand, Tabernero et al. studied this marker as a prognostic factor in patients receiving nab-paclitaxel and gemcitabine and found no correlation with survival[7]. In the present study, the median value of CA 19-9 was 256.98 U/ml. Values above or below the standard reference (37 U/ ml, data not shown) or close to the median, 250 U/ ml, were analyzed as cut-off points and were not related to overall survival (p=0.262 and p=0.519, respectively).
With regard to local therapy, some studies indicate better survival in patients with advanced disease who receive local treatment (radiotherapy or radioablation) at some point in their treatment[11] [12] [13] [24]. Local treatment was used in seven patients in our study, radiotherapy (n=6) and radioablation (n=1), during the treatment of locally advanced (n=4) or metastatic (n=3) disease. These patients survived significantly longer when compared to those who did not (p=0.006). Despite our results, a large randomized trial LAP07, did not shows any benefit for the use of radiation in this setting[14].
As limitations for the present study, we can mention the retrospective and single- centered design and the small number of participants. On the other hand, our study presents information from our daily clinical practice with survival data similar to those observed in phase III clinical studies.
In conclusion, good clinical condition (ECOG 0 or 1), low NLR, and local therapy are associated with better survival in univariate analysis, suggesting their clinical usefulness and applicability in the treatment of locally advanced or metastatic pancreatic cancer.
Conflicts of interest
The authors declare no conflict of interest relevant to this manuscript.
-
REFERENCES
- International Agency of Research on Cancer. Estimated number of new cases in 2018, Asia, Indonesia, both sexes, all ages. World Heal Organ 2018; 876: 2018
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res [Internet] 2014; Jun; 1; 74 (11) 2913-2921 Available from: http://cancerres.aacrjournals.org/cgi/doi/10.1158/0008-5472.CAN-14-0155
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M. et al Increased Survival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine. N Engl J Med [Internet] 2013; Oct; 31; 369 (18) 1691-1703 Available from: http://www.nejm.org/doi/10.1056/NEJMoa1304369
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y. et al FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med [Internet] 2011; May; 12; 364 (19) 1817-1825 Available from: http://www.ncbi.nlm.nih.gov/pubmed/21561347
- Unger JM, Cook E, Tai E, Bleyer A. The Role of Clinical Trial Participation in Cancer Research: Barriers, Evidence, and Strategies. Am Soc Clin Oncol Educ book Am Soc Clin Oncol Annu Meet [Internet] 2016; 35: 185-198 Available from: http://www.ncbi.nlm.nih.gov/pubmed/27249699
- Kadokura M, Ishida Y, Tatsumi A, Takahashi E, Shindo H, Amemiya F. et al Performance status and neutrophil-lymphocyte ratio are important prognostic factors in elderly patients with unresectable pancreatic cancer. J Gastrointest Oncol [Internet] 2016; Dec; 6 (07) 982-988 Available from: http://jgo.amegroups.com/article/view/8283/9417
- Tabernero J, Chiorean EG, Infante JR, Hingorani SR, Ganju V, Weekes C. et al Prognostic Factors of Survival in a Randomized Phase III Trial (MPACT) of Weekly nab-Paclitaxel Plus Gemcitabine Versus Gemcitabine Alone in Patients With Metastatic Pancreatic Cancer. Oncologist [Internet] 2015; Feb; 1; 20 (02) 143-150 Available from: http://theoncologist.alphamedpress.org/cgi/doi/10.1634/theoncologist.2014-0394
- Zhou Y, Wei Q, Fan J, Cheng S, Ding W, Hua Z. Prognostic role of the neutrophil-to-lymphocyte ratio in pancreatic cancer: A meta-analysis containing 8252 patients. Clin Chim Acta [Internet] 2018; Apr; 479: 181-189 Available from: https://linkinghub.elsevier.com/retrieve/pii/S0009898118300329
- Mei Z, Shi L, Wang B, Yang J, Xiao Z, Du P. et al Prognostic role of pretreatment blood neutrophil-to-lymphocyte ratio in advanced cancer survivors: A systematic review and meta-analysis of 66 cohort studies. Cancer Treat Rev [Internet] 2017; Jul; 58: 1-13 Available from: https://linkinghub.elsevier.com/retrieve/pii/S0305737217300853
- Zhou Y, Cheng S, Fathy AH, Qian H, Zhao Y. Prognostic value of platelet-to- lymphocyte ratio in pancreatic cancer: a comprehensive meta-analysis of 17 cohort studies. Onco Targets Ther [Internet] 2018; 11: 1899-1908 Available from: http://www.ncbi.nlm.nih.gov/pubmed/29670365
- Moningi S, Dholakia AS, Raman SP, Blackford A, Cameron JL, Le DT. et al The Role of Stereotactic Body Radiation Therapy for Pancreatic Cancer: A Single-Institution Experience. Ann Surg Oncol [Internet] 2015; Jul; 22 (07) 2352-2358 Available from: http://www.ncbi.nlm.nih.gov/pubmed/25564157
- Chuong MD, Springett GM, Freilich JM, Park CK, Weber JM, Mellon EA. et al Stereotactic body radiation therapy for locally advanced and borderline resectable pancreatic cancer is effective and well tolerated. Int J Radiat Oncol Biol Phys [Internet] 2013; Jul; 1; 86 (03) 516-522 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23562768
- Gurka MK, Collins SP, Slack R, Tse G, Charabaty A, Ley L. et al Stereotactic body radiation therapy with concurrent full-dose gemcitabine for locally advanced pancreatic cancer: a pilot trial demonstrating safety. Radiat Oncol [Internet] 2013; Mar; 1; 8: 44 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23452509
- Hammel P, Huguet F, van Laethem J-L, Goldstein D, Glimelius B, Artru P. et al Effect of Chemoradiotherapy vs Chemotherapy on Survival in Patients With Locally Advanced Pancreatic Cancer Controlled After 4 Months of Gemcitabine With or Without Erlotinib. JAMA [Internet] 2016; May; 3; 315 (17) 1844 Available from: http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.2016.4324
-
Mota JM,
Silva AHC,
Franco AS,
Talans A,
Ribeiro- Ferreira F,
Castria TB de.
et al
FOLFIRINOX for advanced pancreatic adenocarcinoma in Brazil: a single- institution
experience. . Brazilian J Oncol [Internet]. 2018;14(47). Available from: http://brazilianjournalofoncology.com.br/details/38/en-US
- Skelton WP, Parekh H, Starr JS, Trevino J, Cioffi J, Hughes S. et al Clinical Factors as a Component of the Personalized Treatment Approach to Advanced Pancreatic Cancer: a Systematic Literature Review. J Gastrointest Cancer [Internet] 2018; Mar; 7; 49 (01) 1-8 Available from: http://link.springer.com/10.1007/s12029-017-0021-z
- Matsumoto I, Kamei K, Omae K, Suzuki S, Matsuoka H, Mizuno N. et al FOLFIRINOX for locally advanced pancreatic cancer: Results and prognostic factors of subset analysis from a nation-wide multicenter observational study in Japan. Pancreatology [Internet] 2019; Mar; 19 (02) 296-301 Available from: https://linkinghub.elsevier.com/retrieve/pii/S142439031930002X
- Blazer M, Wu C, Goldberg RM, Phillips G, Schmidt C, Muscarella P. et al Neoadjuvant Modified (m) FOLFIRINOX for Locally Advanced Unresectable (LAPC) and Borderline Resectable (BRPC) Adenocarcinoma of the Pancreas. Ann Surg Oncol [Internet] 2015; Apr; 22 (04) 1153-1159 Available from: http://link.springer.com/10.1245/s10434-014-4225-1
- Napolitano F, Formisano L, Giardino A, Girelli R, Servetto A, Santaniello A. et al Neoadjuvant Treatment in Locally Advanced Pancreatic Cancer (LAPC) Patients with FOLFIRINOX or Gemcitabine NabPaclitaxel: A Single-Center Experience and a Literature Review. Cancers (Basel) [Internet] 2019; Jul; 13; 11 (07) 981 Available from: https://www.mdpi.com/2072-6694/11/7/981
- Le N, Sund M, Vinci A, Beyer G, Ashan Javed M, Krug S. et al Prognostic and predictive markers in pancreatic adenocarcinoma. Dig Liver Dis [Internet] 2016; Mar; 48 (03) 223-230 Available from: https://linkinghub.elsevier.com/retrieve/pii/S1590865815006908
-
Pellei C MA.
Prognostic Factors in Pancreatic Cancer: The Role of Perineural, Vascular and Lymphatic
Invasion and of Ca19-9. . J Gastrointest Dig Syst [Internet]. 2013;03(3). Available
from: https://www.omicsonline.org/prognostic-factors-in-pancreatic-cancer-the-role-of-perineural-vascular-and-lymphatic-invasion-and-of-ca2161-069X-3-134.php?aid=17559
- Ballehaninna UK, Chamberlain RS. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J Gastrointest Oncol [Internet] 2012; Jun; 3 (02) 105-119 Available from: http://www.ncbi.nlm.nih.gov/pubmed/22811878
- Chang JC, Kundranda M. Novel Diagnostic and Predictive Biomarkers in Pancreatic Adenocarcinoma. Int J Mol Sci [Internet] 2017; Mar; 20; 18 (03) 667 Available from: http://www.mdpi.com/1422-0067/18/3/667
-
Hua Y-Q,
Wang P,
Zhu X-Y,
Shen Y-H,
Wang K,
Shi W-D.
et al
Radiofrequency ablation for hepatic oligometastatic pancreatic cancer: An analysis
of safety and efficacy. Pancreatology [Internet] 17 (06) 967-973 Available from:
http://www.ncbi.nlm.nih.gov/pubmed/29129384
Corresponding author:
Publication History
Received: 15 February 2020
Accepted: 24 July 2020
Article published online:
27 August 2020
© 2022. This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
Paloma Porto Amorim, Ana Caroline Sobral Patu, Camila Sarteschi, José Fernando do Prado Moura. Locally Advanced and Metastatic Pancreatic Cancer: Survival analysis and prognostic factors in a case series. Brazilian Journal of Oncology 2020; 16: e-20200027.
DOI: 10.5935/2526-8732.20200027
-
REFERENCES
- International Agency of Research on Cancer. Estimated number of new cases in 2018, Asia, Indonesia, both sexes, all ages. World Heal Organ 2018; 876: 2018
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res [Internet] 2014; Jun; 1; 74 (11) 2913-2921 Available from: http://cancerres.aacrjournals.org/cgi/doi/10.1158/0008-5472.CAN-14-0155
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M. et al Increased Survival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine. N Engl J Med [Internet] 2013; Oct; 31; 369 (18) 1691-1703 Available from: http://www.nejm.org/doi/10.1056/NEJMoa1304369
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y. et al FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med [Internet] 2011; May; 12; 364 (19) 1817-1825 Available from: http://www.ncbi.nlm.nih.gov/pubmed/21561347
- Unger JM, Cook E, Tai E, Bleyer A. The Role of Clinical Trial Participation in Cancer Research: Barriers, Evidence, and Strategies. Am Soc Clin Oncol Educ book Am Soc Clin Oncol Annu Meet [Internet] 2016; 35: 185-198 Available from: http://www.ncbi.nlm.nih.gov/pubmed/27249699
- Kadokura M, Ishida Y, Tatsumi A, Takahashi E, Shindo H, Amemiya F. et al Performance status and neutrophil-lymphocyte ratio are important prognostic factors in elderly patients with unresectable pancreatic cancer. J Gastrointest Oncol [Internet] 2016; Dec; 6 (07) 982-988 Available from: http://jgo.amegroups.com/article/view/8283/9417
- Tabernero J, Chiorean EG, Infante JR, Hingorani SR, Ganju V, Weekes C. et al Prognostic Factors of Survival in a Randomized Phase III Trial (MPACT) of Weekly nab-Paclitaxel Plus Gemcitabine Versus Gemcitabine Alone in Patients With Metastatic Pancreatic Cancer. Oncologist [Internet] 2015; Feb; 1; 20 (02) 143-150 Available from: http://theoncologist.alphamedpress.org/cgi/doi/10.1634/theoncologist.2014-0394
- Zhou Y, Wei Q, Fan J, Cheng S, Ding W, Hua Z. Prognostic role of the neutrophil-to-lymphocyte ratio in pancreatic cancer: A meta-analysis containing 8252 patients. Clin Chim Acta [Internet] 2018; Apr; 479: 181-189 Available from: https://linkinghub.elsevier.com/retrieve/pii/S0009898118300329
- Mei Z, Shi L, Wang B, Yang J, Xiao Z, Du P. et al Prognostic role of pretreatment blood neutrophil-to-lymphocyte ratio in advanced cancer survivors: A systematic review and meta-analysis of 66 cohort studies. Cancer Treat Rev [Internet] 2017; Jul; 58: 1-13 Available from: https://linkinghub.elsevier.com/retrieve/pii/S0305737217300853
- Zhou Y, Cheng S, Fathy AH, Qian H, Zhao Y. Prognostic value of platelet-to- lymphocyte ratio in pancreatic cancer: a comprehensive meta-analysis of 17 cohort studies. Onco Targets Ther [Internet] 2018; 11: 1899-1908 Available from: http://www.ncbi.nlm.nih.gov/pubmed/29670365
- Moningi S, Dholakia AS, Raman SP, Blackford A, Cameron JL, Le DT. et al The Role of Stereotactic Body Radiation Therapy for Pancreatic Cancer: A Single-Institution Experience. Ann Surg Oncol [Internet] 2015; Jul; 22 (07) 2352-2358 Available from: http://www.ncbi.nlm.nih.gov/pubmed/25564157
- Chuong MD, Springett GM, Freilich JM, Park CK, Weber JM, Mellon EA. et al Stereotactic body radiation therapy for locally advanced and borderline resectable pancreatic cancer is effective and well tolerated. Int J Radiat Oncol Biol Phys [Internet] 2013; Jul; 1; 86 (03) 516-522 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23562768
- Gurka MK, Collins SP, Slack R, Tse G, Charabaty A, Ley L. et al Stereotactic body radiation therapy with concurrent full-dose gemcitabine for locally advanced pancreatic cancer: a pilot trial demonstrating safety. Radiat Oncol [Internet] 2013; Mar; 1; 8: 44 Available from: http://www.ncbi.nlm.nih.gov/pubmed/23452509
- Hammel P, Huguet F, van Laethem J-L, Goldstein D, Glimelius B, Artru P. et al Effect of Chemoradiotherapy vs Chemotherapy on Survival in Patients With Locally Advanced Pancreatic Cancer Controlled After 4 Months of Gemcitabine With or Without Erlotinib. JAMA [Internet] 2016; May; 3; 315 (17) 1844 Available from: http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.2016.4324
-
Mota JM,
Silva AHC,
Franco AS,
Talans A,
Ribeiro- Ferreira F,
Castria TB de.
et al
FOLFIRINOX for advanced pancreatic adenocarcinoma in Brazil: a single- institution
experience. . Brazilian J Oncol [Internet]. 2018;14(47). Available from: http://brazilianjournalofoncology.com.br/details/38/en-US
- Skelton WP, Parekh H, Starr JS, Trevino J, Cioffi J, Hughes S. et al Clinical Factors as a Component of the Personalized Treatment Approach to Advanced Pancreatic Cancer: a Systematic Literature Review. J Gastrointest Cancer [Internet] 2018; Mar; 7; 49 (01) 1-8 Available from: http://link.springer.com/10.1007/s12029-017-0021-z
- Matsumoto I, Kamei K, Omae K, Suzuki S, Matsuoka H, Mizuno N. et al FOLFIRINOX for locally advanced pancreatic cancer: Results and prognostic factors of subset analysis from a nation-wide multicenter observational study in Japan. Pancreatology [Internet] 2019; Mar; 19 (02) 296-301 Available from: https://linkinghub.elsevier.com/retrieve/pii/S142439031930002X
- Blazer M, Wu C, Goldberg RM, Phillips G, Schmidt C, Muscarella P. et al Neoadjuvant Modified (m) FOLFIRINOX for Locally Advanced Unresectable (LAPC) and Borderline Resectable (BRPC) Adenocarcinoma of the Pancreas. Ann Surg Oncol [Internet] 2015; Apr; 22 (04) 1153-1159 Available from: http://link.springer.com/10.1245/s10434-014-4225-1
- Napolitano F, Formisano L, Giardino A, Girelli R, Servetto A, Santaniello A. et al Neoadjuvant Treatment in Locally Advanced Pancreatic Cancer (LAPC) Patients with FOLFIRINOX or Gemcitabine NabPaclitaxel: A Single-Center Experience and a Literature Review. Cancers (Basel) [Internet] 2019; Jul; 13; 11 (07) 981 Available from: https://www.mdpi.com/2072-6694/11/7/981
- Le N, Sund M, Vinci A, Beyer G, Ashan Javed M, Krug S. et al Prognostic and predictive markers in pancreatic adenocarcinoma. Dig Liver Dis [Internet] 2016; Mar; 48 (03) 223-230 Available from: https://linkinghub.elsevier.com/retrieve/pii/S1590865815006908
-
Pellei C MA.
Prognostic Factors in Pancreatic Cancer: The Role of Perineural, Vascular and Lymphatic
Invasion and of Ca19-9. . J Gastrointest Dig Syst [Internet]. 2013;03(3). Available
from: https://www.omicsonline.org/prognostic-factors-in-pancreatic-cancer-the-role-of-perineural-vascular-and-lymphatic-invasion-and-of-ca2161-069X-3-134.php?aid=17559
- Ballehaninna UK, Chamberlain RS. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J Gastrointest Oncol [Internet] 2012; Jun; 3 (02) 105-119 Available from: http://www.ncbi.nlm.nih.gov/pubmed/22811878
- Chang JC, Kundranda M. Novel Diagnostic and Predictive Biomarkers in Pancreatic Adenocarcinoma. Int J Mol Sci [Internet] 2017; Mar; 20; 18 (03) 667 Available from: http://www.mdpi.com/1422-0067/18/3/667
-
Hua Y-Q,
Wang P,
Zhu X-Y,
Shen Y-H,
Wang K,
Shi W-D.
et al
Radiofrequency ablation for hepatic oligometastatic pancreatic cancer: An analysis
of safety and efficacy. Pancreatology [Internet] 17 (06) 967-973 Available from:
http://www.ncbi.nlm.nih.gov/pubmed/29129384