

Subscribe to RSS
DOI: 10.1055/a-2253-9588
3D ultrasound evaluation of fetal ears in prenatal syndrome diagnosis – a comparative study
3D-Ultraschall-Beurteilung fetaler Ohren in der pränatalen Syndromdiagnostik – eine VergleichsstudieAuthors


Abstract
Purpose The aim of the study was to assess fetal ears on prenatal 3D ultrasound and compare ear surface patterns and measurements between fetuses with syndromes and healthy fetuses.
Materials and Methods Our study is based on 3D ultrasound images of 100 fetuses between the 20th and 37th week of gestation. We compared 50 ears of fetuses with syndromes (syndrome group) to 50 gestational age-matched ears of healthy fetuses (control group). The syndrome group consisted of fetuses with Trisomy 21 (n=13), Trisomy 18 (n=9) and other syndromes (n=28). The evaluation was based on measuring the ear length and width as well as developing categories to describe and compare different ear surface anomalies.
Results Ears of fetuses with Trisomy 18 were on average 0.423 cm smaller in length (P<0.001) and 0.123 cm smaller in width (P=0.031) and grew on average 0.046 cm less in length per week of gestation (P=0.027) than those of healthy fetuses. Ears of fetuses with Trisomy 21 differed from healthy fetuses regarding the form of the helix (P=0.013) and the ratio of the concha to the auricle (P=0.037). Fetuses with syndromes demonstrated less ear surface details than their controls (syndrome group: P=0.018, P=0.005; other syndromes subgroup: P=0.020). We saw an increased richness of ear surface details at a later gestational age both in the fetuses with syndromes and the healthy fetuses.
Conclusion Ears of fetuses with Trisomy 18 were smaller than their matched controls. Fetuses with syndromes varied in the evaluation of their ear surface from those of healthy fetuses. The ear surface can be analyzed with 3D ultrasound and might be useful as a screening parameter in syndrome diagnosis in the future.
Zusammenfassung
Ziel Ziel unserer Studie war es, Oberflächenmuster und Messwerte der Ohren syndromaler und gesunder Feten mithilfe des pränatalen 3D-Ultraschalls zu bestimmen und zu vergleichen.
Material und Methode Unsere Studie basiert auf 3D-Ultraschallbildern von 100 Feten zwischen der 20. und 37. Schwangerschaftswoche. Wir verglichen 50 Ohren syndromaler Feten (Syndromgruppe) mit 50 Ohren gleichaltriger gesunder Feten (Kontrollgruppe). Die Syndromgruppe bestand aus Feten mit Trisomie 21 (n=13), Trisomie 18 (n=9) und sonstigen Syndromen (n=28). Die Auswertung basierte auf der Messung der Ohrenlänge und -breite sowie der Entwicklung von Kategorien verschiedener Oberflächenanomalien.
Ergebnisse Ohren von Feten mit Trisomie 18 waren durchschnittlich 0,423cm kürzer (P<0,001), 0,123cm schmaler (P=0,031) und wuchsen 0,046cm pro Schwangerschaftswoche weniger in der Länge (P=0,027) als die in der Kontrollgruppe. Ohren von Feten mit Trisomie 21 wichen gegenüber gesunden Feten in der Beurteilung der Helixform (P=0,013) und dem Verhältnis der Concha zur Ohrmuschel (P=0,037) ab. Das Detailreichtum der Ohrenoberfläche syndromaler Feten war gegenüber denen der Kontrollfeten erniedrigt (Syndromgruppe: P=0,018, P=0,005; sonstige Syndrome: P=0,020). Sowohl syndromale als auch gesunde Feten wiesen eine Zunahme des Detailreichtums der Ohrenoberfläche mit steigendem Gestationsalter auf.
Schlussfolgerungen Ohren von Feten mit Trisomie 18 waren kleiner als die der Kontrollgruppe. Ohren von syndromalen Feten unterschieden sich in der Bewertung ihrer Oberfläche von gesunden Feten. Die Ohrenoberfläche kann im 3D-Ultraschall analysiert werden und könnte als Screening-Parameter in der Syndromdiagnostik hilfreich sein.
Introduction
Prenatal ultrasound is an important screening tool for congenital anomalies, which occur in 2.40% of all births in Europe [1]. The prevalences are 0.21% for Down syndrome (Trisomy 21) and 0.05% for Edwards syndrome (Trisomy 18) [1]. Early prenatal diagnosis allows adequate parental counseling and a timely decision about whether to continue the pregnancy [2] and is important for planning the birth and potential postnatal treatment [2] [3]. Aside from ultrasound, the importance of noninvasive prenatal testing (NIPT) as a screening method for syndromes has increased in the past years [4]. However, it is limited [4] [5]. Besides prenatal ultrasound and NIPT, invasive testing is unsuitable for screening due to the associated risks and intensive costs [6]. It still is the most exhaustive option for karyotype assessment and can be indicated after risk calculation through prenatal ultrasound [5] [7]. Previous studies have shown that syndromal diseases are often associated with outer ear malformations and suspect that prenatal ear screening may be helpful in predicting the risk for syndromes [2] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16].
Hereditary ear malformations can occur on a solitary basis or as part of an underlying syndrome associated with other malformations [17]. The incidence of outer ear deformities in newborns varies greatly, depending on the population and definition criteria and ranges from 0.02% [18] to 57.46% [19]. The primitive outer ear develops at the beginning of 10 weeks of gestation (WG) and continues to grow and differentiate during gestation [20] to then present with a complex anatomic structure [8] ([Fig. 1]). Anomalies of the fetal face and ears may be sonographically detectable by the late first trimester [9] [20], though some authors postulate that the best time for ear examination is during second trimester screening [10]. In our study 3D ultrasound of fetal ears was performed between 20 and 37 WG.

Besides measuring the ears, our main intention was to find cumulative ear surface anomalies. We put them in categories in order to make them tangible, measurable, and comparable. We hypothesized that there are ear anomalies which correlate with fetal syndromes. As far as we know, this is the first study to develop different categories to describe the outer ear pattern using 3D ultrasound.
Materials and Methods
Study population
This retrospective explorative study included data from 100 fetuses and was conducted at our perinatal outpatient department between 2013 and 2022. We analyzed the 3D raw data volumes of one ear per fetus. The study comprised fetuses with syndromes (syndrome group) and healthy fetuses without syndromes (control group) between 20 and 37 WG. The gestational age was defined in the first trimester using the crown-rump length.
The syndrome group was categorized in three subgroups based on the genetic test result: subgroup 1 (Trisomy 21), subgroup 2 (Trisomy 18), and subgroup 3 (other syndromes including Trisomy 9, Trisomy 13, Noonan syndrome, Fragile X syndrome, Peters plus syndrome, Escobar syndrome and other syndrome complexes with unknown or unremarkable genetics). The inclusion criterion for the syndrome group was the visibility of the outlines of the outer ear in 3D ultrasound. We matched the fetuses of the syndrome group with controls of the same gestational age with a maximum difference of three days. The fetuses of the control group were selected according to image quality.
There were no maternal exclusion criteria besides an age under 18 years. The data were collected during routine examinations with informed consent. The study was approved by the institutional ethics board (2022–865-f-S) and carried out in accordance with the Declaration of Helsinki.
Data acquisition and analysis
The examination was performed by prenatal ultrasound specialists with an iU22 and EPIQ7 ultrasound system equipped with a 6MHz X6–1 xMatrix transducer (Philips Medical Systems, Bothell, Washington, USA). The fetal ear with better visibility was examined by 3D ultrasound at the end of the routine ultrasound examination. Every 3D raw data volume was adjusted in axial alignment and all three orthogonal planes simultaneously using QLAB 13 (Philips Medical Systems, Bothell, Washington, USA) to then be saved as a single 3D image ([Fig. 2]). In these images the ear could be sized using ZEN core 3.2 (Zeiss Microscopy, Jena, Germany).

Referring to Sondern et al. [11], the ear length was measured in its longest dimension from the most caudal point of the ear lobe to the most apical point of the upper helix, while the ear width was measured from the most posterior edge of the tragus to the outline of the helix orthogonal to the ear length. All measurements were taken from the outer tissue boundary. By dividing the ear length by the ear width, we calculated the ear length to ear width ratio (length/width ratio).
In a second step we analyzed the pattern of the outer ear by defining seven pattern categories: helix contour, lobe contour, concha to auricle ratio, upper ear to lobe ratio, ear in ear, surface details, and dimples. For each pattern category, visually discernible subcategories were defined. The subcategory occurring most frequently in the control group was considered normal and will be mentioned first in the following. Ears with insufficient image quality were excluded in each pattern category.
Helix contour as a description of the helix outline was defined as oval, round, spiky, or flipped/cropped upper ears. Lobe contour could be considered unremarkable, slimmed, thickened or atrophied/attached. The calculation of the concha to auricle ratio is pictured in [Fig. 3]a and was scored as unremarkable, enlarged ([Fig. 3]a left side), narrowed ([Fig. 3]a right side), or jug ears. [Fig. 3]b demonstrates the upper ear to lobe ratio, which was larger than/equal in size ([Fig. 3]b left side) or smaller ([Fig. 3]b right side). The ear in ear pattern was divided into not present or present whenever the form of the concha resembled the outline of the whole ear ([Fig. 3]c). The category surface details considered the level of surface definition from detailed to poor in detail, thickened, and rudimentary. In the seventh pattern category we rated the ears based on the presence of no, one, or various dimples.

The anomaly score counted the number of categories evaluated as not normal and was only applied if the ear was evaluated in all seven categories. A maximum score of 7 out of the 7 pattern categories would be the most anomalous.
Clinical data, such as WG at ultrasound and, if applicable, the WG at birth, birth weight, birth weight percentile, pH level of the umbilical artery, APGAR score at 5 min, sex of the fetus, and livebirth were extracted from the electronic patient file in Orbis (Orbis SE, Saarbrücken, Germany) and ViewPoint 6 (GE HealthCare, General Electric Company, Boston, Massachusetts, USA). Similarly, the biparietal diameter (BPD) and BPD percentile were extracted from ViewPoint 6. If these were not measured, we calculated them percentile-appropriate to the WG from the nearest documented value. By dividing the ear length by the BPD, we calculated the ear length to BPD ratio (length/BPD ratio).
Statistics
Statistical analyses were conducted using IBM SPSS Statistics version 28 (IBM Corporation, Armonk, New York, USA) and R version 4.3 (R Foundation for Statistical Computing, Vienna, Austria). All P-values were two-sided and considered to be statistically noticeable when ≤0.05. As no adjustment for multiple testing was applied, all P-values need to be interpreted as exploratory.
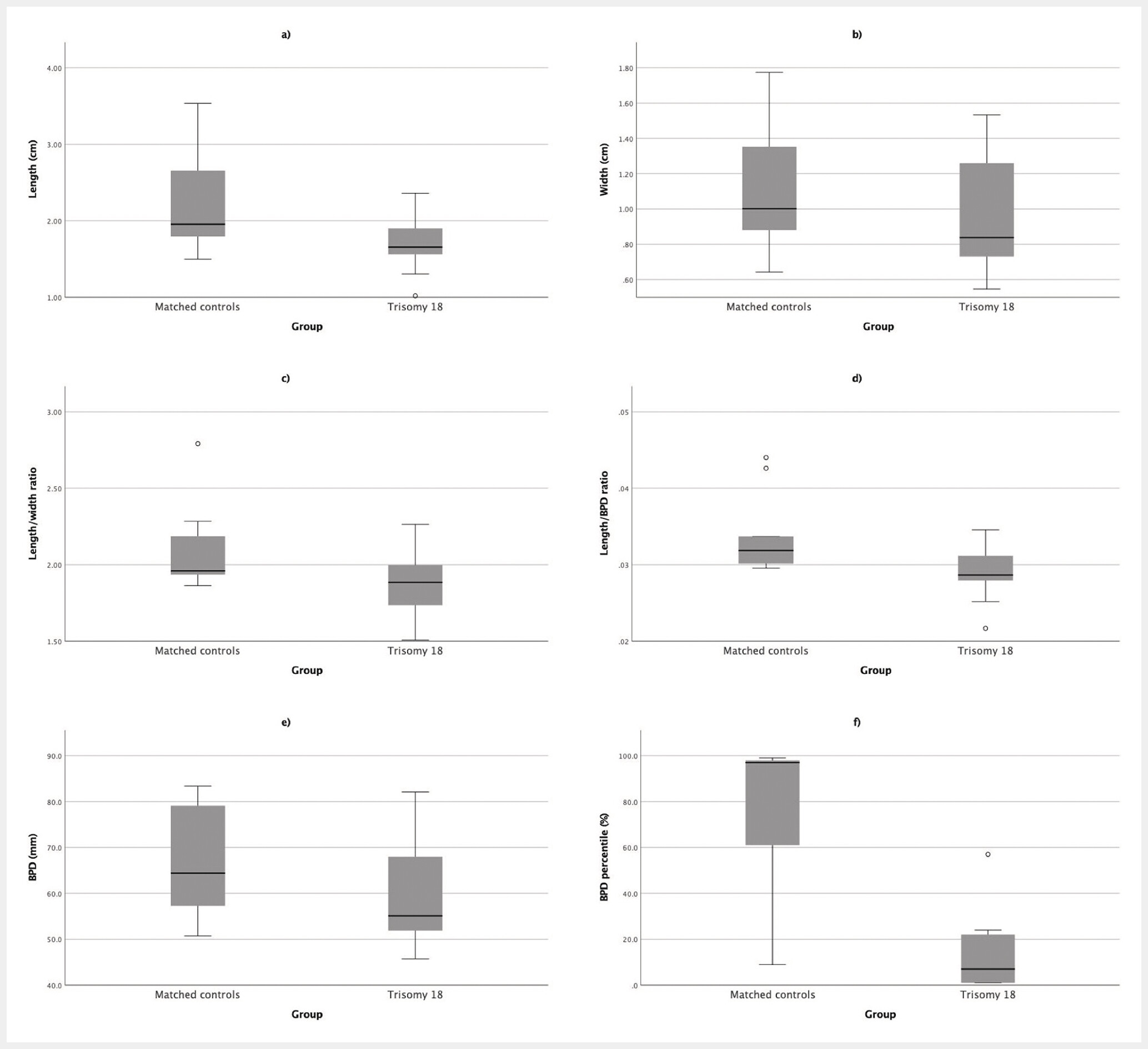
Metrical clinical data, sonographic measurements, and the anomaly score were presented as median and interquartile range (IQR, presented as lower and upper quartile) using descriptive statistics. For comparison of the syndrome group or subgroup and control group, the Mann-Whitney U test was applied as well as the Wilcoxon signed-ranked test for respective matched pairs. Boxplots were used to accentuate the discrepancy of sonographic measurements between the Trisomy 18 subgroup and its matched controls.
We utilized linear regression without interaction to depict the difference of average ear length, ear width, length/width, and length/BPD ratio of the syndrome group as well as for the three subgroups in a WG-dependent comparison with the control group. Regression coefficients, 95% Wald confidence intervals (CI), and corresponding P-values were calculated.
Grouped scatterplots illustrated the WG-dependent progression of ear measurements for the syndrome group and control group, as well as for the Trisomy 18 subgroup and its matched controls. For these two groups we additionally calculated regression coefficients, CI and P-values using linear regression with interaction to compare the growth of their ear measurements to the respective controls.
For non-metrical clinical data and the pattern categories, absolute and relative frequencies were reported. The Fisher’s exact test was performed as well as the Cochran-Mantel-Haenszel test for respective matched pairs. A visualization of the distribution of surface detail variation between the syndrome group and control group during pregnancy was portrayed in bar charts.
Results
100 fetuses were included in the study, with 50 in the control group and 50 in the syndrome group (subgroup 1: n=13, subgroup 2: n=9, subgroup 3: n=28). All sonographic measurements and metric demographic characteristics of the whole syndrome group and control group are shown in [Table 1]. Sonographic ear measurements were achievable in all cases.
All ear and BPD-related measurements were noticeably smaller in the Trisomy 18 subgroup than in the respective control group, as visualized in [Fig. 4]. An ear of a fetus with Trisomy 18 was on average 0.423 cm shorter in length (CI –0.619, –0.226, P<0.001) and 0.123 cm less wide (CI –0.236, –0.011, P=0.031) than an ear in the control group ([Table 2]).
Concerning ear growth in length, there was a noticeable difference in both the syndrome group and the Trisomy 18 subgroup compared to their controls ([Fig. 5], [Fig. 6]). While ear growth in length per WG was on average 0.085 cm in the control group, an ear of the syndrome group grew on average 0.026 cm more (CI 0.003, 0.048, P=0.028). Ears of fetuses with Trisomy 18 grew on average 0.046 cm less in length per WG (CI –0.087, –0.005, P=0.027) than their references in the control group with an average of 0.131 cm.


All categorial data including the seven pattern categories are listed in [Table 3]. A pattern category could successfully be assessed in 82.8% of the syndrome group (41.4/50) and in 89.4% of the control group (44.7/50).
Ears of fetuses with Trisomy 21 (n=11) varied noticeably from their control group (n=13) in the category helix contour (P=0.013). The oval helix contour categorized as normal was found less often in Trisomy 21 (18.2%) than in healthy fetuses (69.2%), while round ears were more often seen in Trisomy 21 (72.7% vs. 15.4%, respectively). An oval ear of a healthy fetus is pictured in [Fig. 2]h as well as a round ear of a fetus with Trisomy 21 in [Fig. 2]e.
Trisomy 21 ears (n=9) differed statistically noticeably from their respective control group (n=11) with respect to the concha to auricle ratio (P=0.037). 33.3% were classified as unremarkable (control group: 81.8%), 22.2% were classified with an enlarged concha (control group: 0.0%), 44.4% with a narrowed concha (control group: 9.1%) and 0.0% with jug ears (control group: 9.1%).
Evaluation of surface details revealed that the ears in the syndrome group were detailed noticeably less often than their controls (P=0.018, P=0.005). The same applies for the ears in the subgroup of other syndromes (P=0.020). Both fetuses with syndromes and healthy fetuses showed an increase in ear detail richness during gestation ([Fig. 7]). The ears in the control group ([Fig. 7]a) were considered 40.0% detailed initially, progressing to 100.0% at a later WG, whereas in the case of the ears in the syndrome group ([Fig. 7]b) details increased from 11.1% to 45.5% with age. [Fig. 8] demonstrates ears of healthy fetuses, one at 21 WG ([Fig. 8]a) and one at 30 WG ([Fig. 8]b), illustrating that the older ear is more detailed and less thickened.
The presence of dimples did not differ statistically noticeably (P=0.082) between the syndrome group (n=40) and the control group (n=43), but the ears of healthy fetuses appeared more likely to have various dimples (23.3%), as shown in an example in [Fig. 2]d, than those of the fetuses with syndromes (7.5%).


33 fetuses of the syndrome group and 32 fetuses of the control group could be included in the anomaly score. There was no statistically noticeable difference between the syndrome group and the control group (P=0.192, P=0.674), but there was a tendency for a higher anomaly score in the Trisomy 21 subgroup (4.0 (IQR 3.0, 4.5), n=9) than in its control group (2.5 (IQR 2.0, 3.8), n=8; P=0.060, P=0.313).
Any further results regarding the subgroup analysis and the evaluation in all pattern categories as well as the anomaly score are presented in the supplemental material comprising Table S1–S7.
Discussion
Based on 3D ultrasound images, we successfully measured fetal ears, examined their outer appearance, and compared the results between fetuses with syndromes and healthy fetuses.
Our study was able to show that the ears of fetuses with Trisomy 18 were noticeably smaller and increased less in length with gestational age than their controls. The evaluation of the outer ear showed noticeable differences between ears of fetuses with syndromes and healthy fetuses. The ears of fetuses with syndromes tended to be rounder, more often thickened, and less detailed. The level of surface detail increased noticeably with increasing WG in both the syndrome and control group. Therefore, a lack of detail in early WG should not be mistaken for an ear anomaly. The presence of dimples could also be discussed in the context of surface details as they may be more likely to occur with detailed than thickened ears.
To our knowledge, there are currently no other studies using 3D sonography to examine the ear surface patterns in the context of prenatal syndrome screening.
There are several studies that previously measured ear length with 2D ultrasound [6] [7] [11] [12] [13] [14] [15] [21] and 3D ultrasound [11] [16] [21]. Many of them ascertained a strong positive correlation between ear length and WG [6] [7] [12] [13] [21], which is in line with our results. A reduced ear length in fetuses with chromosomal anomalies and aneuploidy has previously been demonstrated and this measurement is therefore recommended as part of prenatal ultrasound screening by several authors [6] [7] [12] [13] [14] [15]. The ear length seems to be the most promising ear measurement parameter, while the ear width is not suggested for prenatal screening [14]. In order to estimate regular ear growth and compare ear measurements with standard biometric values, such as the BPD, stipulation of ear length percentiles could be helpful.
Prenatal ultrasound and especially 3D ultrasound have improved vastly over the last years [22]. Various studies have highlighted the benefits of 3D ultrasound for analyzing the fetal face and ears due to better visualization of complex surfaces, high detail accuracy, as well as the capability to show different planes simultaneously and evaluate orthogonality [2] [8] [9] [11] [16] [22] [23]. The fetal face portrayed in 3D images looks very similar to the postnatal appearance [3] and may be easier for parents to visualize [23] and also facilitates demonstration by clinicians to both parents and colleagues [3] [9] [11] [22] [23]. Besides 3D ultrasound, in the recent past, the usage of artificial intelligence for detecting syndrome-specific fetal anomalies has become more popular [24] [25], and fetal facial abnormalities could thus be linked to Trisomy 21, 18, 13 and rare genetic diseases [25].
With all the advantages of 3D ultrasound, simple measurements such as the ear length are comparable in 2D ultrasound [11] [21]. 3D ultrasound is more time-consuming [9] and should be seen as an addition not an alternative to 2D ultrasound [9] [22]. The limitations of 3D ultrasound, such as the fetal position, reduced amniotic fluid, maternal obesity, and movement artifacts, are similar to 2D ultrasound [10]. However, rotation of the 3D ultrasound probe can show planes that would not be detectable with 2D ultrasound [9] [22] [23].
In general, the ears of both fetuses with syndromes and healthy fetuses have a very individual and variable appearance. With our category system, we tried to classify ear anomalies more objectively, but ear pattern evaluations by clinicians as well as ultrasound measurements are rather subjective. It should be mentioned that ear anomalies can be singular and not symmetrically represented on both ears [23]. Due to limited visualization on ultrasound, we only analyzed one ear per fetus. The sample size was sometimes smaller in the syndrome group, as pattern identification was not always possible due to image quality, while the control group was selected for ideal image quality. A general limitation of our study was the relatively small number of cases for the statistical evaluation of a heterogeneous syndrome group. Further studies with bigger syndrome populations will be needed.
In conclusion, we were able to show that besides ear measurements the ear surface pattern can be analyzed with 3D ultrasound and varies between fetuses with syndromes and healthy fetuses. We suspect that ear measurements and ear surface patterns might be useful as screening parameters in prenatal syndrome diagnosis, whereby our pattern categories could potentially be incorporated into artificial learning methods.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Dolk H, Loane M, Garne E. The prevalence of congenital anomalies in Europe. Adv Exp Med Biol 2010; 686: 349-364
- 2 Biard J-M, Payrat S, Clapuyt P. et al. Antenatal diagnosis of CHARGE syndrome: Prenatal ultrasound findings and crucial role of fetal dysmorphic signs. About a series of 10 cases and review of literature. Eur J Med Genet 2021; 64: 104189
- 3 Werner H, Castro P, Daltro P. et al. Prenatal diagnosis of Apert syndrome using ultrasound, magnetic resonance imaging, and three-dimensional virtual/physical models: three case series and literature review. Childs Nerv Syst 2018; 34: 1563-1571
- 4 Gregg AR, Skotko BG, Benkendorf JL. et al. Noninvasive prenatal screening for fetal aneuploidy, 2016 update: a position statement of the American College of Medical Genetics and Genomics. Genet Med 2016; 18: 1056-1065
- 5 Yuan X, Yong W, Dai L. et al. The role of non-invasive prenatal testing and ultrasound in prenatal screening of fetal chromosomal abnormalities in singleton: a retrospective study. Ann Transl Med 2023; 11: 111
- 6 Awwad JT, Azar GB, Karam KS. et al. Ear length: a potential sonographic marker for Down syndrome. Int J Gynaecol Obstet 1994; 44: 233-238
- 7 Lettieri L, Rodis JF, Vintzileos AM. et al. Ear length in second-trimester aneuploid fetuses. Obstet Gynecol 1993; 81: 57-60
- 8 Bürkel K, Krämer U, Möllers M. et al. 3D Ultrasound Evaluation of the Fetal Ear – Comparison of an xMatrix Probe with a Conventional Mechanical Probe. Ultraschall in Med 2017; 38: 508-514
- 9 Kurjak A, Azumendi G, Andonotopo W. et al. Three- and four-dimensional ultrasonography for the structural and functional evaluation of the fetal face. Am J Obstet Gynecol 2007; 196: 16-28
- 10 Wei J, Ran S, Yang Z. et al. Prenatal ultrasound screening for external ear abnormality in the fetuses. Biomed Res Int 2014; 2014: 357564
- 11 Sondern K, Kreitz K, Hammer K. et al. 3D Ultrasound Evaluation of the Fetal Outer Ear: Novel Biometry Ratio and Comparison of Different Surface Display Modes. Fetal Diagn Ther 2019; 46: 200-206
- 12 Yeo L, Guzman ER, Ananth CV. et al. Prenatal detection of fetal aneuploidy by sonographic ear length. J Ultrasound Med 2003; 22: 565-576
- 13 Birnholz JC, Farrell EE. Fetal ear length. Pediatrics 1988; 81: 555-558
- 14 Shimizu T, Salvador L, Hughes-Benzie R. et al. The role of reduced ear size in the prenatal detection of chromosomal abnormalities. Prenat Diagn 1997; 17: 545-549
- 15 Chitkara U, Lee L, Oehlert JW. et al. Fetal ear length measurement: a useful predictor of aneuploidy?. Ultrasound Obstet Gynecol 2002; 19: 131-135
- 16 Chang CH, Chang FM, Yu CH. et al. Fetal ear assessment and prenatal detection of aneuploidy by the quantitative three-dimensional ultrasonography. Ultrasound Med Biol 2000; 26: 743-749
- 17 Bartel-Friedrich S, Wulke C. Classification and diagnosis of ear malformations. GMS Curr Top Otorhinolaryngol Head Neck Surg 2007; 6: Doc05
- 18 Conway H, Wagner KJ. Congenital anomalies of the head and neck as reported on birth certificates in New York City, 1952 to 1962 (inclusive). Plast Reconstr Surg 1965; 36: 71-79
- 19 Zhao H, Ma L, Qi X. et al. A Morphometric Study of the Newborn Ear and an Analysis of Factors Related to Congenital Auricular Deformities. Plast Reconstr Surg 2017; 140: 147-155
- 20 Hill MA. Early human development. Clin Obstet Gynecol 2007; 50: 2-9
- 21 Hatanaka AR, Rolo LC, Mattar R. et al. Reference intervals for fetal ear length between 19 and 24 weeks of pregnancy on 3-dimensional sonography. J Ultrasound Med 2011; 30: 1185-1190
- 22 Merz E, Welter C. 2D and 3D Ultrasound in the evaluation of normal and abnormal fetal anatomy in the second and third trimesters in a level III center. Ultraschall in Med 2005; 26: 9-16
- 23 Shih JC, Shyu MK, Lee CN. et al. Antenatal depiction of the fetal ear with three-dimensional ultrasonography. Obstet Gynecol 1998; 91: 500-505
- 24 Stirnemann JJ, Besson R, Spaggiari E. et al. Development and clinical validation of real-time artificial intelligence diagnostic companion for fetal ultrasound examination. Ultrasound Obstet Gynecol 2023;
- 25 Tang J, Han J, Xue J. et al. A Deep-Learning-Based Method Can Detect Both Common and Rare Genetic Disorders in Fetal Ultrasound. Biomedicines 2023; 11: 1756
Correspondence
Publication History
Received: 21 November 2023
Accepted after revision: 25 January 2024
Accepted Manuscript online:
25 January 2024
Article published online:
04 March 2024
© 2024. Thieme. All rights reserved.
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Dolk H, Loane M, Garne E. The prevalence of congenital anomalies in Europe. Adv Exp Med Biol 2010; 686: 349-364
- 2 Biard J-M, Payrat S, Clapuyt P. et al. Antenatal diagnosis of CHARGE syndrome: Prenatal ultrasound findings and crucial role of fetal dysmorphic signs. About a series of 10 cases and review of literature. Eur J Med Genet 2021; 64: 104189
- 3 Werner H, Castro P, Daltro P. et al. Prenatal diagnosis of Apert syndrome using ultrasound, magnetic resonance imaging, and three-dimensional virtual/physical models: three case series and literature review. Childs Nerv Syst 2018; 34: 1563-1571
- 4 Gregg AR, Skotko BG, Benkendorf JL. et al. Noninvasive prenatal screening for fetal aneuploidy, 2016 update: a position statement of the American College of Medical Genetics and Genomics. Genet Med 2016; 18: 1056-1065
- 5 Yuan X, Yong W, Dai L. et al. The role of non-invasive prenatal testing and ultrasound in prenatal screening of fetal chromosomal abnormalities in singleton: a retrospective study. Ann Transl Med 2023; 11: 111
- 6 Awwad JT, Azar GB, Karam KS. et al. Ear length: a potential sonographic marker for Down syndrome. Int J Gynaecol Obstet 1994; 44: 233-238
- 7 Lettieri L, Rodis JF, Vintzileos AM. et al. Ear length in second-trimester aneuploid fetuses. Obstet Gynecol 1993; 81: 57-60
- 8 Bürkel K, Krämer U, Möllers M. et al. 3D Ultrasound Evaluation of the Fetal Ear – Comparison of an xMatrix Probe with a Conventional Mechanical Probe. Ultraschall in Med 2017; 38: 508-514
- 9 Kurjak A, Azumendi G, Andonotopo W. et al. Three- and four-dimensional ultrasonography for the structural and functional evaluation of the fetal face. Am J Obstet Gynecol 2007; 196: 16-28
- 10 Wei J, Ran S, Yang Z. et al. Prenatal ultrasound screening for external ear abnormality in the fetuses. Biomed Res Int 2014; 2014: 357564
- 11 Sondern K, Kreitz K, Hammer K. et al. 3D Ultrasound Evaluation of the Fetal Outer Ear: Novel Biometry Ratio and Comparison of Different Surface Display Modes. Fetal Diagn Ther 2019; 46: 200-206
- 12 Yeo L, Guzman ER, Ananth CV. et al. Prenatal detection of fetal aneuploidy by sonographic ear length. J Ultrasound Med 2003; 22: 565-576
- 13 Birnholz JC, Farrell EE. Fetal ear length. Pediatrics 1988; 81: 555-558
- 14 Shimizu T, Salvador L, Hughes-Benzie R. et al. The role of reduced ear size in the prenatal detection of chromosomal abnormalities. Prenat Diagn 1997; 17: 545-549
- 15 Chitkara U, Lee L, Oehlert JW. et al. Fetal ear length measurement: a useful predictor of aneuploidy?. Ultrasound Obstet Gynecol 2002; 19: 131-135
- 16 Chang CH, Chang FM, Yu CH. et al. Fetal ear assessment and prenatal detection of aneuploidy by the quantitative three-dimensional ultrasonography. Ultrasound Med Biol 2000; 26: 743-749
- 17 Bartel-Friedrich S, Wulke C. Classification and diagnosis of ear malformations. GMS Curr Top Otorhinolaryngol Head Neck Surg 2007; 6: Doc05
- 18 Conway H, Wagner KJ. Congenital anomalies of the head and neck as reported on birth certificates in New York City, 1952 to 1962 (inclusive). Plast Reconstr Surg 1965; 36: 71-79
- 19 Zhao H, Ma L, Qi X. et al. A Morphometric Study of the Newborn Ear and an Analysis of Factors Related to Congenital Auricular Deformities. Plast Reconstr Surg 2017; 140: 147-155
- 20 Hill MA. Early human development. Clin Obstet Gynecol 2007; 50: 2-9
- 21 Hatanaka AR, Rolo LC, Mattar R. et al. Reference intervals for fetal ear length between 19 and 24 weeks of pregnancy on 3-dimensional sonography. J Ultrasound Med 2011; 30: 1185-1190
- 22 Merz E, Welter C. 2D and 3D Ultrasound in the evaluation of normal and abnormal fetal anatomy in the second and third trimesters in a level III center. Ultraschall in Med 2005; 26: 9-16
- 23 Shih JC, Shyu MK, Lee CN. et al. Antenatal depiction of the fetal ear with three-dimensional ultrasonography. Obstet Gynecol 1998; 91: 500-505
- 24 Stirnemann JJ, Besson R, Spaggiari E. et al. Development and clinical validation of real-time artificial intelligence diagnostic companion for fetal ultrasound examination. Ultrasound Obstet Gynecol 2023;
- 25 Tang J, Han J, Xue J. et al. A Deep-Learning-Based Method Can Detect Both Common and Rare Genetic Disorders in Fetal Ultrasound. Biomedicines 2023; 11: 1756