

Subscribe to RSS
DOI: 10.1055/a-2453-2494
Complete extraction of main pancreatic duct residual and microstones using an 8-wire basket catheter
Authors

Abstract
Background and study aims Extracorporeal shock wave lithotripsy (ESWL), pancreatoscopy-guided electrohydraulic lithotripsy (EHL), and endoscopic retrograde cholangiopancreatography (ERCP) are primary treatments for symptomatic main pancreatic duct (MPD) stones. However, incomplete clearance of residual/microstones post-treatment may cause symptom recurrence. We hypothesized that the 8-wire biliary basket catheter could be suitable for MPD stone extraction and aimed to analyze its ability to achieve more complete clearance of MPD residual/microstones.
Patients and methods Patients suspected of having MPD residual/microstones ≤ 5 mm because of abdominal symptoms, computed tomography examination results, and pancreatography results after previous therapy, including ERCP, EHL, and extracorporeal shock wave lithotripsy, were retrospectively enrolled. Patients with severe MPD stenosis/biliary obstruction requiring ERCP drainage were excluded. Extraction of residual/microstones was attempted using an 8-wire basket that is widely expandable in the narrow pancreatic duct and can capture and sweep stones in the narrow pancreatic duct. Technical success was defined as extraction of residual/microstones. The primary outcome was the technical success rate. Secondary outcomes were therapeutic details of stone extraction using the 8-wire basket catheter, including symptom improvements.
Results The technical success rate was 100% for seven patients; 1 to 8 residual/microstones were extracted. An improvement was observed in five patients with symptoms after the previous therapy. Three patients underwent residual stone extraction after extraction using a dedicated basket. No patient experienced symptom recurrence during the 270-day follow-up period.
Conclusions The 8-wire basket resulted in successful MPD residual/microstone extraction and pancreatic symptom improvement. This method may prevent symptom recurrence caused by incomplete residual/microstone clearance.
Introduction
Main pancreatic duct (MPD) stones cause pain and reduce quality of life [1]. Extracorporeal shockwave lithotripsy (ESWL) is recommended for treatment of obstructive radiopaque MPD stones larger than 5 mm in the head/body of the pancreas; however, the rate of complete stone clearance using ESWL is only 70% [2]. Recently, pancreatoscopy-guided electrohydraulic lithotripsy (EHL) has become an attractive alternative to ESWL, with reported technical and clinical success rates of more than 85% [3].
Endoscopic retrograde cholangiopancreatography (ERCP), comprising pancreatic sphincterotomy and pancreatic basket/balloon, is the standard method of extracting radiolucent MPD stones smaller than 5 mm [2]. Additional extraction of residual pancreatic stones using ERCP after fragmentation by ESWL has not been recommended by studies that included limited numbers of patients and follow-up periods [4]. However, according to a recent study, the long-term symptom recurrence rate associated with incomplete stone clearance was significantly higher than that associated with complete stone clearance, and small residual stones, including those remaining after adequate fragmentation using ESWL or EHL, may cause symptom recurrence [5].
Patients sometimes experience pancreatic pain caused by MPD residual/microstones and require endotherapy. Residual/microstone clearance using a dedicated basket catheter has been previously reported [5] [6]. However, we hypothesized that an 8-wire basket catheter, which is usually used for clearance of bile duct stones [7], could be suitable for MPD residual/microstone extraction because of its design, shape, and rotating function. The usefulness of the 8-wire basket catheter for treating pancreatic stones has not yet been reported. Therefore, this pilot study analyzed the ability of the 8-wire basket catheter to achieve complete clearance of pancreatic residual/microstones.
Patients and methods
Eligibility criteria
This retrospective case series was designed and conducted according to the principles of the Declaration of Helsinki. This study was registered in the University Hospital Medical Network Clinical Trials Registry (UMIN000052706) after receiving approval from our Institutional Review Board (IRB protocol number: 023007K). The requirement for informed consent was waived because of the retrospective nature of the study.
From January 2021 to September 2023, data from consecutive patients with symptomatic chronic pancreatitis and pancreatic stones were retrospectively extracted from the electronic medical records. MPD stones were confirmed by evaluating upstream MPD dilation via endoscopic ultrasound or computed tomography (CT). Patients with suspected MPD residual/microstones ≤ 5 mm in the pancreatic head and body because of abdominal symptoms, CT examination results, and pancreatography results after previous therapy, including ERCP, EHL, and ESWL, and those who underwent ERCP stone extraction were included in the study. Patients with recent biliary obstruction/severe pancreatic stenosis requiring repeated ERCP drainage/stenting were excluded. Patients with severe MPD stenosis have a high risk of stone impaction.
Residual/microstone extraction
A duodenoscope (JF 260V; Olympus Medical Systems, Tokyo, Japan) was inserted in the duodenum and cannulated in the MPD using an ERCP catheter (Swish; Boston Scientific, Marlborough, Massachusetts, United States) with a 0.025-inch guidewire (M-through; Asahi Intecc, Aichi, Japan). MPD residual or microstones were extracted using an 8-wire basket catheter (Medi-Globe 8-wire nitinol basket; Medico Hirata Inc., Osaka, Japan) ([Fig. 1] a). The 8-wire basket catheter is typically used for biliary tract stone extraction. It is composed of eight nitinol wires with an outer sheath diameter of 8.5F and has a rotating function. The basket is widely expandable in the 5-mm narrow duct; therefore, it has the ability to capture/sweep stones in the narrow pancreatic duct ([Fig. 1] b, [Fig. 1] c). Temporary pancreatic stents were not placed after the procedure. Pancreatoscopy was not performed following the stone extraction.

A dedicated basket (Reforma; Piolax Medical Devices Inc., Kanagawa, Japan) is often used for MPD stone extraction. This basket is composed of nitinol wires with fine reticular structures, loose mesh, and an outer sheath tip diameter of 5.7F ([Fig. 1] d). It is also easily expandable in the 5-mm narrow duct ([Fig. 1] e, [Fig. 1] f). In some cases, the dedicated basket was used before stone extraction using the 8-wire basket catheter.
Definitions and outcomes
Technical success was defined as achievement of residual/microstone extraction using an 8-wire basket catheter. After 8-wire stone extraction, patients were followed every 3 to 6 months through medical interviews and imaging examinations, mainly CT, to evaluate improvements in symptoms and stone clearance.
The primary outcome was the technical success rate. Secondary outcomes were symptom improvement after the final stone extraction using the 8-wire basket catheter and therapeutic details of stone extraction using the 8-wire basket catheter.
Results
Patient flow is shown in [Fig. 2]. Seven patients with MPD stones, excluding patients with severe MPD stenosis/biliary obstruction requiring repeated pancreatic stent exchanges due to repeated obstructive pancreatitis/cholangitis, were finally enrolled. [Table 1] shows patient baseline characteristics and previous therapy before stone extraction using the 8-wire basket catheter. MPD stones had a diameter of 3 to 10 mm, and the dilated MPD of 3 to 10 mm. Previous therapy included pancreatic sphincterotomy (100% of patients), EHL (57.1% of patients), balloon dilation of slight MPD stenosis (28.6% of patients), and stone extraction using a dedicated nitinol basket (42.9% of patients). It was confirmed that the pancreatic stones had been broken into pieces by pancreatoscopy after the EHL. One patient underwent ESWL because the pancreatoscope could not be inserted to reach the MPD stone located deep in the pancreatic body. Previous therapy was performed one to four times.
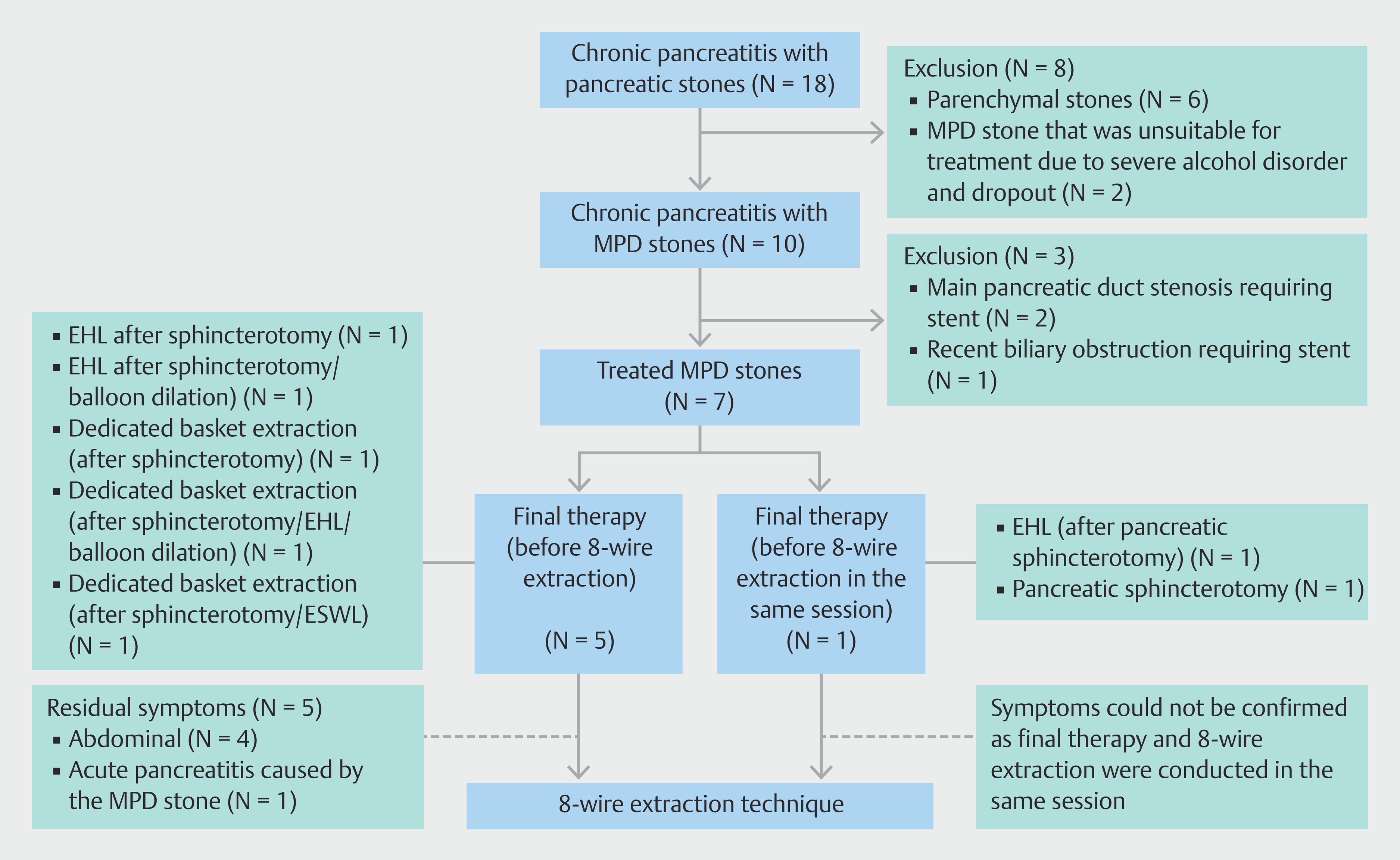
[Table 2] shows therapeutic details and outcomes of stone extraction using the 8-wire technique. All patients had standard anatomy, and stone extraction was undertaken via a major papilla. After the final therapy session performed before extraction using the 8-wire technique, 71.4% of patients experienced symptoms, including abdominal pain, discomfort, and acute pancreatitis, during a median of 33 days. The technical success rate was 100%, and one to eight residual/microstones were extracted. All five patients with symptoms after the final therapy session before 8-wire extraction experienced symptom improvement after undergoing 8-wire extraction ([Video 1]). Two patients underwent 8-wire stone extraction after the final endotherapy treatment in the same session. Three patients underwent residual stone extraction using the 8-wire basket catheter after stone extraction using the dedicated basket ([Fig. 3], [Video 1]). Three patients experienced an elevated serum amylase level; however, no patients experienced pancreatitis after ERCP.

Finally, 85.7% of patients experienced disappearance or decrease in size of MPD stones and improvement in upstream MPD dilation, as observed on CT, after extraction using the 8-wire basket catheter. During the median follow-up period of 270 days after the 8-wire technique for stone extraction, no patients experienced recurrent symptoms.
Discussion
During this study, patients experienced symptoms and a high success rate after previous endotherapy. All patients underwent multiple residual/microstone extractions using an 8-wire basket catheter. All patients who had symptoms before undergoing the 8-wire technique for stone extraction experienced symptom improvement.
Although the standard stone extraction balloon is also used to treat pancreatic stones, it is not designed for treatment of pancreatic duct. Adjusting the balloon diameter to the appropriate size is difficult, and the balloon often ruptures in the narrow pancreatic duct. In addition, excessive balloon expansion causes procedure-related pancreatitis. In addition, the sheath is often unable to reach the target stone. Therefore, the dedicated pancreatic stone basket was constructed [6].
However, in this study, all three patients who underwent stone extraction using the dedicated basket also underwent residual stone extraction using the 8-wire basket. The dedicated basket designed for MPD microstone extraction allows retractable catheter delivery and has a thin catheter diameter of 5.7F. The thin catheter can pass over the microstones in the narrow MPD ([Fig. 4] a). However, the basket mesh is dense, and relatively large stones that the catheter cannot pass over are pushed out during expansion ([Fig. 4] b, [Fig. 4] c, [Fig. 4] d).

The 8-wire basket catheter, which is usually used for biliary tract stone extraction, does not have a thin outer sheath. Therefore, the catheter cannot pass over relatively small stones ([Fig. 4] e). However, the nitinol material and characteristic spherical structure of the 8-wire offer flexibility and widely expand and surround the narrow pancreatic duct lumen compared with conventional stainless-steel catheters. The wires are expanded as a wide mesh in the narrow MPD and follow the shape of the lumen, thus allowing capture of MPD stones, including relatively large stones, in the basket lumen ([Fig. 4] f, [Fig. 4] g). The rotational structure makes it possible to capture more stones. Even when the catheters cannot pass through because of slight MPD stenosis, the 8-wire basket can be advanced and deployed. In addition, a slightly expanded basket with an inner stone package may sweep microstones ([Fig. 4] h). Therefore, the MPD stone retrieval ability of the 8-wire basket may be better than that of a dedicated pancreatic stone basket. Although our method is not unique, using an 8-wire basket may achieve more complete clearance of MPD stones.
According to a meta-analysis of the therapeutic efficacy of ESWL for MPD stones, complete and partial stone clearance rates were 70% and 22%, respectively, and only 53% and 33% of patients experienced no or mild-to-moderate pain, respectively, during the 2-year follow-up period. It has been estimated that 30% to 50% of patients with calcified chronic pancreatitis who undergo ESWL with or without ERCP experience recurrent symptoms [2].
EHL/laser lithotripsy during pancreatoscopy are recommended for extraction of MPD stones. A recent meta-analysis reported no significant difference in technical success, duct clearance, or adverse events between both techniques [3].
The reported MPD clearance rate ranges from 43% to 100% [2] [3], and the rates of complete and partial pain relief are 61.8% and 20.6%, respectively, during a 6-month follow-up period [8].
Early symptom recurrence within 3 months of ERCP for stone extraction may be caused by residual MPD stones [6], and incomplete stone extraction is a significant risk factor for recurrent pancreatic pain; however, complete stone extraction during endotherapy is technically difficult [9]. Some studies have reported that ESWL with systemic ERCP may not be valid because pancreatic pain did not improve [4]. However, confirmation of complete stone extraction is difficult in clinical practice because residual/microstones are not detectable using pancreatography and CT.
According to a recent study, 62.5% of patients who underwent incomplete stone clearance experienced symptom recurrence. The dedicated basket resulted in a symptom recurrence rate of 16.7% after complete stone clearance; however, use of a conventional device resulted in a symptom recurrence rate of 47.2% [5]. Furthermore, the recurrence rate increased as the follow-up period increased. This finding suggests that latent residual stones may cause symptom recurrence. Similarly, undetectable residual fragmented stones may cause symptom recurrence [5]. In addition, radiolucent protein plugs may become calcified and symptomatic during the clinical course [2]. Furthermore, complete MPD stone clearance is required to prevent symptom recurrence, and stone extraction using the 8-wire technique may facilitate this clearance.
Although no patient experienced basket impaction and pancreatitis in this study, the 8-wire technique may cause basket impaction or post-procedure pancreatitis, especially in cases with MPD stenosis. Release of the impacted basket is possible; however, the 8-wire basket catheter should be extracted after dilation of downstream slight stenosis in the MPD. ESWL/stone crusher/EHL has been reported to be useful for rescue stone removal in cases of basket impaction [10]. Extraction of pancreatic stones has a higher risk of pancreatitis than that of choledocholithiasis. To prevent pancreatitis, a temporary pancreatic stent should be considered [2] in cases involving 8-wire extraction.
To the best of our knowledge, this is the first series to report usefulness of the 8-wire basket catheter for MPD residual/microstone clearance and symptom improvement. However, this study has some limitations. Some patients did not experience severe pancreatic pain, and the number of patients analyzed was small. In addition, long-term outcomes of MPD residual/microstone extraction could not be observed during this study. Therefore, further comparative studies should analyze symptom recurrence among a larger number of patients during long-term follow-up.
Conclusions
In conclusion, MPD residual/microstone extraction using an 8-wire basket catheter was achieved with a high success rate and contributed to improvement in pancreatic symptoms. This method may help prevent symptom recurrence associated with MPD residual/microstones.
Conflict of Interest
The authors declare that they have no conflict of interest.
-
References
- 1 Löhr JM, Dominguez-Munoz E, Rosendahl J. et al. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United European Gastroenterol J 2017; 5: 153-199
- 2 Dumonceau JM, Delhaye M, Tringali A. et al. Endoscopic treatment of chronic pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Updated August 2018. Endoscopy 2019; 51: 179-193
- 3 McCarty TR, Sobani Z, Rustagi T. Per-oral pancreatoscopy with intraductal lithotripsy for difficult pancreatic duct stones: a systematic review and meta-analysis. Endosc Int Open 2020; 8: E1460-e1470
- 4 Dumonceau JM, Costamagna G, Tringali A. et al. Treatment for painful calcified chronic pancreatitis: extracorporeal shock wave lithotripsy versus endoscopic treatment: a randomised controlled trial. Gut 2007; 56: 545-552
- 5 Saito T, Nakai Y, Mizuno S. et al. Long-term outcome of endotherapy for pancreatic stones by using a dedicated pancreatic basket catheter. J Gastroenterol Hepatol 2021; 36: 2424-2431
- 6 Sasahira N, Isayama H, Tokyokawa Y. et al. A novel basket catheter to facilitate endoscopic removal of pancreatic stones (with video). Gastrointest Endosc 2013; 78: 925-929
- 7 Kaneko T, Ishii T, Hamanaka J. et al. Novel 8-wire basket catheter is useful for endoscopic removal of common bile duct stones up to 10 mm: A multicenter prospective study. J Hepatobiliary Pancreat Sci 2024; 31: 213-221
- 8 Gerges C, Albers D, Schmitz L. et al. Digital single-operator pancreatoscopy for the treatment of symptomatic pancreatic duct stones: a prospective multicenter cohort trial. Endoscopy 2023; 55: 150-157
- 9 Tadenuma H, Ishihara T, Yamaguchi T. et al. Long-term results of extracorporeal shockwave lithotripsy and endoscopic therapy for pancreatic stones. Clin Gastroenterol Hepatol 2005; 3: 1128-1135
- 10 Yagi S, Kurita Y, Nakajima A. Removal of pancreatic stones stuck in basket catheter with peroral pancreatoscopy and electronic hydraulic lithotripsy. Dig Endosc 2021; 33: e14-e15
Correspondence
Publication History
Received: 27 May 2024
Accepted after revision: 12 October 2024
Accepted Manuscript online:
28 October 2024
Article published online:
18 November 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Georg Thieme Verlag KG
Oswald-Hesse-Straße 50, 70469 Stuttgart, Germany
-
References
- 1 Löhr JM, Dominguez-Munoz E, Rosendahl J. et al. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United European Gastroenterol J 2017; 5: 153-199
- 2 Dumonceau JM, Delhaye M, Tringali A. et al. Endoscopic treatment of chronic pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Updated August 2018. Endoscopy 2019; 51: 179-193
- 3 McCarty TR, Sobani Z, Rustagi T. Per-oral pancreatoscopy with intraductal lithotripsy for difficult pancreatic duct stones: a systematic review and meta-analysis. Endosc Int Open 2020; 8: E1460-e1470
- 4 Dumonceau JM, Costamagna G, Tringali A. et al. Treatment for painful calcified chronic pancreatitis: extracorporeal shock wave lithotripsy versus endoscopic treatment: a randomised controlled trial. Gut 2007; 56: 545-552
- 5 Saito T, Nakai Y, Mizuno S. et al. Long-term outcome of endotherapy for pancreatic stones by using a dedicated pancreatic basket catheter. J Gastroenterol Hepatol 2021; 36: 2424-2431
- 6 Sasahira N, Isayama H, Tokyokawa Y. et al. A novel basket catheter to facilitate endoscopic removal of pancreatic stones (with video). Gastrointest Endosc 2013; 78: 925-929
- 7 Kaneko T, Ishii T, Hamanaka J. et al. Novel 8-wire basket catheter is useful for endoscopic removal of common bile duct stones up to 10 mm: A multicenter prospective study. J Hepatobiliary Pancreat Sci 2024; 31: 213-221
- 8 Gerges C, Albers D, Schmitz L. et al. Digital single-operator pancreatoscopy for the treatment of symptomatic pancreatic duct stones: a prospective multicenter cohort trial. Endoscopy 2023; 55: 150-157
- 9 Tadenuma H, Ishihara T, Yamaguchi T. et al. Long-term results of extracorporeal shockwave lithotripsy and endoscopic therapy for pancreatic stones. Clin Gastroenterol Hepatol 2005; 3: 1128-1135
- 10 Yagi S, Kurita Y, Nakajima A. Removal of pancreatic stones stuck in basket catheter with peroral pancreatoscopy and electronic hydraulic lithotripsy. Dig Endosc 2021; 33: e14-e15