

RSS-Feed abonnieren
DOI: 10.1055/s-0034-1391964
A prospective randomized study of the difference in diagnostic yield between endoscopic ultrasound-guided fine-needle aspiration (EUSFNA) needles with and without a side port in pancreatic masses
Autor*innen
Corresponding author
Publikationsverlauf
submitted 10. Dezember 2014
accepted after revision 04. März 2015
Publikationsdatum:
26. Mai 2015 (online)

Background and study aims: Two 22G needles with similar designs, apart from the absence (A) or presence of a side port (B), are available for endoscopic ultrasound (EUS)-guided fine-needle aspiration (FNA). The side port was designed to increase diagnostic yield but this advantage was unproven. This study evaluated the difference in diagnostic yield between both needles in pancreatic masses.
Patients and methods: This was a prospective multicenter randomized cross-over study. Patients with pancreatic masses were randomized to one needle for the first two passes, followed by the other for the next two passes. A pathologist blinded to the needle assessed each puncture for cellularity and morphology. The diagnostic yield between both needles was compared.
Results: In total, 30 patients were recruited (mean lesion size: 3.5 cm, range: 1.2 – 6.3). Comparison of cellularity adequacy: first pass: A vs. B: 26/30 vs. 24/30 (P = 0.488): 2nd pass: A vs. B: 25/30 vs. 26/30 (P = 0.718). Comparison of diagnostic accuracy: first pass: A vs. B: 22/30 vs. 23/30 (P = 0.766); after two passes: A vs. B: 26/30 vs. 26/30 (P = 1.0). When all four passes were assessed, adequate cellularity was obtained in 29/30 and the correct diagnosis was obtained in 28/30 patients. There were no procedural complications.
Conclusions: There was no significant difference in diagnostic yield between EUSFNA needles with or without a side port for pancreatic masses.
Study registration: NCT02092519.
Introduction
Endoscopic ultrasound-guided fine-needle aspiration (EUSFNA) is an important diagnostic tool, with an excellent safety profile [1] [2] [3]. The diagnostic yield of EUSFNA varies depending on the type of lesion. It is generally regarded that solid pancreatic masses are the most difficult lesions on which to perform EUSFNA, and generally, a higher number of needle passes is required to obtain adequate cytological samples and achieve an acceptable diagnostic yield, compared to lesions such as lymph nodes and liver lesions [2] [3]. In addition, EUS-guided core biopsies, rather than EUSFNA, would be required in the context of suspected lymphoma or gastrointestinal stromal tumors, because histological rather than cytological evaluation would be needed [3]. The somewhat lower rates for solid pancreatic lesions compared to lymph nodes could be due to the underlying desmoplastic changes associated with pancreatic malignancies, especially if there is underlying chronic pancreatitis or when the tumor is well differentiated.
To improve the diagnostic yield of EUSFNA, measures such as having rapid on-site cytopathological evaluation of the aspirated material to guide the number of needle passes being performed, performing a predetermined minimum number of needle passes in the absence of rapid on-site cytopathological evaluation, using a fanning mechanism during the EUSFNA process, or application of suction, are used [4] [5]. In addition, needle designs may be modified and one such innovation is a needle with a cutting mechanism located at the side of the needle tip that can facilitate obtaining core biopsies and improve diagnostic yield (Procore needle; Cook Medical, Bloomington, IN, United States) [6] [7]. Recently, another new 22 gauge (G) needle was introduced with a side port at the needle tip (Olympus, Tokyo, Japan). The theoretical basis for introduction of the side port was to facilitate the process of fine-needle aspiration (FNA), and to increase the diagnostic yield for cytology. This is different from the Procore needle which aimed to obtain histology. There have been preliminary retrospective or non-randomized non-comparative data on a mixture of lesions that suggested a high diagnostic yield with this side port needle [8] [9]. However, there are no prospective multicenter randomized controlled studies to ascertain the validity of the assumption. In particular, it would be of interest to determine whether this new needle design could increase the diagnostic yield for lesions such as pancreatic masses on which it is difficult to perform EUSFNA, but which at the same time, only require adequate cytology and not histology to achieve diagnosis.
The study aimed to compare the diagnostic yield of 22G needles with or without a side port during EUSFNA of pancreatic masses.
Patients and methods
Setting and trial design
This was an international, multicenter, single blinded, randomized, prospective pilot study that compared the diagnostic yield of 22G EUSFNA needles with or without a side port in the context of EUSFNA of pancreatic masses. Three tertiary institutions were involved: (1) Department of Gastroenterology and Hepatology, Changi General Hospital, Singapore; (2) Division of Gastroenterology, Asan Medical Centre, Seoul, Korea; (3) Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan.
Subjects
The study period was from April 2013 to March 2014. The inclusion criterion was all patients referred for EUSFNA of pancreatic masses who provided written informed consent for procedure and study participation. The exclusion criteria were: (1) presence of active gastrointestinal bleeding; (2) presence of coagulopathy as defined by a platelet count < 50 000/mm3 and/or international normalized ratio > 1.5; (3) the current use of thienopyridines (e. g. clopidogrel) in patients requiring antiplatelet therapy [10]; (4) absence of procedural informed consent. The protocol was approved by the local Institutional review boards and all patients gave informed consent for the study and procedure. The study was registered at ClinicalTrials.gov (NCT02092519).
Interventions
The two 22G needles being compared were both manufactured by Olympus (Tokyo, Japan) and were similar in design apart from the absence or presence of a side port, i. e. EZ-Shot 2 (model: NA-220H-8022) and EZ-Shot 2 with side port (NA-230H-8022) ([Fig. 1]). The needles were packaged with a 20 mL syringe for application of suction. Full suction was used during EUSFNA. Randomization of the needle used for initial puncture was carried in blocks of five with equal assignment. Once the first two punctures had been performed, the alternative needle was used for the subsequent two needle passes.

EUSFNA was performed using a curvilinear echoendoscope according to standard techniques by an experienced credentialed endoscopist [11]. The pancreatic mass was visualized, and the 22G needle (depending on randomization, either with or without side port) was introduced into the accessory channel of the echoendoscope and the mass was punctured under real time ultrasonic guidance. After withdrawal of the stylet and application of suction by attachment of a syringe with negative pressure, the needle was moved to and fro within the lesion, and then the needle was withdrawn and the aspirated material was expressed onto glass slides by reinsertion of the stylet, and direct smears were made either by the endoscopist or cytotechnician. This process was repeated once using the first needle. The alternative needle was then used to make two further punctures.
After expressing the cellular material onto glass slides, half the slides were air-dried and half were fixed with alcohol (95 % ethanol) for subsequent cytological assessment. An adequate specimen was defined as at least four clusters of pancreatic acinar cells with or without the presence of malignant-appearing cells. A cytopathologist blinded to the needle used for EUSFNA characterized each individual needle pass for assessment of adequate cellularity (0 [inadequate] or 1 [adequate]) and made a diagnosis of malignancy (insufficient, normal, “suspicious,” malignant). The diagnosis arrived at for each needle pass was compared with the final diagnosis which was based on a composite of cytology, histology, and clinical course over the next 6 months.
Statistics
As this was an exploratory study, we aimed for a total sample size of 30 pancreatic masses, with each center contributing 10 cases. The intent was to review the outcome and then decide whether to extend the study based on the observed trend. To be able to show an increase in diagnostic yield from 85 % (the current performance target for EUSFNA of pancreatic malignancy) [2] to 95 % with a power of 80 % would have required a sample size of 140 in a two tailed test. The outcome variables were: (1) compare 1st pass cellular adequacy rates of each needle; (2) compare the overall cellular adequacy rate of each needle; (3) compare 1st pass diagnostic accuracy adequacy rate of each needle; (4) compare the overall diagnostic accuracy rate between both needles. These categorical data were analysed using the Chi-squared or Fisher’s exact test. A P value of < 0.05 was taken to be statistically significant. Statistical analysis was performed using SPSS V.19.0 software (SPSS Inc, Chicago, IL, United States).
Results
Patients
A total of 30 patients with pancreatic masses were recruited for the study. The mean age was 65.2 years (range: 43 – 82; SD [11.3]) and 53 % were women. The mean size of the pancreatic mass was 3.5 cm (range: 1.2 – 6.3; SD [1.2]). In terms of location of the pancreatic masses, 15 (50 %) were located at the pancreatic head, 7 (23.3 %) were located at the pancreatic neck or body and 8 (26.7 %) were located at the pancreatic tail. Each patient had four EUSFNA needle passes; overall, a total of 120 needle passes were performed. There were no EUSFNA related adverse events or complications. Based on a diagnostic gold standard that combined cytology, histology, and clinical course, the final diagnoses of these lesions were pancreatic adenocarcinoma (24/30), pancreatic neuroendocrine tumor (2/30), distal cholangiocarcinoma (1/30), pancreatitis related pseudotumor (2/30), and serous cystadenoma (1/30).
Assessment of cellularity
Assessment of adequacy of cellularity was performed for each individual needle pass. The yield for the individual first and second needle passes, and when both passes were combined, was compared between the two needles. When needles with and without a side port were compared, there were no statistically significant differences in terms of achieving adequate cellularity of aspirate in the first pass (80 vs. 86.7 %, P = 0.488) and after two needle passes (93.3 % vs. 96.7 %, P = 0.554). After four needles passes, adequate cellularity of aspirate was achieved in 96.7 % (29/30) of cases. Results are summarized in [Table 1].
Assessment of cellular morphology and diagnostic accuracy
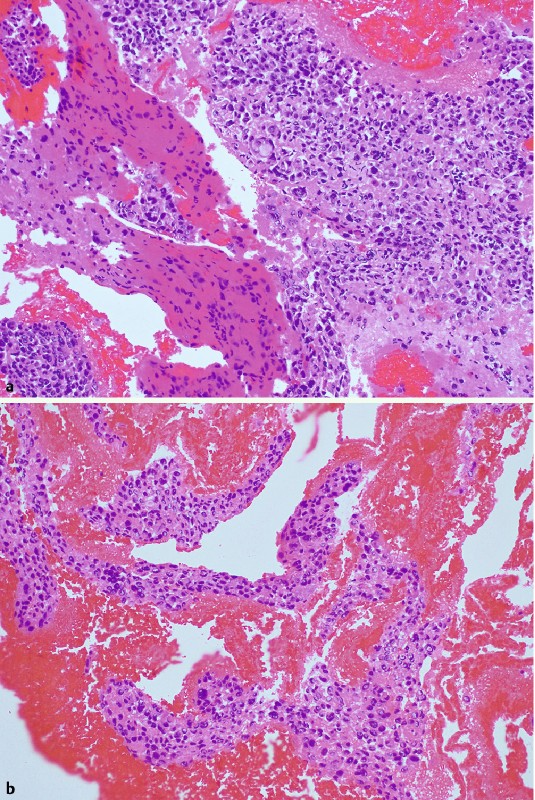
Assessment of cellular morphology was performed for each individual needle pass. The outcome for the individual first and second needle pass, as well as when both passes were combined, was compared between the two needles. Results are summarized in [Table 2]. In terms of diagnostic accuracy, there were no statistically significant differences between needles with or without side port ([Fig. 2 a, b] and [Fig. 3 a, b]) for the first pass (76.7 % vs. 73.3 %, P = 0.766) and when both needle passes were combined (86.7 % vs. 86.7 %, P = 1). When the four passes for each lesion were assessed together, the correct diagnosis was obtained in 24/24 cases of pancreatic adenocarcinoma, 1/2 neuroendocrine tumor, 2/2 pseudotumor, 1/1 serous cystadenoma and 0/1 case of cholangiocarcinoma, giving an overall diagnostic accuracy of 96.7 % (28/30).

Discussion
Our results showed that having an additional side port at the needle tip did not increase cytological yield for EUSFNA of pancreatic masses. The concept behind the needle design was to have an additional opening to permit passive inflow of aspirate during the EUSFNA process. In experienced hands, high rates of cytological and diagnostic yield could be achieved, regardless of whether or not there was a side port. As mentioned earlier, this needle design is somewhat different from that of a core biopsy needle, which has an additional large port with a cutting edge at the end of the needle; this cutting edge facilitates obtaining histological specimens.
In our study design, we randomized the sequence of needle used for puncture, and each needle was used twice, with a total of four passes per patient. This was to balance efficacy and safety, given that a potentially higher complication rate may occur with more needle passes. Pellisé Urquiza et al. showed that, in the context of pancreatic masses, the cytological yield plateaued off after four needle passes [4]. In addition, recent studies also suggested that a satisfactory yield may be achieved with two needle passes, especially if the material gathered with a 22G needle was also sent for histopathological examination in addition to cytopathological analysis [12] [13]. Although there have been reports which have suggested that the use of suction may increase bloodiness of the aspirate without increasing the diagnostic yield [14], we used suction in all cases, given the anticipated lower yield from pancreatic masses compared to tissues such as lymph nodes, as well as the fact that suction has been shown to be useful in the context of pancreatic masses [3] [15].
Two other studies have been published concerning side port needles. Kaffes and Corte first published their initial experience in 16 consecutive patients [8]. It was a single center case series and comprised a mixture of lesions including pancreatic masses, lymph nodes, and cysts. On-site cytopathological assessment was available. Diagnostic material was obtained at the first pass in 56.2 % of patients. The mean number of passes required to reach a diagnosis was 2.1. Diagnosis was made on first pass in 62.5 % of solid non-lymph node lesions. The diagnosis was reached in 94 % of patients [8]. They subsequently published a multicenter, non-comparative study in which 30 patients with solid lesions were evaluated. The indications included pancreatic or biliary masses (24), retroperitoneal or peri-duodenal masses (2), enlarged lymph node (2), a gastric submucosal tumor, and a subcarinal mass. All but one case had a diagnosis made (96.7 %). The mean number of passes required to reach a diagnosis was 1.7 [9]. Both studies were non-comparative and it was uncertain whether it was truly the presence of the side port that resulted in the high diagnostic yield. Importantly, our study differed from these two studies. It enrolled a homogenous group of patients with pancreatic masses; it is known to be more difficult to perform EUSFNA in these masses. In addition, it was a prospective randomized study that compared two 22G needles. We established that the presence of the side port did not further increase diagnostic yield.
Our study had several strengths. It was multicenter, prospective, and comparison was randomized. The cytopathologist was blinded to the needle used for each puncture. Limitations included the relatively small sample size and the fact that the endoscopist was not blinded to the needle used. It may have been better to randomize and use one needle per patient, such that all four passes were made using the same needle for each patient. However, using both needles for a single lesion had the potential advantage of addressing intrapatient variations and confounders, such that the same type of lesion was evaluated each time. It is also not practical to perform four needle passes with each needle, with a total of eight needle passes per patient, given the risk. We set a predetermined number of needle passes to standardize the evaluation of the diagnostic yield of each needle, and also to overcome the problem of no on-site cytopathological assessment.
To conclude, the 22G EUSFNA side port needle is safe and effective. However, there was no significant difference in diagnostic yield between EUSFNA needles with or without a side port for pancreatic masses. After four passes, adequate cellularity was obtained in 96.7 % of patients and the correct diagnosis was achieved in 93.3 %.
Competing interests: The study was independently designed and conducted by the authors. However, all needles were provided as samples by Olympus (Tokyo, Japan).
-
References
- 1 Gan SI, Rajan E, Adler DG et al. The role of EUS. Gastrointest Endosc 2007; 66: 425-434
- 2 Wani S, Wallace MB, Cohen J et al. Quality indicators for EUS. Gastrointest Endosc 2015; 81: 67-80
- 3 Polkowski M, Larghi A, Weynand B et al. Learning, techniques, and complications of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Technical Guideline. Endoscopy 2012; 44: 190-205
- 4 Pellisé Urquiza M, Fernández-Esparrach G, Solé M et al. Endoscopic ultrasound-guided fine needle aspiration: predictive factors of accurate diagnosis and cost-minimization analysis of on-site pathologist. Gastroenterol Hepatol 2007; 30: 319-324
- 5 Holt BA, Varadarajulu S, Hebert-Magee S. High-quality endoscopic ultrasound-guided fine needle aspiration tissue acquisition. Adv Ther 2014; 31: 696-707
- 6 Iglesias-Garcia J, Poley JW, Larghi A et al. Feasibility and yield of a new EUS histology needle: results from a multicenter, pooled, cohort study. Gastrointest Endosc 2011; 73: 1189-1196
- 7 Hucl T, Wee E, Lakhtakia S et al. Feasibility and efficiency of a new 22G core needle: a prospective comparison study. Endoscopy 2013; 45: 792-798
- 8 Kaffes A, Corte C. Fine needle aspiration at endoscopic ultrasound with a novel side-port needle: a pilot experience. Therap Adv Gastroenterol 2012; 5: 89-94
- 9 Kaffes AJ, Chen RY, Tam W et al. A prospective multicenter evaluation of a new side-port endoscopic ultrasound-fine-needle aspiration in solid upper gastrointestinal lesions. Dig Endosc 2012; 24: 448-451
- 10 Boustière C, Veitch A, Vanbiervliet G et al. Endoscopy and antiplatelet agents. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2011; 43: 445-461
- 11 Vilmann P, Saftoiu A. Endoscopic ultrasound-guided fine needle aspiration biopsy: equipment and technique. J Gastroenterol Hepatol 2006; 21: 1646-1655
- 12 Moller K, Papanikolaou IS, Toermer T et al. EUS-guided FNA of solid pancreatic masses: high yield of 2 passes with combined histologic-cytologic analysis. Gastrointest Endosc 2009; 70: 60-69
- 13 Turner BG, Cizginer S, Agarwal D et al. Diagnosis of pancreatic neoplasia with EUS and FNA: a report of accuracy. Gastrointest Endosc 2010; 71: 91-98
- 14 Wallace MB, Kennedy T, Durkalski V et al. Randomized controlled trial of EUS-guided fine needle aspiration techniques for the detection of malignant lymphadenopathy. Gastrointest Endosc 2001; 54: 441-447
- 15 Puri R, Vilmann P, Săftoiu A et al. Randomized controlled trial of endoscopic ultrasound-guided fine-needle sampling with or without suction for better cytological diagnosis. Scand J Gastroenterol 2009; 44: 499-504
Corresponding author
-
References
- 1 Gan SI, Rajan E, Adler DG et al. The role of EUS. Gastrointest Endosc 2007; 66: 425-434
- 2 Wani S, Wallace MB, Cohen J et al. Quality indicators for EUS. Gastrointest Endosc 2015; 81: 67-80
- 3 Polkowski M, Larghi A, Weynand B et al. Learning, techniques, and complications of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Technical Guideline. Endoscopy 2012; 44: 190-205
- 4 Pellisé Urquiza M, Fernández-Esparrach G, Solé M et al. Endoscopic ultrasound-guided fine needle aspiration: predictive factors of accurate diagnosis and cost-minimization analysis of on-site pathologist. Gastroenterol Hepatol 2007; 30: 319-324
- 5 Holt BA, Varadarajulu S, Hebert-Magee S. High-quality endoscopic ultrasound-guided fine needle aspiration tissue acquisition. Adv Ther 2014; 31: 696-707
- 6 Iglesias-Garcia J, Poley JW, Larghi A et al. Feasibility and yield of a new EUS histology needle: results from a multicenter, pooled, cohort study. Gastrointest Endosc 2011; 73: 1189-1196
- 7 Hucl T, Wee E, Lakhtakia S et al. Feasibility and efficiency of a new 22G core needle: a prospective comparison study. Endoscopy 2013; 45: 792-798
- 8 Kaffes A, Corte C. Fine needle aspiration at endoscopic ultrasound with a novel side-port needle: a pilot experience. Therap Adv Gastroenterol 2012; 5: 89-94
- 9 Kaffes AJ, Chen RY, Tam W et al. A prospective multicenter evaluation of a new side-port endoscopic ultrasound-fine-needle aspiration in solid upper gastrointestinal lesions. Dig Endosc 2012; 24: 448-451
- 10 Boustière C, Veitch A, Vanbiervliet G et al. Endoscopy and antiplatelet agents. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2011; 43: 445-461
- 11 Vilmann P, Saftoiu A. Endoscopic ultrasound-guided fine needle aspiration biopsy: equipment and technique. J Gastroenterol Hepatol 2006; 21: 1646-1655
- 12 Moller K, Papanikolaou IS, Toermer T et al. EUS-guided FNA of solid pancreatic masses: high yield of 2 passes with combined histologic-cytologic analysis. Gastrointest Endosc 2009; 70: 60-69
- 13 Turner BG, Cizginer S, Agarwal D et al. Diagnosis of pancreatic neoplasia with EUS and FNA: a report of accuracy. Gastrointest Endosc 2010; 71: 91-98
- 14 Wallace MB, Kennedy T, Durkalski V et al. Randomized controlled trial of EUS-guided fine needle aspiration techniques for the detection of malignant lymphadenopathy. Gastrointest Endosc 2001; 54: 441-447
- 15 Puri R, Vilmann P, Săftoiu A et al. Randomized controlled trial of endoscopic ultrasound-guided fine-needle sampling with or without suction for better cytological diagnosis. Scand J Gastroenterol 2009; 44: 499-504